
Abstract
Osteomyelitis in children commonly affects long bones such as the femur, tibia, and humerus. There have been relatively few documented studies of osteomyelitis at unusual locations, such as the calcaneus. The objective of this study is to systematically review information on the diagnostic and treatment methods of calcaneal osteomyelitis as well as associated complications. Methods included research database searches using primarily PubMed and EMBASE databases. Results of the review show no clear approach to diagnosis and treatment of calcaneal osteomyelitis in children. Clinical presentation of refusal to bear weight was the most common clinical symptom. Magnetic resonance imaging was 100% diagnostic in studies that used this modality, compared with X-rays, which were 14%-71.4% diagnostic. Blood cultures were diagnostic in 27% to 55% of cases, and erythrocyte sedimentation rate was elevated in 79% to 97% of cases. Methicillin-sensitive Staphylococcus aureus was the most common cultured organism. Treatment involved either antibiotics alone or in combination with surgical debridement/evacuation. Penicillin, penicillin derivatives, cephalosporins, clindamycin, and chloramphenicol were the most commonly used antibiotics, with duration varying from 5 days to 10 weeks. The most common complication was recurrent osteomyelitis.
“Heel pain in children has a vast array of differential diagnoses, which can delay diagnosis and treatment of calcaneal osteomyelitis.”
Introduction
Osteomyelitis is a relatively common infection among the pediatric population and can result from a direct puncture wound or hematogenous spread.1-3 Systemic bacteremia can result in hematogenous seeding of long bones, most commonly the femur, tibia, and humerus, but can also involve unusual sites such as the clavicle, ribs, talus, and calcaneus.4-7 Previous literature has reported the rate of occurrence of calcaneal osteomyelitis to be between 3% and 10%.2,3,5,8-10 Acute hematogenous calcaneal osteomyelitis origin has been reported to occur in 43% to 63% of calcaneal osteomyelitis cases. 1
Heel pain in children has a vast array of differential diagnoses, which can delay diagnosis and treatment of calcaneal osteomyelitis.1,3,6,9,11-14 Systemic symptoms such as fever and leukocytosis are present in most cases of long-bone osteomyelitis but are often absent in calcaneal osteomyelitis, which can prolong correct diagnosis.4,10,11,12,15 Delays in diagnosis can result in several complications, such as growth disturbances, contiguous spread of infection to surrounding joints, and additional surgical interventions.2,10,16
Osteomyelitis of the calcaneus is a relatively rare occurrence, with few documented case reports and minimal, small retrospective reviews completed on the topic. No standard protocol for diagnosis or treatment has been established. There has been no systematic review completed on this topic. The aim of this review is to provide a systematic review of diagnosis, treatment, and outcomes of osteomyelitis involving the calcaneus.
Methods
A comprehensive literature review was completed. All types of studies were considered, including retrospective studies, prospective studies, and case reports. The literature review was completed primarily using PubMed and EMBASE research databases. The references listed in the obtained articles were also reviewed in efforts to include all applicable articles. Keywords included hematogenous, osteomyelitis, calcaneus, and children.
The inclusion criterion for this study was based on information provided within the case report or study. Required information included the following: number of participants, age, method of diagnosis, and method(s) of treatment. Articles were excluded from the review if the required information, as noted above, was not reported. Publishing dates did not exclude articles from the review. Only articles available in English, or with English summaries, were considered for review; see Figure 1.
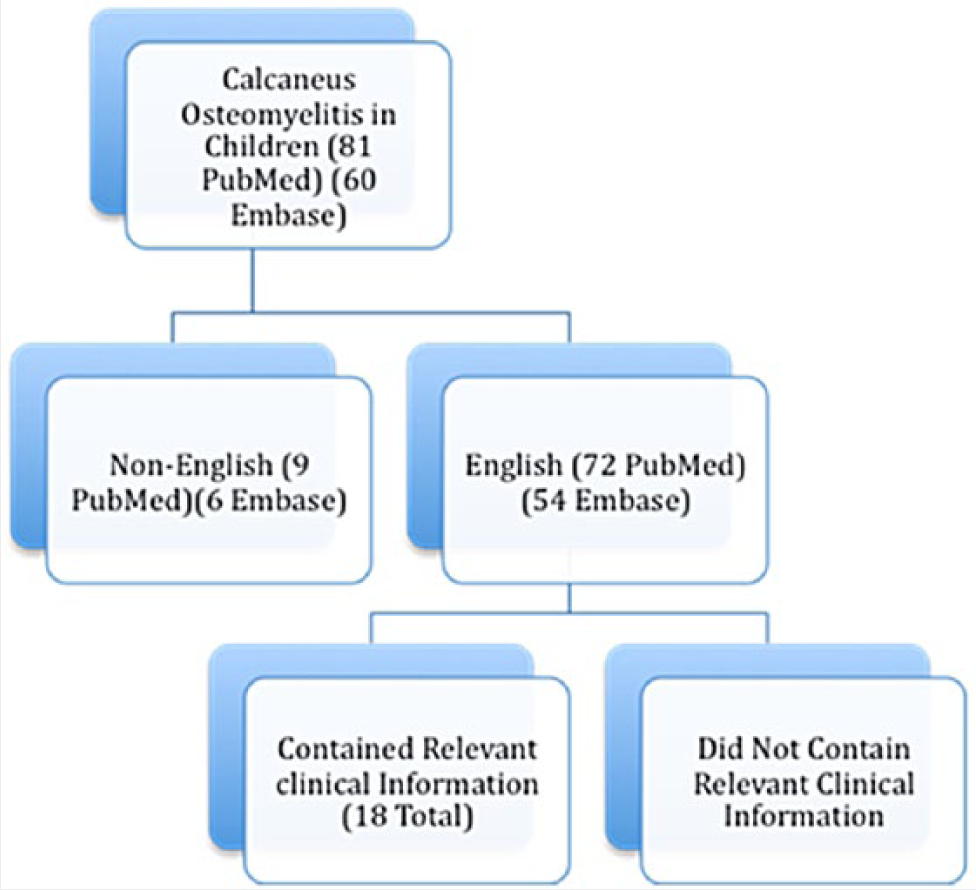
Flow chart of article selection.
The articles were reviewed, and information was collected and compiled into tables. Information of interest included the following: number of cases, number of male and female patients, average age, clinical symptoms, time to diagnosis, method of diagnosis, organisms cultured, treatments given, including antibiotic and surgical options, and complications.
Results
In total, there were 18 articles fitting the inclusion criteria and were included within the review. There were a total of 243 cases of calcaneal osteomyelitis that were reviewed; see Table 1. In total, 142 were male and 97 female. Cases reported by Morrey et al 12 did not include gender and, therefore, did not contribute to the gender distribution. The average age was 7.6 years. Average time to presentation was 17.1 days. Previous injury was reported in 72 of the 243 reported cases (26.9%), and recent illness was reported in 35 of 243 cases (14.4%). Approximately 136 of the 234 (56%) cases did not report a history of a previous illness or injury.
Below are the 18 articles fitting inclusion criteria listed alphabetically by Author.
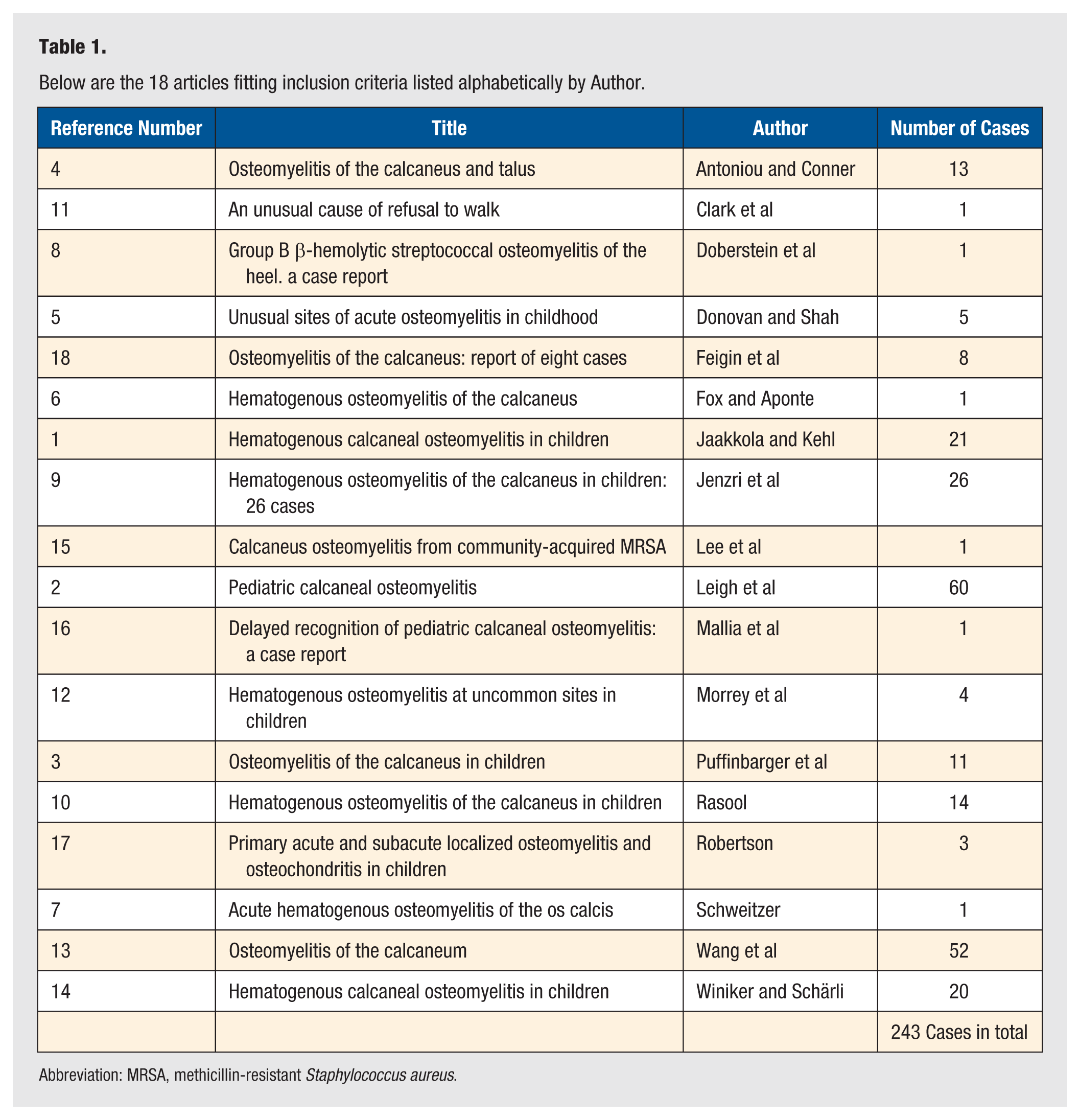
Abbreviation: MRSA, methicillin-resistant Staphylococcus aureus.
Several methods of diagnosing calcaneal osteomyelitis were reported, including clinical symptoms and laboratory testing. Such methods included the following: blood culture, tissue/wound culture, bone biopsy, aspiration, plain X-ray, ultrasound, magnetic resonance imaging (MRI), bone scan, laboratory findings of elevated erythrocyte sedimentation rate (ESR), C-reactive protein, white blood cell count, and clinical presentation. Many of these methods were used in combination to establish a diagnosis.
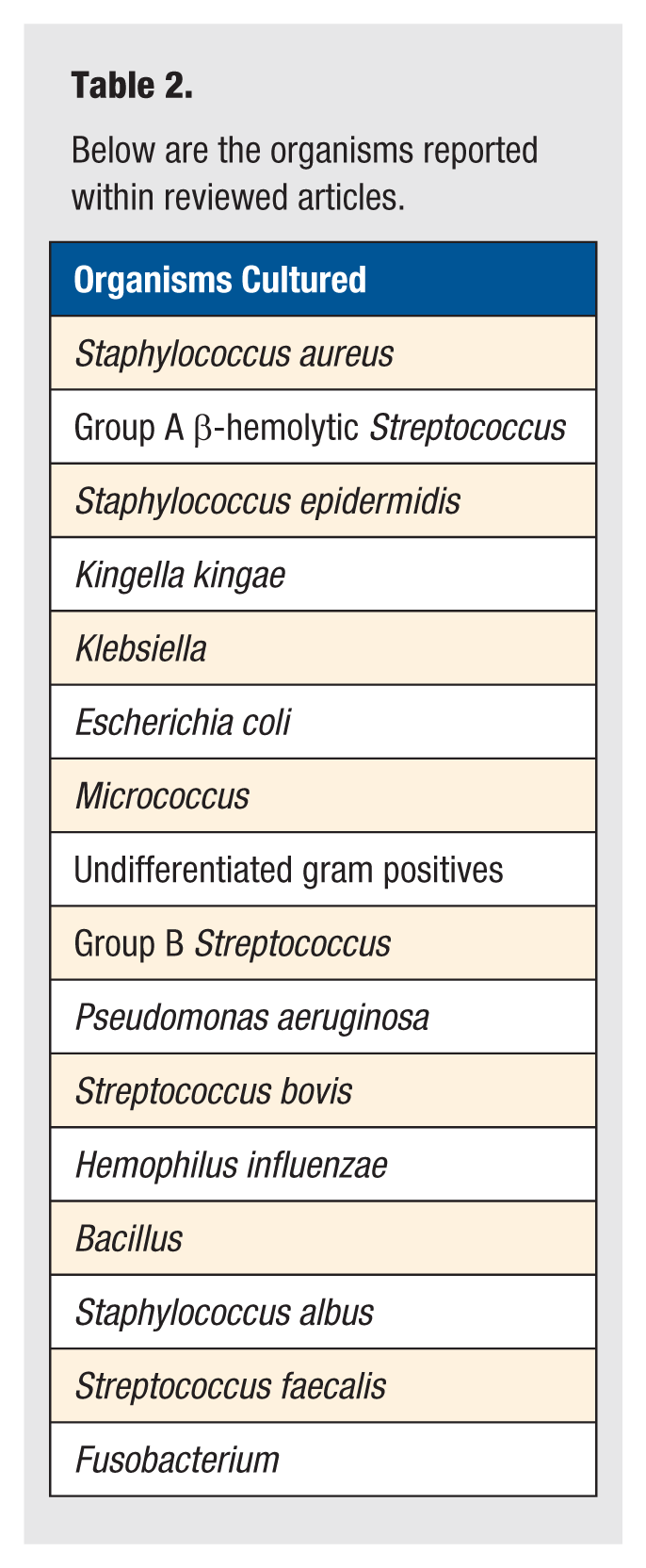
Of the cases reporting blood culture, tissue/wound culture, and bone biopsy, there were several bacteria found; see Table 2. Methicillin-sensitive Staphylococcus aureus was the most common organism reported. There was 1 documented case of methicillin-resistant S aureus (MRSA).
Below are the organisms reported within reviewed articles.
Diagnostic modalities reported in the studies varied significantly; refer to Table 3. ESR elevations were noted in 79% to 97% of cases when considering studies that included more than 10 cases.2,13,14 Blood culture results varied among studies and were positive in 27% to 55% of cases when cultures were obtained.2,14
Summary of the most commonly used diagnostic modalities and the corresponding diagnostic percentage.
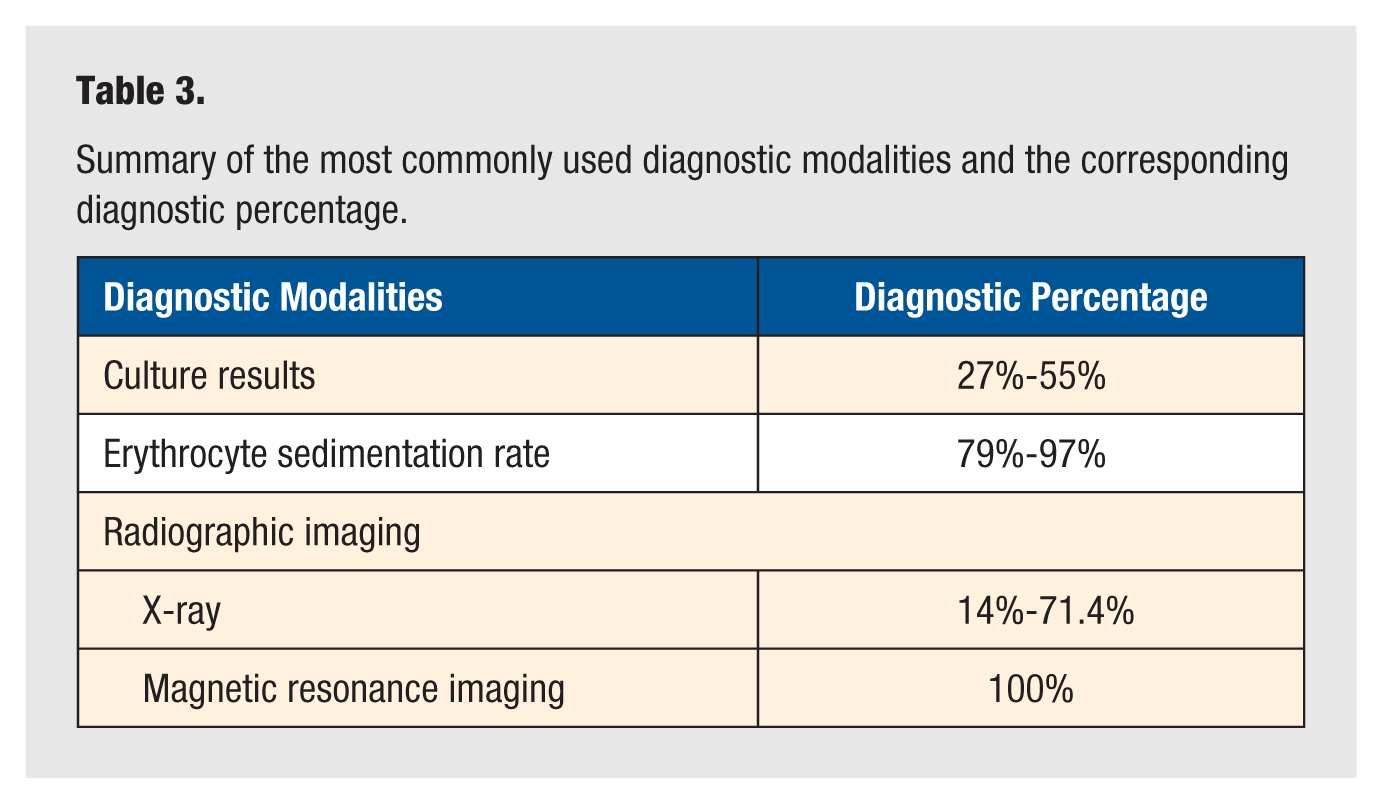
Magnetic resonance imaging was not available as a diagnostic tool in earlier studies but was used in recent studies.2,9,15,16 Plain radiographs indicated diagnostic lesions in 14% to 71.4% of patients, whereas MRI was diagnostic in 100% of patients imaged.1,2,16 Radiographic descriptions of lesions were fairly uniform, noting soft-tissue swelling overlying the lesion and localized bone destruction with surrounding inflammation. 17 Similar initial radiographic findings were reported with the presence of soft-tissue swelling as the most common radiographic feature.7,10,15,17,18
Treatment with antibiotics and surgery were the 2 most common treatment categories. No studies reported methods of treatment that differed from these 2 categories. Treatment with antibiotics was reported as a therapeutic modality in all studies. The use of antibiotic therapy as the sole treatment modality was seen in 30% to 48% of cases reported in some reviews.1,14 The choice of antibiotic, duration of treatment, and route of administration differed with each study. Penicillin, penicillin derivatives, cephalosporins, clindamycin, and chloramphenicol were the most commonly used antibiotics. Intravenous antibiotics were used most often in the inpatient setting, with patients being discharged home on oral equivalents. Duration of antibiotic treatment most commonly ranged from 10 days to 5 weeks. Information regarding antibiotic choice, duration, and route was not reported in references 9 and 12. There was no standard measurement of successful treatment with antibiotics alone; further studies and criteria are needed to establish successful antibiotic treatment.
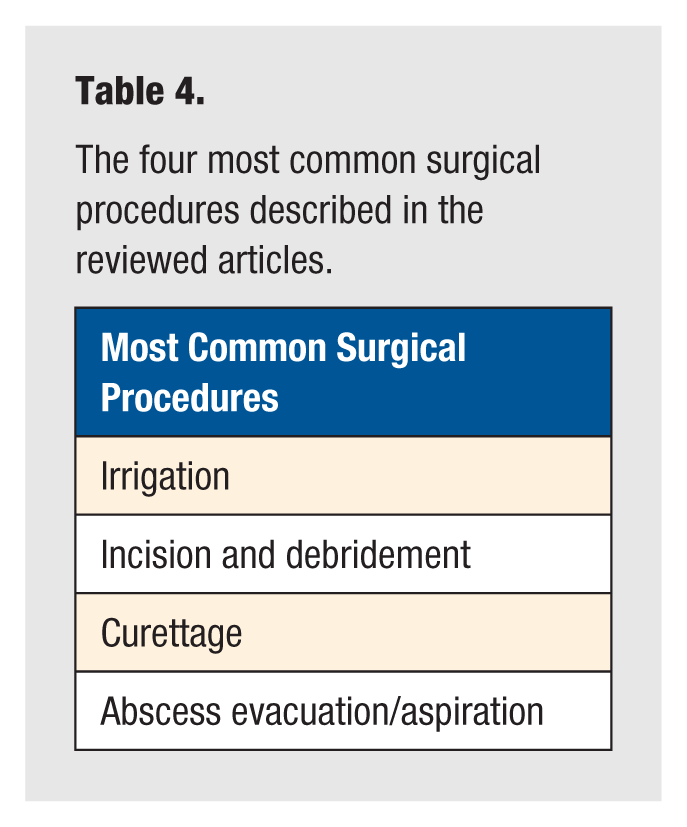
Surgical treatments provided varied greatly and were not performed in all cases. The lowest rate of surgical intervention was reported in 20% of cases, with the highest rate of surgical intervention reported being 100%.2,10 The most common surgical procedures are noted in Table 4. Indications for surgery varied among studies, but the most common indications were continued pain, localized erythema and swelling despite initial treatment, and the presence of abscess or osseous destruction with imaging.
The four most common surgical procedures described in the reviewed articles.
Immobilization was not consistently used as a treatment modality. Winiker and Schärli 14 reported that 100% of patients were placed in plaster casts postoperatively to decrease mobilization and weight-bearing activity. 14 Splinting was occasionally preformed prior to diagnosis because of initial misdiagnosis. 12 There have been no reported benefits to immobilization with calcaneal osteomyelitis.
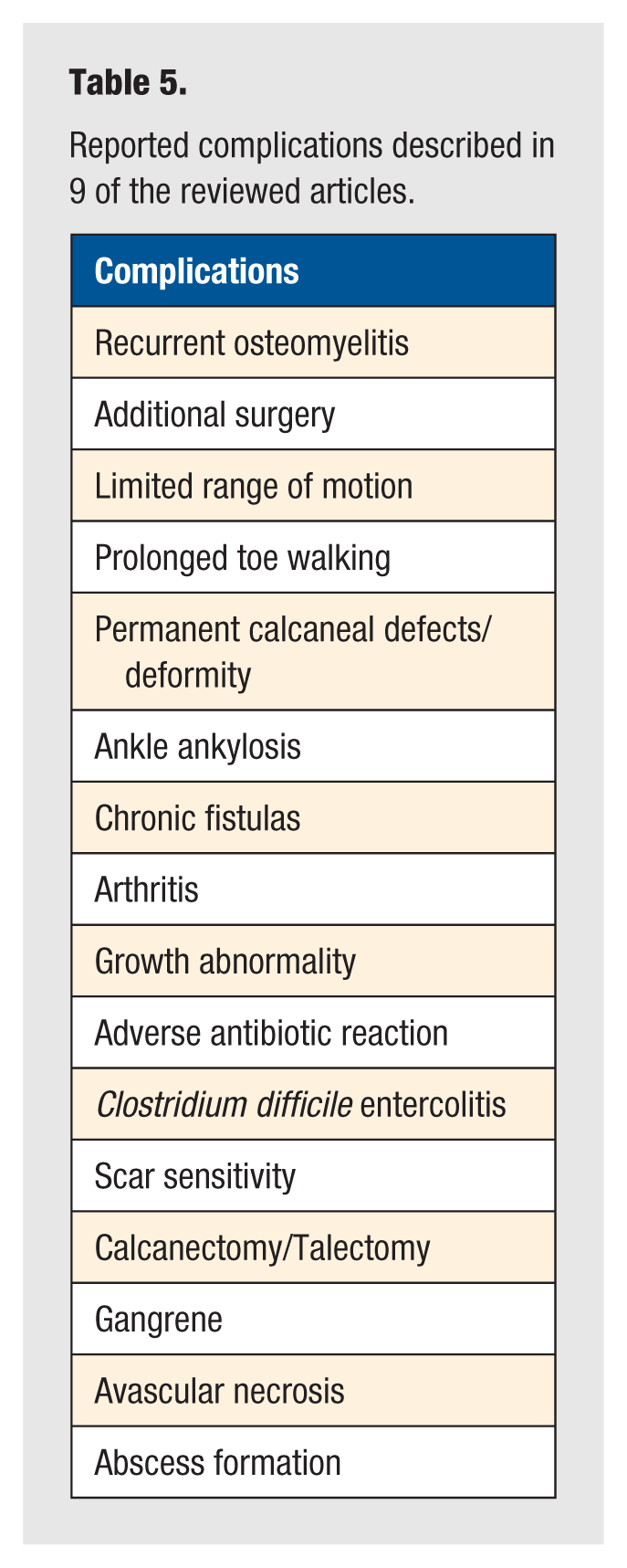
Complications were reported in 9 of the reviewed articles and are listed in Table 5. Recurrence of osteomyelitis was the most common complication and was found in up to 17% of cases. 2 It is unclear based on the information within the articles if there is an association between the duration of antibiotic use and the development of recurrence. One study found ankle ankylosis and limited range of motion in 27% of cases along with chronic fistula formation in 26% of cases. 9 However, these poor outcomes were only reported in patients with delayed presentation/diagnosis, with onset of symptoms on average 17 days before initial evaluation. 9 Growth abnormalities were reported as complications, with incidence ranging from 3.8% to 9%.3,13 Although growth abnormalities were noted, most were asymptomatic and noted only on radiographic imaging.3,13 Complications were most commonly seen in patients presenting 6 to 15 days after onset of symptoms. 10
Reported complications described in 9 of the reviewed articles.
Discussion
Osteomyelitis within the pediatric population is a common occurrence and typically involves the metaphysis of long bones but can involve atypical locations, such as the calcaneus. The calcaneal epiphysis demonstrates vascular anatomy and blood flow that is similar to metaphyseal vasculature, allowing the calcaneus to behave similar to the metaphysis of a long bone.4,9,11 Reduced blood flow in this area of bone can lead to hematogenous spread of bacteria, predisposing the calcaneus to infection without direct trauma. 11
Diagnosis of calcaneal osteomyelitis is often delayed because of an atypical presentation.4,10,11,12,15 Among the literature reviewed, the most common initial presenting symptoms of osteomyelitis of the calcaneus were severe refusal to bear weight, localized tenderness, pain, and swelling. Additionally, history of a prior injury was reported in 26.9% of cases and a recent illness in 14.4%. This information suggests that although prior illness and injury are not present in the majority of cases, they are not uncommon occurrences. If a history of recent illness or injury is present, osteomyelitis of the calcaneus should be considered. The average age of presentation was 7.6 years, with a 58.4% male predominance. A high index of suspicion, given clinical presentation and patient demographics, must be in place for identification and early treatment. The focus must be on an earlier diagnosis in order to improve prognosis and prevent potential adverse complications as outlined in Table 5.
Treatments described in the literature focused on antibiotic therapy and surgical intervention. A variety of surgical techniques were used (see Table 4) in management; however, there is little data to suggest which technique provides the best clinical outcome. Further studies are needed to compare operative techniques. It is unclear which specific antibiotics should be initiated as also the duration and route. The antibiotic choice in many of the studies was initially empirical and then later switched to a pathogen-specific antibiotic based on culture results. The most common organism cultured in all the studies was S aureus and, therefore, would be appropriate to initiate treatment with antibiotics to cover methicillin-sensitive S aureus. Local sensitivities and susceptibilities should be considered if S aureus is suspected. MRSA was found in 1 case, and therefore, empirical treatment against MRSA should not be initiated. 15 In many cases, intravenous antibiotics were given while awaiting surgery and postoperatively, subsequently switching to oral solutions on discharge. No standard of care was recognized. Duration of treatment was also variable, with no specific course reported. Further prospective studies regarding antibiotic regimens need to be completed in order to assess the most beneficial treatment options regarding antibiotics.
Limitations of the study were reflective of the nature of the study. This study was a literature review, containing mostly retrospective studies. No randomized controlled studies were found on this topic.
Osteomyelitis involving the calcaneus has not been well reported in the literature, and no standardized approach to diagnosis and treatment exists. Delaying the diagnosis and treatment can put the patient at risk of developing chronic and debilitating complications. Diagnosis often involves a high clinical suspicion given the history and physical exam and can be supported by elevated ESR, positive blood cultures, and abnormalities noted on X-ray and MRI. An earlier diagnosis can be made with MRI and should be completed in patients if the clinical history and exam is suggestive of osteomyelitis and/or symptoms worsen or do not improve. Initiating conservative treatment with antibiotics early in the disease process may prevent the need for surgical interventions and further prevent complications. Specific guidelines and protocols for the diagnosis and management of hematogenous calcaneal osteomyelitis cannot be determined based on the information gathered in this study because of the vast variation of modalities utilized. However, with the information provided, future prospective studies regarding the diagnosis and management of hematogenous calcaneal osteomyelitis can be completed. Furthermore, the concepts and principles of hematogenous osteomyelitis of the calcaneus in children can be applied to other regions of the lower limb, including the foot and ankle.