
Abstract
“Some foot and ankle surgeons have perceived the condition to be a medical curiosity and only a minor anomaly, causing little immediate or long-term functional impairment.”
Introduction
A ball-and-socket ankle is an abnormal configuration of the ankle joint characterized by rounding of the trochlear surface of the talus. 1 The normal trapezoidal-wedge shape of the trochlear surface, which normally articulates with the tibiofibular portion of the joint, is altered to that of a hemisphere. 1 A concavity subsequently develops in the articular surface and epiphysis of the distal tibia to become congruent with the hemispherical, convex talus. In addition, the distal fibular articular surface and epiphysis becomes broader and more concave than the normal talofibular articulation (Figure 1). 1

Ball-and-socket ankle configuration. Anteroposterior weight-bearing radiograph demonstrating the typical configuration of a ball-and-socket ankle on the right compared with a normal ankle on the left. Note the valgus ankle alignment, hemispherical trochlear surface of the talus, reciprocal concavity of the distal tibial articular surface, and broader, concave distal fibular articulation.
This abnormality was first described in the German orthopaedic literature by Politzer 2 in 1931 but was not described in the English literature until 1958 by Lamb. 3 Commonly associated conditions include a short tibia, tarsal coalitions, absent digital rays, and fibular hypoplasia.4,5 Some authors propose that the condition represents a congenital defect, 1 whereas others have suggested it to be an acquired deformity driven by these associated limb anomalies. 6
There is no consensus regarding the natural history of the ball-and-socket ankle joint, and the literature provides no guidelines for the management of patients with this condition either at an early stage or after the development of ankle or subtalar arthrosis. 7 In fact, the natural history remains a matter of debate.7,8 Some foot and ankle surgeons have perceived the condition to be a medical curiosity and only a minor anomaly, causing little immediate or long-term functional impairment. 7 In a review of 51 patients with this deformity, Pappas and Miller 1 reported no symptoms attributable to this deformity at a mean follow-up of 17 years, with the oldest patient at 37 years of age.
Although many authors claim that no patients are symptomatic and thus no treatment is indicated, 1 others have advocated the use of an ankle-foot orthosis to control pronation and prevent progressive ankle valgus. 9 Some suggest early intervention at the subtalar joint to correct impingement and prevent or treat subsequent arthrosis.7,10 Other authors have reported late pain and/or degenerative changes associated with this abnormality. 11
In this study, we review the surgical management of 4 adult patients with ball-and-socket ankle deformity who developed end-stage subtalar and/or ankle joint arthritis. Surgical interventions included subtalar arthrodesis as well as total ankle arthroplasty in these patients. To our knowledge, this represents the first series in the literature describing surgical management of adults with end-stage arthritis in the subtalar and tibiotalar joints, in the setting of ball-and-socket ankle deformity.
Materials and Methods
After obtaining appropriate institutional review board (IRB) approval, we retrospectively reviewed a series of 4 adult patients with clinical and radiographic evidence of a ball-and-socket ankle configuration as described by Pappas and Miller, 1 who were treated by the senior author (JKD). All 4 patients underwent surgical treatment on the affected extremity. In each case, the surgical indication was to relieve pain and/or correct deformity for either end-stage tibiotalar or subtalar arthritis refractory to all conservative measures. All 4 patients underwent either subtalar arthrodesis or total ankle replacement (TAR). Any patient who was treated at our institution with a ball-and-socket ankle configuration who underwent a different surgical procedure or was treated with nonoperative management was excluded from this study.
At follow-up, we inquired about pain, limitation of activities, and difficulty with shoe wear. One of the patients who underwent total ankle arthroplasty was entered into a prospective database of patients undergoing ankle replacement at our institution, and several outcome measurements, including American Orthopaedic Foot and Ankle Society (AOFAS) Scores, Short Form 36 (SF-36), Visual Analog Scores (VAS) for pain, and Short Musculoskeletal Function Assessment (SMFA) Scores, were collected prospectively. All patients underwent weight-bearing radiographs preoperatively and at regular intervals postoperatively. Any failures, defined as requiring removal of one or both metal components for infection or loosening, were recorded.
Results
A total of 5 ankles in 4 patients were identified that met the inclusion criteria. There were 3 subtalar arthrodeses in 2 patients and 2 primary TARs in 2 patients. The mean age of the patients was 69.0 (range = 56 to 81) years, with the average age of those who underwent subtalar arthrodesis being 76.0 years and those who underwent TAR being 62.0 years. At an average follow-up of 30.5 (range = 17 to 59) months, there were no failures, although one patient who underwent TAR was found to have aseptic loosening and was considered an impending failure. Average follow-up was 38.0 months for those who underwent subtalar arthrodesis and 23.0 months for those who underwent TAR. The average number of associated procedures to achieve a balanced plantigrade foot was 0.7 (range = 0-2) in the subtalar arthrodesis group compared with 5.5 (range = 4-7) in the TAR group.
Patient 1
The first patient was a 71-year-old man who presented complaining of progressive worsening pain in his right ankle and hindfoot for 3 years. He had exhausted conservative therapy, including corticosteroid injections into the subtalar joint, which had previously eliminated his pain. Preoperative imaging confirmed a ball-and-socket ankle configuration with severe degenerative changes in his subtalar joint (Figure 2). He underwent subtalar arthrodesis combined with medial cuneiform opening wedge osteotomy to correct for midfoot varus and a partial distal fibulectomy to address subfibular impingement. Postoperatively, he was immobilized in a short leg cast and made non–weight bearing for a period of 6 weeks. By 3 months postoperatively, the patient had progressively advanced his activities, including resuming golf. By 6 months postoperatively, he rated his pain as a 0 out of 10, ambulated with a normal gait, and was very happy with his outcome. He had good evidence of radiographic union and was released to full activity. At the most recent follow-up 24 months from his surgery, the patient continued to do well, playing golf regularly, and with no complaints.

Patient 1: Anteroposterior (A) and lateral (B) weight-bearing radiographs demonstrating ball-and-socket ankle configuration. Computed tomography (CT) scan demonstrating severe degenerative changes in the subtalar joint (C and D). Postoperative radiographs at 6 months (E) and 1 year (F) after surgery demonstrating solid arthrodesis at the subtalar joint.
Patient 2
The second patient was an 81-year-old man who presented with a 10-year history of progressive bilateral ankle and hindfoot pain refractory to conservative bracing and custom shoe inserts. On weight-bearing radiographs, he was noted to have bilateral ball-and-socket ankle deformities (Figure 3). He maintained 30° of hindfoot inversion and 10° of eversion on physical exam, although this movement was painful for him. Live fluoroscopic evaluation suggested the presence of mobile but arthritic subtalar joints. He underwent corticosteroid injections into his bilateral subtalar joints with excellent but temporary relief of his pain. A CT scan confirmed severe degenerative changes in his bilateral subtalar joints. He thus underwent left subtalar arthrodesis. Postoperatively, he was immobilized in a short leg cast and made non–weight bearing for a period of 6 weeks. By 3 months postoperatively, the patient had progressively advanced his activities. He had some mild persistent heel pain, which was treated with shoe inserts. By 8 months postoperatively, he was having some persistent pain, and a CT scan was obtained, which showed a possible nonunion. However, by 14 months postoperatively, the patient was pain free and was very happy with his outcome. He, therefore, underwent right subtalar arthrodesis, with an identical postoperative course of immobilization. By 4 months postoperatively, the vast majority of his pain was gone, and at 10 months, he appeared to have solid fusions in both hind feet. He was very pleased with his overall outcome.

Patient 2: Anteroposterior weight-bearing radiograph (A) demonstrating bilateral ball-and-socket ankle configuration. Lateral radiographs (B and C) showing subtalar arthrosis, with CT scan (D and E) confirming severe degenerative changes in the bilateral subtalar joints. Postoperative radiographs at 6 months after surgery (F and G) demonstrating solid arthrodeses at the subtalar joints.
Patient 3
The third patient was a 56-year-old woman who presented with a history of right ankle pain, swelling, and deformity since she was a child. Of note, we had recently performed a conversion of a failed left tibiotalar arthrodesis, which was performed by an outside foot and ankle surgeon, to a TAR and she was very satisfied with her outcome. Clinically, her right ankle was in significant valgus, and radiographs confirmed a ball-and-socket ankle configuration with severe arthrosis in the tibiotalar joint (Figure 4). She was also noted to have an ipsilateral subtalar coalition. She thus underwent primary TAR with the INBONE prosthesis (Wright Medical, Arlington, TN) with multiple concomitant procedures to achieve a neutral plantigrade foot, including gastrocnemius recession, fibular and cuneiform osteotomies, and prophylactic pinning of the medial malleolus to prevent an impending stress fracture. Because of the lack of sufficient native talar bone stock, the talar component was essentially positioned on the superior calcaneus. Postoperatively, she was immobilized in a short-leg fiberglass cast and made non–weight bearing for 6 weeks. Her weight bearing was then progressively advanced. Unfortunately, the patient continued to have medial-sided pain on the right ankle, although she was able to ambulate. A CT scan 15 months postoperatively showed lucency around the tibial and talar component stems, concerning for loosening. Erythrocyte sedimentation rate and C-reactive protein inflammatory markers were within normal limits. She was offered a revision of her ankle prosthesis for suspected aseptic loosening, but the patient has declined any further intervention. Outcome data were collected prospectively on this patient, and she did demonstrate an increase of AOFAS total scores from 40 preoperatively to 50 at 1 year postoperatively. She showed similar modest improvements in SF-36 scores (34.8 preoperatively to 46.5 at 1 year after surgery), SMFA Function (50.7 preoperatively to 30.9 at 6 months and 41.9 at 1 year postoperatively), and Bother (52.1 preoperatively to 22.9 at 6 months and 39.6 at 1 year postoperatively). Her VAS scores ultimately remained relatively unchanged, improving from 83 preoperatively to 62 at 6 months postoperatively but worsening to 89 at 1 year postoperatively.
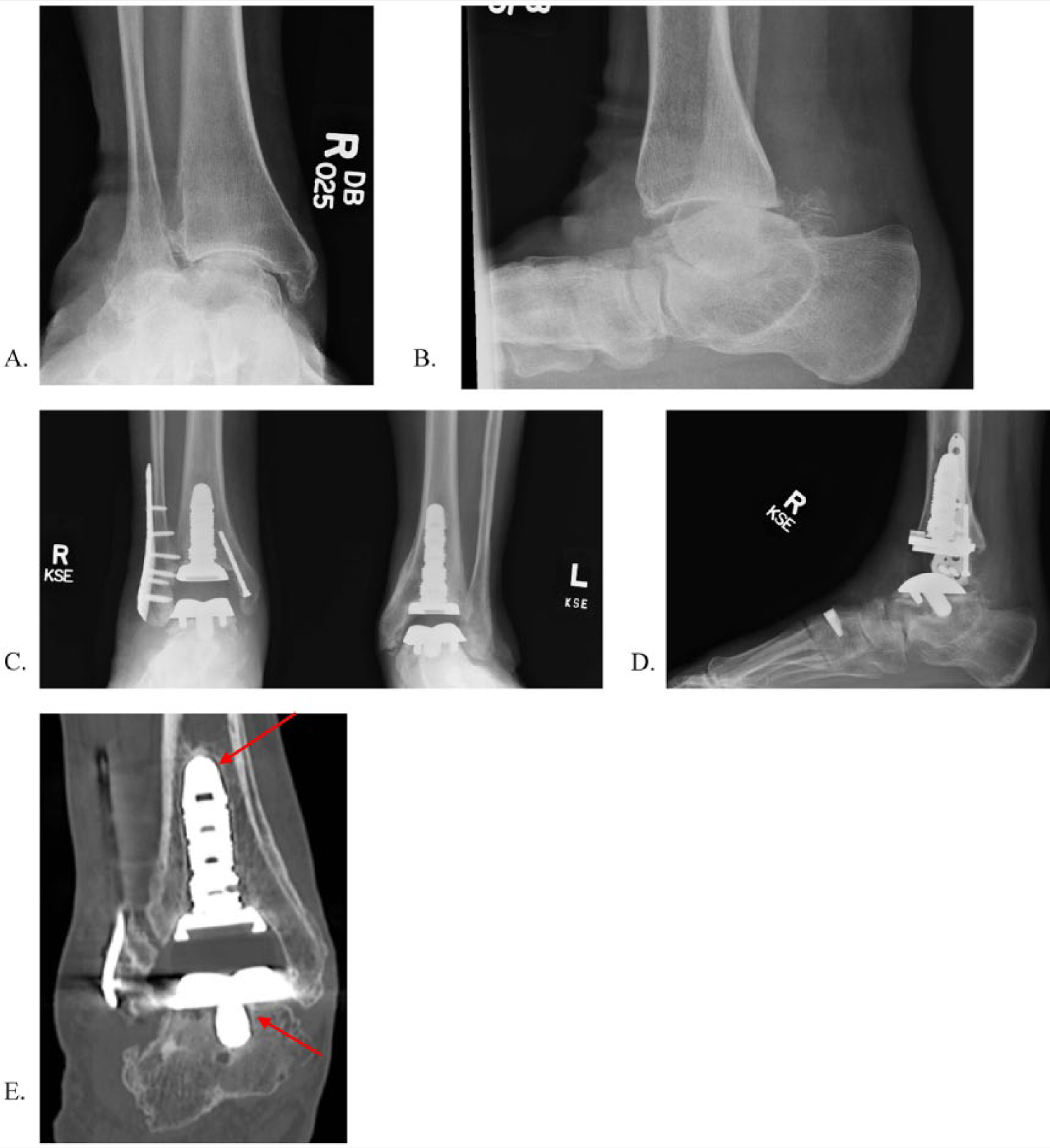
Patient 3: Anteroposterior (A) and lateral (B) weight-bearing radiographs demonstrating a ball-and-socket ankle configuration with severe degenerative changes in the tibiotalar joint. Immediate postoperative radiographs (C, D) showing well-aligned total ankle prosthesis with fibular osteotomy fixed with a plate, prophylactic fixation of the medial malleolus, and cuneiform osteotomy with titanium spacer. CT scan (E) obtained 15 months postoperatively showing faint lucencies around the tibial and talar component stems (arrows) concerning for loosening.
Patient 4
The fourth patient was a 68-year-old man who presented with more than 10 years of progressive intractable right ankle pain refractory to conservative measures, including oral nonsteroidal anti-inflammatory medications and bracing. Clinically, his ankle was in significant valgus, and radiographs confirmed a ball-and-socket ankle configuration with severe arthrosis in the tibiotalar joint (Figure 5). He, therefore, underwent primary TAR with the INBONE prosthesis (Wright Medical, Arlington, TN), with multiple concomitant procedures to achieve a neutral plantigrade foot, including medial calcaneal sliding osteotomy, gastrocnemius recession, fibular and cuneiform osteotomies, lateral ankle ligament reconstruction, and transfer of the peroneus brevis and longus to the posterior tibial tendon. Postoperatively, he was immobilized in a short-leg fiberglass cast and made non–weight bearing for 9 weeks. At 11 weeks postoperatively, he developed a posteromedial soft-tissue abscess that required 2 operative debridements, polyethylene component exchange, and 8 weeks of parenteral antibiotic therapy. At 6 months postoperatively, the patient was extremely pleased with his outcome, could walk without any assistive device, and had no signs of recurrent or deep infection.
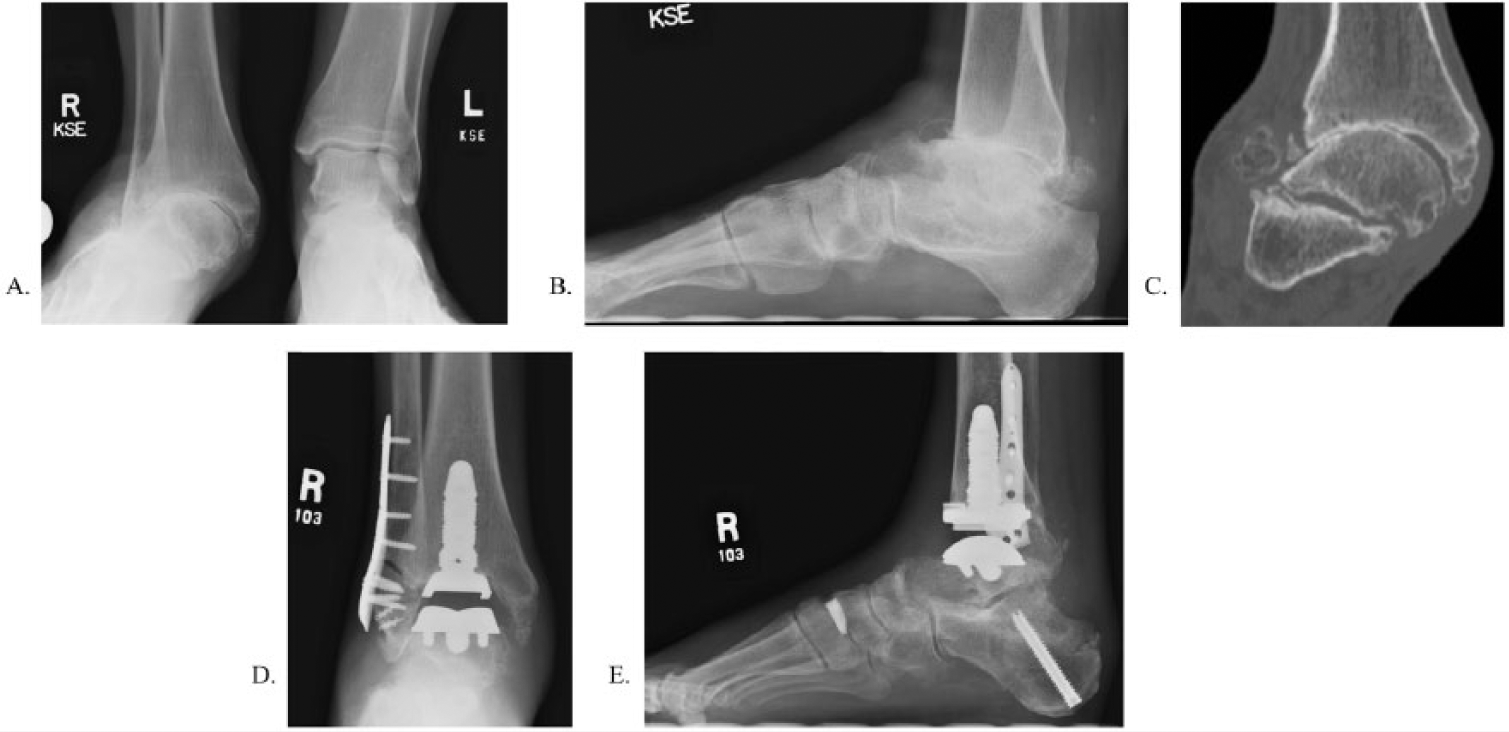
Patient 4: Anteroposterior (A) and lateral (B) weight-bearing radiographs and CT scan (C) demonstrating a ball-and-socket ankle configuration on the right side with severe degenerative changes in the tibiotalar joint. Immediate postoperative radiographs (D, E) showing well-aligned total ankle prosthesis with fibular, calcaneal, and cuneiform osteotomies.
Discussion
The ball-and-socket ankle deformity, first described by Politzer 2 in 1931, is characterized by abnormal hemispherical rounding of the trochlear surface of the talus with a reciprocal concavity in the articular surface and epiphysis of the distal tibia. 1 The condition often occurs unilaterally, although bilateral cases such as the patient included in this series are not unusual.3,4,11 Gender predilection remains unclear because some authors contend that men are more commonly affected, 11 whereas others report that the condition appears to affect men and women equally. 7 It is rarely diagnosed before the age of 4 until normal ossification of the talocrural joint progresses. 7
Many authors contend that this often represents a single aspect of a greater spectrum of anomalous limb development rather than an isolated finding.1,7,10 It is often a component of the spectrum of postaxial hypoplasia of the limb.7,12 Commonly associated musculoskeletal abnormalities include tarsal coalitions, leg length discrepancies with tibia and/or fibula shortening, acetabular dysplasia, genu valgum deformity, absent cruciate ligaments, foot syndactylization, and absent digital rays.1,3,4,7,11 The high incidence of synchronous hindfoot coalition has led to the hypothesis that ball-and-socket ankle joints are an adaptive change to compensate for loss of hindfoot eversion and inversion caused by a tarsal coalition.11,13 Because some patients with ball-and-socket ankle deformity have no associated tarsal coalition that would limit subtalar motion, including 4 of the 5 ankles included in this study, other authors suggest that the deformity is the result of a primary germplasm malformation 7 as part of a congenital lower-extremity hemiatrophy syndrome, 3 part of a congenital syndrome of the hindfoot, 5 or an atavistic regression. 1
Pappas and Miller 1 contended that the rounded talus in a ball-and-socket ankle joint allows rotation in the horizontal plane, and the lateral torque normally provided through the subtalar joint prevented by subtalar immobility is provided by the ankle joint itself in these patients. Because the abnormal ankle joint remains inherently stable, many authors have felt it appropriate to treat the condition expectantly with little or no intervention.7,13 In one of the largest case series in the literature, Pappas and Miller 1 reported no symptoms attributable to this deformity in 51 patients with a mean follow-up of 17 years. Although the oldest patient was only 37 years of age at the conclusion of this series, the authors concluded that the abnormality causes little or no functional impairment and, thus, requires no intervention. 1
Over time, however, the ankle tends to drift into valgus because of the abnormally shortened fibula and the hemispherical plafond. 7 Consequently, some authors have described localized impingement-type pain, clinical deformity, difficulty with daily activities, and accelerated shoe wear. 7 Described treatments for the ball-and-socket ankle, however, tend to be directed toward the leg-length discrepancy associated with the condition or correcting any progressive valgus deformity. 7 For example, Steingard and Percy 9 proposed the use of an ankle-foot orthosis to prevent pronation, and Stevens et al 7 proposed medial malleolar epiphysiodesis using a cannulated screw to correct for ankle valgus.
The first case of osteoarthritic change in an ankle with a ball-and-socket configuration was reported in the literature in 1987 by Dennis et al. 11 They reported significant ankle valgus and osteoarthritic degeneration in the distal tibiofibular joint and in an arthritic false articulation between the distal fibula and lateral calcaneus in a single 50-year-old male patient. No significant arthritic change in the abnormal tibiotalar joint was described. This patient was treated conservatively with bracing, shoe inserts, and physical therapy emphasizing ankle inversion. 11 No surgical intervention was performed.
To our knowledge, this series represents the first description of surgical management for ankle and subtalar arthritis in adults with a ball-and-socket ankle configuration. Subtalar arthrodesis was able to be performed with minimal adjunct procedures, with good patient-reported outcomes. In contrast, multiple adjunct procedures were required to achieve balanced plantigrade feet in patients with ball-and-socket ankle deformities undergoing TAR, and outcomes tended to be less predictable than in those who underwent subtalar arthrodesis. For both patients who underwent TAR, the INBONE II prosthesis was chosen to utilize its intramedullary referencing and modular intramedullary tibial component, both of which were felt to be advantageous in these cases of distinctly abnormal tibiotalar configurations to achieve appropriate implant position and maximize coronal plane stability. Limitations of this study include its retrospective design and small sample size. The rarity of the ball-and-socket ankle configuration in the general population, however, makes it difficult to obtain a large patient population; the largest case series in the literature only includes 51 patients. 1 Furthermore, no conclusions about the incidence of subtalar and ankle arthritis in these patients can be drawn from this small case series. It also remains unclear whether the joint degeneration seen in these patients represents an end-stage process caused by abnormal joint kinematics resulting from a ball-and-socket deformity or if the pathology developed independently in a fashion similar to that in individuals with normal ankle configurations.
As previously mentioned, there is no consensus regarding the natural history of the ball-and-socket ankle joint, and many authors contend that affected patients have minimal functional limitations, requiring no intervention.1,7 Many of the studies on this condition have been published in the pediatric literature, however, and the majority of case series do not include patients older than 40 years. Late degeneration of the ankle and subtalar joints in these patients can clearly occur, with similar levels of pain and functional limitation compared with conventional cases of ankle arthritis. Similarly, we have shown that with careful surgical planning with attention to the underlying ball-and-socket deformity, standard surgical interventions for ankle and subtalar arthritis, such as total ankle arthroplasty and subtalar arthrodesis, can be successfully performed. The overall clinical outcome and survivorship, however, may be inferior to that in patients with more normal native ankle configurations.