
Abstract
Hindfoot and distal leg neuropathic fracture collapse secondary to normal pressure hydrocephalus is a very rare clinical pathology. The authors present a case of a 69-year-old woman who sustained a distal tibiofibular fracture that resulted in a recurvatum deformity with idiopathic neuropathy and gait instability on initial presentation. A subtalar and ankle joint arthrodesis was performed achieving rectus alignment of the lower extremity with no postoperative complications. Her neuropathic etiology was negative for common causative factors, including diabetes, infection, nutritional deficiencies, congenital neuropathy, and trauma. Approximately 6 months postoperatively, the patient had persistent bilateral lower extremity weakness with the sensation of her “feet sticking to the floor” on ambulation. A referral to neurology revealed a normal pressure hydrocephalus as a possible etiology for her gait abnormalities and neuropathy. She required a ventriculoperitoneal shunt, with resolved gait disturbance and associated weakness approximately 1.5 years postoperatively.
“Polyneuropathy is a relatively rare association with NPH [normal pressure hydrocephalus], which may further delay appropriate diagnosis.”
Normal pressure hydrocephalus (NPH) is a disorder in which cerebrospinal fluid (CSF) levels are increased leading to enlarged cerebral ventricles while lumbar CSF pressure remains normal.1,2 Brean and Eide 2 found the prevalence of NPH to be 49.3 per 100 00 for people 60 to 69 years of age, increasing to 181.7 per 100 000 for people 70 to 79 years of age. Gait ataxia is often a presenting sign of NPH and manifests with a widened, shuffling or heavy gait.1,3 Some patients report a “magnetic” attraction to the ground with inability to lift their feet. 3 These clinical symptoms, particularly gait abnormalities, improve by approximately 60% after ventriculoperitoneal (VP) shunting. 1
Polyneuropathy is a relatively rare association with NPH, which may further delay appropriate diagnosis. 4 To the best of our knowledge, an association of neuroarthropathy and NPH has not been reported. Charcot’s neuroarthropathy is highly associated with peripheral neuropathy in diabetes leading to severe unstable foot and ankle deformities, ulceration, and decreased quality of life.5-7 The authors present a case report involving a nontraumatic neuropathic distal tibiofibular fracture in a patient with previously undiagnosed NPH.
Case Report
The patient was a 69-year-old woman who presented for initial assessment in February 2013. Eight months prior to consultation, she developed a fracture of the distal leg without any traumatic event. The fracture was treated in a short leg weightbearing cast supplemented with an external bone stimulator for several months’ by another physician prior initial presentation at our clinic. Her past medical history was only significant for hypertension and anxiety with no previous surgical interventions. She denied having diabetes, any distal neuropathy, or congenital neurological disorders. At the time of presentation, she complained of minimal pain; however, she was unable to ambulate more than one city block with complaints of achiness and instability. The patient had a negative history of tobacco use, alcohol use, or other recreational drugs. She had never been treated for any malignancy with chemotherapeutic agents that have been linked to neuropathy. Physical examination revealed an obvious recurvatum deformity to the right lower extremity with instability in the sagittal and frontal planes (Figure 1). Neurological testing demonstrated a distal symmetrical neuropathy with inability to perceive the Semmes Weinstein 5.07 10g monofilament and 128 Hz vibratory testing. Achilles and patellar tendon reflex were intact with full gross motor function in the upper and lower extremity muscle groups. Her Michigan Neuropathy Screening Instrument (MNSI) score was calculated to be 5 out of 10 based on the absent monofilament, absent vibration, and neuropathic deformity. 8 Gait analysis demonstrated an antalgic shuffling pattern with decreased cadence, widened stance, and limp to the affected side.

Clinical photo of patient on initial examination with distal recurvatum of the leg.
Weightbearing plain film ankle radiographs showed a transverse, comminuted tibial fracture with a concomitant displaced spiral fracture of the fibula seen approximately 2 cm proximal to the ankle joint (Figures 2 and 3). There was anterior translation of the foot and the distal tibiofibular fracture demonstrated hypertrophic bone formation surrounding the fracture pattern resulting in a mild varus deformity. The sagittal plane deformity demonstrated a 78° apex with noted recurvatum deformity (Figures 2 and 3). No other fractures or gross abnormalities are seen on plain films. Laboratory testing revealed a normal hemoglobin A1c at 5.6, fasting glucose of 96 mg/dL, albumin of 4.1, total protein of 6.7, prothrombin time 12.9 seconds, international normalized ratio 1.0, partial thromboplastin time 33.6 seconds, platelet of 211 with a normal liver panel. No leukocytosis or abnormal hematologic findings seen on the complete blood count.

Anteroposterior ankle view demonstrated distal comminuted tibiofibular fracture pattern with heterotopic bone formation with varus hindfoot deformity.

Lateral weightbearing view with recurvatum deformity with an approximately 78° oriented distal tibiofibular component.
After 2 months of nonsurgical treatment in CAM boot, the patient continued to have gait “instability and uneasiness with her walker” and consented to surgical intervention. She underwent a tibiotalocalcaneal arthrodesis through a lateral transfibular approach. The subtalar and ankle joints were exposed and an osteotomy of the tibia and fibula was performed to realign the deformity. After joint preparation, a 12-mm diameter by 300-mm length Stryker T2 (Kalamazoo, MI, USA). Intramedullary tibial nail was inserted in retrograde fashion across the fracture site with distal and proximal locking screws placed sequentially. Cancellous bone from the tibial medullary canal and fibula was placed within and around the ankle, subtalar, and nonunion sites for healing augmentation. The remaining fibula was then replaced and fixated with 2 screws. Vancomycin powder was placed in the wound prior to standard layered closure to reduce the rate of surgical site infection. 9 The patient was placed into a short leg cast after postoperative edema had subsided at week 1 and treated with a nonweightbearing cast for 3 months. At 3 months, weightbearing films demonstrated osseous trabeculation across the ankle, hindfoot, and fracture sites. She was placed in CAM boot and instructed to increase weightbearing to toleration while using the boot and cane device. At 6 months, solid bony fusion was appreciated on plain films, and she progressed to normal shoe gear with cane device as needed (Figure 4). She also began a physical therapy program at this time. At 1-year follow-up, she noted continued instability without the use of the boot. The patient was observed as having a shuffled, wide-based gait with marked instability. She was subsequently referred to neurology to work up her gait instability and peripheral neuropathy.

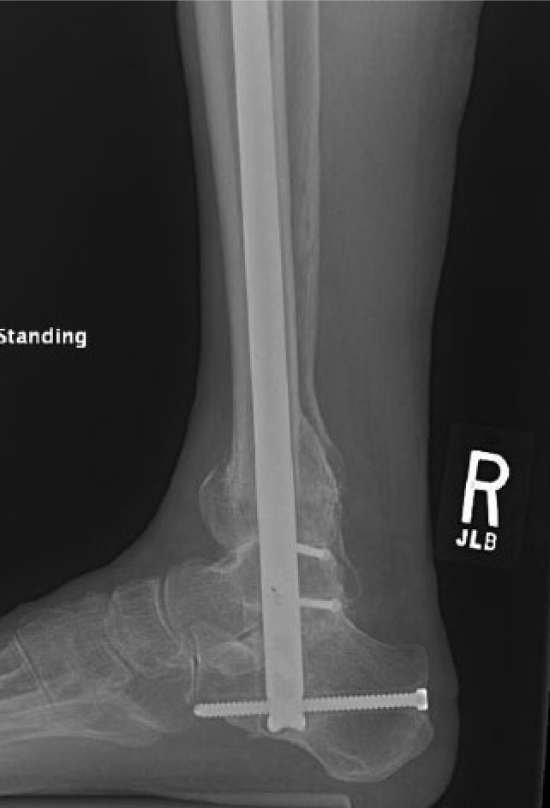
Lateral weightbearing film taken at 6 months postoperatively. Solid ankle and subtalar joint bony fusion with intact hardware and proper perpendicular alignment.
Neurology obtained a brain and cervical magnetic resonance imaging, which revealed morphologic features suggesting the possibility of NPH with ventriculomegaly and gray matter sulci atrophy in addition to flattening of the cervical spinal cord with degenerative changes of C4-C6. She also had complaints of urinary incontinence, with a negative urinary analysis and culture. Electromyographic studies were performed and found to be within normal limits. Neurology felt a spinal cord compression diagnosis would be more consistent with ataxic or “drunk feeling” ambulation, which the patient was not reporting. In addition to the specific gait findings, urinary incontinence with gray matter atrophy, symptoms more favorable for a diagnosis of possible NPH. She subsequently underwent lumbar puncture and CSF drainage with clear and colorless CSF, glucose of 62 and protein of 50 with no resolution of symptoms postdrainage. Ultimately, she had a VP shunt placed, which resulted in marked improvement in her gait. Follow-up 1.5 years after lower extremity reconstruction, she noted improvement in gait and lower extremity alignment was observed (Figures 5 and 6).

Anteroposterior weightbearing film taken at 1.5 years post-operatively with rectus alignment and solid osseous fusion of the hindfoot complex
Lateral weightbearing view taken at 1.5 years post-operatively with a rectus lower leg to hindfoot with complete osseous fusion across the ankle and subtalar joints.
Discussion
First described by Hakim and Adams in 1965, the classic triad of NPH is gait disturbance, urinary incontinence, and dementia. 1 These clinical symptoms are correlated with radiographic and laboratory finding that include ventriulomegaly and normal CSF pressures.1,10 The leading physiologic theory behind NPH is an obstruction of CSF and delayed return in the venous systemic leading to enlargement of lateral ventricles.1,11 NPH can be separated in idiopathic versus secondary etiologies. Known secondary causes include subarachnoid hemorrhage, aneurysms, infectious processes, inflammatory conditions and metabolic bone disease. Idiopathic NPH usually affects those in the sixth and seventh decade of life and diagnosed in the absence of secondary causes. Our 69-year-old female patient had many of the associated symptoms of NPH, mainly presenting with gait apraxia. Apraxia is loss of coordination, manifesting itself in NPH as a shuffling (31%), wide-based gait pattern (50%), and “magnetic” attraction to the ground.1,3,12
Neuropathic arthropathy has been reported as early as 1703 by Sir William Musgrave secondary to complications of venereal disease.5,6,13 Charcot arthropathy, as it was later described, has been associated with several causes including diabetes, leprosy, syringomelia, rheumatoid arthritis, multiple sclerosis, congenital neuropathy, and traumatic injury.6,13 While polyneuropathy linked to NPH is a rare association, Nachnani and Salkind 11 presented a case of a 72-year-old man with generalized weakness of all extremities. Nerve conduction studies demonstrated a demyelinating polyneuropathy that was improved post–lumbar puncture and VP shunt placement. The authors concluded that the polyneuropathy was “superimposed” on the NPH process. 11 Some researchers feel that the existence of both pathologies could be caused by unknown molecules that affect both neurons and CSF fluid. 11 While our patient had normal findings on electromyography, MSNI testing revealed abnormalities consistent with sensory peripheral neuropathy.
Sanders and Frykerg 14 described 5 fracture patterns for the Charcot foot and ankle that report an increased incidence in the midfoot compared with the hindfoot. Complications seen in Charcot’s disease include lower extremity osseous structural collapse with bony fragmentation, gait alternations, neuropathic ulcers, possible amputation, and marked impact on quality of daily life.5-7,10 The anatomical location of the fracture pattern and bony destruction has been shown to occur increasingly in the midfoot, including the tarsometatarsal joints and perinavicular structures (55%) with less incidence involving the hindfoot (9%).14-16 Hindfoot-associated Charcot deformities are inherently less stable are more likely to require surgical intervention to obtain a stable platform for ambulation. 15 However, little is reported on neuropathic leg fractures, with long bone tibial fractures usually associated traumatic injuries. Retrograde tibial intramedullary fixation has been described by several authors as a form fixation for distal tibial fractures.17-19 This form of fixation offers the ability correct gross deformity while acting a stable construct for fracture healing. Our patient did not have any direct ankle joint involvement, but intramedullary nailing as form of correction for severe neuropathic ankle fractures with periarticular involvement has been described as a suitable form of fixation by several authors.17-19 Larger, more rigid constructs have been advocated for neuropathic or Charcot reconstruction to achieve stability and lasting correction. 20 In retrospect, earlier referral to a neurologist should have been considered due to her objective neurologic findings and neuropathic fracture.
Conclusion
To the best of our knowledge, this is the first reported case of neuropathic distal tibiofibular fracture associated with NPH and polyneuropathy. Neuropathic fractures of idiopathic etiology warrant further workup to assess for greater concomitant pathologies that can impede healing or quality of life. Successful reconstruction of this deformity was achieved with a retrograde intramedullary nail as a method of tibiotalocalcaneal arthrodesis.
Footnotes
Declaration of Conflicting Interests
The senior author (DKW) is a consultant for the Stryker Corporation and receives royalties from Arthrex.