
Abstract
Keywords
“The surgical principles are to debride areas of symptomatic tendinosis and intratendinous calcification, promote tendon healing, and correct exacerbating mechanical factors.”
Introduction
Insertional Achilles tendinopathy is a clinical diagnosis comprising the spectrum of acute and chronic pathology involving the Achilles tendon insertion and its surrounding tissues. This condition is a frequent source of pain and cause of presentation to foot and ankle surgeons. Waldecker et al 1 reported a 4% incidence rate of insertional Achilles tendinopathy within a nonathletic population. Kvist 2 retrospectively reviewed 3336 competitive and recreational athletes, with 14% of participants presenting with Achilles tendon issues. He reported that 66% had paratendonitis, and 23% had either retrocalcaneal bursitis or insertional tendinopathy. Surgery was performed in 24% of patients with paratendonitis and insertional disease.
Nonsurgical treatment has mixed results reported within the literature, and surgical intervention is frequently required.3,4 The surgical principles are to debride areas of symptomatic tendinosis and intratendinous calcification, promote tendon healing, and correct exacerbating mechanical factors. 5 Inflamed bursae and areas of prominent bone must also be removed. The surgical technique and extent of tendon detachment are areas of debate. The purpose of this article is to review the surgical outcomes of patients who underwent the use of the suture bridge technique as part of the overall management of insertional Achilles tendinopathy.
Materials and Methods
After institutional review board approval, medical records from 2006 to 2012 were reviewed. A total of 35 patients who underwent surgical management using the suture bridge technique for the treatment of insertional Achilles tendinopathy were identified. All patients in the study presented with posterior heel pain that had failed 3 to 6 months of nonoperative management. All patients had radiographic evidence of an enthesopathy at the Achilles insertion with a prominent posterior calcaneal tuberosity. Patients were included in the study if they were 18 years or older and underwent surgical correction of insertional Achilles tendinopathy and calcaneal exostectomy with the use of the Arthrex Achilles SutureBridge (Arthrex Inc, Naples, FL) to reattach the Achilles tendon with a minimum follow-up of 6 months. Exclusion criteria were incomplete medical records, use of an alternative surgical technique or implant for insertional Achilles tendinopathy, and failure to follow up with the senior author for greater than 6 months. Clinical outcomes were assessed by preoperative and postoperative American Orthopaedic Foot and Ankle Society (AOFAS) hindfoot outcome instruments as well as a subjective postoperative satisfaction questionnaire consisting of 3 questions obtained via a telephone interview. Patients included in this study were evaluated and treated preoperatively, intraoperatively, and postoperatively by the senior author (PRB). Additional information collected from the medical records included data on gender, age, surgical site, postoperative course, and complications. Statistical analysis was performed by the lead author using the Student t test for evaluation of statistical significance (P < .05).
Surgical Technique and Postoperative Course
Each patient was placed in a prone position and a thigh tourniquet was used to maintain hemostasis; all patients received preoperative antibiotics in accordance with Surgical Care Improvement Project guidelines. Following standard prepping and draping, a posterior midline incision was made. The incision was then carried down to the paratenon while maintaining full thickness skin flaps. The paratenon was then incised for later repair. The Achilles tendon was then detached transversely from its insertion, exposing the entire retrocalcaneal exostosis (Figure 1). The degenerative and calcified portions of the Achilles tendon were carefully excised. The exostosis was removed with an oscillating saw or osteotome, and all edges were smoothed with a hand rasp (Figure 2). All calcifications protruding off the calcaneus and within the Achilles tendon were removed, and this was confirmed with an intraoperative fluoroscopic image. The tendon was then tensioned appropriately and reattached to the newly created bleeding cancellous surface of the calcaneus using the Achilles Suture Bridge (Arthrex Inc, Naples, FL) anchor system (Figure 3). The paratenon was closed with 4-0 Monocryl using a locked running stitch, and the skin reapproximated with 3-0 nylon. The patients were immobilized in a non-weight-bearing Jones compressive dressing in gravity equinus for 1 week. At their first postoperative visit, reliable patients were placed in a CAM boot with an Achilles wedge system and those patients deemed unreliable were placed in a cast with the foot in a relaxed position, with all patients being instructed to remain non–weight bearing. All patients remained non–weight bearing until their 3-week follow-up visit, at which time sutures were removed, and they were then allowed to weight bear as tolerated with the use of a CAM boot and Achilles wedge system. Patients were instructed to remove one 5° wedge each week starting from 15° of plantarflexion, until they were able to ambulate at a neutral position in the boot. Patients were then transitioned back into regular shoe gear as tolerated. If necessary, physical therapy was initiated on a case-by-case basis.

Complete Detachment of the Achilles Tendon Exposing Large Calcaneal Exostosis.

Postresection and Debridement of Calcaneus.
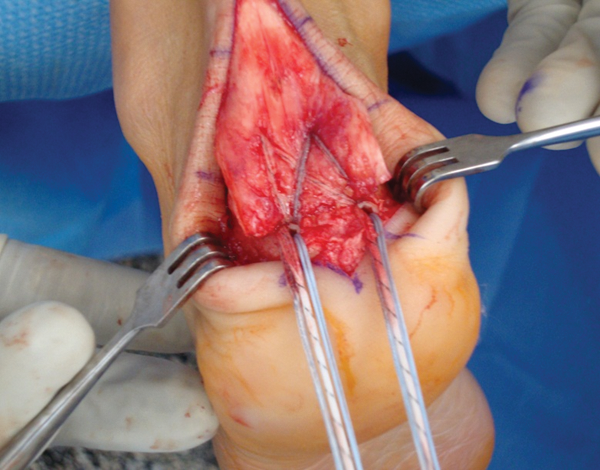
Suture Bridge Construct.
Results
A total of 30 patients met the inclusion criteria: 10 men and 20 women, with an average age of 49.1 ± 9.2 years. Follow-up ranged from 7 months to 65 months, with a mean follow-up of 28.9 ± 16.9 months (Table 1). Preoperative and postoperative AOFAS hindfoot scores were found to be 56.6 ± 14.0 and 91.7 ± 10.4, respectively. This increase was found to be statistically significant (P < .0001; Table 2).
Patient Demographics and Follow-up
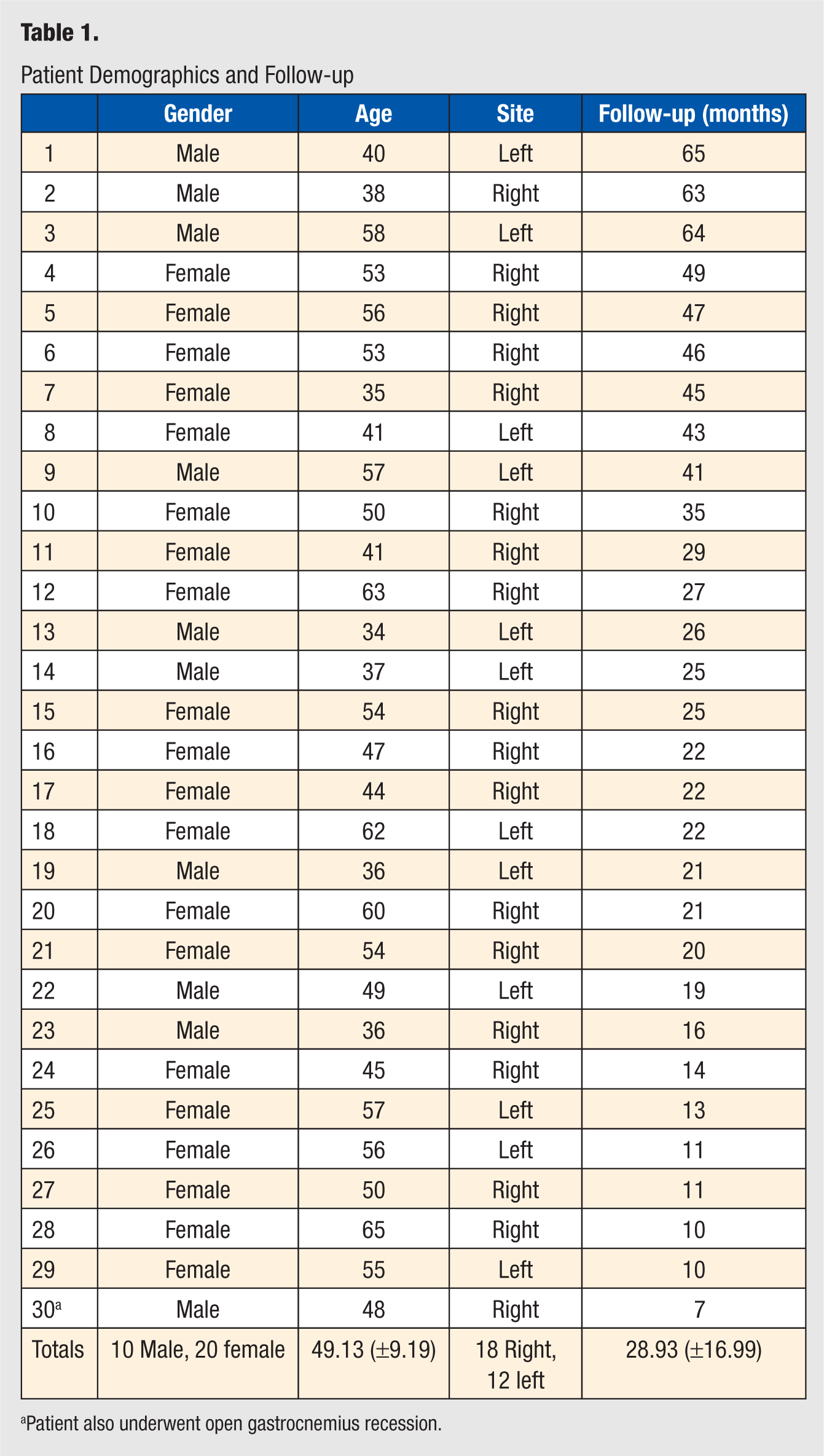
Patient also underwent open gastrocnemius recession.
Preoperative and Postoperative AOFAS Hindfoot Scores
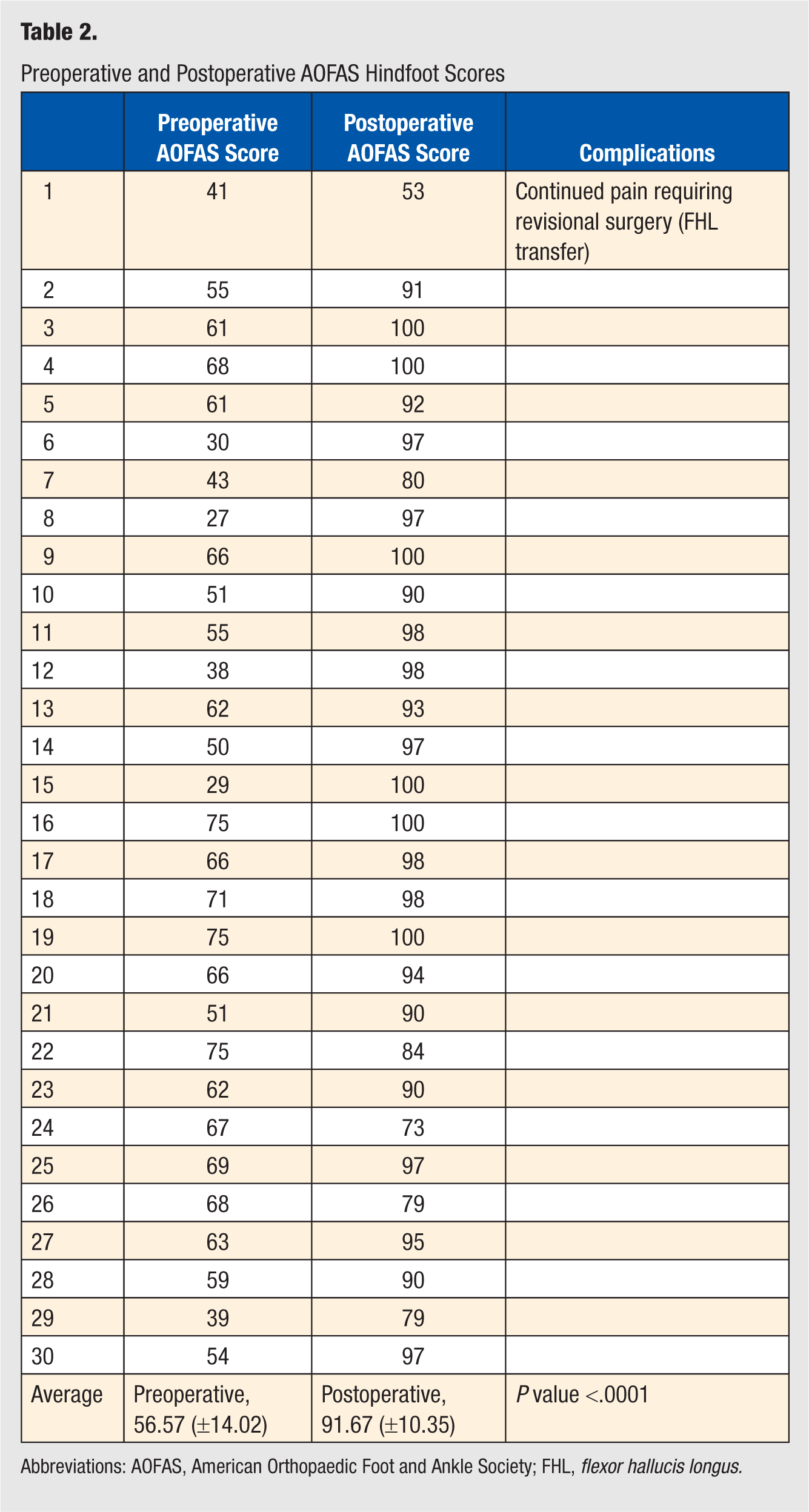
Abbreviations: AOFAS, American Orthopaedic Foot and Ankle Society; FHL, flexor hallucis longus.
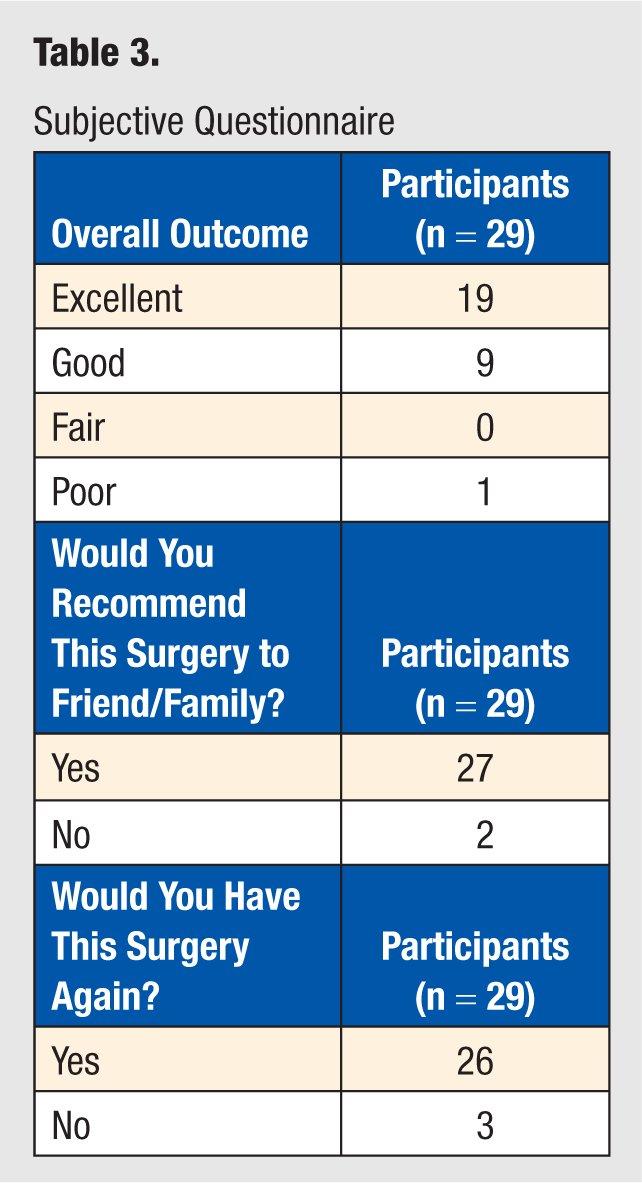
Of 30 patients, 29 were able to be reached by telephone to complete a subjective questionnaire used to assess satisfaction (Table 3). This questionnaire revealed that 19 patients had an excellent outcome, 9 patients had a good outcome, and 1 patient had a poor outcome. This same patient who was unsatisfied with the surgical procedure was having continued pain that required a second surgical procedure, a flexor hallucis longus tendon transfer, performed by a different surgeon. This patient reported ongoing pain with an inability to return to work, dependence on walking aids and bracing, continued need for pain medications, and a generalized decrease in activity level. No patient developed postoperative wound complications, including wound dehiscence or hypertrophic scarring. One patient required an open gastrocnemius recession at the time of his index procedure. Postdebridement, his Achilles tendon was found to be short, and intraoperatively, it was deemed necessary to maintain adequate ankle joint range of motion.
Subjective Questionnaire
Discussion
The true pathogenesis of Achilles tendinopathy remains unknown. Lyman et al 6 investigated the distribution of tensile strain at the insertion of the Achilles tendon during functional range of motion. They hypothesized that the location of highest strain would be anterior, but their cadaveric biomechanical study showed increasing strain in the posterior portion of the tendon. The authors described a stress-shielding effect within the tendon anteriorly. Other biomechanical literature supports the finding that the site affected with tendinopathy is generally located at the site of “stress shielding.” 7 Rufai et al reported the tendency for cartilage-like changes to develop within the tendon on the stress-shielded side of the enthesis, leading to intratendinous bone formation through endochondral ossification. 8 Benjamin et al 9 found that calcification and spur formation at the insertion are not dependent on inflammation or preceding micro tears of the Achilles. They felt that the spur formation was an adaptive process, which increases the surface area at the bone-tendon junction to protect this attachment in the face of increased mechanical loads. 9
Unfortunately, nonoperative treatment of Achilles tendinopathy has mixed results within the literature. The success rates vary from 53% in one study 3 to 89% in another. 4 Overall, the success of nonoperative treatment is most likely dependent on the severity of the tendinopathy, 3 and often times, success is limited because of the multifactorial nature of the pathology. Both the disease process and mechanical irritation from shoe gear can lead to recurrence and failure of conservative treatment. Nonoperative treatment modalities include activity and shoe gear modification, nonsteroidal anti-inflammatory medications, heel lifts, orthotics, cast or boot immobilization, extracorporeal shockwave therapy, and physical therapy. If symptoms persist after 3 to 6 months of conservative therapy, surgical treatment is advised. 10
Many surgical procedures exist for the treatment of insertional Achilles tendinopathy; however, all have common goals: excision of the inflamed retrocalcaneal bursa, thorough debridement of the degenerative and calcified tendon, and removal of the calcaneal exostosis. Kolodziej et al 11 performed a biomechanical study in which cadaveric Achilles tendons were loaded to failure after detaching sequential amounts of the Achilles tendon. They found that one could detach up to 50% of the Achilles without fear of rupture. Calder and Saxby 12 evaluated the clinical outcomes of insertional Achilles tendon surgery and concluded that early weight bearing is safe if less than 50% of the tendon is detached. These findings have led some authors to not recommend completely detaching the tendon. 13 However, McGarvey et al 14 found that 95% of their surgical patients had central calcifications requiring a more extensive debridement. They concluded that limiting resection of the diseased tissue to 50%, for fear of rupture, leads to inadequate debridement and thus failure of surgical treatment. They were also the first to describe the central longitudinal approach to debride the calcified tendon. 14 This technique was further investigated by Nunley and colleagues 15 in 2011. In their study, they utilized a central incision and detached up to 70% of the tendon while maintaining the medial and lateral insertion sites of the Achilles tendon. They concluded that this technique affords the surgeon the ability to treat all areas of the pathology with good long-term success in regard to motion, strength, and overall function while preventing nerve and vascular injury and minimizing wound complications.
Complete detachment of the Achilles tendon has been advocated by several authors.16,17 Wagner compared no or partial detachment (removing less than 50% of the tendon) with complete detachment of the Achilles tendon and concluded that complete detachment allowed for a more adequate debridement and easier removal of the calcaneal exostosis. It should be noted that in their study, they had 2 revisions in the partial detachment group—1 for continued pain secondary to incomplete debridement and the other for an Achilles rupture—whereas the complete detachment group did not require any revisional surgery. 17
It is the opinion of the authors that in order to adequately treat the entirety of the pathology associated with Achilles tendinopathy, the Achilles tendon must be completely detached, leaving the surgeon with the dilemma of reattachment. To our knowledge, our study of 30 patients and 30 surgeries presents the largest patient population in the literature with the longest follow-up to date for the suture bridge technique. The postoperative AOFAS scores as well as the subjective questionnaire support the suture bridge technique as a reproducible surgical procedure, which provides good to excellent patient satisfaction. Our average preoperative and postoperative AOFAS scores of 57 and 92, respectively, showed a statistically significant increase and are similar to the results of other authors. 15 Furthermore, our series demonstrates that removing the entire Achilles tendon and reattaching it with a Suture Bridge construct did not lead to any postoperative Achilles tendon ruptures.
Our study also illustrates the safety of the central posterior incision for Achilles tendon pathology because no wound healing complications developed in our series. This incision placement takes advantage of the fact that it lies centrally along the peroneal angiosome and the posterior tibial angiosome while being medial to the sural nerve.18,19 Highlander and Greenhagen 20 performed a systematic review of the use of posterior leg incisions and found no greater incidence of wound healing complications compared with posterior-medial incisions. 20 The advantage of the posterior incision is the excellent visualization for resection and reattachment of the tendon.
Currently, only case reports regarding the suture bridge technique have been published in the medical literature.21,22 Witt and Hyer 22 reported on 4 cases with successful treatment of Achilles tendinosis where the Arthrex suture bridge was used. The advantages of this technique are that it provides adequate visualization and debridement without the loss of early mobility 21 while providing a large “footprint” or contact area between tendon and bone, thus increasing friction and overall strength of the surgical construct. 23 The large footprint also increases the total surface area of tendon-to-bone contact, theoretically increasing the speed of incorporation. The strength of the suture bridge construct for Achilles pathology has been reported in the treatment of bone affected by Charcot neuroarthropathy, 21 a condition with known poor bone mineral density. 24
Although limited data exist on the use of double row anchor or transosseous fixation techniques for the treatment of insertional Achilles tendinopathy, there are multiple studies investigating its use in shoulder surgery. In their systematic review of double-row versus single- row rotator cuff repairs, Trappey and Gartsman 25 found that the majority of basic science data suggest that double-row repairs have a greater footprint, improved contact area and pressure, better initial fixation strength, and a higher load to failure when compared with single-row repairs. Although many studies have shown the biomechanical superiority of the double-row construct, this has not always been the case in terms of clinical superiority. Franceschi et al 26 enrolled 60 participants who were randomized into double-row versus single-row repair and found no statistical difference in the postoperative functional assessment at a 2-year follow-up. However, this is in contrast to Gartsman et al, 27 who, in their prospective randomized trial comparing a single-row repair to a transosseous equivalent technique (Suture Bridge technique), found a statistically significant difference when rerupture rates were evaluated with ultrasound.
Conclusion
The central incision with complete detachment and reattachment of the Achilles tendon with the suture bridge technique for the treatment of insertional Achilles tendinopathy allows the surgeon adequate visualization to treat all areas of the pathology with minimal risk of nerve injury or wound complications. The suture bridge technique provides an excellent bone-to-tendon healing interface with adequate fixation as demonstrated by the fact that there were no postoperative Achilles tendon ruptures. The technique also provides good to excellent clinical results in 97% of cases at intermediate and long-term follow-ups.