
Abstract
Closed total talus dislocation from tibiotalar, subtalar, and talonavicular joints is a very rare injury. A 25-year-old young man, who had severe ankle distortion while walking down a flight of stairs, was brought to the emergency room complaining of a deformity and pain in his ankle joint. Roentgenographies revealed total talar body extrusion. The patient was treated urgently with open reduction in the authors’ clinic. Tibialis posterior tendon might prevent closed reduction so open reduction with retraction of the tendon may be necessary.
Keywords
The talus rests on the anterior two thirds of the calcaneus. It articulates with the tibia, fibula, and navicular bone. The saddle-shaped superior surface of the talus bears the weight transmitted via the tibia and transfers it onto the hindfoot. Talus lacks muscular attachment and 60% of its surface is covered with cartilage. Closed total talus dislocation from tibiotalar, subtalar, and talonavicular joints is a very rare injury that can occur as a result of high-energy exposure such as fall from a height or a motor vehicle accident.1,2 In this report, we present our experience of the treatment of a patient with closed subtalar dislocation with concomitant ipsilateral talar fracture. At 1 year postoperatively, the foot scored well in terms of stability and range of motion with no signs of avascular necrosis and arthritis.
Case Report
A 25-year-old young man, who had severe ankle distortion while walking down a flight of stairs, had been brought to our emergency room complaining of a deformity and pain in his ankle joint. Range of motion of ankle joint was very limited and his foot was in equinovarus deformity with the talus resting on the lateral side of the foot. Anteroposterior and lateral roentgenographies revealed a dislocated talus (Figure 1) and computed tomographic evaluation (Figure 2) also displayed a small fleck of medial talar body bone residing in its anatomic place.

Preoperative roentgenography.

Preoperative computed tomography scan.
In the operating room, closed reduction was tried urgently, but it was unsuccessful. So, open reduction was attempted using first the lateral horizontal incision over the dislocated talus but it was again impossible to reduce it, so vertical anteromedial medial incision was added, and tibialis posterior tendon was found to be entrapped in the ankle joint preventing the reduction. After reduction, stability was achieved using 2 Kirshner wires, one from navicula to talus and second from calcaneus to tibia (Figure 3). The fracture was found to be anatomically reduced after talar body reduction and was not internally fixed. The incision was repaired and short leg cast was applied. After the operation, capillary circulation of the digits was watched closely and no compartment syndrome sign occurred.
“Total talar dislocation is thought to be endpoint of maximum pronation or supination, coupled with a plantarflexion force placed across it.”
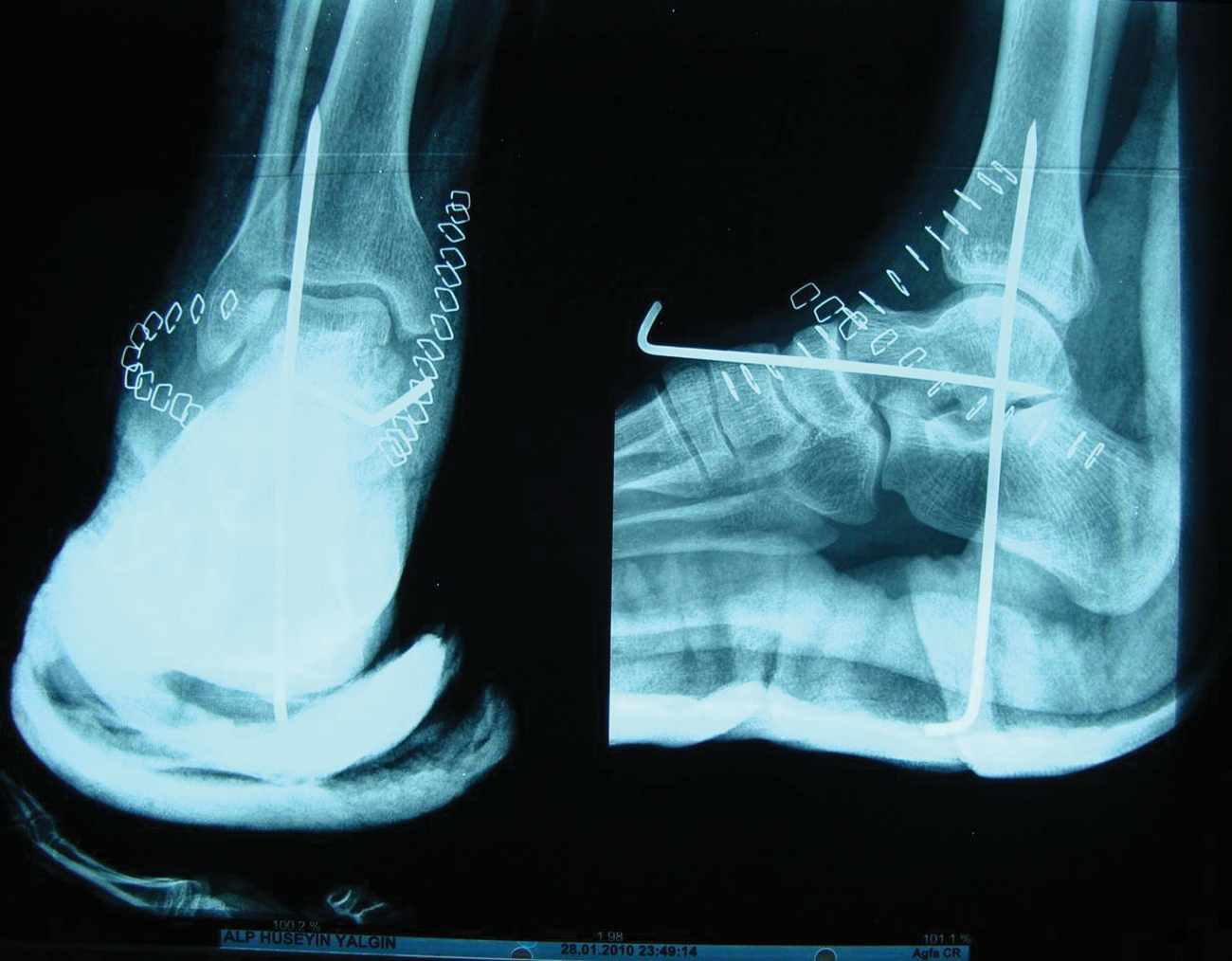
Early postoperative roentgenography.
Six weeks after the operation, the cast and K wires were removed. After the removal of the K wires, physiotherapy for range of motion was started. The patient was mobilized with partial weight bearing using crutches after the K wires were removed. The patient was mobilized with full weight bearing 10 weeks after the operation. After 16 weeks postoperation, radiographic control was done and Hawkins sign were observed (Figure 4). Ankle range of motion was 20° dorsiflexion and 40° plantarflexion (Figure 5). Nonetheless, he was having no ankle instability, was walking with no pain, and was out on a limb at his last control 1 year after the operation. His roentgenographies and magnetic resonance images also displayed no avascular necrosis and fracture nonunion.

Postoperative roentgenography after 4 months with Hawkins sign.

Postoperative ankle range of motion.
Discussion
Total talar dislocation is thought to be endpoint of maximum pronation or supination, coupled with a plantarflexion force placed across it. Leitner 3 described a 3-stage mechanism of dislocation; dislocation of the subtalar joint is the first stage of a total dislocation of talus followed by talonavicular and total extrusion as supination and pronation forces progress. Total talar dislocations are extremely rare. Also, long-term reports with good clinical outcome and no signs of avascular necrosis are few in number. For the treatment of this condition, some authors even recommended primary talectomy with tibiocalceneal fusion. 4 Closed or open reduction has also been mentioned as the treatment of choice in some reports.5,6
As in our case tibialis posterior tendon may prevent closed reduction, so open reduction with retraction of the tendon may be needed. No avascular necrosis was detected in our case and this might be because of minimal soft tissue dissection with preservation of blood supply to the talus.
Surgery was done urgently 1.5 hours after the traumatic event because the skin was tented. This might also have a positive impact on the preservation of the vascularity of the talus. We decided not to fix the fractured fragment because it was small and the fragment had anatomical apposition.
de Palma et al 7 reported 3 cases of irreducible isolated subtalar dislocations and in 2 patients with lateral dislocation where closed reduction failed because of interposition of the posterior tibialis tendon caused by a large tear of the flexor retinaculum. In their third case, a medial dislocation, a displaced extensor retinaculum prevented relocation of the talar head and required resection. 7
The direction of dislocation also seems to play a significant role in the final functional outcome. Medial subtalar dislocations have usually shown good results when treated conservatively, whereas lateral dislocations have been associated with significant disability. 8
If there is tendency to redislocate after reduction, as in our case, K wire transfixation or tibiocalceneal external fixator may be used.
Conclusion
Tibialis posterior tendon might be the structure responsible for closed reduction failure after total talus dislocation. Urgent treatment with minimal soft tissue dissection may prevent avascular necrosis and subsequent collapse of the talus.