
Abstract
Background: Little is known regarding the association of operative time with adverse events following foot and ankle surgery. This study tests whether greater operative time is associated with the occurrence of adverse events following open reduction and internal fixation (ORIF) of the ankle. Methods: The American College of Surgeons National Surgical Quality Improvement Program database was queried for cases of ankle ORIF (primary CPT codes 27766, 27769, 27792, 27814, 27822, 27823) performed during 2005-2016. Operative time was tested for association with the occurrence of adverse events with controls for baseline characteristics and primary CPT code. Results: A total of 20 591 procedures met inclusion/exclusion criteria. The average (±SD) operative time was 75.7 (±37.3) minutes and varied by baseline characteristics and primary CPT code. After controlling for these factors, a 15-minute increase in operative time was associated with an 11% increase in risk for developing surgical site infection (SSI; relative risk [RR]: 1.11; 95% CI: 1.06-1.16), 20% for wound dehiscence (RR: 1.20; 95% CI: 1.11-1.29), 10% for anemia requiring transfusion (RR: 1.10; 95% CI: 1.04-1.17), 60% for cerebrovascular accident (RR: 1.60; 95% CI: 1.17-2.18), 14% for unplanned intubation (RR: 1.14; 95% CI: 1.03-1.26), and 7% for extended length of hospital admission (RR: 1.07; 95% CI: 1.05-1.09). Conclusion: Operative time is linearly and independently associated with the risks for SSI, wound dehiscence, and other adverse events following ORIF of the ankle. Efforts should be implemented to safely minimize operative duration without compromising the technical components of the procedure.
“Short-term complications increase hospital length of stay, which can lead to further complications, delay patient return to function, and ultimately decrease overall physical health.
Introduction
Ankle fractures are common musculoskeletal injuries that are expected to increase as the population ages.1-4 These fractures are debilitating because they require non–weight-bearing status for several weeks following surgery. Short-term complications increase hospital length of stay, which can lead to further complications, delay patient return to function, and ultimately decrease overall physical health. Identifying modifiable factors that place patients at risk for development of adverse events is essential in providing safe and efficacious surgical treatment to patients with fractures of the ankle.
Operative time has been identified as a modifiable risk factor for short-term complications in numerous orthopaedic procedures ranging from total hip arthroplasty (THA) and total knee arthroplasty (TKA) to anterior cervical discectomy and fusion.5,6 Previous research in these fields suggests that a 15-minute increase in operative duration is associated with a proportional increase in surgical site infection (surgical site infection), wound dehiscence, venous thromboembolism risk, extended length of hospital stay, and readmission.5,6 With respect to geriatric ankle fractures, a recent analysis established a correlation between longer operative duration and overall incidence of complication and revision surgery. 7 Although this analysis was valuable in identifying this relationship, the study did not quantify the increase in risk associated with a given increase in operative duration, nor did it consider specific adverse events seperately. 7 Further investigation is warranted to determine which complications are associated with longer duration of surgery and how much risk increase is associated with a given increase in operative duration, so that pragmatic clinical recommendations can be made.
The present study utilizes a large national database with several modes of quality-assured data collection to test for an association of a 15-minute increase in operative time with the occurrence of specific postoperative complications. The hypothesis of this study is that there is a quantifiable increased risk associated with each additional 15-minute increase in operative duration for open reduction and internal fixation (ORIF) of fractures of the ankle.
Methods
The present study is a retrospective analysis of the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP). This program prospectively collects data on all surgical procedures in >600 participating hospitals. Each participating hospital must staff a clinical reviewer that is responsible for assimilation of 274 variables on all surgical patients. Biweekly internal audits are performed by the ACS to measure interrater reliability among clinical reviewers. Previous evaluation of interrater reliability has demonstrated less than 1.8% disagreement.8,9
The 2005-2016 ACS-NSQIP was queried using Current Procedural Terminology (CPT) codes for ORIF of a medial malleolus (27766), posterior malleolus (27769), lateral malleolus (27792), bimalleolar fracture (27814), and trimalleolar fracture with/without fixation of the posterior lip (27822, 27823). Only the primary CPT code was queried, so as to not entirely exclude concomitant procedures that may be required (such as external fixator removal) but to ensure that the primary procedure being billed was the ORIF. Patients were excluded if there were missing data with regard to age, weight, height, gender, type of anesthesia, or comorbidities. Operative time was measured in minutes and defined as the time from initial incision to end of wound closure. To eliminate the influence of outliers, cases in which operative time was less than 25 minutes or greater than 215 minutes were excluded from analysis. Bounds for outliers were selected based on consensus by senior authors of this study. Operative durations less than 25 minutes and greater than 225 minutes were felt to likely be a result of coding/recording errors and were excluded to limit bias.
Data for short-term complications (within 30-days) were collected for all patients. Adverse events included transfusion rate, cardiac arrest, cerebrovascular accident (CVA), deep-vein thrombosis (DVT), wound dehiscence, myocardial infarction (MI), pneumonia, pulmonary embolism (PE), renal insufficiency, sepsis, SSI, unplanned intubation, and urinary tract infection (UTI). Hospital readmission data were collected, though this variable was prospectively collected only after 2013. Data on average length of stay were also collected. Extended length of stay was defined as greater than 1 SD from the mean.
Statistical analysis was performed using Stata 13.1 (College Station, TX). First, the baseline characteristics and procedure types noted above were tested for association with operative duration using bivariate linear regression. Operative time was tested for association with the adverse events noted above using multivariate Poisson regression with robust error variance 10 while controlling for the baseline characteristics and procedure types noted above to determine the relative risk (RR) of developing an adverse event, with a 15-minute increase in operative time. In this method of statistical analysis, the independent variable is time, with a 1-unit change representing 15 minutes. Similarly, the dependent variable is a binary yes/no occurrence of an adverse event. Hence, the interpretation of the RR that results from the regression is the increase in risk associated with a 15-minute increase in operative time. Of note, this is calculated across the full spectrum of observed operative times, such that it is valid/applicable to any 15-minute increase, whether that is from 1 hour to 1 hour and 15 minutes, or from 3 hours to 3 hours and 15 minutes. The level of significance was set at P < .05.
Results
A total of 20 591 cases met inclusion criteria. Age, gender, ASA classification, smoking status, hypertension, dyspnea on exertion, preoperative anemia, and use of general anesthetic were all independently associated with operative time (Table 1).
Operative Time, by Demographic, Comorbidity, and Procedural Characteristics.
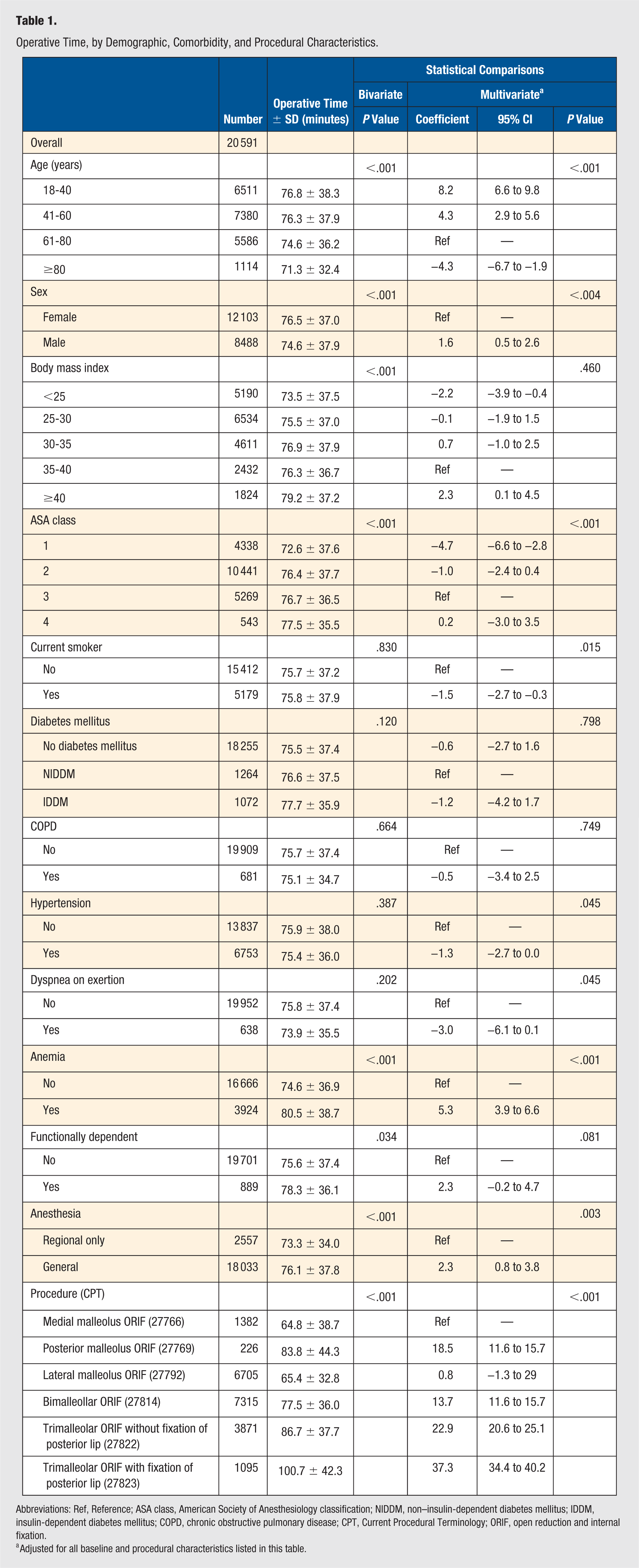
Abbreviations: Ref, Reference; ASA class, American Society of Anesthesiology classification; NIDDM, non–insulin-dependent diabetes mellitus; IDDM, insulin-dependent diabetes mellitus; COPD, chronic obstructive pulmonary disease; CPT, Current Procedural Terminology; ORIF, open reduction and internal fixation.
Adjusted for all baseline and procedural characteristics listed in this table.
The overall incidence of adverse events was 3.52% (Table 2). A 15-minute increase in operative time was associated with a 4% increase in risk for developing any adverse event compared with a patient who did not have that same 15-minute increase in operative time (RR: 1.04, 95% CI: 1.02-1.07; Table 2; Figure 1). Similarly, a 15-minute increase in operative time was associated with an 11% increase in risk for developing surgical site infection (RR: 1.11; 95% CI: 1.06-1.16), 20% for wound dehiscence (RR: 1.20; 95% CI: 1.11-1.29), 10% for anemia requiring transfusion (RR: 1.10; 95% CI: 1.04-1.17), 60% for CVA (RR: 1.60; 95% CI: 1.17-2.18), 14% for unplanned intubation (RR: 1.14; 95% CI: 1.03-1.26), and 7% for extended length of hospital admission (RR: 1.07, 95% CI: 1.05-1.09; Table 2; Figure 2). After adjustment, there was no association between operative time and cardiac arrest, DVT, MI, pneumonia, PE, renal insufficiency, sepsis, UTI, or hospital readmission (P >.05 for each; Table 2).
Association of a 15-Minute Increase in Operative Time With the Rate of Each Adverse Event or Hospital Metric Following Ankle Open Reduction and Internal Fixation.
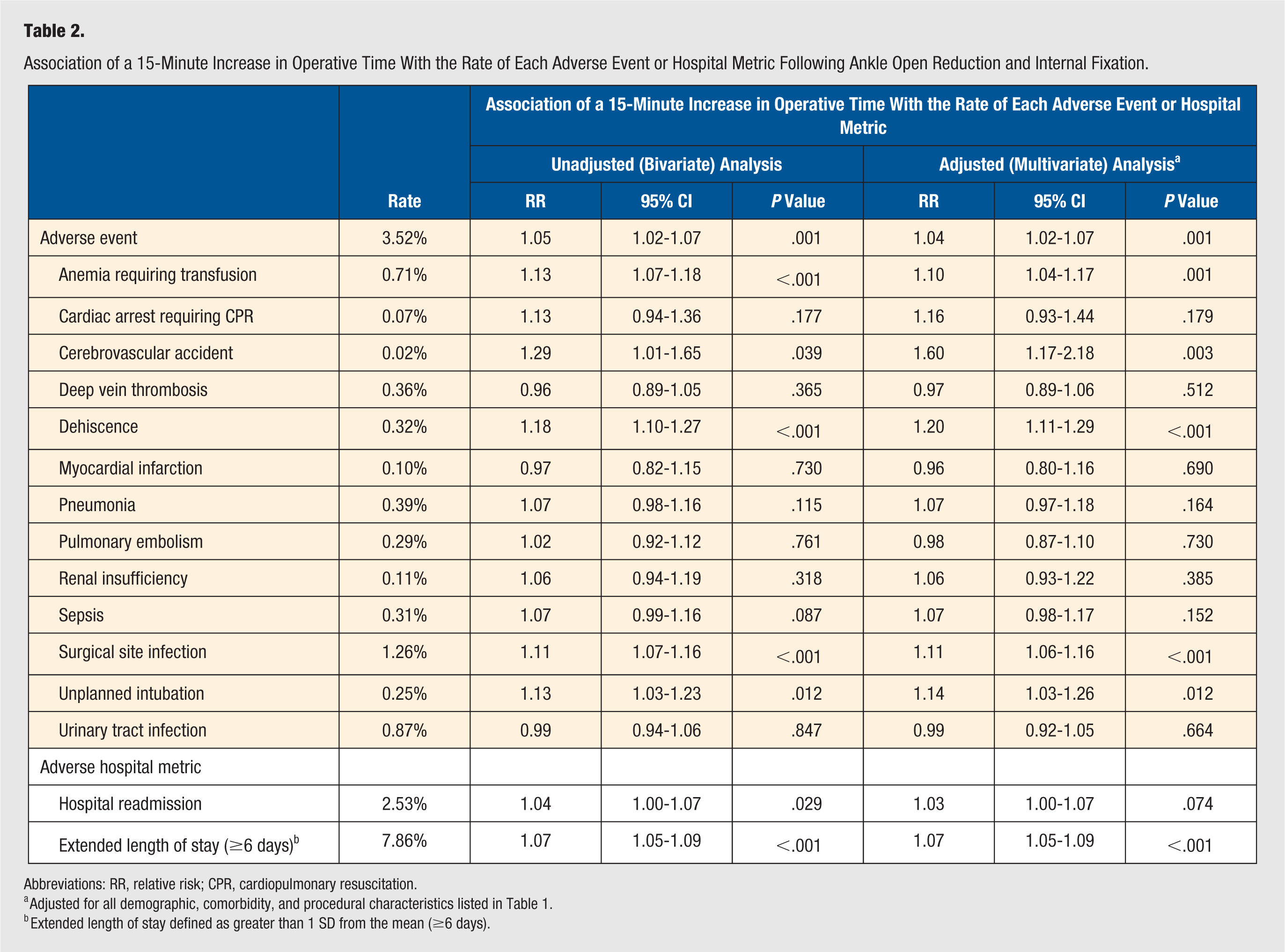
Abbreviations: RR, relative risk; CPR, cardiopulmonary resuscitation.
Adjusted for all demographic, comorbidity, and procedural characteristics listed in Table 1.
Extended length of stay defined as greater than 1 SD from the mean (≥6 days).
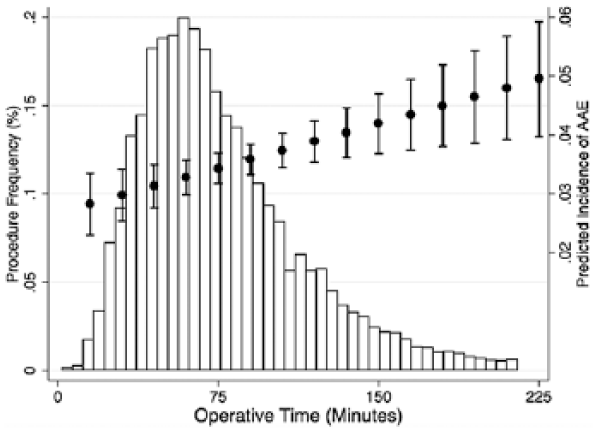
Predicted linear correlation between operative time and frequency of any adverse event (AAE) in comparison to the distribution of operative time.
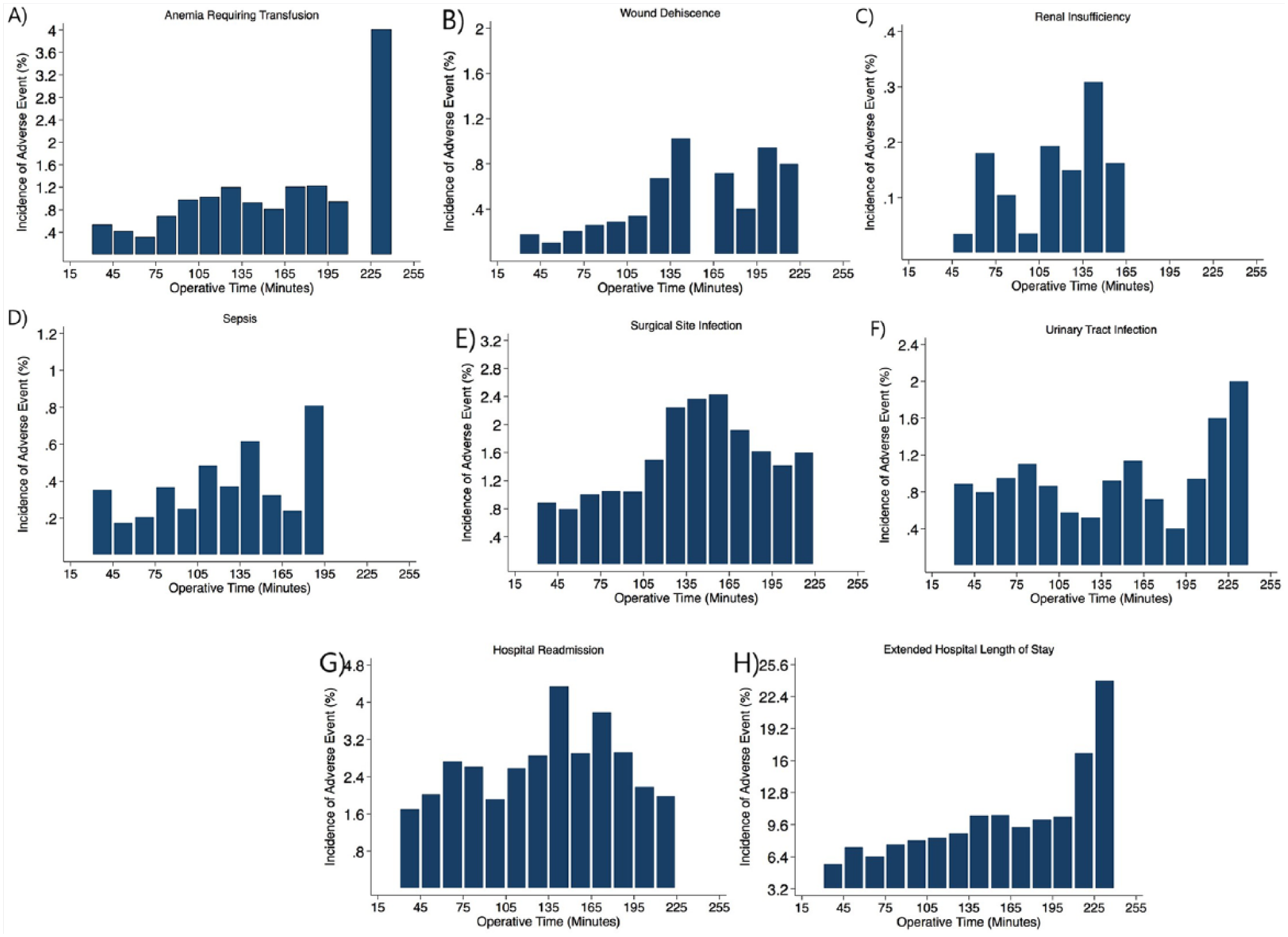
Influence of operative time on specific adverse events: the frequency of each adverse event is plotted for each 15-minute interval of operative time: (A) anemia requiring transfusion, (B) wound dehiscence, (C) renal insufficiency, (D) sepsis, (E) surgical site infection, (F) urinary tract infection, (G) hospital readmission, and (H) extended hospital length of stay.
Discussion
Operative time has been identified as a modifiable risk factor for short-term complications following numerous orthopaedic procedures, ranging from THA and TKA to anterior cervical discectomy and fusion.5,6 However, little is known regarding the association of operative time with complications following foot and ankle surgery. The present study suggests that operative time is independently associated with the development of a range of adverse events following ankle fracture ORIF. Interestingly, the relationship between operative time and adverse events was linear throughout the full range of operative times. An increase in 15 minutes was associated with a quantifiable increase in risk of surgical site infection, wound dehiscence, blood transfusion, stroke, unplanned intubation, and extended hospital length of stay. However, there was no association between operative time and many of the other tested adverse events.
In a single-center retrospective study of 68 patients undergoing ankle fracture ORIF, Aigner et al 7 found operative time to be an independent and modifiable risk factor for postoperative complications. However, the authors did not establish which specific complications were related to longer duration of surgery; rather, they simply tested for correlation with the overall complication rate. Moreover, the study was also limited by selection bias, in that it limited its population to only patients older than 65 years. The present study used a national database with operative time as the sole variable of focus to limit this selection bias and identify which postoperative events are and are not associated with longer surgery.
SSI was found to be the most common complication within our national cohort and also significantly associated with longer operative time (11% increase per 15-minute interval). Etiologies for SSIs have been classically organized into either poor soft-tissue conditions that compromise the soft-tissue envelope or poor overall host conditions, such as hypoalbuminemia and malnutrition 11 ; however, neither of these conditions is modifiable in an acute trauma setting. Longer operative time provides bacteria with more opportunity to seed the wound during open surgery. Additionally, there is greater time for potential contaminations to occur in the surgical back table or during entrance/exits to the operating room. 12
Notably, wound dehiscence was found to have among the highest increases in risk with operative time (20% increase per 15-minute interval). Longer time spent operating implies both greater time with retraction devices in place and greater time with the tourniquet on. Both these factors will contribute to local ischemia. This ischemia is only compounded by the traumatic nature of these injuries that predispose disruption of local blood vessels and tributaries. 13 Both retraction and tourniquet are necessary for successful visualization of fracture patterns and inserting implants; however, the time spent in operation should be managed efficiently to minimize ischemia. Moreover, any potential break from the tourniquet or retraction devices should be utilized.
As important as the complications noted to be associated with operative time are, the complications were noted to have no association. Some of these may be surprising. The occurrence of DVT/PE after TKA is thought to be associated with use of a tourniquet, potentially explaining the higher occurrence of DVT following TKA than THA. 14 However, greater tourniquet time had no impact on the occurrence of either of these events in the present study. Whereas greater operative time was associated with UTI after THA and TKA,5,6 in the present study, there was no association. This is likely related to the lack of use of Foley catheters in most ankle fracture patients, compared with the use of such catheters during THA, TKA, and lumbar fusion procedures.
Operative time may be considered a “proxy outcome” because experienced surgeons are expected to require shorter durations of surgery. 15 Still, operative time is in many ways modifiable. Preoperative planning should be emphasized, which may warrant a lower threshold to order additional radiographic views or a computed tomography (CT) scan. 16 The ability to preemptively determine fracture patterns and trajectories of reduction would certainly improve efficiency in the operating room. The benefits of advanced imaging may be further supported by the advent of new 3D printing technology that can be performed with CT reconstructions.17-19 Yang et al 18 found that trimalleolar ankle fracture cases assisted with 3D prototypes had reduced operative time and intraoperative blood loss. Further research is required to determine the clinical efficacy of these techniques and to determine whether the increase in cost of developing these models may be substantiated by improvements in complication rates. Additionally, resident involvement has been shown to result in longer operative times in the reduction of ankle fractures. 20 Teaching will certainly add time to the surgical procedure, and surgical efficiency must be emphasized during training. Greater guidance should be provided in difficult cases to minimize operative time and decrease the risk of postoperative events.20,21
The present study is limited by factors inherent to the ACS-NSQIP. First, fracture patterns, injury mechanisms, soft-tissue damage, surgical approach, and hardware use are not recorded. These variables each influence operative time, potentially influence the risk for postoperative complications, and are potential confounders. We did attempt to control for these factors by dividing patients into 6 groups based on the CPT code indicative of their type of surgical procedure. These groupings were used as controls in the multivariate regressions, but there exists the risk that these controls were insufficient. Furthermore, the treatment course prior to surgery is unknown for these patients. Some patients may have had a staged reduction with an external fixator, whereas others may have received an ORIF in the acute setting. Some patients may have also had multiple traumatic injuries that were fixed at separate time points. Additionally, the ACS-NSQIP only follows patients for 30 days, so complications occurring after this period are not captured. Finally, failures of reduction, osteonecrosis, and nonunion are not measured by the ACS-NSQIP and so could not be evaluated.
Conclusion
Operative time is linearly and independently associated with the risks for surgical site infection, wound dehiscence, and other adverse events following ORIF of the ankle. Efforts should be made to safely minimize operative duration without compromising the technical components of the procedure.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.