
Abstract
Background: Various treatment modalities have been described for Achilles tendinopathy with varying degrees of success. The rationale for the gastrocnemius recession procedure is to decrease the mechanical overload of the Achilles tendon arising from an equinus contracture. Methods: We retrospectively reviewed 25 patients who underwent an isolated gastrocnemius recession procedure at our institution between May 2013 and April 2015 by a single surgeon. Clinical outcome was evaluated on the basis of pain, utilizing visual analog scale (VAS) scores and the Foot Function Index (FFI) by telephonic interview. Student’s t test and one-way analysis of variance were used for statistical analysis. Results: The average age of patients was 53.2 years with an average body mass index of 35.8 kg/m2. The average follow-up was 13.1 months. All 25 patients had a decrease in VAS scores from an average of 8.9 preoperatively to 2.0 at the 6-week visit. The average FFI went from 73.5 preoperatively to 27.4 at final follow-up. Two out of 25 patients had a postoperative sural neuritis with a total complication rate of 12%. Twenty-one of 25 patients (84%) reported total or significant pain relief. Conclusion: The medium-term results of our study suggest that an isolated gastrocnemius recession is a simple, effective, and safe surgical procedure for the treatment of Achilles tendinopathy.
“The pathogenesis of Achilles tendinopathy is not fully understood but histologic findings of diseased tendons indicate a degenerative process . . .”
Achilles tendinopathy is a complex problem that affects many Americans every year. This disorder is somewhat unique in that it affects both athletes and sedentary individuals. One study found that 7% to 9% of high-level runners suffer from Achilles tendinopathy. 1 However, in another study, up to 31% of Achilles tendinopathy patients did not participate in any vigorous physical activities. 2 The pathogenesis of Achilles tendinopathy is not fully understood but histologic findings of diseased tendons indicate a degenerative process rather than an inflammatory process as one might suspect. These findings are well documented and include fibroblast proliferation, perivascular infiltration of lymphocytes, and myofibroblastic changes that affect blood supply. 3 In addition, the tendon undergoes metaplasia to cartilage-like cells as evidenced by increased glycosaminoglycans and type 2 collagen fibers. 4
Achilles tendinopathy can be classified as either insertional (at the distal portion of the tendon where the Achilles inserts on the calcaneus) or noninsertional depending on the area of maximal tenderness. Insertional Achilles tendinopathy is often associated with a bony protuberance on the posterior superior aspect of the calcaneus called a Haglund’s deformity. In this specific form of Achilles tendinopathy, the degenerative process is thought, in part, to be from mechanical compression of the Haglund deformity on the tendon during maximal dorsiflexion. In the present study, we included both forms of Achilles tendinopathy as they are likely different variations of the same underlying disease process and are treated using the same protocol at our institution.
Methods
We first obtained institutional approval from our hospital review board. We then retrospectively reviewed 25 patients who had undergone an isolated gastrocnemius recession procedure in the past 3 years for the diagnosis of Achilles tendinopathy. This patient sample represented a consecutive, single surgeon sampling. After the diagnosis, every patient underwent at least 3 months of conservative treatment, including casting or walking boot immobilization, typically with a heel wedge insert to relieve stretch on the Achilles. The patients were also given oral anti-inflammatories, started on home stretching programs, and/or physical therapy. Every patient had a positive Silfverskiöld test, which tests for isolated gastrocnemius contracture. The Silfverskiöld test was considered positive if the patient had increased ankle dorsiflexion with the knee flexed compared to the knee fully extended, all while maintaining the transverse tarsal joint locked in inversion. For comparison, the patients were split up into noninsertional Achilles tendinopathy, insertional Achilles tendinopathy with the presence of a heel spur, and insertional Achilles tendinopathy without a heel spur. Paired Student’s t test was used to compare preoperative with follow-up values of visual analog scale (VAS) scores and Foot Function Index (FFI). One-way analysis of variance was used on the stratified group to assess for differences between the 3 groups.
Surgical Technique
After failing nonoperative management, each of the 25 patients decided to undergo a gastrocnemius recession. The procedure was performed under general anesthesia with the patient positioned supine. A tourniquet was placed on the upper thigh and inflated to 300 mm Hg after administration of prophylactic antibiotics and leg exsanguination. We then made a 3-cm longitudinal, posteromedial incision centered at the musculotendinous junction. The paratenon was identified and incised using a scalpel. The gastrocnemius tendon was then encountered and separated from the soleus muscle using blunt dissection with a Freer elevator or the surgeon’s finger. The tendon was then completely transected utilizing Coker clamps to reach across the entire medial to lateral width of the tendon and to bring the tendon into the field of view through the skin incision. Care was taken to ensure the sural nerve was not adhered to the surface of the tendon during the transection. After complete transection, the fascia and paratenon were left open and the skin was closed with 4-0 monocryl (MONOCRYL [poliglecaprone 25] suture, Ethicon, Gargrave, England) and staples. Postoperatively, patients were placed in a walking boot with instructions for full weightbearing as tolerated in the boot. They were all seen at 2 weeks postoperatively for a wound check and staple removal. At that time, the patients were instructed to switch over to supportive shoes as tolerated based on pain control. All patients were taught a home stretching program to maintain their range of motion and then seen again at 10 to 12 weeks postoperatively.
Pain was evaluated using a VAS from 0 (no pain) to 10 (maximal pain) at 2 weeks, 6 weeks, 3 months, 6 months, and 1 year postoperatively. The FFI was obtained preoperatively and at the last follow-up visit as an outcome measure for pain and functional improvement. Subjective assessments such as patient satisfaction and whether or not they would recommend a friend undergo the same procedure were also obtained.
Results
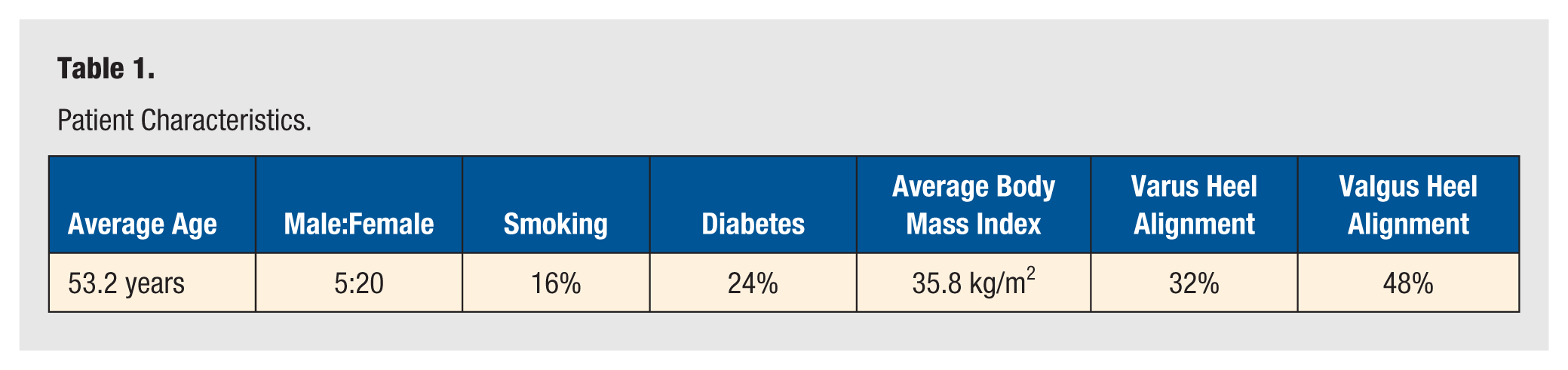
Our series included 25 patients with an average age of 53.2 years (range, 29-88 years) and was composed of 20 females and 5 males (see Table 1). Average body mass index was 35.8 kg/m2 (range, 27.4-53.1 kg/m2). Hindfoot alignment was based on weightbearing physical examination and radiography and was determined to be varus in 8 patients, valgus in 12 patients, and neutral in 5 patients. Average follow-up time was 13.1 months (range, 3-25 months). In all, 16% (4/25) of our patients were smokers and 24% (6/25) were diabetic.
Patient Characteristics.
Sixteen of the patients were deemed to have insertional Achilles tendinopathy due to having maximal tenderness to palpation at the insertion of the Achilles tendon and up to 2 cm proximal. Five patients had maximal tenderness at or near the musculotendinous junction and were deemed to have noninsertional Achilles tendinopathy. The remaining patients (4) had both insertional and noninsertional complaints. Fourteen of the 20 patients (70%) with insertional complaints had evidence of calcific changes to the tendon on radiography. In addition, 8 of the 20 patients (40%) had a Haglund’s deformity. Interestingly, of the patients with insertional complaints and no Haglund’s deformity, 91.7% (11 out of 12 patients) had calcific changes to the Achilles tendon at the insertion site. However, only 32.5% (3 out of 8 patients) of patients with insertional Achilles tendinopathy and a Haglund’s deformity had calcification to the tendon. This difference was statistically significant (P = .022).
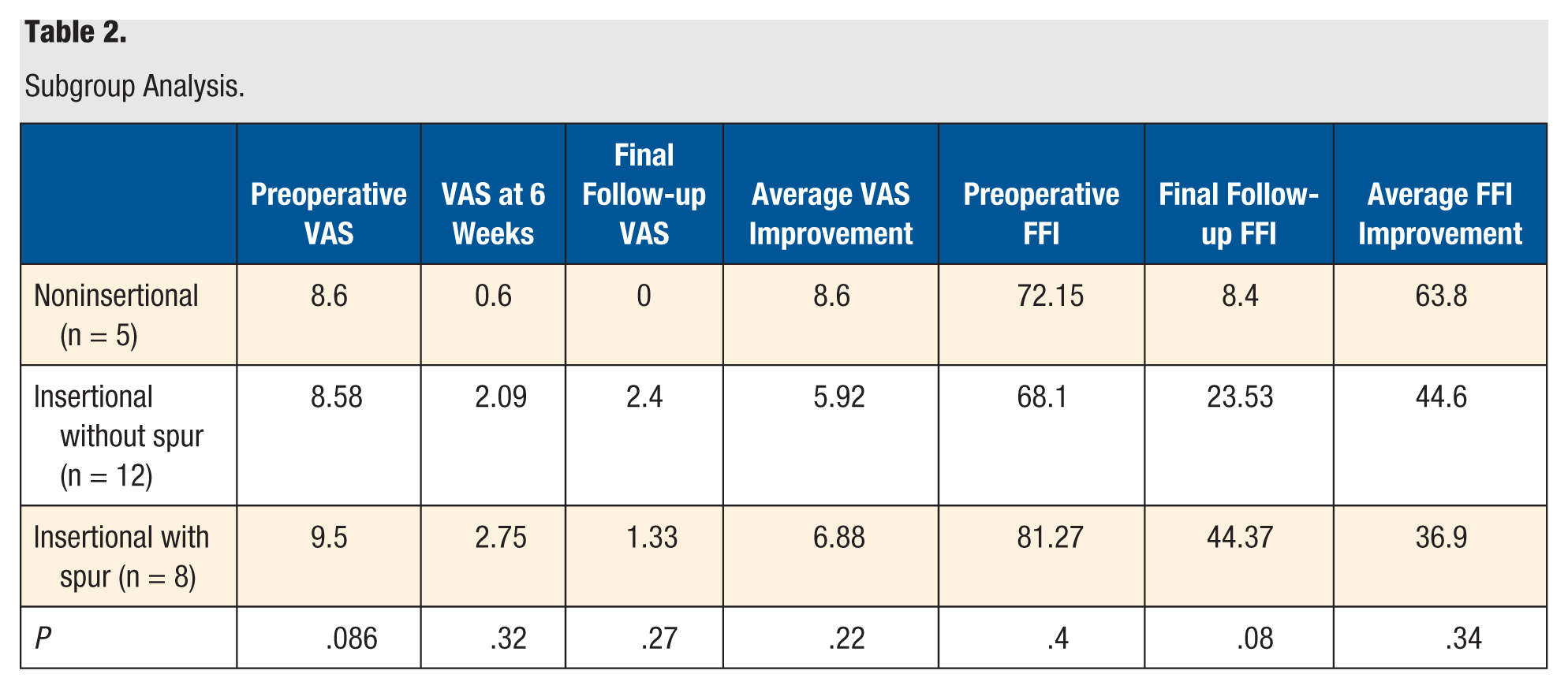
VAS showed marked improvement postoperatively. VAS prior to surgery averaged 8.9 and improved to an average of 2.4 at the 2-week visit and 2.0 at the 6-week visit (P < .001 for both, 2 and 6 weeks) (see Figure 1). While both groups improved, the VAS improvement was slightly better at the 6-week visit in the noninsertional group compared with the insertional group (average VAS improvement of 8.0 vs 6.58, P = .08). FFI also improved significantly from preoperative values to final follow-up (see Figure 2). The average FFI prior to surgery was 73.5 (range, 32.9-100) and the average at final follow up was 27.4 (range, 0-74.7) (P < .001). When the patients were stratified into 3 groups based on the point of maximal tenderness and the presence or absence of a Haglund’s deformity, the VAS and FFI improvements showed no statistical significance between the groups (see Table 2). Twenty-one of 25 patients (84%) reported total or significant pain relief. Twenty of the 25 (80%) patients said they would recommend the surgery to a friend.
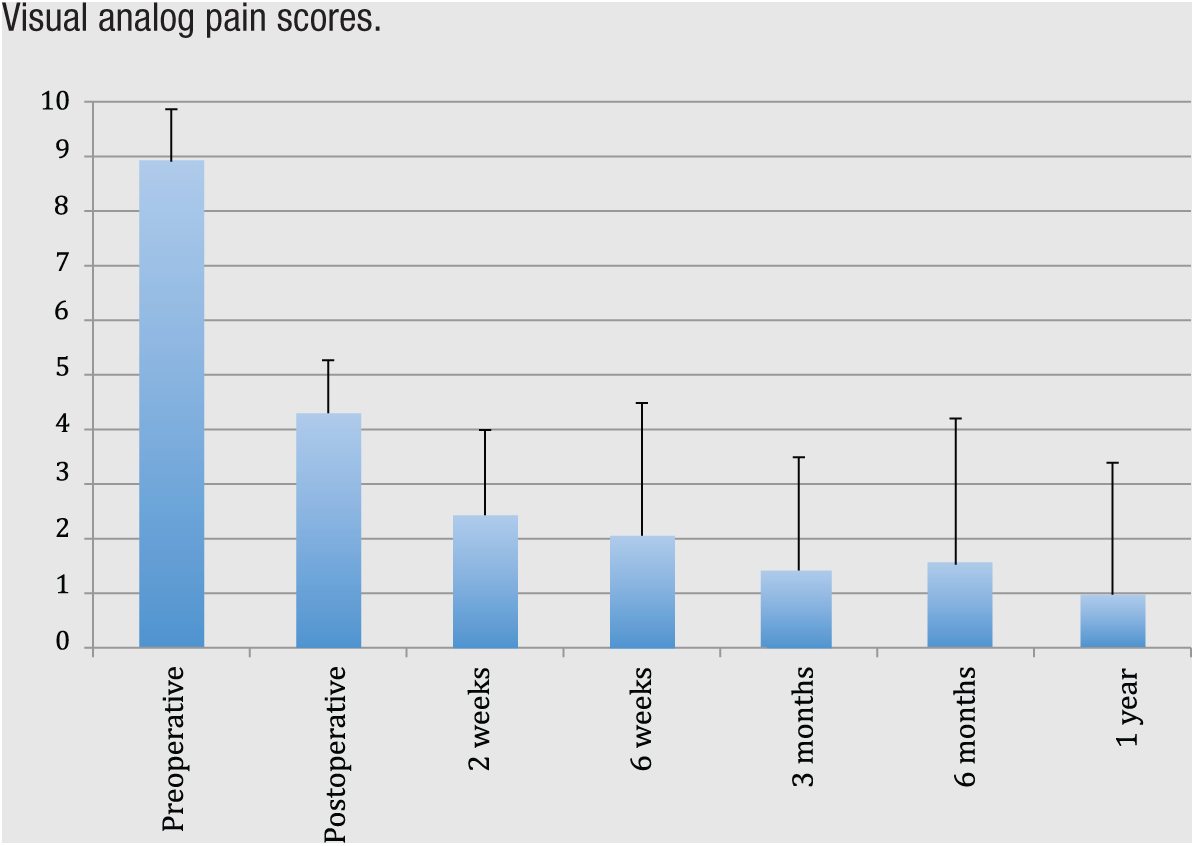
Visual analog pain scores.
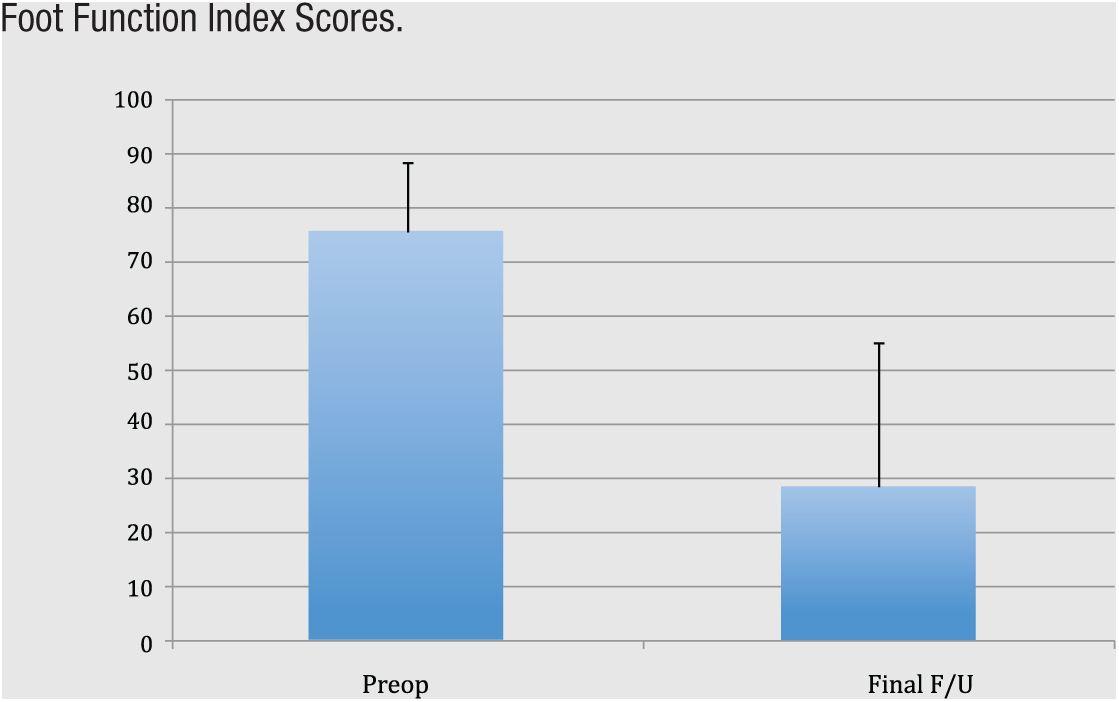
Foot Function Index Scores.
Subgroup Analysis.
There were a few complications to report. Although there were no infections or delayed wound healing that required a repeat surgery, 2 patients did develop sural neuritis postoperatively. Both these patients had documented neuropathy prior the surgical procedure. Another patient (an 88-year-old woman) suffered a distal Achilles tendon rupture at 4 months postoperatively that was treated conservatively in a cast without further complication. Whether or not this was related to her operation is unknown. The combined complication rate in our series was 12% (3 out of 25).
Discussion
Achilles tendinopathy is a common condition that can often be successfully treated without operative intervention. However, there are instances when prolonged nonoperative treatment does not provide the patient with adequate relief of symptoms. Studies have shown a failure of conservative management in 24% to 45% of patients despite up to 6 months of treatment.5,6 When surgery is required, traditional open debridement techniques showed good efficacy but were fraught with complications as Paavola et al 7 reported a 11% early complication rate in 432 patients treated with operative management with 9 out of every 10 complications being a wound healing issue.
One commonly held theory for why Achilles tendinosis develops is that a chronically elevated tension within the tendon leads to microtears and inadequate healing response. Arya and Kulig 8 showed 15% higher strain in tendinopathic Achilles tendons when compared with controls using real time ultrasonagraphy and dynamometry. Child et al 9 reported a statistically significant increase in Achilles tendon-aponeurosis strain in those patients with tendinopathy as compared with control patients. In a 2010 review article on tendinopathy by Magnusson et al, 10 the authors report that for the first 18 to 36 hours after exercise, there is a net negative collagen balance in response to mechanical loading of the fibroblasts such that without appropriate rest, the tendon is continually losing collagen. This would thereby leave the tendon vulnerable to injury. In the case of a sedentary patient who has a chronically tight gastrocnemius muscle, this same mechanical loading of the fibroblasts is occurring all the time. Given there is never any “rest” from this loading, the tendon cannot heal itself or replace the collagen that has been lost. It follows therefore, that if we can surgically lengthen the gastrocnemius, we remove this constant strain on the tendon and give the fibroblasts a chance to heal the tendinopathic tissue.
There have been many recently published case series on using a gastrocnemius lengthening procedure to treat both insertional and noninsertional Achilles tendinopathy. Duthon et al 11 found a near 93% satisfaction rate in treating 14 patients with chronic noninsertional Achilles tendinopathy with isolated gastrocnemius lengthening. Tallerico et al 12 reported a 91% satisfaction rate in their series of 11 patients with insertional Achilles tendinopathy with 14-month follow-up. Gurdezi et al 13 showed that 6 out of 9 patients were satisfied after a proximal medial gastrocnemius release at an average of 2.5-year follow-up. Interestingly, the noninsertional tendinopathy group showed better results than the insertional group with a statistically significant better improvement across both mean Victorian Institute of Sports Assessment–Achilles (VISA-A) and mean AOFAS scores. Kiewiet et al 14 reported a mean decrease in visual pain scale from 7.3 preoperatively to 1.0 at final follow-up in 7 patients with mean follow-up of 34.6 months. Last, Maffulli and Buono 15 found that 15 of 18 patients self-reported good or excellent outcomes after undergoing a release of the medial head of the gastrocnemius for chronic Achilles tendinopathy. Despite the good results that have been published using this strategy, the current literature is comprised of small, retrospective case series and a recent systematic review found only a Grade Cf level of recommendation on using isolated gastrocnemius recession for the treatment of noninsertional Achilles tendinosis and grade I (for insufficient evidence) when using this surgery for insertional Achilles tendinosis. 16
Gastrocnemius recession procedures have been linked with several different postoperative complications. A recent study by Molund et al 17 in 2014 found a self-reported 38% complication rate in a patient sample of 73 patients. This number is extremely high in comparison with most reports; however, only 8/73 (11%) patients had a significant complication. In their study, they report a 4% infection rate, a 2.7% incidence of nerve injury and 1 patient each (1.4%) with deep vein thrombosis, pulmonary embolism, and complex regional pain syndrome following the surgery. The other “complications” were subjective complaints such as continued pain, swelling or leg cramps. In contrast, Maffulli and Buono 15 reported no wound healing complications or sural nerve injuries in their series of 18 patients with an overall complication rate of 0%.
Another concern surrounding gastrocnemius-lengthening procedures is the possible long-term consequences of weakness in the operative limb. Nawoczenski et al 18 showed equivalent peak torque values in their series of 13 patients with mean follow-up of 18 months in the postsurgical limb using the contralateral limb as a control. However, the operative group did report some difficulty with walking uphill, climbing stairs and with running and jumping despite 84.6% of the patients reporting satisfaction with the surgery. Another recently published article reported no functional difference between the limb that underwent a gastrocnemius recession and the nonoperative limb when compared in a validated test battery of 5 explosive-type exercises. 19
Our study represents a relatively large patient sample and is in agreement with the aforementioned studies that gastrocnemius recession is an excellent surgical option for both insertional and noninsertional Achilles tendinopathy. Twenty-four of the 25 patients showed improvement in both VAS and FFI with a statistically significant drop in the mean values of both metrics. In addition, when comparing the subgroups, our results indicate that all patients with Achilles tendinopathy including those with noninsertional as well as insertional Achilles tendinopathy with or without a Haglund’s deformity improved with this surgery. With intermediate-term follow-up, our patient series had 3 total complications, with a complication rate of 12%. The 2 patients who developed sural nerve neuritis both had a history of neuropathy prior to the surgery and was likely due to traction from the retractors. The other complication may have been unrelated to the gastrocnemius recession, as this procedure should theoretically lower the rate of Achilles rupture given the decrease in tensile loads across the tendon post surgically. Even with our complication rate being 12%, this compares favorably with the reported complication rates seen with open surgical debridement, despite having a considerably higher average body mass index and a higher proportion of patients with diabetes than the prior studies.
This study has several limitations. Although 25 patients is a relatively large sample given the paucity of large-cohort studies in this area, once these patients were split into the subgroups, the sample size became quite small. This makes the lack of statistically significant differences between the groups harder to interpret. In addition, the outcome measure used in our article, the Foot Function Index or FFI, is not a validated outcome score for Achilles pathology. Unfortunately, we do not have Victorian Institute of Sport Assessment–Achilles questionnaire scores for this patient group.
Conclusion
Isolated gastrocnemius recession is both a safe and effective surgical option for patients with chronic Achilles tendinopathy that is refractory to nonoperative management. The authors believe it to be an excellent treatment for both insertional and noninsertional Achilles tendinopathy with minimal risk for severe complication or long-term sequelae.