
Abstract
Hallux rigidus is a term describing degenerative joint disease (DJD) to the first metatarsal phalangeal joint (MTPJ). It is the most common DJD encountered in the foot and is the second most common pathology of the great toe behind hallux valgus. The goal of a cheilectomy is to relieve pain and increase MTPJ motion. Critical evaluation of the cheilectomy must include longevity of desired results. The primary goal of this study was to determine how long a cheilectomy can be expected to last before an arthrodesis or joint destructive procedure is performed, if ever. We examined 189 cheilectomies with a mean radiographic follow-up of 235 days and mean chart review follow-up of 1184 days (3.2 years). Analysis showed 5 repeat cheilectomies, 1 interpositional arthroplasty, and only 2 arthrodeses subsequently performed. This retrospective study provides intermediate term evidence that cheilectomy is an appropriate procedure for stages 1, 2, and 3 first MTPJ DJD with reliable, lasting results.
Keywords
“Regardless of the amount of bone resected, the goal is to relieve pain and increase MTPJ [metatarsal phalangeal joint] motion, while debulking the area.”
Introduction
Hallux rigidus is a term describing degenerative joint disease (DJD) to the first metatarsal phalangeal joint (MTPJ). It is the most common DJD encountered in the foot and is the second most common pathology of the great toe behind hallux valgus. 1 Patients commonly complain of pain, stiffness, and shoe gear irritation with this form of arthritis. Conservative treatment includes immobilizing the area, restricting activity, and injections. Failure of conservative efforts leaves many surgical options ranging from cheilectomy to arthrodesis.
A cheilectomy simply refers to removal of exuberant, degenerative bone formation surrounding the joint. 2 The amount of bone resected is debatable. Some authors remove only osteophytes and loose bodies, others recommend resection in-line with the metatarsal shaft, and yet others recommend removal of a larger section of the metatarsal head. Regardless of the amount of bone resected, the goal is to relieve pain and increase MTPJ motion, while debulking the area.
Critical evaluation of the cheilectomy must include longevity of desired results. Much of the literature surrounding a cheilectomy offers only short-term outcomes, mostly of 1 year or less.3-6
Many consider cheilectomy only appropriate in early DJD of the first MTP.4,5,7,8 Others recommend cheilectomy for early and advanced DJD.3,9-13 Preoperative first MTP staging using the Coughlin scale (Table 1) is common to aid in determining the stage of degeneration and is useful in selecting a surgical procedure. 11
Coughlin and Shurnas Clinical Radiographic System a for Grading Hallux Rigidus
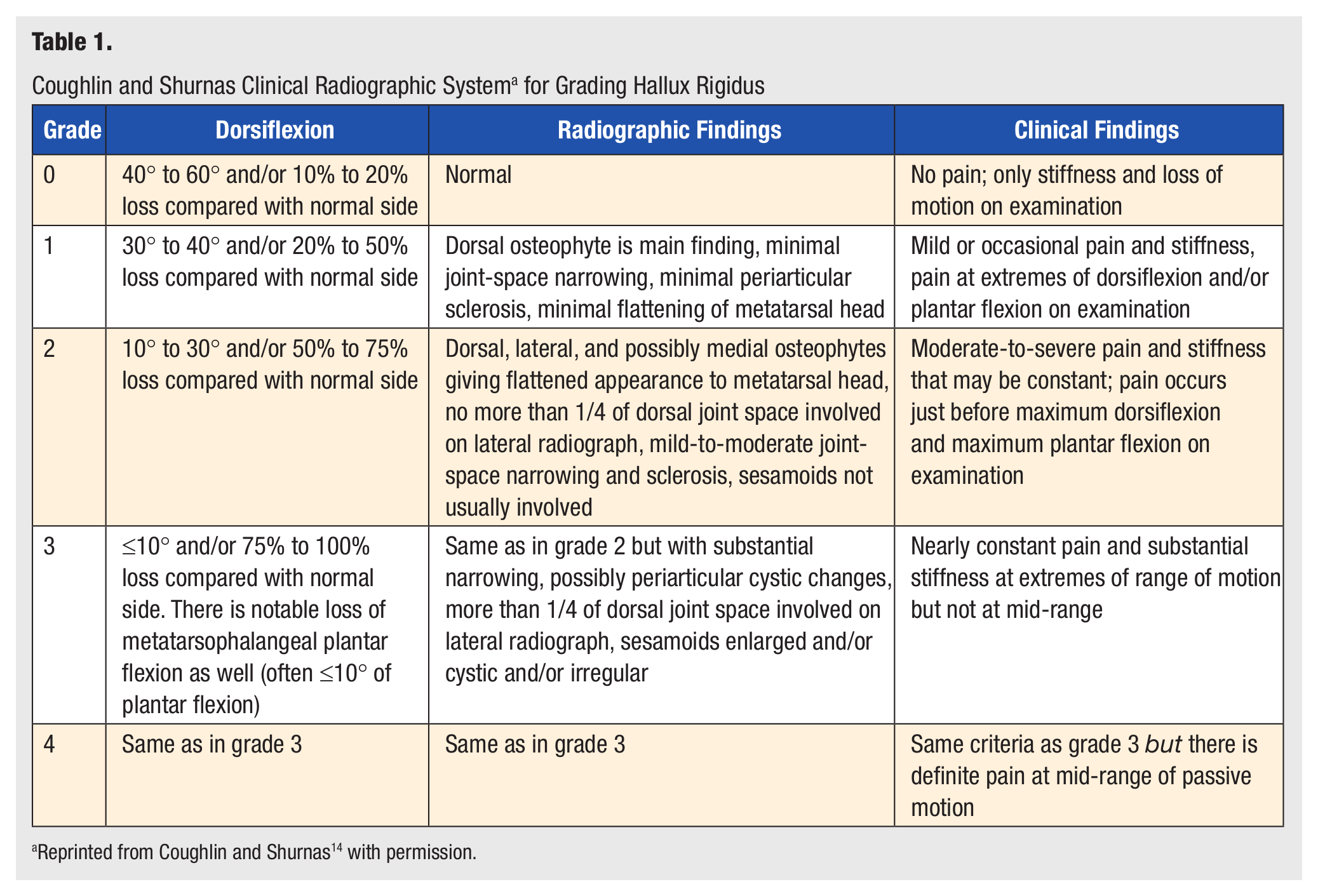
Reprinted from Coughlin and Shurnas 14 with permission.
The purpose of this study was twofold: First, to determine the longevity of success from joint cheilectomy with failure defined as a first MTPJ destructive procedure and second, to determine if staging predicts failure with cheilectomy.
Methods
Approval from the institutional review board at our facility was obtained. A retrospective radiographic and chart review of 197 consecutive cheilectomies was performed on 189 patients (8 bilateral) with hallux rigidus between 2003 and 2010 at a single institution. The diagnosis of hallux rigidus was made by combining clinical and radiographic findings as follows: A clinical exam eliciting pain with range of motion activities and soft tissue swelling combined with a radiographic display of dorsal osteophytes and/or joint narrowing, yet maintaining a congruous joint. Patients who had nonoperative treatment or noncheilectomy procedures performed on the first MTP were excluded. The index procedure was performed by a foot and ankle surgeon from the senior author’s group practice.
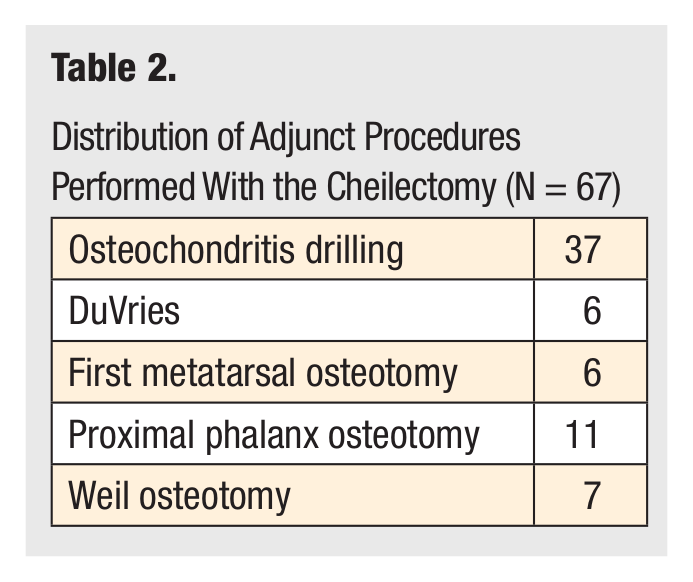
Concomitant surgical procedures were established from the operative report and documented (Table 2). Demographic data were recorded, including patient age, gender, and body mass index. Date of surgery, date of radiographic follow-up, and date of last follow-up were recorded. Preoperative grading using the Coughlin scale was performed and recorded, stage 1 through 3 (Figure 1) based on preoperative radiographs (Figure 2). Patients progressing to repeat first MTP surgery were recorded, including the procedure performed and the date (Table 3); these were considered a failure if a procedure other than a cheilectomy was performed at the first MTP. Success was determined by lack of joint destructive subsequent first MTP surgery. The date of surgery was the starting point and the date of final chart review for the writing of this article was the endpoint.
Distribution of Adjunct Procedures Performed With the Cheilectomy (N = 67)
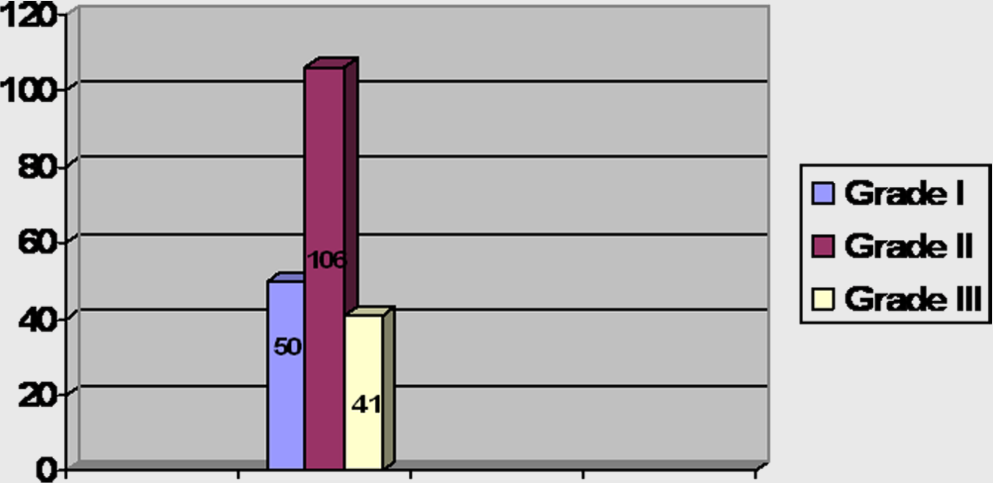
Distribution of radiographic preoperative Coughlin grades (N = 189).

Preoperative anteroposterior (A) and lateral (B) radiographs.
Demographics (Age, Gender), Grade, BMI, Adjunct Procedures, and TTS (N = 7)
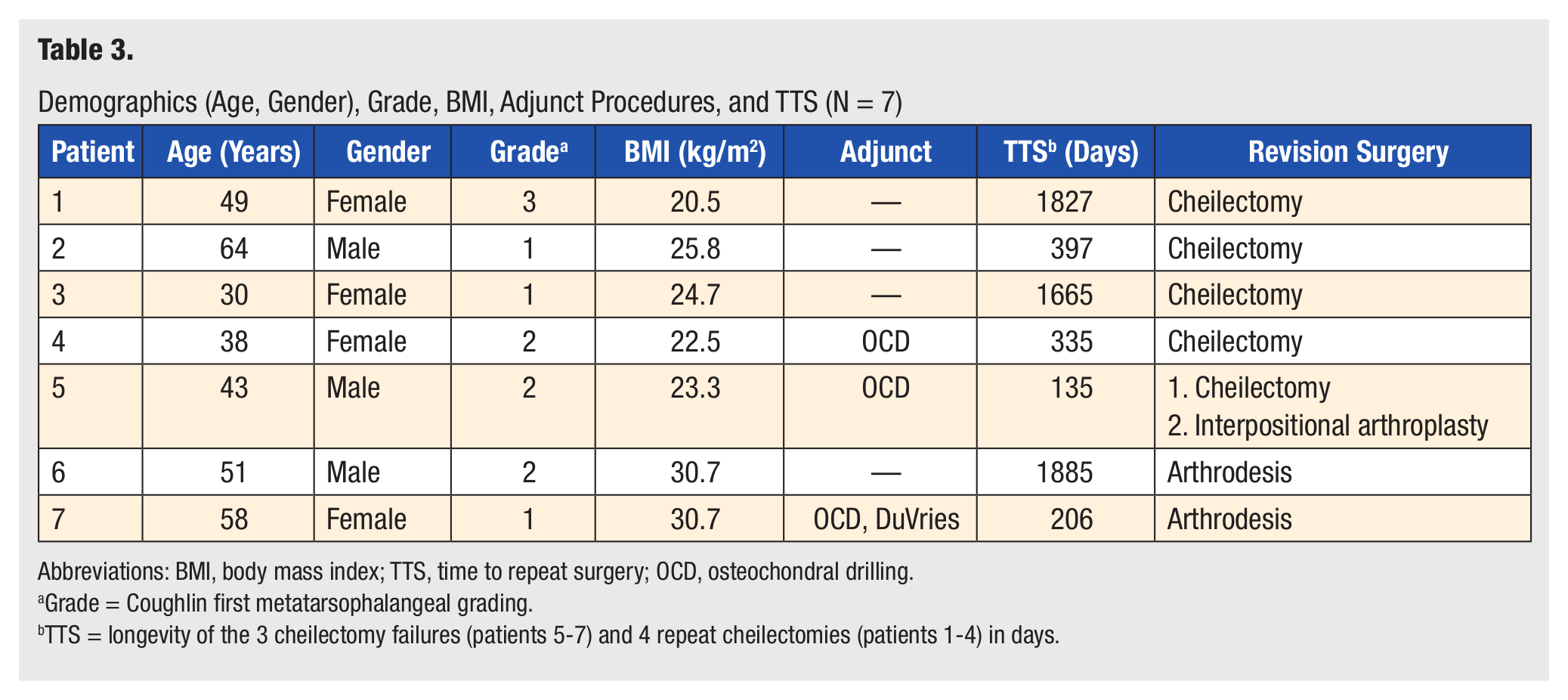
Abbreviations: BMI, body mass index; TTS, time to repeat surgery; OCD, osteochondral drilling.
Grade = Coughlin first metatarsophalangeal grading.
TTS = longevity of the 3 cheilectomy failures (patients 5-7) and 4 repeat cheilectomies (patients 1-4) in days.
Surgical Technique
Cheilectomy was performed with the patient supine on the operating table. General anesthesia was administered, at times in conjunction with a preoperative regional block. A thigh tourniquet was applied and inflated for the entirety of the case. A dorsal incision was made, avoiding the extensor hallucis longus tendon and retracting any neurovascular structures. Electrocautery was used as necessary. Full-thickness flaps were raised exposing the joint. Loose bodies were removed and the cartilage assessed. Ectopic bone was resected with a sagittal saw on the first metatarsal head, in line with the metatarsal, and a rongeur on the proximal phalynx base. If full-thickness cartilage defects were visualized, they were drilled to subchondral bone with a small gauge wire. Range of motion was assessed to verify adequate boney resection. Closure was performed with absorbable and nonabsorbable suture. A soft, sterile dressing was applied after a local injection, if no preoperative block was used.
Weight bearing was allowed immediately in a surgical shoe as tolerated. Dressings were removed at postoperative visit number one, with suture removal and follow-up radiographs performed (Figure 3). Active range of motion activities were introduced at this time. Progression to regular shoe gear as swelling and postoperative pain allowed. Athletic activity was allowed at 12 weeks.

Postoperative anteroposterior (A) and lateral (B) radiographs.
Results
The study population consisted of 189 consecutive patients after excluding patients who had a primary cheilectomy with interpositional arthroplasty, primary arthrodesis, failed implant revision, gout, rheumatoid arthritis or osteomyelitis. This group was composed of 71 men and 118 women with a mean age of 49 ± 10.5 years (range = 13-80 years; Table 3). Eight of these cases were bilateral. The body mass index mean was 27.6 ± 4.9 kg/m2 (range = 19.1-43.0 kg/m2; Table 3). The mean radiographic follow-up time was 235 ± 405 days (0.64 ± 1.11 years), and the mean chart review follow-up time was 1184 ± 831 days (3.23 ± 2.28 years).
Figure 1 displays the distribution of the preoperative radiographic Coughlin grades, consisting of 50 (25%) grade 1, 106 (54%) grade 2, and 41 (21%) grade 3. The procedures that were performed along with the cheilectomy are displayed in Table 2. These were 37 osteochondral drillings, 6 DuVries arthroplasties, 6 first metatarsal osteotomies, 11 proximal phalanx osteotomies, and 7 Weil osteotomies. Revision surgery was performed on 7 patients at the first MTP, with only 2 of these progressing to first MTP arthrodeses and 1 joint destructive interpositional arthroplasty. The other revision procedures were 4 repeat cheilectomies. The details of these cases are displayed in Table 3.
The failure rate of the cheilectomy procedure was found to be 1.5% in this study, with failure defined as subsequent arthrodeses or another type of joint destructive procedure. No significant correlation was found between these failures and the demographics, radiographic grading, longevity, or adjunct procedures, using the Pearson coefficient in SPSS statistical software (SPSS 13.0, Chicago IL).
Discussion
The 98.5% success rate of the cheilectomy procedure of the first MTP found in this study is consistent with other rates in the literature, ranging from 70% to 96%.5,10,15,16 The majority of these successes were found in patients with hallux rigidus grades 1 and 2.4,5,8 Easley et al 16 found none of their cheilectomy grade 1 and 2 patients needing to have an arthrodesis after 5 years. They also found that only 2 of the 12 grade 3 patients needed arthrodeses.
Coughlin and Shurnas 14 stated that the cheilectomy was successful in their patients with grades 1, 2, and 3 who had <50% metatarsal head cartilage loss. Feltham et al 10 found no significance among preoperative grades but did find higher American Orthopaedic Foot and Ankle Society scores in patients >60 years old. An additional proximal phalanx osteotomy was found to improve outcomes in patients with grade 1 and 2 hallux rigidus with <70° of dorsiflexion after the cheilectomy. 17 Another study evaluated high-level professional athletes with grade 1 and 2 hallux rigidus who had a cheilectomy was performed, and no further procedure was needed 5 years postoperatively. 18
Our study cohort ranged from grades 1 to 3 and we found no significant correlation with the success of the cheilectomy and preoperative grade. Although we did not include operative cartilage findings, outside of OCD drilling, this has been noted in other studies and may be beneficial to perform in future studies.
The success that has been found with this procedure is encouraging since cheilectomy has been shown to yield a low complication rate of 0% to 3%.19-21 Some have evaluated the biomechanics following this procedure. Significant improvements in cadence, stride length, and stance/swing ratio were noted 18 months following a cheilectomy procedure. 22 These findings support the continued use of cheilectomy for stage 1 through stage 3.
Limitations of this study are inherent with this being a retrospective study and we did not have a control group. Also, this study lacked a patient subjective outcome score. Future studies would likely include comparing the success rates of different hallux rigidus procedures in specific preoperative settings to determine the most effective. Also, looking at other preoperative predictive factors such as, demographics, grading, longevity, for the other hallux rigidus procedures could lead to more decisive surgical planning.
In conclusion, we found that the cheilectomy was a successful procedure for Coughlin grades 1, 2, and 3 hallux rigidus after a mean of 3 years. This adds to the existing literature leading to the favorability of this procedure.