
Abstract
Background. Morton’s neuroma is a common cause of forefoot pain. Outcomes of conservative therapy are mixed and many patients undergo operative intervention. Radiofrequency ablation has recently gained favor as a treatment option, although the optimal regime is unknown. This study investigates the effectiveness of 2 versus 3 cycles of radiofrequency ablation for the treatment of Morton’s neuroma. Methods. We surveyed a cohort of patients with Morton’s neuroma who had progressed to radiofrequency ablation after failed conservative treatment. Patients received either 2 or 3 cycles of radiofrequency ablation by a single surgeon. We assessed patients based on their change in numerical pain rating scale, symptom improvement, complications, and progression to surgical excision through a series of telephone interviews. Outcomes between the 2 treatment arms were compared by parametric tests. Results. Twenty-eight patients were included in the study. Eighteen patients with 21 neuromas received 2 cycles and 10 patients with 11 neuromas received 3 cycles. Mean time of follow-up was 12.9 months. Overall, 88% of patients were either very or moderately satisfied with their outcome. In patients who received 2 cycles mean numerical pain scores decreased from 7.9 ± 1.1 to 3.4 ± 2.4 postprocedure. Three patients progressed to operative excision. In patients who received 3 cycles, numerical pain scores decreased from 8.0 ± 1.0 to 1.5 ± 2.0 postprocedure. One patient progressed to operative excision. Patients who received 3 cycles had reduced medium-term pain postoperatively compared with 2 cycles (3.4 ± 2.4 vs 1.5 ± 2.0, P = .011). Conclusion. Radiofrequency ablation provides a high rate of patient satisfaction in the treatment of Morton’s neuroma with few side effects. It appears that 3 cycles may be superior to 2 cycles but a randomized controlled trial will be required to confirm these results.
“RFA [radiofrequency ablation] appears to be efficacious for the treatment of morton’s neuroma; however, the optimal treatment regime is unknown.”
Morton’s neuroma is a common and often debilitating cause of forefoot pain. It was first described by the chiropodist Lewis Durlacher in 1845 as a neuralgic affectation that attacks the plantar nerve between the third and fourth metatarsal bones 1 and later in 1876 by Thomas G. Morton, who attributed the pain to pathology of the fourth metatarsophalangeal joint and nerve irritation from the neighbouring bony structures. 2 The source of the problem is now generally accepted to be an entrapment neuropathy of the plantar digital nerve as it travels deep to the transverse intermetatarsal ligament within the web space. 3 It is characterized histologically by endoneural hyalinization, intraneural fibrosis, endoneural sclerosis and edema, and demyelination. The presence of demyelination may be the most relevant finding as outlined in a study that showed no difference in histological changes between asymptomatic control and patients with Morton’s neuroma, with the exception of demyelination. 3
Nonoperative management consists of activity modification, use of appropriate footwear with lower heels and broader toe boxes, orthotics, and local web space injections of local anesthetic and corticosteroid. 4 Outcomes of conservative therapy are mixed. 5 Nerve decompression or neurectomy is reserved for those with recalcitrant pain not relieved by nonoperative measures. Neurectomy is often considered the mainstay of operative treatment; however, its clinical effectiveness has been questioned. Good outcomes may be found in up to 85% of patients.6-8 However, in a large retrospective study by Womack et al, 9 the authors found that 40% of patients had poor results 10 years postneurectomy. Poor outcomes are usually due to either postoperative scarring or recurrence of symptoms, thought due to the formation of a terminal stump that results from neural regeneration. 5 Additional surgery does not appear to improve the outcome in patients with recurrence of symptoms. 10 Surgical alternatives to nerve decompression and neurectomy are evolving and include endoscopic decompression, cryogenic denervation, and radiofrequency ablation. 5
Radiofrequency ablation (RFA) is a less invasive treatment option that is not currently widely used. A radiofrequency generator impresses a voltage on an electrode tip to create an electric current. This current acts on charged ions within the tissue creating an oscillatory motion and friction heating. Thermocoagulation necrosis of biological tissue usually occurs when the tissue temperature exceeds 70°C. 11 This technology is used commonly in the treatment of solid organ tumors, trigeminal neuralgia, cardiac arrhythmias, and facet joint osteoarthritis. RFA appears to be efficacious for the treatment of Morton’s neuroma12-15; however, the optimal treatment regime is unknown. This study examines the effect various cycles of RFA have on patient reported outcomes.
Materials and Methods
We performed a retrospective review of all patients who had Morton’s neuroma treated with RFA between February 2011 and February 2015. Inclusion criteria were a clinical diagnosis of Morton’s neuroma, ultrasound or magnetic resonance imaging diagnosis when clinical diagnosis was not clear, 2 failed corticosteroid injections at least 6 weeks prior to RFA treatment, and no prior foot surgery. The Greenslopes Research and Ethics Committee have granted ethics approval for this study.
All procedures were performed as a day case in the operating theatre. A radiofrequency lesion generator was used to perform the ablation (Neurotherm NT 1100, Neurotherm, Wilmington, MA, USA). Repeat history and examination was performed prior to the procedure, and the point of maximal tenderness was marked. General anesthesia or intravenous sedation was then administered. A grounding pad was attached to the patient. Under aseptic technique, a 22-gauge cannula was introduced to the point of maximal tenderness through a dorsal approach approximately 2 cm proximal to the skin web fold in the appropriate intermetatarsal space. The needle and cannula sheath were passed deep to the transverse metatarsal ligament and then the guide needle was removed and the radiofrequency electrode inserted. The current (milliamperes) was increased until the tissue temperature surrounding the electrode tip reached 90°C. The electrode was left for 4 minutes, and this was repeated over 2 or 3 cycles. A combination of 0.75% ropivacaine and 1 mL betamethasone was then injected into the procedure site. Patients were discharged the same day and allowed to weight bear as tolerated.
We assessed patients prior to radiofrequency ablation and at least 4 months postprocedure. They were assessed based on a numerical pain rating scale (NPS), patient satisfaction, complications and progression to surgical excision through a series of telephone interviews. Data were prospectively entered into a spreadsheet (Microsoft Excel) and later transferred to SPSS (version 22.0) for Macintosh for further analysis. Patient characteristics and outcomes were examined in relation to number of cycles of RFA; 2 or 3. Continuous variables were compared with Mann-Whitney U test and nominal variables with Fisher’s exact test.
Results
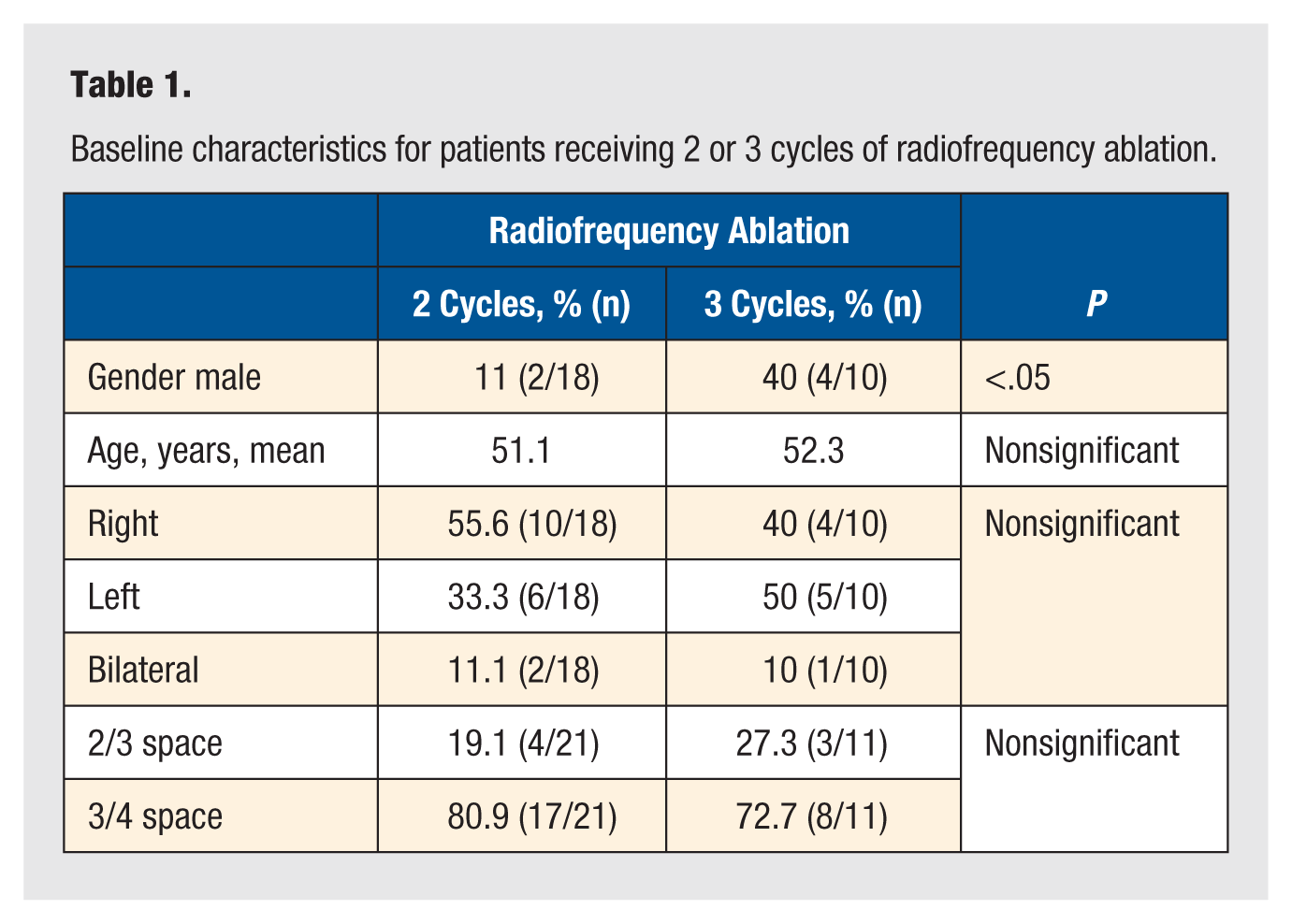
Twenty-eight patients with 32 neuromas were included in the study. There was 79% (22/28) females and mean age of 51 years. Twenty-one neuromas (n = 18) received 2 cycles and 11 neuromas (n = 10) received 3 cycles of RFA. Baseline characteristics were similar between groups, except for gender (see Table 1). Mean time of follow-up was 12.9 months (range 5-26 months). Overall, 87.5% of patients were either very or moderately satisfied with their outcome. There were no identified complications in our cohort.
Baseline characteristics for patients receiving 2 or 3 cycles of radiofrequency ablation.
Patients who received 3 cycles had significantly reduced midterm pain postoperatively compared with 2 cycles (3.4 ± 2.4 vs 1.5 ± 2.0, P = .011, see Table 2). In patients who received 2 cycles numerical pain scores decreased for all but 3 patients, with the mean numerical pain score falling from 7.9 to 3.4 postprocedure (P < .01). Of the 21 neuromas, 14.2% had complete resolution of symptoms, 71.4% had partial relief and 14.2% had no benefit. Three patients progressed to operative excision. In patients who received 3 cycles, numerical pain scores decreased for all patients except one, with the mean numerical pain score falling from 8.0 to 1.5 postprocedure (P < .01). Of the 11 neuromas, 27.2% had complete resolution of symptoms, 63.6% had partial relief, and 9.1% had no benefit. One patient progressed to operative excision.
Primary outcomes for patients receiving 2 or 3 cycles of radiofrequency ablation.
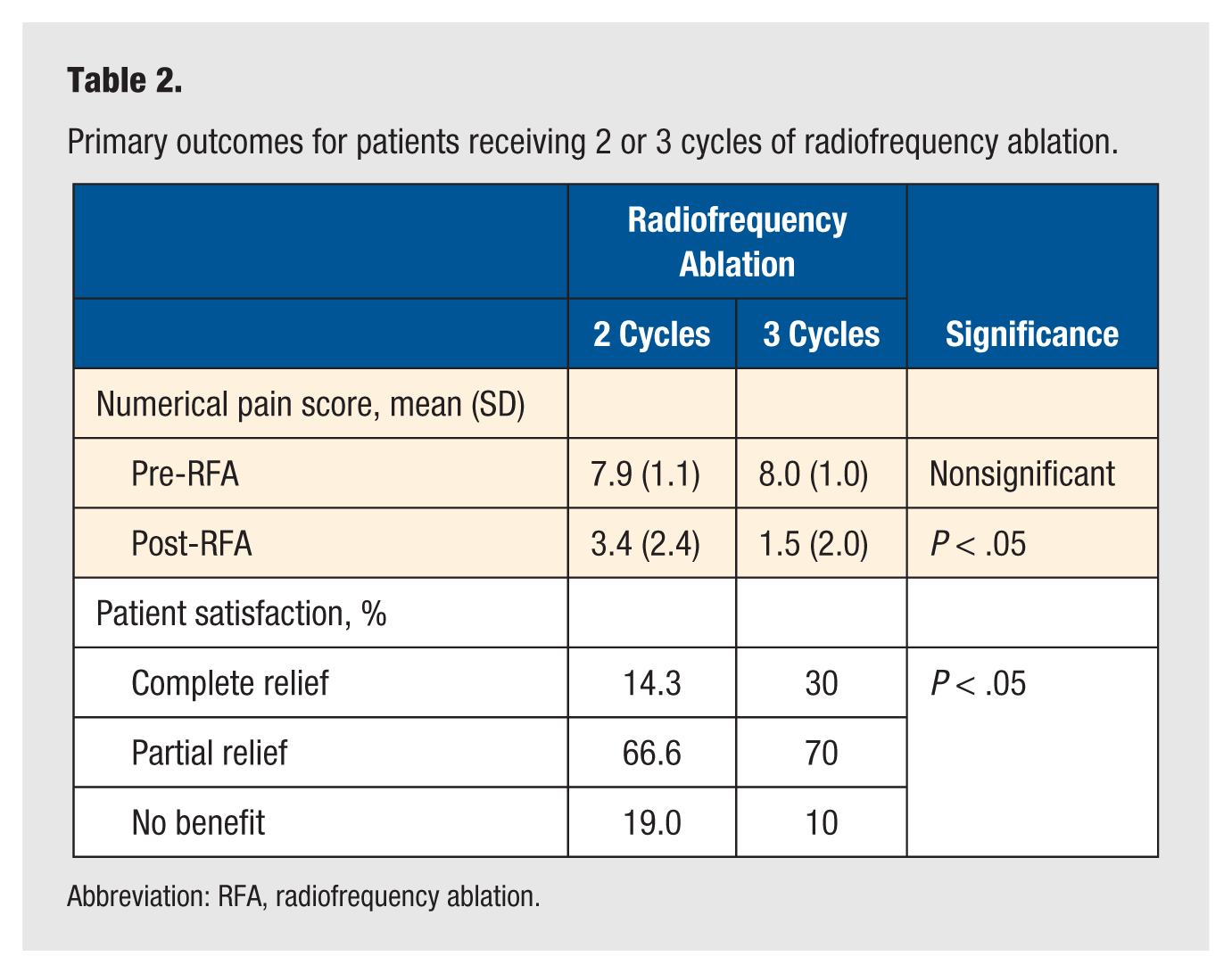
Abbreviation: RFA, radiofrequency ablation.
For the 4 patients who had no relief of symptoms, the mean numerical pain score decreased from 7.5 ± 1.7 to 7.0 ± 2.0. All these patients proceeded to neurectomy. Postneurectomy, 1 patient experienced complete relief and 3 had partial relief of symptoms.
Discussion
This study demonstrates good results using RFA for the treatment of Morton’s neuroma at medium-term follow-up. In addition, it appears that patients who had 3 cycles had better outcomes than patients who had 2 cycles.
The results from our study show a high patient satisfaction rate in both groups. At a mean 13 months following RFA, we found 87.5% of neuromas had either complete or partial relief of symptoms and only 12.5% of neuromas went on to operative excision. Previous studies examining the use of RFA for Morton’s neuroma have shown similar results. Finney et al 12 explored percutaneous electrocoagulation in 1989 and claimed a 70% reduction in the number of patients progressing to surgery. Recently, Genon et al 13 reviewed 37 patients for an average of 10.6 months and found that 86.8% of patients were satisfied, with only 28.9% proceeding to open neurectomy. Moore et al 14 examined 29 patients and found 83% had complete relief of symptoms at an average of 13 months post-RFA. Ultrasound-guided RFA has also been reported. Chuter et al 15 examined 25 patients for 6 months post–ultrasound-guided RFA and found improvement in symptoms in more than 85% of cases with only 10% progressing to excision.
At a mean 13 months, patients who received 3 cycles had reduced medium-term pain and post-RFA compared with patients who received 2 cycles (see Table 1). In addition, neuromas receiving 3 cycles had a trend toward increased likelihood of complete relief (27.2% vs 14.2%, nonsignificant) and reduced likelihood of progressing to neurectomy (9.1% vs 14.2%, nonsignificant). We are unaware of any study examining the effectiveness of variable regimes for the treatment of Morton’s neuroma with RFA. Most studies used a single cycle for between 90 and 180 seconds.13,14 We hypothesize that dividing the treatment doses may increase the intraneural coagulation, thereby improving outcomes without increased local complications.
Pulsed RFA is an option using higher voltage of radiofrequency applied intermittently to allow the elimination of heat. This decreases tissue temperature potentially minimizing neurodestruction. A recent case report shows good results when pulsed was combined with continuous radiofrequency ablation for Morton’s neuroma. 16 When treating trigeminal neuralgia this protocol showed fewer side effects while maintaining efficacy. 17 Therefore, further research investigating continuous versus pulsed RFA is required.
The long-term effectiveness of RFA is currently unknown. The process of thermocoagulation in RFA seals the epineurium around the proximal part of the nerve thus preventing neural stump formation. 11 As neural regeneration is thought to be the cause of recurrence, we would expect the risk of recurrence after radiofrequency to be low. Long-term follow-up is required to explore this further.
The pathogenesis of Morton’s neuroma is hypothesized to be related to nerve entrapment and irritation of the intermetatarsal nerve as it passes under the deep intermetatarsal ligament. As a result, many authors recommend surgical decompression for cases that fail nonoperative treatment. 18 Alternatively, patients are often offered a neurectomy with the expectation of good short- to medium-term results. However, adverse events following neurectomy are common and include postoperative infection, or problematic incisional tenderness. 5 Recurrence of symptoms may occur in up to 20% of patients and the treatment of recurrence is difficult. 6 Postneurectomy, patients may be limited in their weightbearing capacity and normally require 2 weeks off work or study to allow their wounds to heal. In contrast, RFA can be done as a day procedure with minimal recovery time, minimal scarring, and a low risk of bleeding or infection. Skin burns are a known complication of RFA, with an incidence of 0.1% to 3.2% for second-/ third-degree and 5% to 33% for first-degree burns in the treatment of liver tumors. 19 We had no skin complications in our cohort and could not find any reported cases of cutaneous thermal necrosis in the literature for the treatment of Morton’s neuroma. Higher current RFA may attribute to an increased risk of skin burns. Burns are normally found along the leading edge of the grounding pad site, and therefore correct size and orientation of these pads are essential.
Steroid injections are a commonly used nonoperative treatment, with all of our patients trialing 2 injections prior to RFA. We are unaware of any randomized controlled trials outlining their clinical effectiveness in the treatment of Morton’s neuroma. A cohort study on ultrasound-guided steroid injections found complete pain relief in 28% of neuromas 9 months after treatment, although 31% required surgery. 20 It appears that the benefit of steroid injections may be short term with pain levels returning to baseline at 12 months. 21 Adverse events can include the development of debilitating fat pad atrophy, skin thinning, or hyperpigmentation. 22
We found no difference in the outcomes of second versus third web space neuromas. Excision of neuromas from the second web space is associated with poorer outcomes 9 and previous RFA studies have shown greater efficacy in third web space neuromas. 13 Outcomes are likely related to probe placement and intermetatarsal head distance. Other studies have included the use of ultrasound 15 and fluoroscopy 14 to increase the accuracy of RFA probe placement.
This study shows that RFA can provide good patient satisfaction. This is the first study examining various RFA protocols and patient reported outcomes. It appears that a protocol with 3 cycles may be superior to 2 cycles. This study is limited by short follow-up and small sample size. A randomized controlled trial is required to examine long-term outcomes of RFA, and comparison with simple neural decompression or neurectomy. RFA is a useful addition in the treatment algorithm for Morton’s neuroma. It has the potential for complete pain relief and rapid recovery with minimal complications.