
Abstract
Glomus tumor, originally known as an angioneuromyoma, is a benign neoplasm arising from specialized structures called glomus bodies, involved in thermoregulation. Although it has been reported at a number of sites in the body, this rare tumor is most commonly seen in the subungual areas of the digits of the hand. Only a handful of lesions have been reported in the toes. Because most foot conditions are treated by podiatrists and dermatologists, orthopaedic surgeons are generally unaccustomed to making early diagnoses. The purpose of this case report is to alert the attending surgeon regarding the possibility of glomus tumor as a cause of chronic toe pain. Also it has been observed that the behavior of this tumor varies with the site of occurrence—whether digital or extradigital. So we have extensively reviewed all similar reports in the literature to analyze the behavior of this tumor at this unusual location, apart from comparing it with the more common finger variety, to ensure it possibly is not a misclassification like the chemodectomas that were earlier thought to be glomus tumors.
Introduction
Glomus tumor, a benign neoplasm of neuromyoarterial tissue, is commonly seen in subungual regions of the digits of the upper extremity. An extradigital variety, although uncommon, is also well known. However, among the digital variety, glomus tumors have very rarely been reported in the toes. Considering this rare occurrence, the diagnosis may not be readily apparent.1,2 Moreover, toe disorders are generally treated by dermatologists or podiatrists, so many orthopaedic surgeons tend to be unaccustomed to diagnosing such a condition. 2 The purpose of this article is to alert the attending physician to consideration of this tumor as a rare possible cause of a painful toe, thereby preventing an undue delay in diagnosis and management of such patients. Also, because considerable differences exist between the digital and extradigital variety, expecting something similar, we conducted an extensive literature search to analyze the behavior of the tumor at this rare site and compare it with the conventional upper-extremity digital presentation.
Case Report
A 19-year-old female patient presented to our department with a history of bursting pain in the left great toe for the past 8 years for which she had been consulting various doctors. There was no history of trauma. Over past 2 years, she had visited 5 physicians, and all of them had advised conservative therapy, administering a variety of analgesics, although none had been providing her with permanent relief. From one of her prescriptions, we discovered that she had been put on Amitryptiline, an antidepressant as well, for a period of 6 weeks, but with no benefit. On probing further, she gave us a history of cold hypersensitivity. Examination revealed an area of point tenderness directly over a faint bluish hue visible over the nail plate. There were no trophic changes observed, however. Our clinical suspicion at once was a glomus tumor, though this seemed an extremely uncommon site. We confirmed it with radiological investigations and got a radiograph and magnetic resonance imaging (MRI) done. The latter clearly demonstrated the subungual lesion that was lying beneath the nail bed but was not causing any osseous erosion. Informed consent was taken, and the patient was prepared for surgical removal of the lesion. The tumor was excised after removing the nail plate, and the nail plate was reapplied. Grossly it was a purplish red fleshy mass of size 4 × 3 mm2 (Figures 1-3). The diagnosis was confirmed on biopsy. The patient became completely asymptomatic after 3 weeks of surgery. She has been under follow-up for the past 16 months now and is completely free from pain, with no signs of recurrence.

Clinical Photograph of the Tumor.

Magnetic Resonance Imaging Showing the Tumor in Coronal Section.

Magnetic Resonance Imaging Showing the Tumor in Sagittal Section.
Discussion
Glomus tumor is a benign neoplasm arising from a neuromyoarterial apparatus called glomus body (size varies from 120-220 µm). Glomus bodies are arteriovenous shunts, surrounded by glomus cells, present in the Sucquet Hoyer canal, which contract via sympathetic activity, thereby regulating blood flow to the extremities. Hence, they play a role in thermoregulation, decreasing blood flow when the body is exposed to cold and increasing it when it is hot. Glomus bodies are located in the dermis throughout the body but more densely concentrated in apical skin areas, primarily the fingertips, followed by the base of foot and the rest of the body.1,2 The most common site of occurrence of this tumor is the subungual area of the fingers, and it may constitute almost 2% to 5% of all hand tumors.2,3 However, there are reports of glomus tumors in many other sites, such as the wrist, forearm, elbow, arm, shoulder, buttock, thigh, knee, leg, back, nose, cheek, ear lobe, trachea, lungs, mediastinum, tongue, stomach, rectum, bone, and patellar tendon.4 -6 Only occasionally has this tumor been reported in toes.
The glomus tumor was first mentioned by Wood 7 in 1812, but a complete description of its character was given by Masson in 1924. 8 This neoplasm is more common in women, particularly in the age group of 30 to 50 years. In fact, the normal glomus begins to appear a few months after birth, develops fully in adulthood, and atrophies after the age of 60 years. Familial occurrence of the tumor has also been reported. 2 In its commonest location—namely, the subungual tissue of the fingers—the glomus tumor generally presents with a characteristic triad of intense paroxysmal pain, pinpoint tenderness, and hypersensitivity to cold. Pain is the most common symptom and is generally sharp and bursting in nature and may radiate to the base of the toe. One may be able to find a bluish discoloration below the nail plate or a palpable mass that deforms the nail plate.1,2 A previous history of trauma may be elicited, but connection with previous injury has not been established yet, although some authors have suggested that injury causes weakness of the glomus and a later reactive hypertrophy. 9 Almost 90% of the lesions are solitary, but multifocal involvement (around 10% cases) can occur and is particularly seen in association with neurofibromatosis type 1. 10 It has been related to a gene located in the 1 p 2111 chromosome with an autosomal dominant pattern of inheritance. Kohout and Stout 11 reported a higher incidence of multiple lesions in patients younger than 16 years.
Microscopically, the lesion comprises uniform cells, somewhat epithelial in nature distributed outside an abundant branching vasculature. Although 4 types are reported—angiomatous, paucivascular, neuromatous, and mucoid hyaline—an exact categorization is often not possible owing to the frequent mixture of various types. However, the angiomatous component usually predominates. The capsule is a pseudocapsule formed by condensation of surrounding tissue and may show infiltration in 1% to 2% of cases, but generally without any evidence of malignant change. The reported rate of malignant degeneration is less than 1%, and lesions that are >2 cm or located deep within the dermis generally tend to go malignant. 2
Though this is a rare, small benign lesion, generally <1 cm in size (largest reported being 1.5 inches), the morbidity caused by this lesion is great. The tumor has both myelinated and nonmyelinated nerve fibers entering the capsule, shown to be capable of releasing neurotransmitters such as substance P. Distortion of the capsule because of changing vascularity generates a bursting pain, which at times can be severely disabling.2,12 Despite causing such a heavy morbidity, there is almost always a delay in its diagnosis, and it is not unusual to label these patients as malingerers or neurotics. Many patients are labeled as having chronic paronychia and treated for the same for years. Those who tend to give a history of previous trauma are often misdiagnosed as having a subungual hematoma. Rarely, the surgeon tends to consider the possibility of subungual melanoblastomas or a Koenen’s tumor (peri/subungual fibroma), but these are generally not that painful. However, with a clear history, meticulous examination, and modern investigations, it is very easy to pick up the tumor early. Love’s test—that is, pain when applying pressure—has a sensitivity of 100%, but a specificity of 0%. The Hildreth test, with a sensitivity of 77% to 92% and a specificity of 91% to 100%, is based on the vascular nature of this tumor. It consists of applying a tourniquet above the systolic pressure; if the pain disappears, it is probably a sign of glomus tumor. 2 Transillumination can also be used in confirming the diagnosis. The radiological image is pathognomonic if there is osseous erosion caused by the lesion; else one may need an MRI, where a dark outlined image is seen on T1 sections and a bright outlined mass is noticed in T2 sections. On dynamic MR contrast angiogram, the lesion shows intense enhancement in the arterial phase with tumor blush. Ultrasonography may show a hypoechoic lesion, with significant vascularity on color Doppler. 13
Treatment is primarily surgical, requiring complete excision of the lesion. The tumor may be accessed via the nail plate avulsion or a periungual approach depending on the location. A transungual extraction (through a window) has been described, but is generally impractical because many a time, the nail may be dystrophic. Recovery generally takes 2 to 4 weeks, but at times, it may take a couple of months for the patient to feel no pain. Some authors have suggested prescribing indomethacin after 10 days of treatment to control pain, but we have no experience with it because our patient demonstrated significant relief around a week after excision. Although recurrence rates varying from 0% to 30% have been reported, 2 a good surgical excision is generally uneventful. Recurrence, if it happens early, is usually a result of incomplete removal of the tumor and, if it happens late, is because of the appearance of a second tumor.
Extradigital glomus tumors do not share all the characteristics of the subungual digital variety. They more commonly affect men in their fourth to seventh decade of life. 14 Though pain is a common symptom, the other 2 features of the classic triad—cold hypersensitivity and pressure tenderness—may not be apparent in the extradigital variety. Similarly, history of previous trauma may be present more commonly with the extradigital variety. 14 What makes them different is still an unanswered question. Considering the differences between these 2 subtypes, our attention shifted to the subungual lesions of fingers and toes. We conducted an extensive literature search to evaluate whether as in the case of chemodectomas, which were once labeled as glomus tumors but eventually came to be known as a separate entity with a separate tissue of origin, something similar was true for the toe lesions as well.
In Table 1, we have comprehensively summarized almost all descriptions of glomus tumors of toes given by different authors till date. Interpretations from the table helped us make many useful predictions. Even in toes, the tumor seemingly presents much in the same manner, with the classical triad of symptoms, with most cases clustering in the 25- to 60-year-old age group. Although the female preponderance of 3 is to 1 is there for tumors in fingers, the predilection seems to be much stauncher for the toe variety, with almost all except a couple of reports referring to female sex. However, the distribution between left and right side appears to be somewhat more balanced. Most tumors in toes are also subungual in location, just like in the upper extremity, where the pulp variety constitutes less than 10%. One must, however, note that an intraosseous glomus of the toe nail has also been reported, which had to be treated by partial amputation of the toe. 15 In such cases, the glomus bodies are located in the medullary canal of the distal phalanges. But these lesions have more commonly been reported around the ankle, proximal ulna, and fibula. 16 However, going by the available reports, the toe glomi can be subclassified as follows: subungual, intraosseous, and pulp lesions.
Characteristics of Glomus Tumor of Toes From Previous Similar Case Reports.
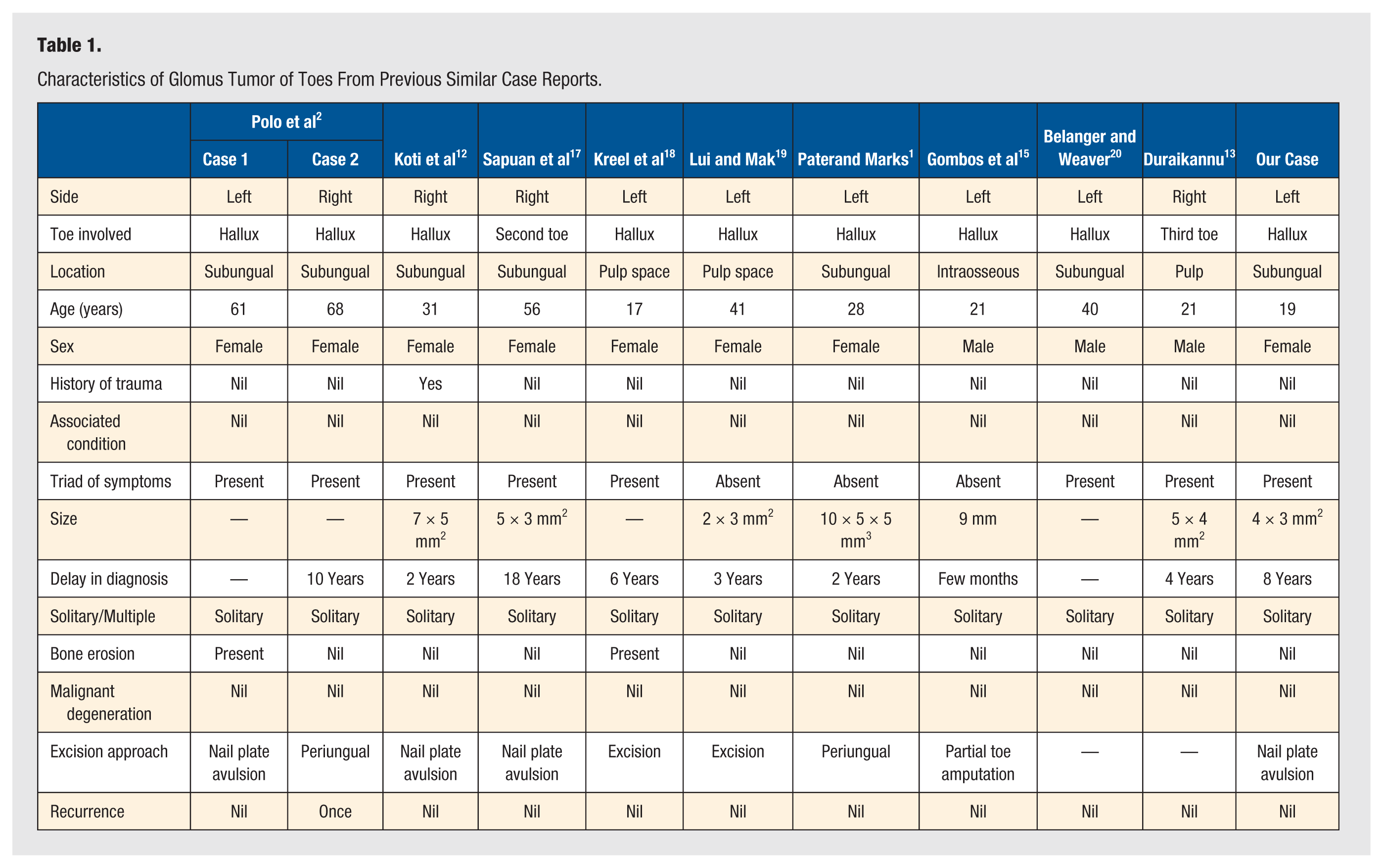
Nevertheless, there are also some notable differences between the 2 forms of presentation. Whereas glomus in the fingers makes up almost 75% of the total, the frequency is much less for toes. This probably could be explained by the relatively lower density of glomus bodies in the foot. However, the presence of a still-hidden compounding factor cannot be ruled out because glomus has even been described at sites lacking glomus bodies. 14 Whatever the reason, the fact that the toe is a rare site does account for a long delay in diagnosis. Often, these tumors are overlooked and diagnosed after years. The average delay, as evident from Table 1, for tumors of the toe nails is approximately 75 months (a few months to 15 years). In their case series of 60 patients Ozdemir et al 21 described a mean time delay of 6 years (ranging from 6 months to 30 years), from the onset of symptoms to surgery, for the hand lesions as well. For the finger variety, any and all digits can be involved. In fact, Al-Qattan 22 described multiple glomus tumors involving all digits, but in the lower extremity, the situation is very different. Not only is the involvement of fourth and fifth toes still unreported, but almost all toe tumors reported have involved the great toe. There is also no report of bilateral occurrence in toe nails yet. Whereas in the upper limb 10% of lesions may be multiple, most occurring in conjuncture with neuro fibromatosis (NF), only Brems et al 23 have reported one such association in the case of a glomus of toes. The prognosis, however, seems to be much better for toe tumors because no recurrence has been reported by any author, as against a low but significant recurrence rate of 11.9% by Conant and Wiesenfeld 24 and 17% by Lin et al 25 for the hand lesions.
Conclusion
Glomus tumor should always be kept in mind as a rare but possible differential, particularly if a young or middle-aged woman presents with a painful lesion of the toes. Although it behaves very much in a manner similar to its counterpart in the subungual areas of the hand, at this unusual location, there is generally a greater delay in diagnosis, even though the prognosis here may be better. Through this article, we want to stress the need for an early diagnosis and treatment, so as to reduce the great morbidity suffered by patients. However, whether glomus tumor of toes needs a separate status like the chemodectomas or the extradigital varieties needs to be further researched, particularly in the context of its exceptionally low frequency and the great predilection it has for the great toe. With the data available, these could only be considered a rarer presentation of the upper-extremity digital glomus tumors.