
Abstract
Stress fractures of the proximal fifth metatarsal are common injuries in elite athletes. Fixation using an intramedullary screw represents the most popular surgery performed for treating these injuries, with excellent results in most cases. However, multiple reports in the literature highlight the possibility of painful hardware, usually related to the presence of the screw head, following intramedullary fixation In this case report, we outline 4 cases of professional athletes who developed lateral-based foot symptoms following complete healing of their surgically treated proximal fifth metatarsal fractures and were found to have significant cuboid edema on magnetic resonance images. We also outline recommendations regarding specific surgical technique considerations aiming to minimize this possible complication.
Often, such screws are left in situ in athletes while they continue to compete, as an attempt to further decrease this risk of refracture.”
Introduction
Stress fractures of the proximal fifth metatarsal are common injuries in elite athletes, either from chronic stress or low-energy trauma, or most often a combination of both.1,2 Although management of these injuries can include either conservative or operative treatment,2-5 given that the risk of refracture reported is up to 12% to 30% in athletes, operative treatment is typically favored.2,6 Excellent clinical results can be expected in 80% to 100% of cases treated surgically. 2 Although reports of specific surgical interventions are varied, fixation using an intramedullary screw represents the most popular surgery performed for treating these injuries. 7 Often, such screws are left in situ in athletes while they continue to compete, as an attempt to further decrease this risk of refracture. However, several reports in the literature highlight the possibility of painful hardware, usually related to the presence of the screw head following intramedullary fixation, with rates ranging from 9% to 30%.3,8,9
Interestingly, the exact etiology of this type of symptom is not completely known. It has been hypothesized that the presence of a prominent screw head could lead to soft-tissue impingement, especially of the peroneus brevis tendon, increasing the likelihood of a hardware removal.10,11 In response to this concern, many have advocated for headless compression screw fixation, with the aim of reducing the proximal soft-tissue impingement caused by the screw, although the proposed advantages of this approach have yet to be validated in the literature.12,13
We describe 4 cases of professional athletes who developed lateral-based foot symptoms following complete healing of their surgically treated proximal fifth metatarsal fractures and were found to have significant localized bone edema of the cuboid when assessed by magnetic resonance images (MRIs). To the best of our knowledge, this is the first report within the literature of this “Cuboid Edema Syndrome.” We also highlight recommendations regarding specific surgical technique considerations that could potentially minimize this complication.
Case 1
A 26-year-old male NBA basketball player was diagnosed with a proximal metaphyseal-diaphyseal stress fracture of the fifth metatarsal in September 2014. He was treated with open reduction and internal fixation (ORIF) using a 5.5 mm × 55 mm headed compression screw (Figure 1). The fracture went on to heal uneventfully, as confirmed on both conventional radiographs and computed tomography (CT) scans. The patient returned to full play and did well until 6 months postoperatively (February 2015), when he complained of localized pain just proximal to the base of the fifth metatarsal. An MRI was performed, which showed diffuse bone edema of the distal and lateral aspects of the cuboid when assessed on T2/STIR images (Figure 2). With the concern that a prominent screw head could be driving the problem, the patient underwent screw exchange to a 5.5-mm headless screw. He did well initially with resolution of the proximal lateral pain, but on return to play, following a minor sprain, he presented again with ongoing pain, now slightly more distal, right at the base of the fifth metatarsal. Radiographs at this point revealed a refracture at the original fracture site. The patient then underwent revision ORIF, with removal of the current hardware and placement of a headed 6.5 mm × 50 mm compression screw. Particular attention was paid to properly countersink the screw head into the base of the fifth metatarsal. He went on to heal this fracture and gradually returned to full play without persistent lateral-based symptoms.

Radiographic findings for case 1, status post–initial open reduction and internal fixation fifth metatarsal: These radiographs from September 2014 demonstrate initial open reduction and internal fixation with a 5.5 mm × 55 mm compression screw.
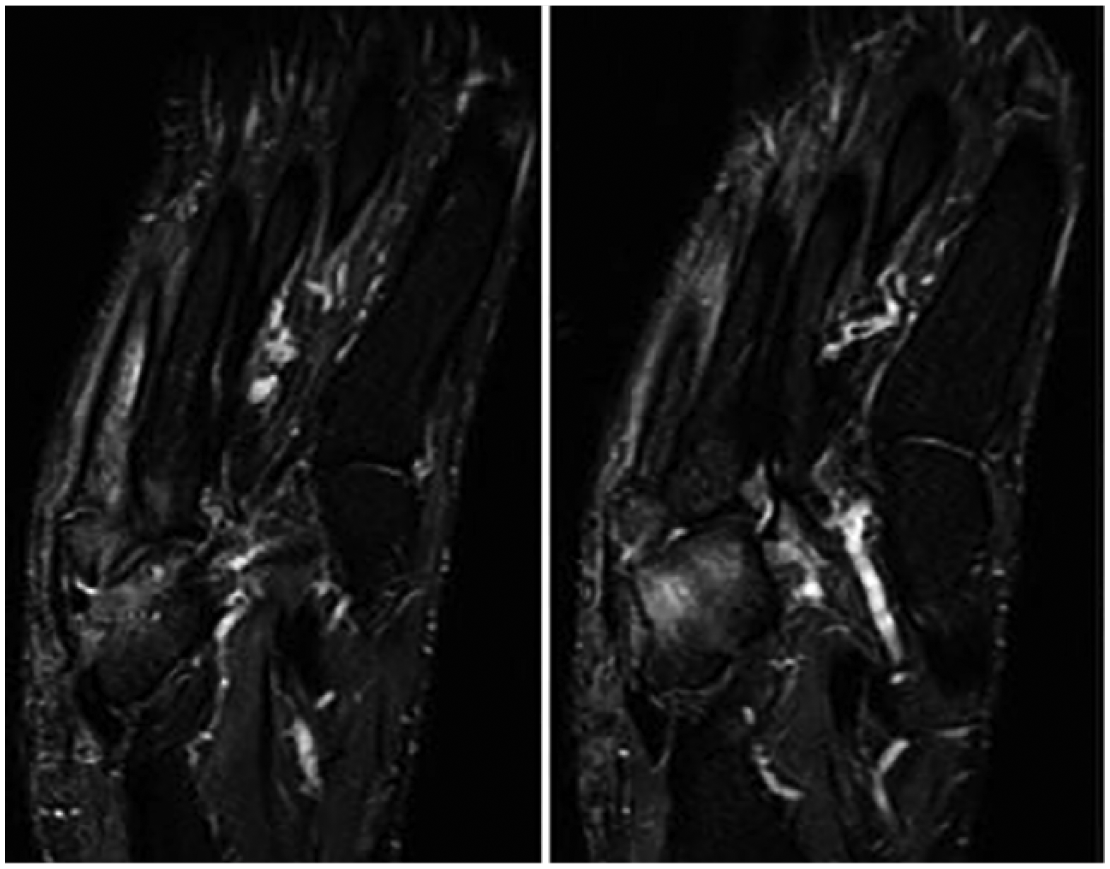
MRI findings for case 1, status 6 months post–ORIF fifth metatarsal. These coronal and sagittal T2 MRI cuts were obtained 6 months following ORIF fifth metatarsal fracture because of persistent pain just proximal to the fifth metatarsal base.
Case 2
A 22-year-old male professional soccer player was treated in July 2013 for a right proximal fifth metatarsal metaphyseal-diaphyseal stress fracture. Initial treatment consisted of percutaneous screw fixation and local injection of bone marrow aspirate concentrate into the fracture zone. A 45 mm × 5.5 mm partially threaded full-bore headed screw was used. He had an uneventful early postoperative course. However, by 9 weeks postoperatively, although he was fully bearing weight, he had persistent lateral-based pain, just proximal to the base of the fifth metatarsal. CT and radiographic findings at the time showed a persistent fracture line with delayed bone healing. He was treated with various adjuvant treatments to increase osseous healing such as vitamin D supplementation, protected weight bearing, and shockwave therapy. At the 12-week postoperative mark, his fracture was fully healed on CT scan, but he still had persistent lateral-based pain at the level of the cuboid. T2/STIR MR images demonstrated diffuse bone edema in the distal and lateral aspect of the cuboid and no other important findings. Concerned that there was perhaps some impingement related to a prominent screw head, he underwent hardware removal and revision to a headless 5.5 mm × 40 mm screw, which was carefully countersunk into the fifth metatarsal. By 5 months postoperatively, the patient’s pain at the level of the cuboid had resolved; however, some distal pain within the metatarsal shaft persisted. Radiographs and CT scan revealed no new fracture line, but there was concern for a stress riser effect at the distal aspect of the screw within the canal given the location of his pain. Hardware removal of the headless screw was considered, but the patient decided to continue to play and to insist with conservative treatment for a little longer. Because the patient has moved to a different state, further follow-up is not available.
Case 3
A 23-year-old male NBA basketball player was treated in October 2014 for a proximal metaphyseal-diaphyseal stress fracture of the fifth metatarsal. Initial treatment consisted of ORIF using a 5.5 mm × 55 mm headed compression screw. After routine healing of this fracture, he resumed full activity without complications. However, 18 months following his initial surgery, he had recurrent lateral-based pain. Radiographs at that time demonstrated 2 distinct fracture lines consistent with a refracture at the level of the original fracture. Surgical revision was then performed with placement of a 6.5 mm × 50 mm headed screw. After an uneventful postoperative course, he resumed full activity for the 2016-2017 season. At the end of the season, however, he returned to our clinic with lateral midfoot pain, just proximal to the base of the fifth metatarsal. An MRI at that time demonstrated healed metatarsal fracture lines, with T2/STIR bone marrow edema pattern in the distal cuboid, similar to the findings seen in previous cases (Figure 3). The patient was advised to have the hardware exchanged, but he decided to undergo conservative treatment with a cortisone injection around the screw head to continue playing until the end of the season. Revision surgery and hardware exchange would be considered moving forward if the symptoms persisted.
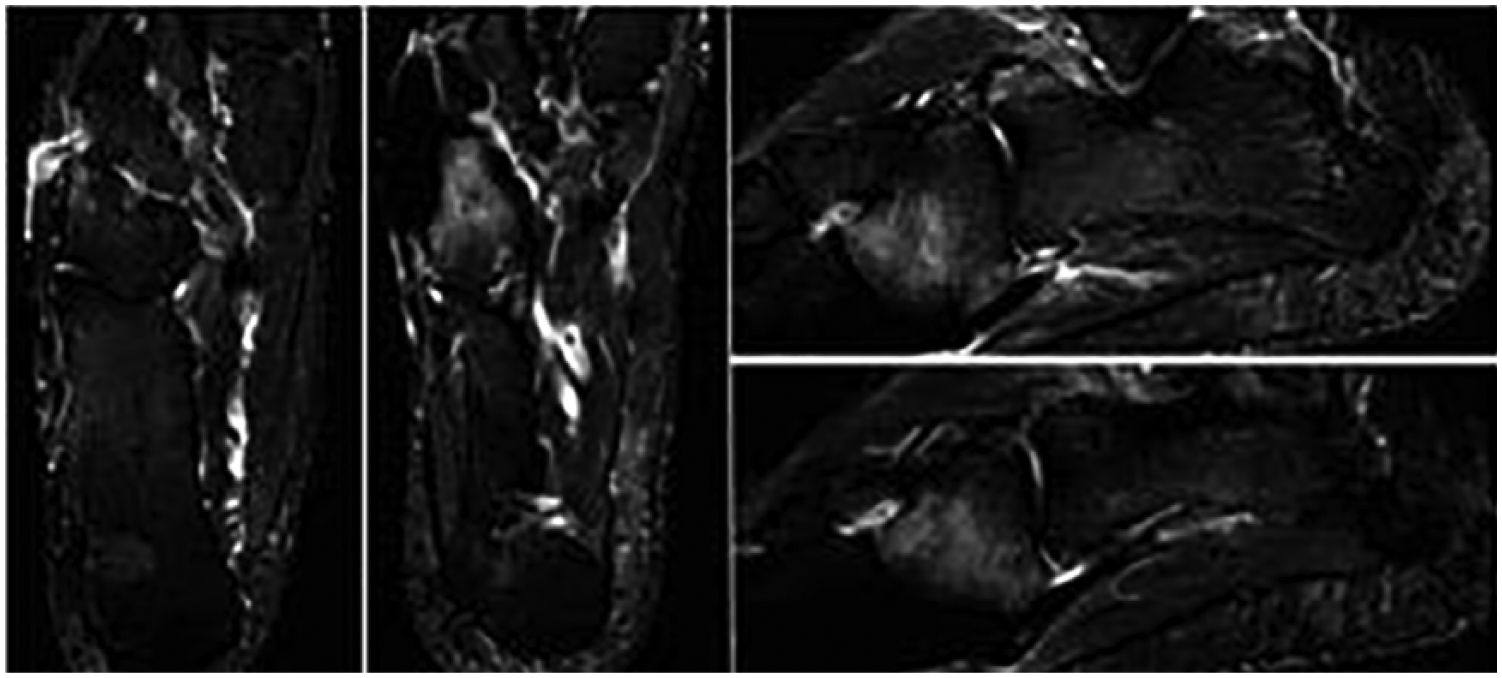
Magnetic resonance image (MRI) findings for case 3, status post–screw revision with persistent lateral foot pain: These coronal and sagittal T2 MRI images were obtained in June 2017 as the patient continued to have lateral foot pain following screw exchange. Despite showing a healed fracture, bone marrow edema of the cuboid is evident, potentially secondary to impingement.
Case 4
A 19-year-old male NBA basketball player who sustained a metaphyseal-diaphyseal stress fracture of the proximal fifth metatarsal in May 2017 underwent open reduction and internal fixation using a partially threaded 45 mm × 5.5 mm headed cannulated screw at an outside center (Figure 4). Three weeks later, on presentation to our institution, he had persistent, unexpected pain for this stage on the lateral aspect of his midfoot, just proximal to the base of the fifth metatarsal. MRI at that time demonstrated T2/STIR edema in the proximal aspect of the fifth metatarsal as expected but also the same pattern within the distal and lateral aspects of the cuboid. He continued on a standard postoperative course, initiating progressive and protected weight bearing at 6 weeks postoperatively. With persistent pain in this same area at the 4-month postoperative mark, a new MRI was performed, showing persistent T2/STIR findings of bone edema in the anterolateral cuboid (Figure 5). The patient decided to continue with conservative treatment at that point. Following a new injury 1 month later, at the 5-month postoperative mark, the patient was diagnosed with a refracture that necessitated revision ORIF using a 6.5 mm × 50 mm partially threaded, full-bore headed screw with a focus on fully seating the screw head within the base of the metatarsal. He subsequently went on to heal this fracture and returned to full level of play without lateral-based foot pain.

Radiographic findings for case 4, 6 weeks status post–open reduction and internal fixation fifth metatarsal: Type 2 fifth metatarsal treated with a partially threaded 45 mm × 5.5 mm cannulated screw, May 2017.
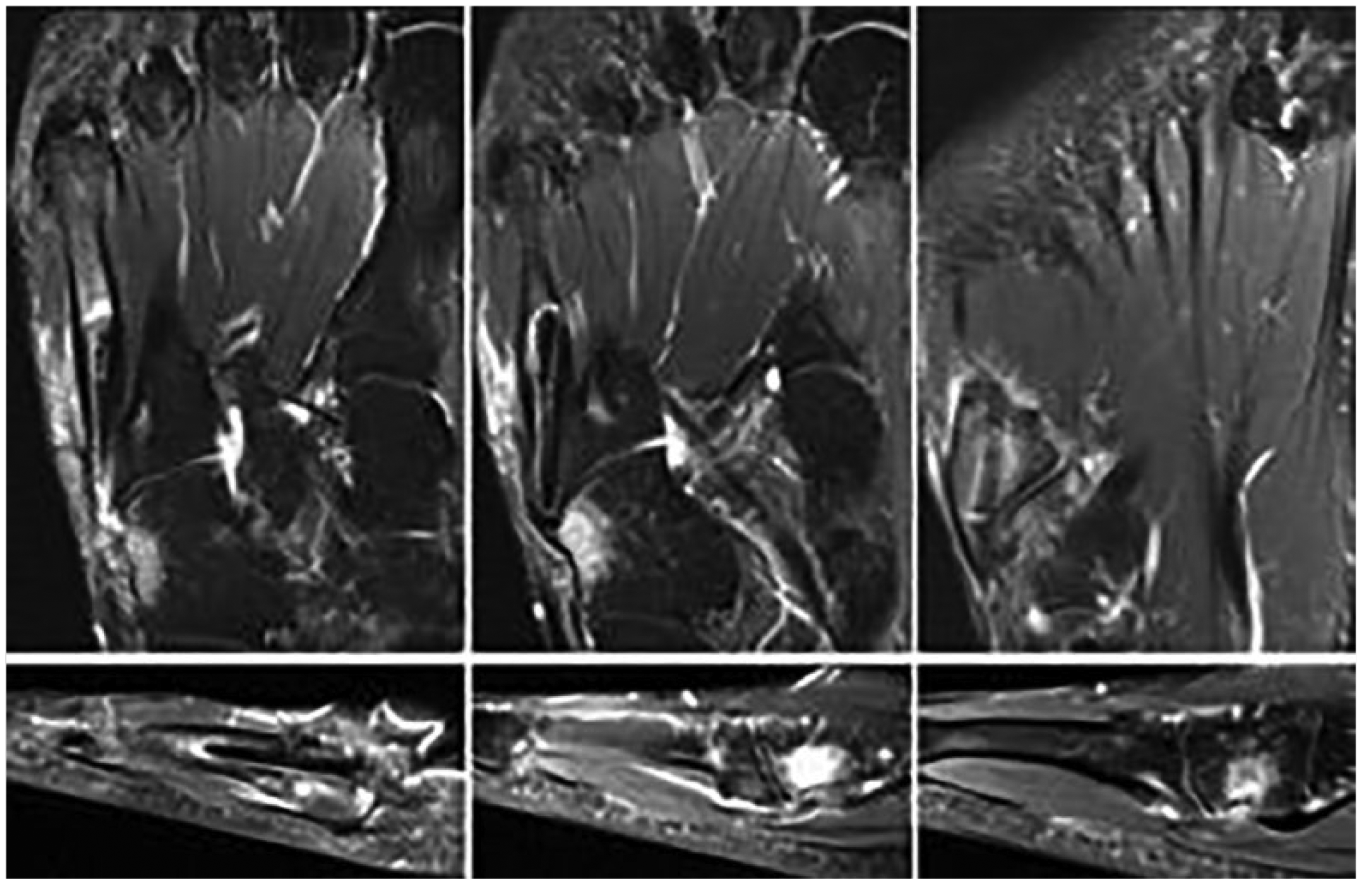
MRI findings for case 4, status post-ORIF fifth metatarsal: These coronal and sagittal T2 MRI cuts were obtained 4 months postoperatively. Images demonstrate residual inflammation of the fracture site as well as edema in the distal lateral cuboid.
Discussion
In this study, we have presented 4 cases where intramedullary fixation of metaphyseal-diaphyseal stress fractures of the proximal fifth metatarsal was done using the “high and inside” technique (that takes into account the anatomy and natural bowing of the bone10,11), which resulted in adequate healing of the fracture; but, subsequently, patients had persistent lateral pain in the midfoot, just proximally to the fifth metatarsal base. This clinical scenario that we dubbed cuboid edema syndrome was characterized by recurrent and persistent lateral midfoot pain after fracture healing, and T2/STIR MRI findings of bone marrow edema of the distal and lateral aspects of the cuboid, possibly related to the prominence of the hardware (headed screws) and consequent mechanical impingement on the distal cuboid.
On review of the literature, we found that different authors have reported on lateral foot pain and “proximal discomfort” after surgical fixation of proximal fifth metatarsal fractures.3,8 Mologne et al described a suspected “impingement syndrome” in 2 athletes out of 19 operated on for this type of injury, which completely resolved after screw removal. They also reported on some discomfort in 3 patients that did not prevent them from participating in all sports, without providing further details about a clear diagnosis. 8 MRI was not utilized in this study.
DeLee et al 3 described tenderness over the entry point of the screw in 3 patients out of 10 and pain under the head of the fifth metatarsal bone in 5 patients. In the majority of these patients, soft liners/insoles were sufficient to relieve the symptoms. The authors concluded that a proper countersinking was important to avoid any proximal prominence of the screw head that could potentially lead to impingement of the hardware in the surrounding soft tissue/bone. 3
Although a clear etiology for cuboid edema syndrome has yet to be clearly established, the clinical and MRI findings as well as the treatment course of the patients presented in our study support the idea of a possible mechanical impingement of the proximal aspect of the hardware into the distal aspect of the cuboid. Other possible reasons for persistent lateral symptoms and/or cuboid bone marrow edema on MR images would be technical errors during insertion of the screw, direct injury to the cuboid at the time of the surgery, soft-tissue irritation/impingement, peroneal tendinopathy, and lateral columns overload.
A recent cadaveric study by Watson et al 14 found that the cuboid is often and specifically at risk when positioning the entry point for the fifth metatarsal screw fixation centrally within the base of the fifth metatarsal (which allows for the straightest trajectory within the proximal canal). As such, the authors recommended considering reaming away of the lateral portion of the cuboid or performing a cuboid osteoplasty to allow for access to this central entry point. 14 These anatomical findings could partially explain our clinical findings in the current case series where lateral foot symptoms were associated with bone marrow edema within the cuboid following ORIF of the fifth metatarsal. However, in this study, it was not possible to ascertain if either a specific technique or any type of intramedullary fixation of the fifth metatarsal would be related to the development of this complication.
With regard to the features of the hardware used to fix proximal fifth metatarsal fractures, different studies in the literature have recommend the use of headless screws as another way to potentially minimize hardware-related symptoms.2,15-17 However, concerns have been raised regarding the appropriateness of a headless cannulated screw fixation in this setting, specifically because solid screws have been found to have a higher resistance to failure than cannulated screws. 2 This has prompted many surgeons to preferentially select full-bore, albeit headed, screws, typically placed in the “high and inside” position. Various developments for a fracture-specific screw have also been attempted, but rigorous clinical comparison of the available options is still lacking.10,11 Further to this, the optimal screw length and size has also not yet been determined definitively in the literature and may vary depending on the individual characteristics and anatomical variations. 2 Selecting a shorter or undersized (diameter) screw may not provide adequate fixation and could potentially facilitate the proximal migration of the screw toward the cuboid. Furthermore, in terms of length, a screw that is too long may similarly contribute to its migration and loosening because of the anatomical curvature of the fifth metatarsal representing a natural stop to its progression in the bone. 14
Another recommendation that avoids the prominence of a screw head at this level has been recently described by Mitchell et al. 18 These authors advocate for plantar plating of proximal metaphyseal-diaphyseal and diaphyseal injuries citing that it provides a more biomechanically stable construct that inherently avoids these problems with proximal impingement. 18 One potential concern with this construct, however, is that with the rate of nonunion and refracture still present, failure of this hardware could occur, leaving small hardware remnants within the canal, presenting the surgeon with a more challenging revision surgery than is typically seen with intramedullary screw fixation.
In conclusion, we describe the cuboid edema syndrome as a possible complication following intramedullary fixation of proximal metaphyseal-diaphyseal fifth metatarsal fractures. It is clinically characterized by recurrent and persistent lateral midfoot pain and MRI findings of bone marrow edema of the distal and lateral aspects of the cuboid on T2/STIR images, potentially related to mechanical impingement of the proximal aspect/head of the screw into the cuboid. Based on our experience of such cases, we recommend the use of the shortest screw possible that allows adequate intramedullary engagement and complete countersinking of the proximal aspect of the screw within the bone, whether it is headed or headless. Depth of countersinking and final screw position should be assessed intraoperatively in multiple orthogonal fluoroscopic views to ensure that there is no evidence of screw prominence. Surgeon awareness and early clinical suspicion of this entity is important when patients present with persistent pain at the lateral aspect of the midfoot despite evidence of routine healing of the fracture. MRI is essential in confirming this specific diagnosis. Establishing further evidence on the optimal way to treat these fractures while avoiding hardware-related symptoms, soft-tissue impingement, and the cuboid edema syndrome described here warrants further study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.