
Abstract
The initial management of ankle fracture-dislocations is the crucial step in the treatment of these emergent traumatic injuries. A stepwise approach is necessary to properly evaluate, diagnose, and treat ankle fracture-dislocations. The goal of initial management is to evaluate the vascular status of the extremity and then restore proper alignment of the talus underneath the tibia. A retrospective review was performed on 40 patients, who presented to a community-based hospital emergency room, treated by the foot and ankle service for ankle fracture-dislocation. An analysis of patient demographics, injury pattern/classification, number of reduction attempts, and immobilization method was performed and evaluated. This analysis was correlated with a review of the literature to develop an algorithm for the initial management of ankle fracture-dislocations recommending the use of a bivalved below-the-knee fiberglass cast for maintained stabilization post reduction.
“A stepwise approach is required for the treatment of ankle fracture-dislocations and has been used for years by physicians treating these complex injuries.”
Introduction
Ankle fracture-dislocations are medical emergencies encountered by foot and ankle surgeons. The disruption of the ankle mortise can lead to significant complications if not evaluated and reduced in a timely manner.1(pp105-108),2-5 Emergent reduction of an ankle fracture-dislocation is warranted secondary to several important factors. Dislocation may compromise the vascular status of extremity, gross malalignment of the osseous structures creates pressure ischemia on areas of the skin, early reduction provides less postinjury edema, prompt dislocation reduction prevents further damage to articular cartilage, and realignment of the ankle provides pain relief.1-3(pp101-105),5-7
An ankle dislocation most commonly involves an associated ankle fracture.1,2,8,9 Because of the strong construct of the ligaments that stabilize the ankle mortise, pure dislocations are rare.1,9-12 When they occur, the initial management does not differ from that of an ankle fracture- dislocation where emergent reduction of the ankle dislocation is necessary.1,8,11,12
A stepwise approach is required for the treatment of ankle fracture- dislocations and has been used for years by physicians treating these complex injuries.1-5 Although these treatment protocols have been documented previously in word form, a treatment algorithm is yet to be developed. Using a combination of a review of the literature and clinical experience, an algorithm was developed for the treatment of ankle fracture-dislocations.
Patients and Methods
A retrospective review was performed on 40 patients (Table 1) who presented to a community-based hospital emergency room with an ankle fracture-dislocation treated by the foot and ankle service with reduction performed by one of the authors (JRB, SNP, AJT, or SESB) within 2 hours of injury. Treatment was performed using a stepwise treatment approach and standard reduction methods. An analysis of patient demographics, injury pattern/classification, number of reduction attempts, and immobilization method was performed and evaluated (Table 2). This analysis was correlated with a review of the literature to develop an algorithm for initial management of ankle fracture-dislocations (Figure 1). Although the primary focus of this article was to report our outcomes using a specified treatment algorithm for ankle fracture-dislocations, we also examined whether age, gender, fracture type, and method of postreduction immobilization (below-the-knee bivalved fiberglass cast or below-the-knee combination plaster splint—plaster of Paris back-slab along with plaster of Paris stirrup) were associated with failure to maintain initial reduction. Independent t test was used to test for differences in mean age. For fracture type, we grouped all ankle joint dislocations with supination external rotation (SER) IV injury pattern (n = 35) together and compared this type with all other injury patterns in the study—pronation abdution (PAB) III (n = 1), pronation external rotation (PER) IV (n = 1), Salter–Harris II (n = 1), and pilon (n = 1). Dichotomous independent variables (gender, fracture type, postreduction immobilization) were then examined for their association with a successfully maintained reduction using Fisher’s exact test. All tests were 2-tailed. P < .05 was considered significant.
Ankle Fracture-Dislocation Demographics
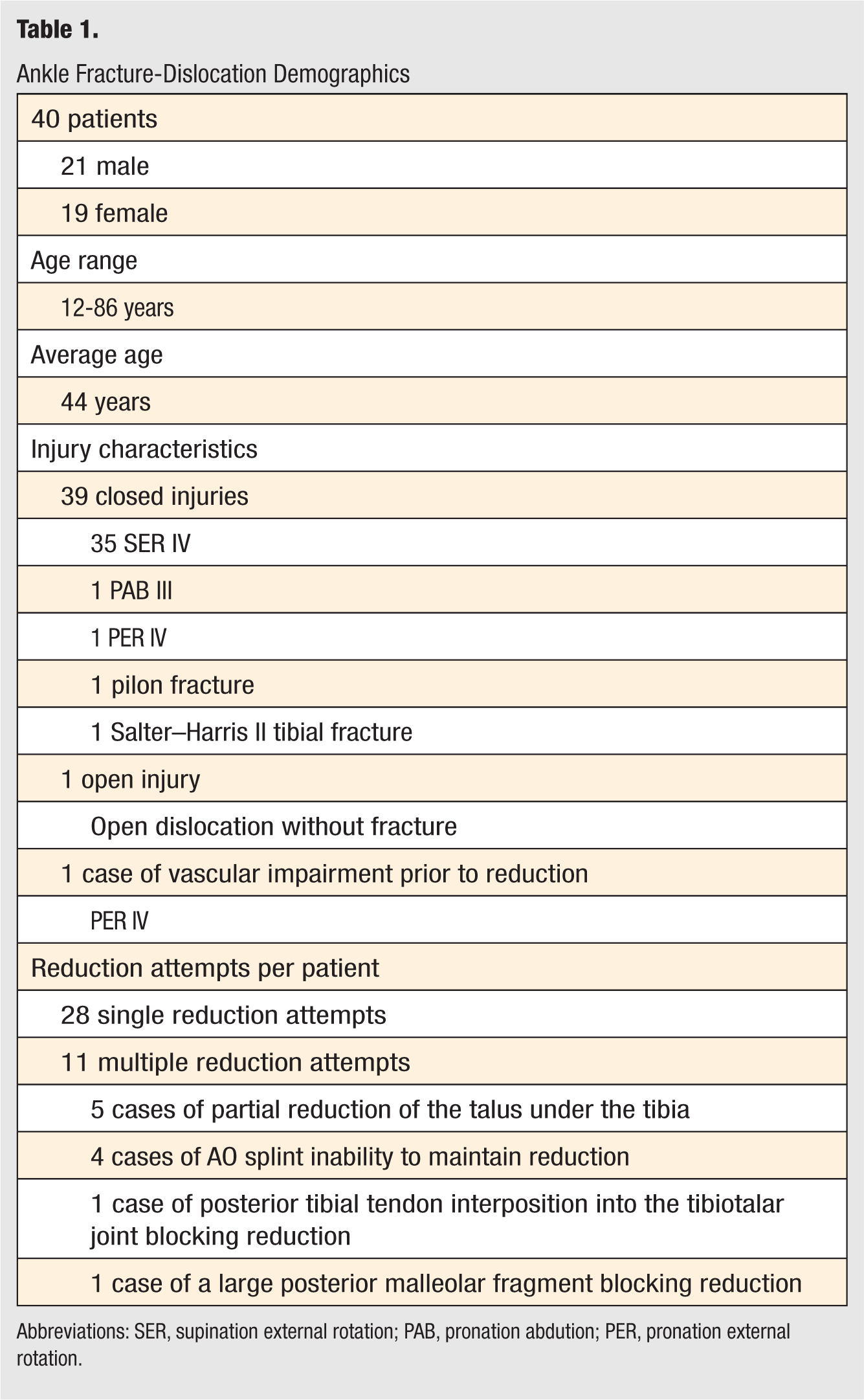
Abbreviations: SER, supination external rotation; PAB, pronation abdution; PER, pronation external rotation.
Analysis of Patient Demographics
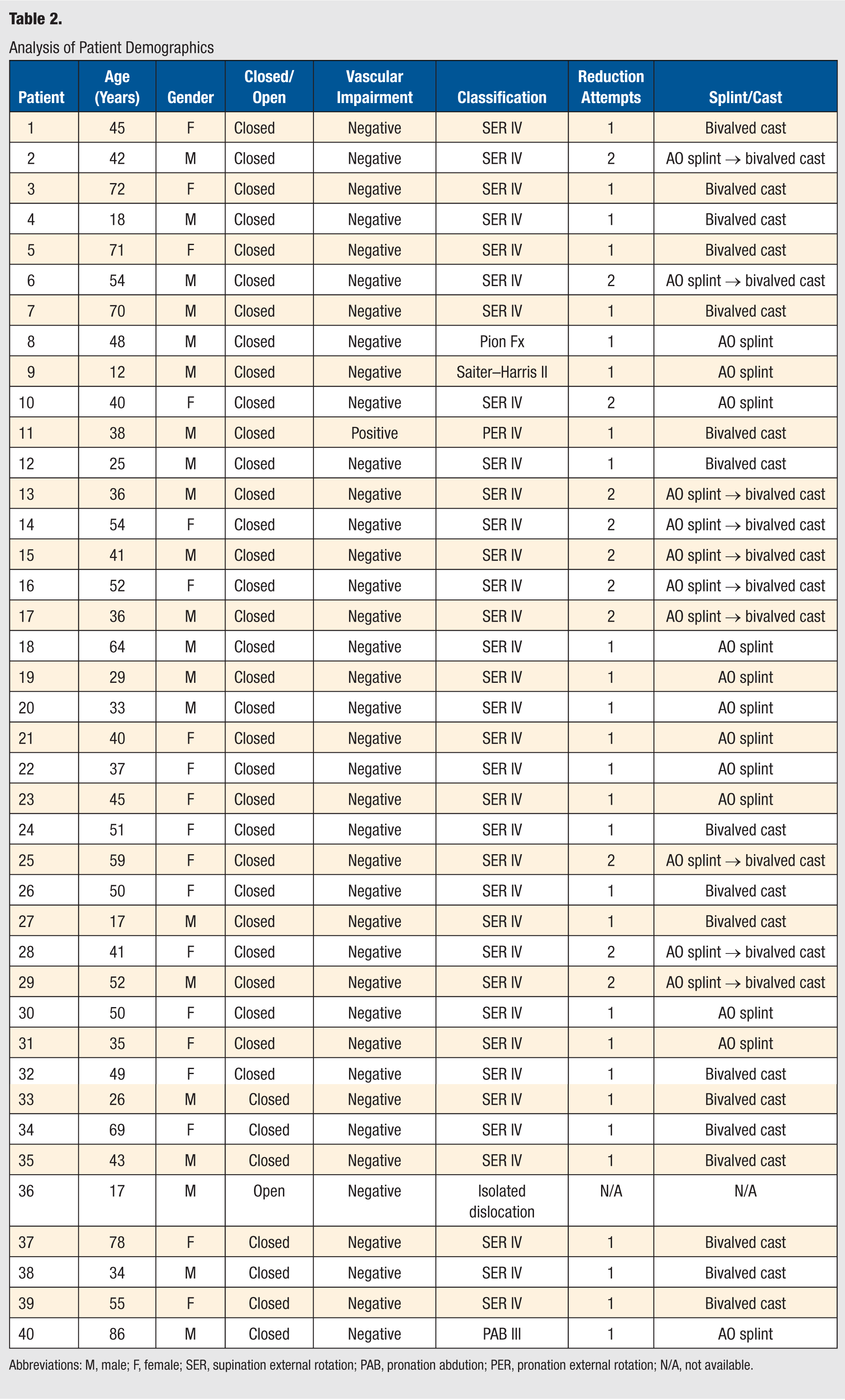
Abbreviations: M, male; F, female; SER, supination external rotation; PAB, pronation abdution; PER, pronation external rotation; N/A, not available.
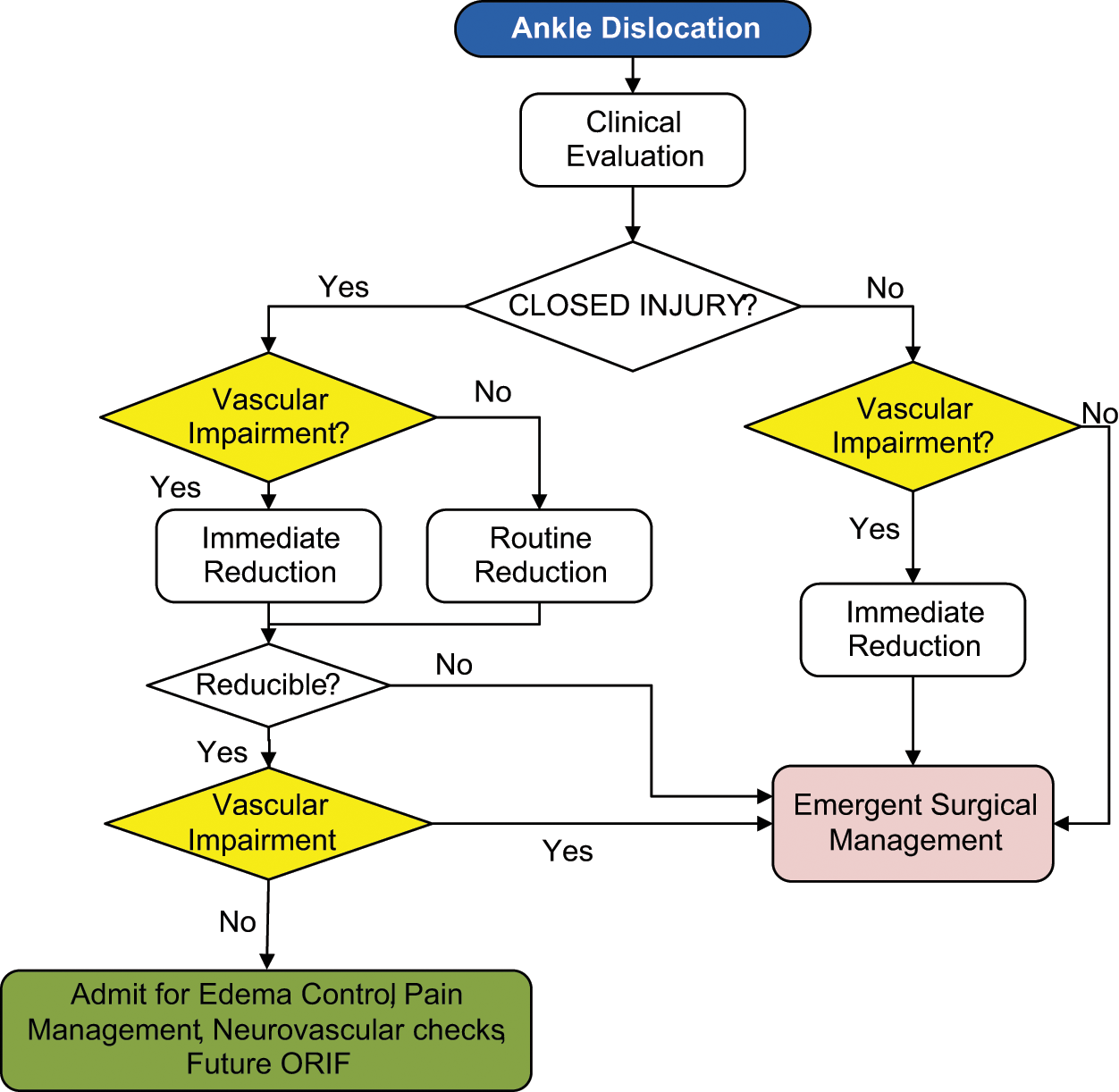
Initial management algorithm for ankle fracture-dislocations.
Results
Age, gender, and fracture type were not associated with the ability to maintain reduction (P > .05). However, those patients initially receiving a below-the-knee combination plaster splint were more likely to require a second reduction attempt because of failed stabilization than those receiving a below-the-knee bivalved fiberglass cast (50% [11/22] vs 0% [0/17], P = .0007). There were no cases of a loss of reduction when initially using a below-the-knee bivalved fiberglass cast for stabilization after closed reduction (Figure 2). Of note, all 11 cases of the use of a below-the-knee combination plaster splint that required a second reduction were subsequently reduced and correction maintained with the use of a below-the-knee bivalved fiberglass cast. Cases of a below-the-knee combination plaster splint not maintaining reduction were often secondary to the increased setting time of the plaster material in these unstable injury patterns (Figures 3). The setting time of plaster may take approximately 4 to 5 minutes depending on water temperature, with the colder the water the longer the setting time.

(A, B) Prereduction photographs of a 49-year-old female patient who sustained a left ankle fracture-dislocation after slipping on ice. (C, D) Anteroposterior and lateral prereduction radiographs. (E, F) Anteroposterior and lateral postreduction radiographs after closed reduction using a bivalved fiberglass cast, which reveal adequate reduction of the talus under the tibia. (G) Postreduction photograph of the bivalved fiberglass cast.

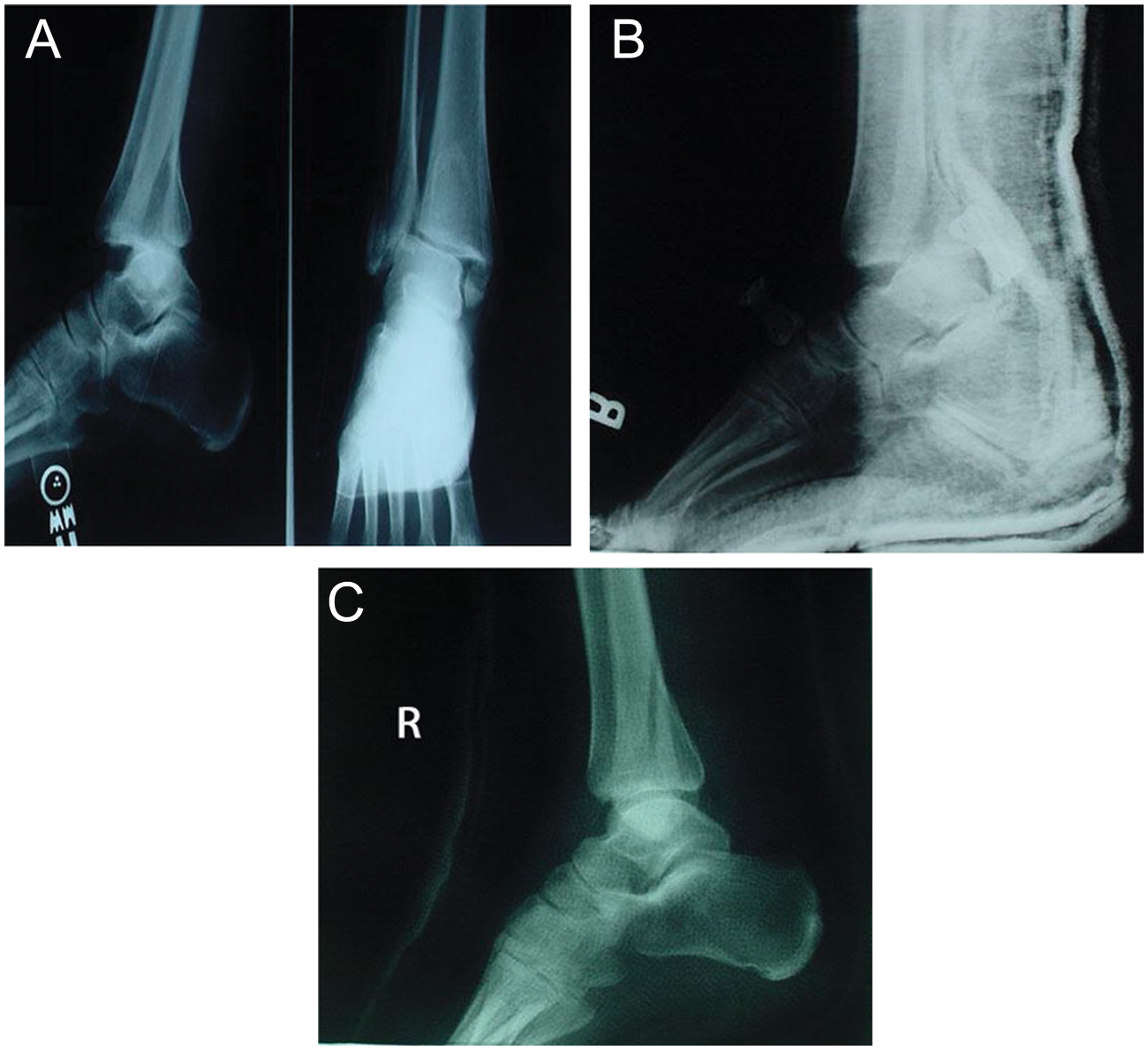
(A, B) Anteroposterior lateral and mortise prereduction radiographs of a 48-year-old male truck driver who sustained a left ankle pilon fracture-dislocation after stepping down out of his truck awkwardly, twisting the ankle. (C, D) Anteroposterior and lateral initial postreduction radiographs after closed reduction using a plaster AO splint, which reveal inadequate reduction of the talus under the tibia secondary to splint failure. (E, F) Anteroposterior and lateral second postreduction radiographs after closed reduction using a bivalved fiberglass cast, which reveal adequate reduction of the talus under the tibia.
Discussion
An ankle fracture-dislocation is an emergent traumatic injury to the lower extremity. Stabilization of any life-threatening injuries is performed prior to management of the injured extremity.13,14 Reduction of the fracture-dislocation is the gold-standard treatment management for the condition. The objectives of reduction are to restore proper alignment of the talus underneath the tibia, decrease soft tissue injury to the extremity, provide pain relief, and to prevent or restore vascular impairment to the extremity.1-4,7,14
The neurovascular status of the extremity and open versus closed injury are the 2 critical clinical entities that determine treatment management for an ankle dislocation.1,2,14,15 Neurovascular compromise is encountered secondary to arterial obstruction, as seen with posterior fibular displacement creating excessive tension on the extensor retinaculum causing obstruction of the dorsalis pedis artery. 16 Clinical signs of vascular impairment include absence of pulses via handheld Doppler evaluation of the deep peroneal artery and the posterior tibial arteries, ischemic skin changes, and delayed capillary fill time. Positive signs of vascular impairment require immediate reduction under conscious sedation or intra-articular local anesthesia block prior to any radiographic evaluation being performed.2,7,17,18 If there is continued vascular compromise with handheld Doppler evaluation after successful ankle realignment, emergent surgical intervention is necessary.
Open injury requires intravenous antibiotic therapy and emergent surgical management in the operating room setting. Irrigation and debridement of the open wound is performed along with reduction of the dislocation and osseous stabilization using internal or external fixation depending on fracture-dislocation instability and size and location of the open injury. 1 Tetanus status is determined and treated appropriately.
Closed injuries without vascular compromise are initially managed through closed reduction technique under conscious sedation or intra-articular local anesthesia block after initial prereduction radiographs are obtained.1,2,7 Once adequate reduction is obtained, the patient is admitted for edema control, pain management, neurovascular checks, and future surgical management for definitive internal or external fixation osseous stabilization.2,4,5
There are several methods for closed reduction noted in the literature.1,3,4,6,13,14,19,20 Quigley 13 described a method of traction using a trapeze and stockinette. A modified version of Quigley’s traction is valuable when assistants are not available during reduction. 14 A stockinette is placed on the involved extremity up to the hip so it does not slip. The stockinette is then hung via trapeze or IV pole over the patient’s contralateral shoulder, inverting the foot and reducing the facture-dislocation. Postreduction radiographs are obtained holding this position and then immobilization is applied.
When assistance is available, the preferred method is a counter pressure technique. An assistant flexes the knee and provides proximal counter pressure and stabilization at the proximal tibia to aid the physician reducing the fracture-dislocation at the level of the ankle. This position also decreases tension on the Achilles tendon allowing for easier reduction.2,5 The physician performing the reduction places one hand on the posterior heel, cupping the heel. The other hand grasps the lateral forefoot with digits 2 to 5 on the dorsal foot and the thumb on the plantar foot with the foot in a slight plantar flexed position. The direction of reduction is based on the dislocation and fracture pattern.1,3,5,20 The technique and hand placement for reduction does not differ based on fracture type, only the direction of reduction. The standard method is to increase the deformity, then distract in the opposite direction.
For the most common fracture pattern seen in our series, SER IV, the counter pressure method has been described in extensive detail by D’Angelantonio et al 6 in 2009. The authors described a 3-phase protocol consisting of limb stabilization, fracture reduction, and immobilization. The authors concluded that although closed reduction is not appropriate for all ankle fractures, the procedure can be used as a singular treatment in some cases but is most often used as an initial procedure prior to surgical management.
An inability to reduce an ankle fracture-dislocation into adequate alignment, talus under the tibia, may be encountered secondary to a number of causative factors.1,20-25 Potential causes include an associated large posterior malleolus fragment, interposition of soft tissue structures, fixed displacement of the fibula behind the tibia, and inadequate immobilization. When inadequate reduction is obtained, a subsequent reduction attempt is performed. Several failed reduction attempts necessitates open surgical reduction.
Ankle fracture-dislocation encountered with a large posterior malleolar fragment may impede the ability to reduce the talus under the tibia. 5 In this instance, the physician performing closed reduction will take the thumb of the hand cupping the posterior heel and place it underneath the posterior malleolus fragment on the medial ankle region. During reduction, the physician pushes upward on this posterior malleolus fragment while reducing the dislocation to allow the talus to reduce under the tibia (Figure 4).
(A) Anteroposterior and lateral prereduction radiographs of a 59-year-old female patient who sustained a right ankle fracture-dislocation. (B) Lateral initial postreduction radiograph after closed reduction using a plaster AO splint, which reveals inadequate reduction of the talus under the tibia secondary to a large posterior malleolar fragment blocking reduction. (C) Lateral second postreduction radiographs after closed reduction with manipulation of the large posterior fragment during closed reduction and subsequent use of a bivalved fiberglass cast, which reveals adequate reduction of the posterior malleolar fragment and the talus under the tibia.
Cases of interposition of soft tissue structures are uncommon but often reported causes of inability to reduce an ankle fracture-dislocation.1,20-24 Medial soft tissue structures are the most frequently reported subset of structures that inhibit the reduction of an ankle fracture- dislocation.1,21 This is most often seen in pronation/eversion injuries where entrapment of the posterior tibial tendon into the tibiotalar joint has been identified as a cause of preventing reduction.1,20-24 Entrapment of the posterior tibial tendon within the tibiofibular interosseous space has also been reported as a cause of inadequate reduction. 21
Other less common causes for irreducible ankle fracture-dislocation include osseous impingement, osseous fragments, foreign bodies, and ruptured ligament interposition. Fixed displacement of the fibula behind the tibia was first reported by Bosworth 26 in 1947 as an osseous impingement that creases an inability to reduce an ankle fracture-dislocation. Closed reduction attempts when this injury pattern is encountered, classically referred to as a Bosworth fracture, are usually unsuccessful, and open surgical reduction is necessary.1,20,25
In reviewing our case series, ankle dislocations most often occurred with an associated ankle fracture (39/40). The majority of the ankle fracture-dislocations were classified as an SER IV fracture pattern (35/40). The most prevalent cause of an inability to maintain an ankle fracture-dislocation in adequate alignment was secondary to inadequate immobilization. The use of a postreduction bivalved fiberglass cast was noted to be superior in maintaining reduction versus a below-the-knee combination plaster splint. There is scattered anecdotal evidence favoring bivalved cast immobilization versus splint immobilization after closed reduction of an ankle fracture- dislocation, as splint immobilization provided inadequate stabilization.1,5,27,28 To our knowledge, our case series is the first to provide statistical evidence favoring a below-the-knee bivalved cast immobilization over below-the-knee combination plaster splint immobilization after closed reduction of ankle fracture-dislocation.
Our study did have limitations. All the patients in the case series presented to a community-based hospital emergency room. All these injuries were low-energy rotational “slip and fall” or sports-related injuries. High-velocity trauma cases are absent from the series as the patient’s were not seen in a trauma center. This is reflected in the low number of open ankle fracture-dislocations reported in our series and the overall majority of cases classified as an SER IV variant. However, this does correlate with the findings of Still and Atwood 29 in their retrospective analysis of 41 ankle fractures, where SER IV was the most common grade of injury.
Of interesting note, Ashworth and Patel 30 in 1998 reported a case of compartment syndrome following ankle fracture-dislocation. Twelve hours after closed reduction of bimalleolar ankle dislocation immobilized in a bivalved cast, their patient had increased pain that was nonresponsive to analgesia and altered sensation to the bottom of the foot. The patient underwent emergency fasciotomy for deep posterior compartment syndrome 1 hour after the onset of his symptoms. They indicated that compartment syndrome associated with an ankle fracture is a very rare occurrence.
In conclusion, when reduction of ankle fracture-dislocations are approached in a stepwise manner and with the use of a below-the-knee bivalved cast, the number of reduction attempts and complications are decreased. By following a stepwise approach as seen in our algorithm for the initial management of ankle fracture-dislocations, patient care in these injuries is improved.