
Abstract
Background: The proposed benefit of total ankle replacement (TAR) over ankle fusion is preserved ankle motion, thus we hypothesized that an increase in range of motion (ROM) is positively correlated with validated patient-reported outcome measures (PROMs) in individuals receiving TAR. Methods: Patients undergoing TAR at a single academic medical center between 2007 and 2013 were evaluated in this study. In addition to a minimum of 2-year follow-up, complete preoperative and postoperative outcome measures for the Foot and Ankle Disability Index (FADI), Short Musculoskeletal Function Assessment (SMFA) Bother and Function Indices, Visual Analog Scale (VAS), and 36-Item Short Form Health Survey (SF-36) were requisite for inclusion. Standardized weightbearing maximum dorsiflexion and plantarflexion sagittal radiographs were obtained and previously described ankle and foot measurements were performed to determine ankle ROM. Results: Eighty-eight patients met inclusion criteria (33 INBONE, 18 Salto-Talaris, 37 STAR). Mean time to final ROM radiographs was 43.8 months (range 24-89 months). All aforementioned PROMs improved between preoperative evaluation and most recent follow-up ( P < .01). Final ankle ROM was significantly correlated with postoperative FADI, SF-36 Mental Component Summary (MCS), SMFA Bother and Function Indices, and VAS. Additionally, dorsiflexion was positively associated with FADI, SF-36 MCS, and SMFA Function ( P < .05) but plantarflexion had no such influence on outcomes. No differences were identified with subset stratification by prosthesis type, fixed versus mobile-bearing design or etiology. Conclusion: In this TAR cohort with prospectively collected outcomes data, radiographic sagittal plane ankle motion was positively correlated with multiple PROMs. Disease-specific and generic health-related quality of life PROMs demonstrated improvement postoperatively in all domains when evaluating final total range of motion. Patients who undergo TAR for end-stage osteoarthritis with improvement in ROM demonstrate a direct correlation with improved patient-centric metrics and outcome scores.
“Preservation of ankle motion may improve quality of life as evidenced by patient-reported outcome measures (PROMs).”
Total ankle arthroplasty (TAR) offers patients with end-stage ankle arthritis a chance at preserved ankle range of motion (ROM) and near-physiologic gait mechanics at intermediate- and long-term follow-up.1-5 Though TAR and arthrodesis have both yielded positive results for pain control and patient satisfaction,6,7 gait patterns in TAR more closely resemble the biomechanics seen in patients unaffected by arthritis than those of their arthrodesis counterparts. 3 These findings have been validated associating a more normalized gait in patients with overall greater dorsal motion in the sagittal plane. 8 Furthermore, a cadaveric study showed that fixed and mobile-bearing total ankle prostheses enable more physiologic joint mechanics than ankle arthrodesis. 9 Additionally, TAR enables a higher level of function on uneven surfaces, hills, stairs, and inclines. 10 The proposed benefit of TAR over ankle fusion is preserved ankle motion. Preservation of ankle motion may improve quality of life as evidenced by patient-reported outcome measures (PROMs).
Improvements in PROMs are seen in multiple TAR patient demographics, including those with relatively high body mass index (>35 kg/m2), diabetes, ipsilateral subtalar arthrodesis, and even active smokers.11-14 PROMs represent increasingly important instruments for effect measurement as the United States embraces new reimbursement models and relies on PROMs for gauging value.15,16 This comes with the caveat that PROMs must be validated to justify their utility.
To our knowledge, sagittal plane ROM in TAR has not been evaluated as a correlate of validated outcome measures. The purpose of the present study is to compare postoperative sagittal plane ROM to validated disease-specific and generic health-related quality of life (HRQoL) scores in fixed and mobile-bearing TAR prostheses. We hypothesized that absolute ROM is positively associated with validated PROMs in individuals undergoing TAR.
Methods
Patient Enrollment
A retrospective review of all patients enrolled in our prospectively collected TAR database between May 2007 and October 2013 was conducted. Eighty-eight patients met inclusion criteria (33 INBONE I/II, 18 Salto-Talaris, 37 STAR). Mean time to final ROM radiographs was 43.8 months (range 24-89 months). Further details on TAR database collection and contents have been previously reported.1,17-20 Patients were suitable for inclusion in this study if they met the following criteria: underwent a TAR with a fixed-bearing Salto-Talaris (Integra LifeSciences Corporation, Plainsboro, NJ), mobile-bearing STAR (Stryker, Kalamazoo, MI), or fixed-bearing INBONE I or II (Wright Medical Group, Inc, Arlington, TN) prosthesis, final weightbearing ROM radiographs were obtained at a minimum of 2 years after surgery and complete preoperative and 2-year postoperative validated PROMs were recorded. Exclusion criteria included those who had prior fusion procedures, revision total ankle arthroplasty, subsequent revision procedures or missing PROM data. This study was approved by the institutional review board at our medical center.
Radiographic Measures
Plantarflexion and dorsiflexion lateral radiographs of the foot were obtained in a standardized fashion at a 1-m distance from the x-ray source and included the entire foot and ankle as previously described by Coetzee et al. 21 Maximum dorsiflexion was achieved by having the patient bend the ipsilateral knee and take one step forward with the contralateral foot, simulating one stride-length. Similarly, maximum plantarflexion films were obtained by having the patient take one step back with the contralateral foot, simulating one stride-length (Figure 1). To maintain standardization, plantarflexion and dorsiflexion views were obtained with both feet flat on the ground. ROM was subsequently measured using previously published radiographic landmarks. 22 The specific measurements obtained are as follows and can be seen in Figure 2:
Total motion arc (Figure 2A) was defined as the arc of motion that the tibia traveled with the ground acting as a constant for measurement purposes. The mechanical axis of the tibia in plantar flexion (obtained by a bisecting line of the tibia) was subtracted from the same line in dorsiflexion lateral radiographs. 23
Talar motion (Figure 2B) was defined as the arc of motion that the talus moved with respect to the ground in a similar fashion to that above. Measurements were obtained irrespective of tibia motion utilizing the Cobb angle function with one arm parallel to the footplate and the other approximating the axis of the talus. The long axis of the talus was obtained by taking the perpendicular to a line drawn across the widest aspect of the talar head along the articular surface. The motion arc was defined by subtracting the Cobb angle in plantarflexion from the Cobb angle in dorsiflexion.
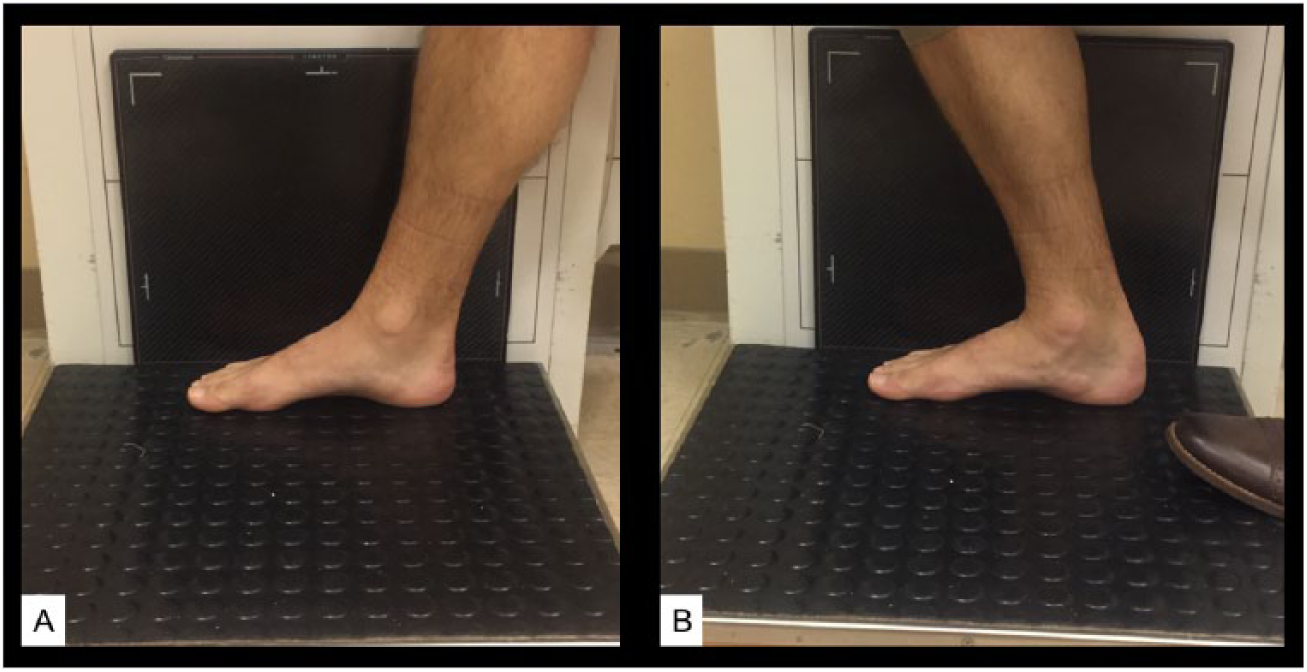
Technique of obtaining range of motion radiographs with patient in maximum plantar flexion (A) and dorsiflexion (B).
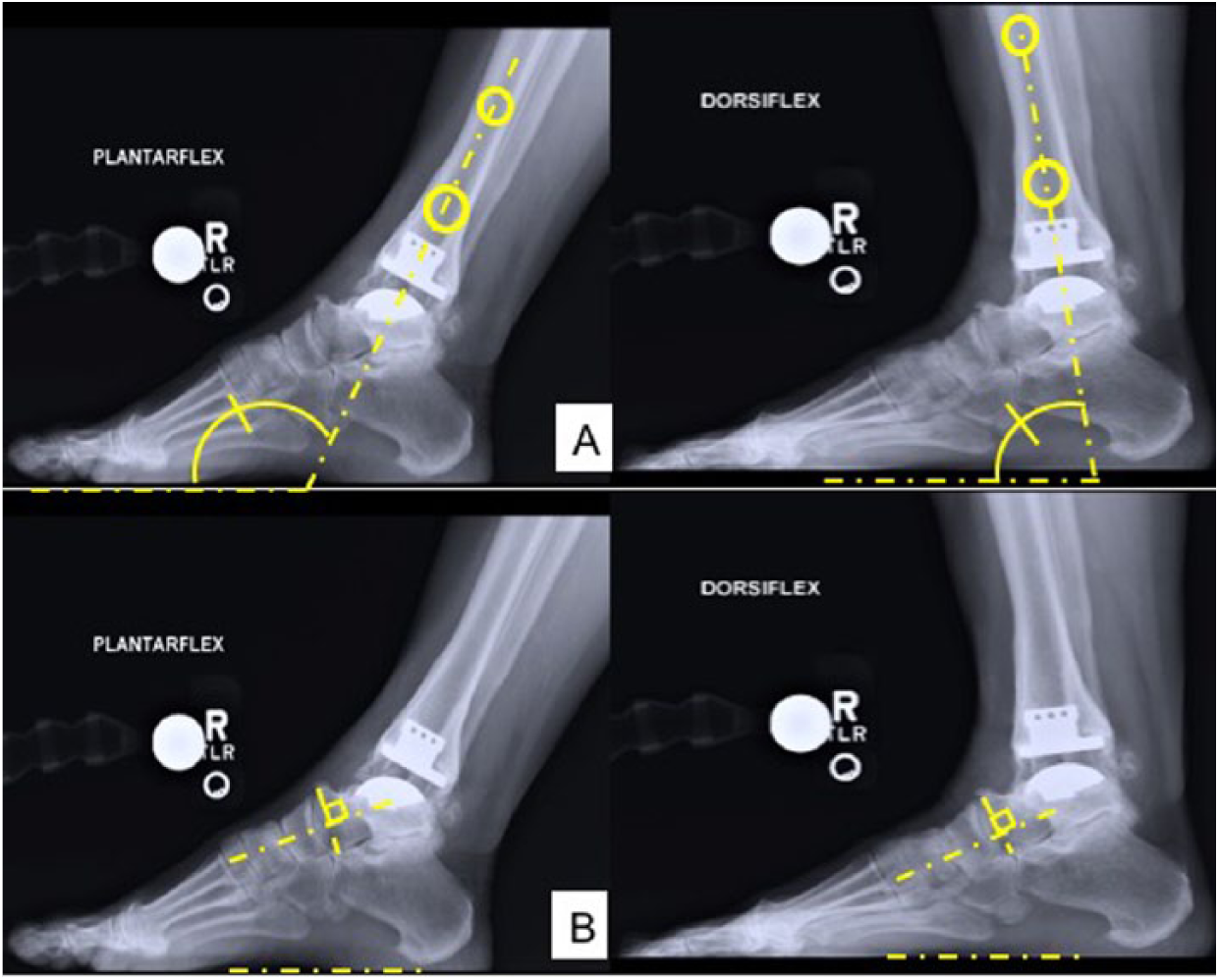
Total motion arc (A) and talar motion arc (B).
The actual ankle motion through the prosthesis was calculated by subtracting the total arc of talar motion (measurement 2) from the total motion arc (measurement 1).
Patient-Reported Outcome Measures
Complete preoperative and postoperative validated outcome measures were requisite for inclusion in the study. The Foot and Ankle Disability Index (FADI), Short Musculoskeletal Function Assessment (SMFA) Bother and Function Indices, Visual Analog Scale (VAS), and 36-Item Short Form Health Survey (SF-36) were used as they are validated functional outcome scores. Patients were excluded if their only complete preoperative PROM was the nonvalidated AOFAS (American Orthopaedic Foot and Ankle Society) score as analysis of this score was not deemed as value adding.
Statistical Analysis
A correlation sample size estimation was calculated based on an α level of .05, power of 0.90, and r of 0.5 for moderate correlation, yielding a minimum of 38 patients necessary to conduct the investigation. Data were normally distributed with a skewness of 0.2 and visual assessment of quantile plots. A priori statistical plan consisted of 1-way analysis of variance for categorical predictors and continuous outcomes, followed by 2-tailed Student’s t test with Tukey’s test if significance detected in analysis of variance. Dichotomous predictors and continuous outcomes were analyzed for significance with 2-tailed Student’s t test.
An interobserver reliability test was completed for ROM measurement validation. The 3 observers were asked to measure all radiographic angles and 4 weeks later, 20 of the measurements were repeated; intraobservor intraclass correlation coefficients (ICCs) were found to range from 0.953 to 0.994 for ROM metrics. Interobservor ICCs ranged from 0.827 or 0.914 for the same parameters. Statistical analysis was performed by an individual with an advanced degree in biostatistics. JMP 12 Pro software (SAS Corporation, Cary, NC, USA) was used for analysis.
Results
Etiologies were identified as primary osteoarthritis in 28 patients (32%), posttraumatic in 51 patients (58%), rheumatoid arthritis in 7 patients (8%), and avascular necrosis in 3 patients (3%); there were no differences in preoperative PROMs when stratified by etiology. No difference was detected in mean total ankle ROM between INBONE I/II (38.0° ± 9.7°), Salto-Talaris (38.0° ± 12.0° degrees), and STAR (37.7° ± 14.1°) prostheses (P = .98). Similarly, no difference in mean total ankle ROM was identified when stratified by fixed (38.0° ± 10.5°) versus mobile-bearing (37.7° ± 14.1°) prosthesis types (P = .92). Among all TAR patients, ankle plantarflexion and dorsiflexion averaged 24.0° ± 9.0° and 13.9° ± 6.7° from neutral, respectively.
All aforementioned PROMs improved between preoperative evaluation and most recent follow-up (P < .01). Final ankle ROM was significantly correlated with postoperative SF-36 Mental Component Summary (MCS), SMFA Bother and Function, and VAS (Table 1). Final ankle ROM was correlated with final FADI (P < .01) and with the magnitude of improvement in FADI (P = .03). Additionally, dorsiflexion was positively associated with FADI, SF-36 MCS, and SMFA Function (P < .05) but plantarflexion had no such influence on outcomes. No differences were identified when adjusted for prosthesis type, fixed versus mobile-bearing design, or etiology in multivariate regression analysis.
Preoperative to Postoperative Differences in Patient-Reported Outcome Measures (PROMs) and Correlation of Plantarflexion (PF), Dorsiflexion (DF), and Range of Motion (ROM) With PROMs. a
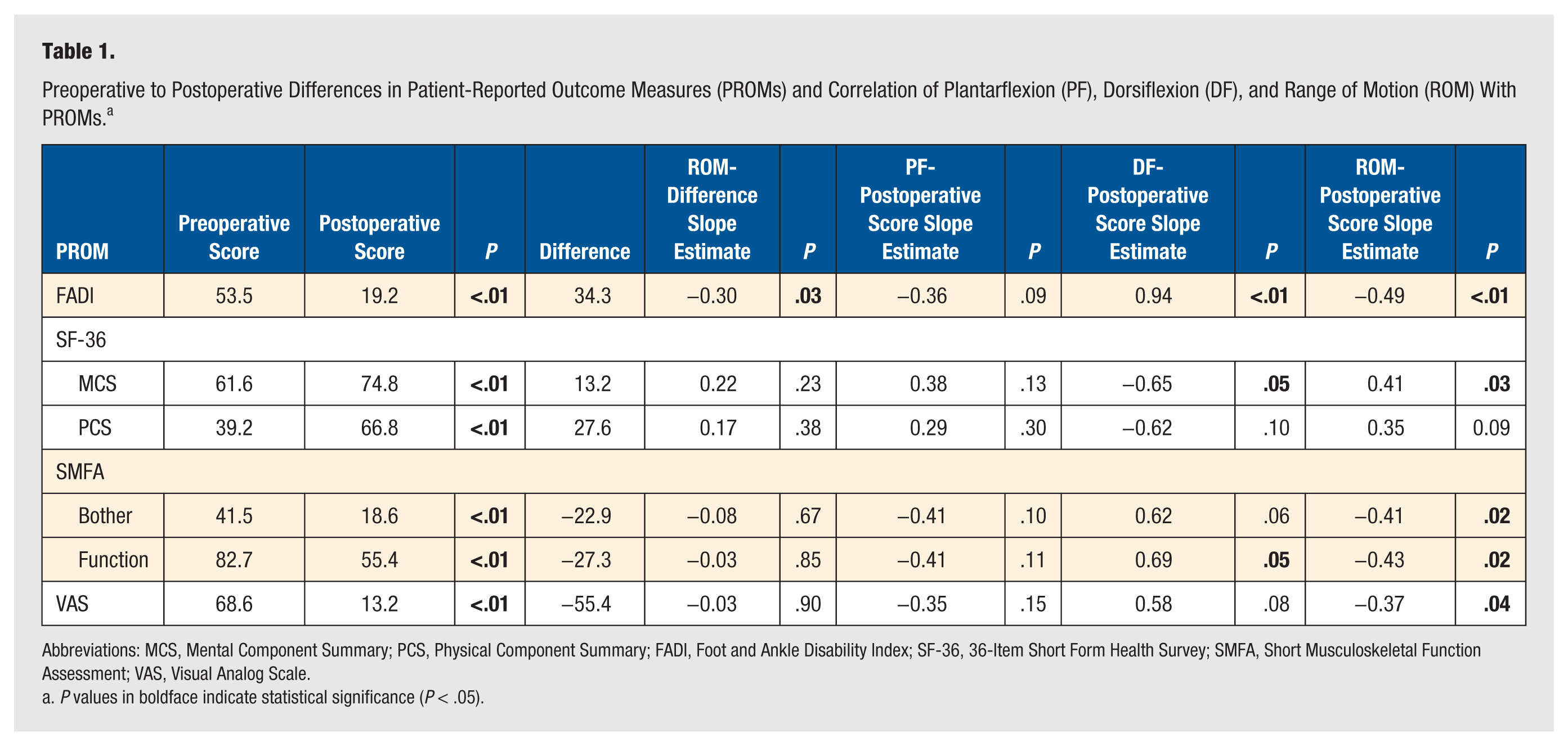
Abbreviations: MCS, Mental Component Summary; PCS, Physical Component Summary; FADI, Foot and Ankle Disability Index; SF-36, 36-Item Short Form Health Survey; SMFA, Short Musculoskeletal Function Assessment; VAS, Visual Analog Scale.
P values in boldface indicate statistical significance (P < .05).
Discussion
The onus has been placed on surgeons to prove the value of the procedures we perform to patients, payers, policy makers, and other key stakeholders. Demonstration of validated PROMs constitutes an integral component of success within the context of value-based health care. As payers become increasingly draconian in their assessment of surgical indications and what merits reimbursement, the need for evidence supporting the surgeries we perform and technology we use has become paramount. The findings from this study demonstrate that increased overall range of motion after TAR is directly correlated to final patient-reported outcomes and their satisfaction from the procedure.
TAR is a powerful procedure for alleviation of pain from end-stage ankle arthritis and represents a technological advance as compared with arthrodesis. Though some of the purported benefits of TAR such as preservation of adjacent joints and deceleration of peritalar and midfoot arthritis have not been fully bore out in sound epidemiologic evaluations, the patient perspective strongly suggests that the motion these implants afford is something that they value.4,5
Lewis et al 14 demonstrated significant improvement in VAS and SF-36 total scores in patients treated with primary TAR as well as those treated with TAR and ipsilateral subtalar arthrodesis. Both groups exhibited improvement in overall functional scores as well as objective tests such as sit-to-stand and walking speed. 16 Lampley et al 13 similarly found significant improvements in SMFA and SF-36 in nonsmokers and smokers undergoing TAR. These findings allude to a role for TAR in returning patients to a greater level of activity, even in more complex cases and challenging patient populations.
The present study demonstrated statistically and clinically significant improvements in validated disease-specific and HRQoL PROMs. The minimal clinically important difference (MCID) has been described as approximately half the standard deviation for PROMs in the lower extremity literature. 24 The MCID for the SF-36 PCS has been identified as between 5.5 and 7.8; this is exceeded by the improvement of 27.6 in our study—meaning that the improvement has clinical significance and is not simply a statistical anomaly due to overpowering.24,25 The net improvement in SMFA Function Index in the studied cohort is 27.3, which exceeds the MCID for the SMFA Function Index of 4.4 signifying clinical significance. 24
Though ROM has been posited to improve outcomes, physical exam ROM testing often belies the true amount of hindfoot motion and there have been no studies correlating more precise radiographic ROM measurements with PROMs.9,21,26 In the presented cohort, postoperative total ROM, or final ankle ROM, is positively correlated with PROMs. Interestingly, absolute plantarflexion was not correlated with any of the measured PROMs. This is seemingly counter to classic teachings that patients prefer ankle plantarflexion for ease of shoewear. Instead, patients associated dorsiflexion with FADI, SF-36 MCS, and SMFA Function (P < .05), supporting a potential role for dorsiflexion in floor clearance during gait.
A weakness of our study is the lack of preoperative ROM radiographs, which were not universally adopted until late 2015. This does not allow us to make any comparative conclusions to preoperative studies and overall change in magnitude of ROM. This study aims to associate PROMs with final ROM; however, further studies are required to demonstrate the effect of change of overall motion and how it effects functional outcome. We hypothesized that etiology of disease may play a role in this due to preexisting stiffness of the joint and soft tissue compromise but were unable to identify significant correlations in this study. Furthermore, weaknesses of this study are related to the limitations of registry data and its inherent biases. Though this study is based on a prospectively followed cohort of TAR patients, there were a large number of patients excluded due to incomplete preoperative validated PROMs. In the infancy of our institutional TAR database, the AOFAS score and its subsets were heavily used prior to full knowledge regarding validation of various foot and ankle outcome measures.
Conclusions
In this TAR cohort with prospectively collected outcomes data, radiographic sagittal plane ankle motion was positively correlated with multiple PROMs. Disease-specific and generic HRQoL PROMs demonstrated improvement postoperatively in all domains. TAR is a surgical option for patients with end-stage ankle arthritis and ROM is associated with improved patient-centric metrics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.