
Abstract
Extraskeletal osteochondromas are benign, slow growing, and often painless neoplasms. Although they are histologically similar to conventional osteochondromas, extraskeletal osteochondromas are not attached to a parent bone. When a well-defined osseous mass in the soft tissue without any direct continuity with the adjacent bone or joint is encountered, a diagnosis of extraskeletal osteochondroma should be strongly considered. It should be identified to avoid unnecessary aggressive surgical treatment. We present a patient with symptomatic extraskeletal osteochondroma of the medial arch of the foot. It was treated by local excision and no evidence of local recurrence clinically or radiographically after 51 months of follow-up.
“Osteochondral neoplasms of soft tissue are uncommon and usually arise from synovial tissue in joints, tendon sheaths, or bursae.”
Introduction
Osteochondromas are common and typically arise from the metaphyseal ends of long bones but have been found in virtually every bone in the body. They demonstrate mature bone with a cartilaginous cap and continuation of the medullary cavity with that of the long bone. Osteochondral neoplasms of soft tissue are uncommon and usually arise from synovial tissue in joints, tendon sheaths, or bursae. Rarely, extraskeletal osteochondromas with extensive ossification arise outside synovial compartments. 1 They should be distinguished from conventional osteochondromas. Although they are histologically similar, extraskeletal osteochondromas are not attached to a parent bone. 7 There are only a few case reports about the occurrence of these tumors in the foot.1-8 Here, we report a case of extraskeletal osteochondroma of the medial arch of the foot.
Case Report
A 16-year-old male noticed a mass over his left foot for 10 years. There was no preceding injury. The mass increased in size in recent 3 years before he sought medical advice. There was pain over the mass on palpation and no rest pain was experienced.
Clinically, there was a 4- to 5-cm bony hard mass in the medial arch of his left foot (Figure 1). Radiographs of his left foot showed calcified mass at the medial arch close to the navicular (Figure 2). Computed tomogram showed a 3.7 × 3.6 × 4.0 cm calcified lesion (Figure 3). Magnetic resonance imaging showed a soft tissue mass within the left abductor hallucis muscle with no definite invasion to the surrounding structure. There were foci of ossification within the mass (Figure 4). A bony mass of size of 4 × 3 × 2.5 cm with a shiny white cartilaginous surface at one edge (Figure 5) was excised in November 2007. The mass was within the abductor hallucis muscle and the posterior tibial tendon was spared. Histological examination showed a cartilaginous cap covering cancellous bone. The chondro-osseous junction showed growth plate columns with gradual transition. The bony trabeculae had mixed woven and trabecular patterns, with more remodeling activity at the periphery. It was consistent with an osteochondroma. On 51 months of follow-up, there was no evidence of local recurrence clinically or radiographically.
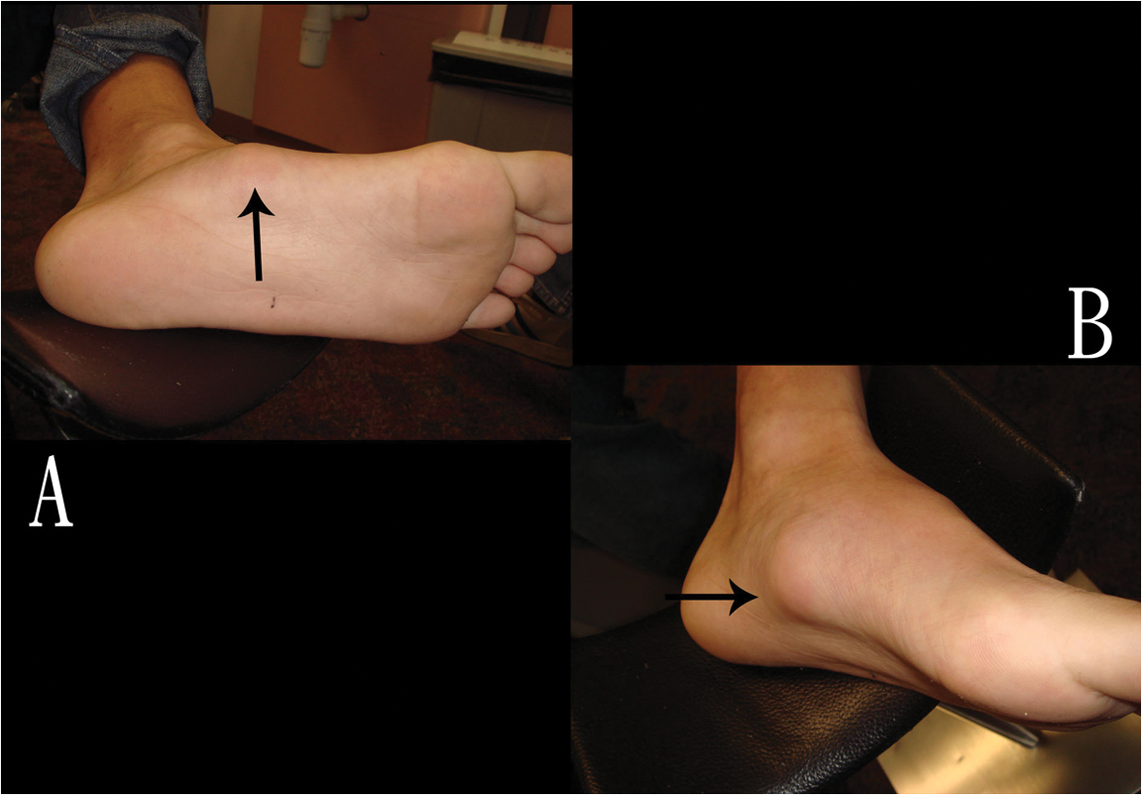
(A, B) Clinical photos of the patient’s left foot with the arrow pointing to the mass.
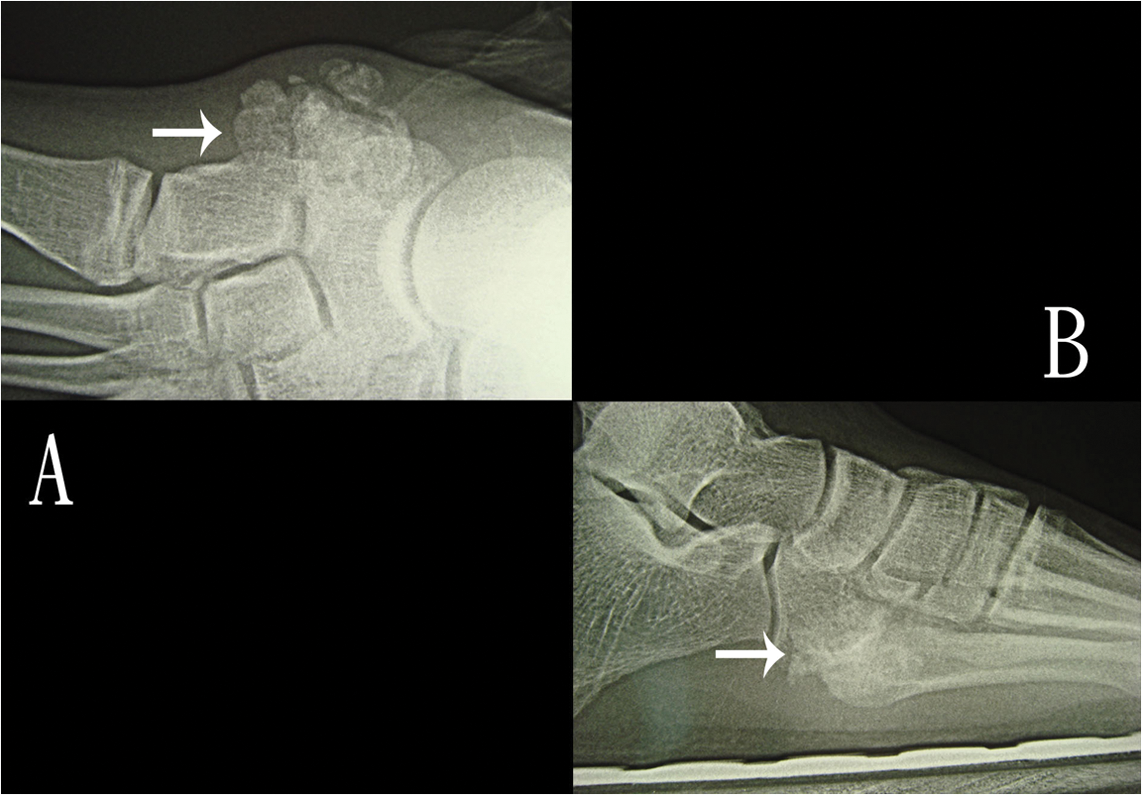
Dorsoplantar (A) and lateral (B) views of the foot with the arrow pointing to the mass.
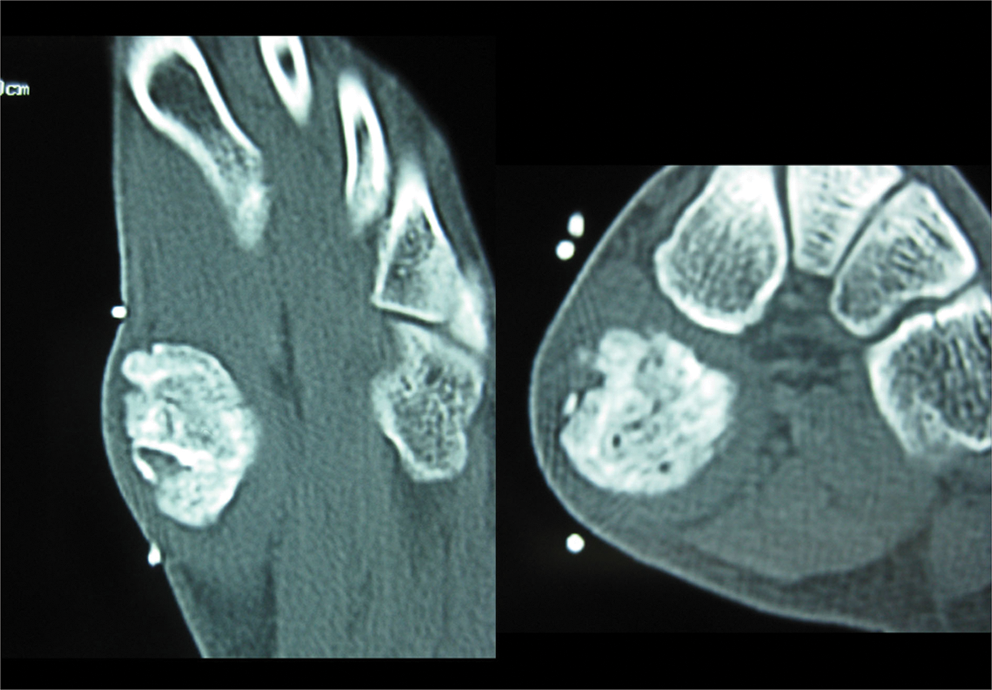
Computed tomogram of the patient’s left foot showing a dense calcified, well-demarcated mass.
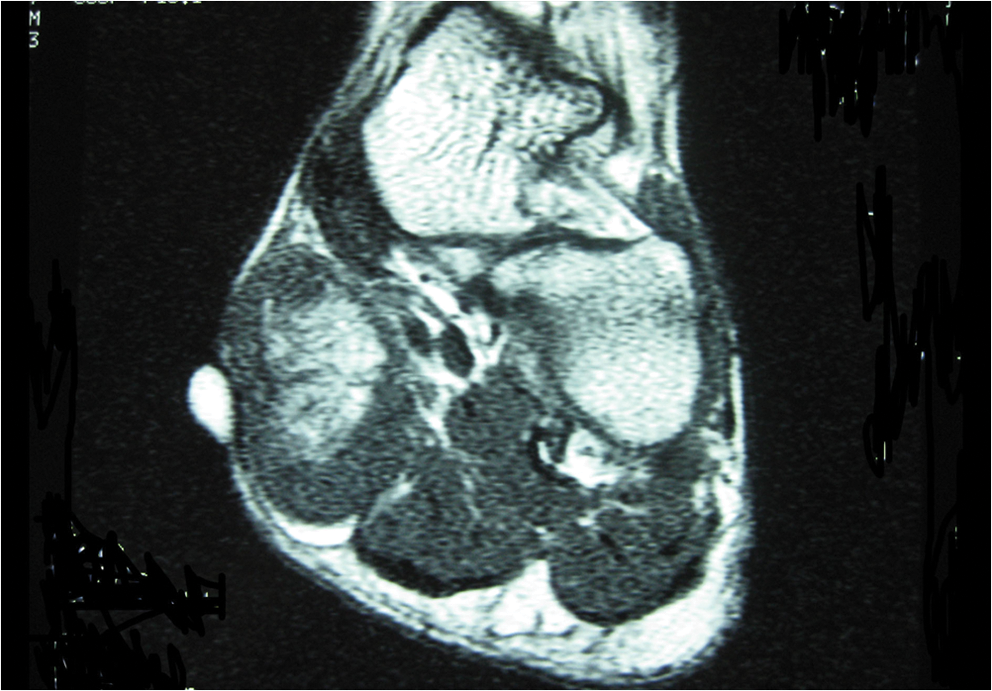
Magnetic resonance imaging showed a soft tissue mass within the left abductor hallucis muscle with no definite invasion to the surrounding structure. There were foci of ossification within the mass.
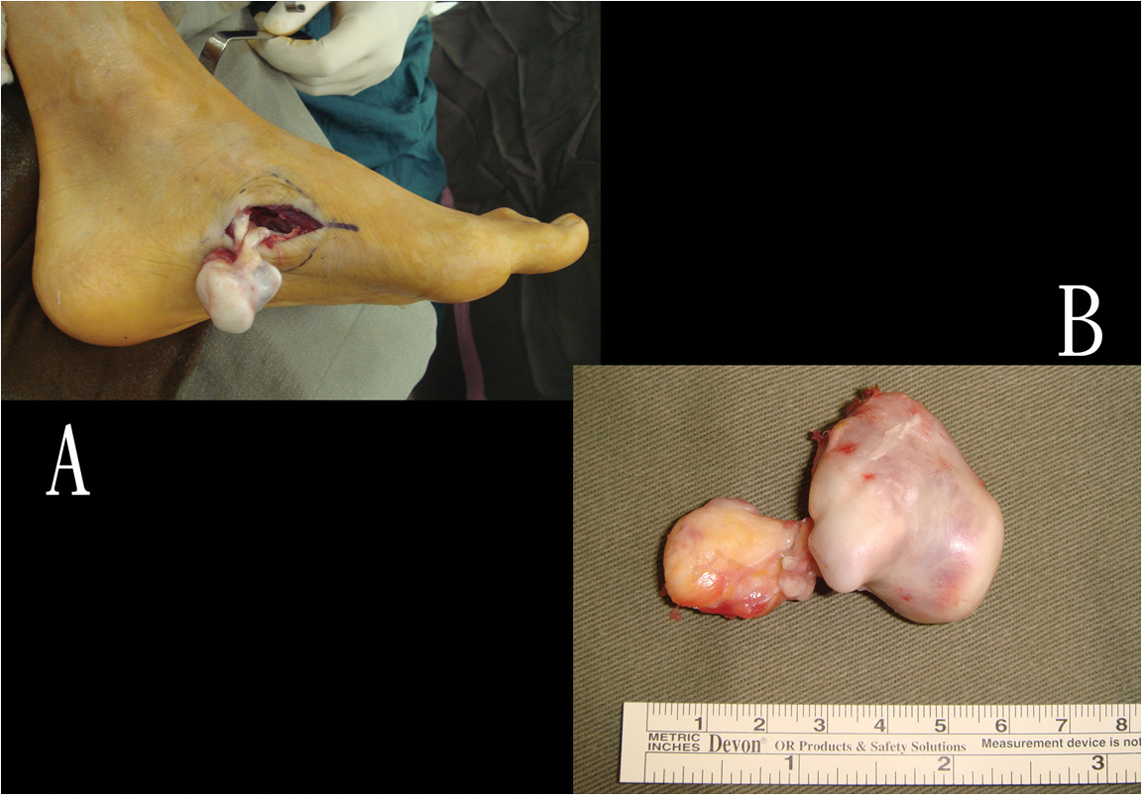
(A, B) The mass was enucleated.
Discussion
Extraskeletal osteochondromas typically grow slowly and may scallop underlying bone, but rarely cause pain. 1 Nearly all these lesions were small, rarely exceeding 2 cm in diameter.1,2 The size of the mass in our case may be because of its location, which is not the weight-bearing part of the sole and the mass can grow to a bigger size before it becomes symptomatic. Although most of these lesions are asymptomatic, they may become secondarily symptomatic because of associated neuritis, irritation from shoe gear, callus formation, or decreased range of motion when adjacent to a joint. Trauma is not typically related to the occurrence of these lesions. However, a fractured extraskeletal osteochondroma may result in pain.1,2 Moreover, associated stress fracture of adjacent bones 4 and arthritis of adjacent joints 2 have been reported as a source of pain. In contrast to our case, they have been mostly reported in adults between the fourth and sixth decades of life rather than in adolescents without antecedent trauma. A sex predilection is yet to be identified. 2 Approximately 70% of them were found in the upper extremity, with the majority found in the fingers; 25% of lesions involved the lower extremity, with the majority found in the foot.1,2
Extraskeletal osteochondroma of the plantar medial arch has been reported by Spencer and Blitz. 2 The patient complained of arch pain, which was attributed to the secondary degenerative joint disease in the base of the third and fourth metatarsals, which may have been attributable to the altered pressure of the mass with weight bearing. There was no evidence of any secondary degenerative joint disease in our patient. The pain experienced by our patient was attributed to the easy contusion of the mass because of its size.
The radiographic findings of extraskeletal osteochondromas typically consist of well-circumscribed, lobulated masses at the extraskeletal location with dense, central calcifications or areas of ossification on computed tomography.1,2 Bony changes are infrequent, but occasionally, cortical sclerosis, and even cortical erosions have been described. Occasionally, signs of degenerative joint disease adjacent to the lesion can be demonstrated by computed tomography. Magnetic resonance imaging can further define the margins of the mass, in conjunction with determining the intramedullary and extraosseous extent of the mass. Magnetic resonance imaging shows a well-demarcated heterogenous lesion that has low signal mostly on T1-weighted images and mixed high and low in T2-weighted images. Areas of mature ossification have intermediate T2 signal intensity except for densely calcified areas, which again have low signal intensity. 7 In addition, magnetic resonance imaging was shown to determine the size of the unossified cartilage cap, which can help to rule out a sarcoma. A cartilage cap generally demonstrates low-to-intermediate signal intensities on T1-weighted images, and high signal intensities on T2-weighted images. 2
The gross appearance of an extraskeletal osteochondroma is a well-encapsulated mass, firm to palpation and often attached to a tendon or its sheath. 6 The histologic characteristics are defined as a single mass that is peripherally encased with mature hyaline cartilage, with an osseous center, organized in a manner similar to that of a conventional osteochondroma and the lesion cannot be intra-articular. 2 At the core are areas of prominent endochondral ossification, along with areas of lamellar and trabecular bone. The thickness of the cartilage rim varies, and was reported to be as thin as 0.2 cm and as thick as 1.2 cm. Cellular atypia is somewhat common in the cartilage cap, and should not be mistaken for a more aggressive process or malignancy, for example, chondrosarcomas.2,6
The differential diagnosis of an extraskeletal osteochondroma includes those pathologies with discrete mass containing mature ossification. It includes conventional osteochondroma, osseous lipoma, synovial chondromatosis, myositis ossificans, extraskeletal chondroma, periosteal chondroma, periosteal chondrosarcoma, synovial sarcoma, chondrosarcoma, and nonmalignant entities, including tumoral calcinosis, pseudomalignant osseous tumor, and ossifying fibromyxoid tumor of soft parts. It is important to keep in mind that although mature ossification is generally associated with a benign etiology, malignancy should be included in the differentials. Sarcomas such as synovial sarcoma as well as primary soft tissue chondrosarcoma and osteosarcoma may contain dense calcification, which can resemble bone formation; however, in these entities the zonal phenomenon is typically absent. The diagnosis of extraskeletal osteochondroma should be considered when a mass with mature ossification and typical chondroid matrix is seen in the distal extremities.1,2,5,7 Although cellular atypia is somewhat common in the cartilage cap, extraskeletal osteochondromas are well encapsulated and are not reported to undergo malignant transformation. It is therefore important to correlate the histologic findings, clinical scenario, and radiographic findings. 2
The pathogenesis of soft tissue osteochondromas remains unclear. The following mechanisms2,4,5,7 have been suggested:
cells near the surface of bone that are capable of producing cartilage migrate and become fastened to the connective tissue;
precartilagenous tissue persisting in the tendon just above the joint of its insertion converts to active phase;
metaplasia of pleuripotent cell line derived from the joint synovium, tenosynovium, and connective tissue occurs because of stimulation by unknown factors;
hamartomatous pathogenesis;
the result of displaced physeal chondrocytes into adjacent soft tissue, which ultimately develop new endochondral bone growth;
Adipose tissue metaplasia was also suggested as a cause, attributable to the metamorphosis from a lipoma into an extraskeletal osteochondroma;
metaplastic transformation of mesenchymal cells as a result of repeated trauma, as the lesion is found in the plantar, weight-bearing regions in most reported cases of soft tissue osteochondroma of the foot; and
as a variant of extraskeletal chondromas that undergo extensive enchondral ossification to form an extraskeletal osteochondroma.
The behavior of extraskeletal osteochondroma is poorly characterized but limited data suggests that they have a benign fashion and local recurrence is rare.2,4,6,7 There have been no report of malignant changes or metastasis. Although conservative treatment has been suggested unless the lesions cause pain, limit range of motion, or demonstrate signs of malignancy, 2 most of the authors recommended surgical excision of the mass4,7 as it is curative. Frequently, the mass can be easily enucleated 3 and early recognition of this entity by clinical and radiological evaluation will help avoid unnecessary extensive surgery. 4 The indications of the surgical excision of the mass in this case were the presence of local pain and preventing the occurrence of arthrosis in any articulating or adjacent joints. 2
In summary, extraskeletal osteochondromas are benign, slow-growing, and often painless neoplasms. When a well-defined osseous mass in the soft tissue without any direct continuity with the adjacent bone or joint is encountered, this diagnosis should be strongly considered. It should be identified to avoid unnecessary aggressive surgical treatment. 2