
Abstract
Background. Intramedullary screw fixation of Jones fractures using partially threaded screws is a common method of fixation for these injuries, but refracture continues to be a problem. Various other fixation strategies, such as headless compression screws, plantar plating, and tension-band wiring. have been developed to mitigate these issues. Biomechanical studies with regard to these other fixation strategies are limited. Herein, we investigate the compression strength and angular stiffness of Jones fractures fixed with Herbert-style headless compression screws. Methods. Jones fractures were created in 10 fresh-frozen pairs of cadaveric fifth metatarsals. A bone from each pair was instrumented with either a conventional, partially threaded screw 5.0 or 6.5 mm in diameter, or a headless compression screw 5.0 or 7.0 mm in diameter. Sizes were determined via sequential tapping until a snug fit was obtained. Each metatarsal was stressed via cantilever bending over 1000 cycles. We monitored compression and displacement throughout. Results. Headless compression screws achieved a significantly higher amount of stiffness than conventional, partially threaded screws (P = 0.005). There was no statistically significant difference with respect to compression. Conclusion. In a cadaveric model, headless compression screws achieved a greater amount of fracture stiffness versus conventional, partially threaded screws.
Keywords
“We believe Herbert-style headless compression screws will have greater angular stiffness compared with partially threaded screws in Jones fracture fixation.”
Jones fractures are fractures at the metaphyseal-diaphyseal junction at the base of the fifth metatarsal. This injury often takes a prolonged time to unite when treated nonoperatively due to the decreased blood supply at the vascular watershed between the metaphysis and diaphysis.1,2 As a result, operative fixation has been advocated in athletes and those with persistent symptoms to improve chance and speed of union. 3 Intramedullary screw fixation with partially threaded screws is one of the most common methods of fixation for these fractures, but there continues to be a 10% to 15% refracture rate.4-7 An undersized screw is the primary risk factor for refracture, but optimal size is difficult to determine intraoperatively.8,9 As such, other techniques, such as plantar or lateral plating, tension-band wiring, and headless compression screws, have emerged as alternatives.10-12 The senior author switched from conventional screws to headless compression screws after experiencing several refractures and nonunions with conventional screws. Currently, there is limited biomechanical evidence to justify these new approaches. Prior studies have focused on variably threaded headless compression screws and found similar compression stability after cyclic loading, higher pull-out force, but lower peak compression and greater angulation with repeated loading versus conventional, partially threaded screws.13-15 Thus far, we have not seen similar biomechanical studies for Herbert-type headless compression screws (Figure 1).
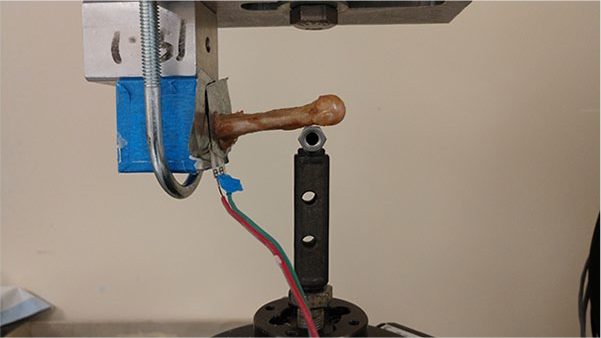
Biomechanical testing setup (left) and view of the sensor used (right).
The purpose of this study is to compare the angular stiffness and peak compression of Herbert-type headless compression screws to that of conventional, partially threaded screws in a cadaveric model. We believe Herbert-style headless compression screws will have greater angular stiffness compared with partially threaded screws in Jones fracture fixation.
Methods
Sample Size
Ten matched pairs of fresh-frozen human cadaveric feet were obtained. Demographics of the cadaveric sample are listed in Table 1. An a priori power analysis based on data from Orr suggested that 28 matched pairs were needed for sufficient power. 13 This number of samples was found to be cost prohibitive. Instead, our plan was to obtain preliminary data using 10 pairs and scale up if needed. We decided not to test beyond 10 matched pairs when we found the data already reached statistical significance.
Demographics of the Cadaveric Sample.
Specimen Preparation
The fifth metatarsals were dissected out of each pair and scanned with computed tomography (CT) to ensure no bone abnormalities were present. DEXA (dual-energy X-ray absorptiometry) scans were not performed for several reasons: (1) the effect of bone density is accounted for using matched pairs; (2) CT scan can more accurately detect any bony defects, which has a higher likelihood to be unilateral and not be identified on DEXA; and (3) the additional cost involved. An osteotomy transverse to the longitudinal axis of the bone was made using a sagittal saw at the metaphyseal-diaphyseal junction.
A FlexiForce A401 Sensor (TekScan, Inc, South Boston, MA) was used to measure contact compression force between the proximal and distal fragments of each fifth metatarsal. A 6-mm hole was punched through the center of the A401 compression sensor, which was then placed in the fracture site to allow the fixation screw access through the sensor (Figure 1). Provisional reduction was held using a K-wire. Afterward, either a headless compression screw (Fixos, Stryker, Kalamazoo, MI) or conventional partially threaded screw (Asnis JFX, Stryker, Kalamazoo, MI) was advanced through the sensor and across the fracture site (Figure 2). Screw diameter was determined by tapping the bone with sequentially larger screw taps until a snug fit was established, as previously described. 16 Screw sizes were either 5 mm or 6.5 mm in the partially threaded screw group and 5 mm or 7 mm in the headless compression group. Screw length was 70% of the metatarsal length, as determined in a prior study. 13
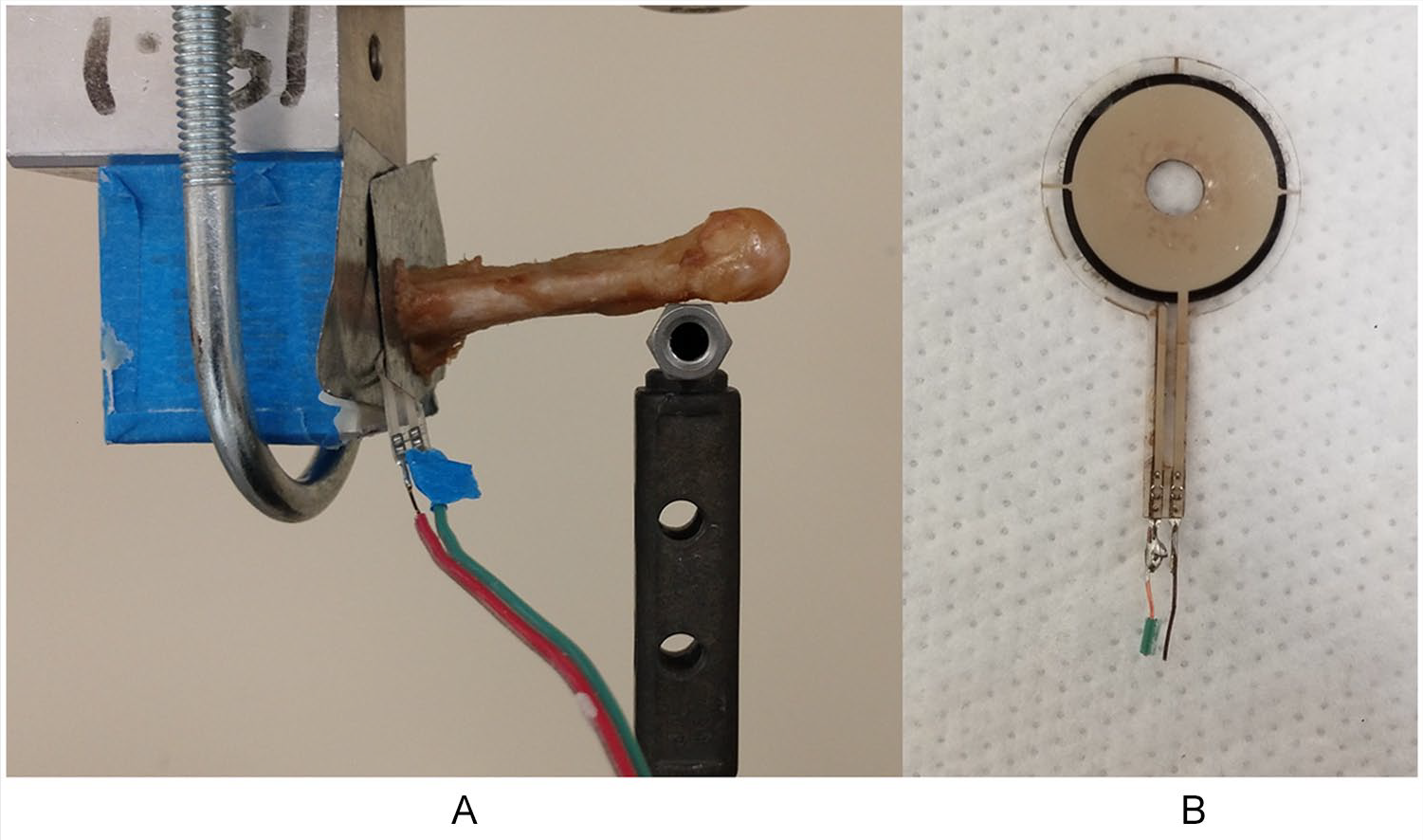
(A) Headless compression screw. (B) Partially threaded screw used for Jones fracture fixation.
Biomechanical Testing
The compression sensor was calibrated using weights before each biomechanical test. The proximal end of the fifth metatarsals were potted in polymethylmethacrylate up to the level of the fracture site. The potted ends were then clamped into a custom cantilever bending jig mounted to the actuator of an MTS 858 Mini-Bionix (MTS Corp, Eden Prairie, MN) testing system (Figure 1). The distal end of the metatarsal rested on a perpendicular bar attached to a 500 N load cell. Force measurements from the compression sensor were recorded immediately before loading cycles. Each specimen then underwent 1000 cycles of a 25 N dorsally directed bending force at a rate of 2 Hz. A 25 N load was used as this is the estimated physiologic load on the fifth metatarsal head during ambulation. 17 At each 100-cycle increment, the specimen was unloaded, and a compression force measurement was again recorded. At the end of the loading protocol, a final, unloaded, unclamped compression force measurement was taken. In concordance with a prior study, fracture site angulation was over 10°. 13
Load versus displacements curves were generated for each test. The 100th cycle of each loading test was used to calculate initial stiffness, which was the slope of the loading curve. Final stiffness was calculated from the loading curve of the final, 1000th cycle. Paired t tests with α = .05 were used to detect differences in fifth metatarsal initial displacement at 100 cycles, final displacement at 1000 cycles, initial stiffness, final stiffness, initial compression, and final compression.
Results
There were no significant differences in diameter and length between metatarsal pairs. Descriptive and statistical results from the biomechanical testing of Jones fracture fixation in 10 matched-pair fifth metatarsals with headless compression and partially threaded screws are presented in Table 2. Screw sizes used and the corresponding internal cortical diameter of the fifth metatarsals instrumented are listed in Table 3. One screw in the partially threaded group failed after 900 cycles and was still included in the final analysis because it lasted for the majority of the testing. Fracture site displacement was found to be decreased after 1000 cycles versus the first 100 cycles. This was consistent across both screw types and was consistent across all screws tested except those reaching failure. Furthermore in the headless compression group, fracture site compression increased briefly at cycles 800 to 900, but decreased back to normal levels at cycle 1000.
Descriptive Statistics Regarding Fracture Site Stiffness and Compression Between Headless Compression Screws and Partially Threaded Screws a .
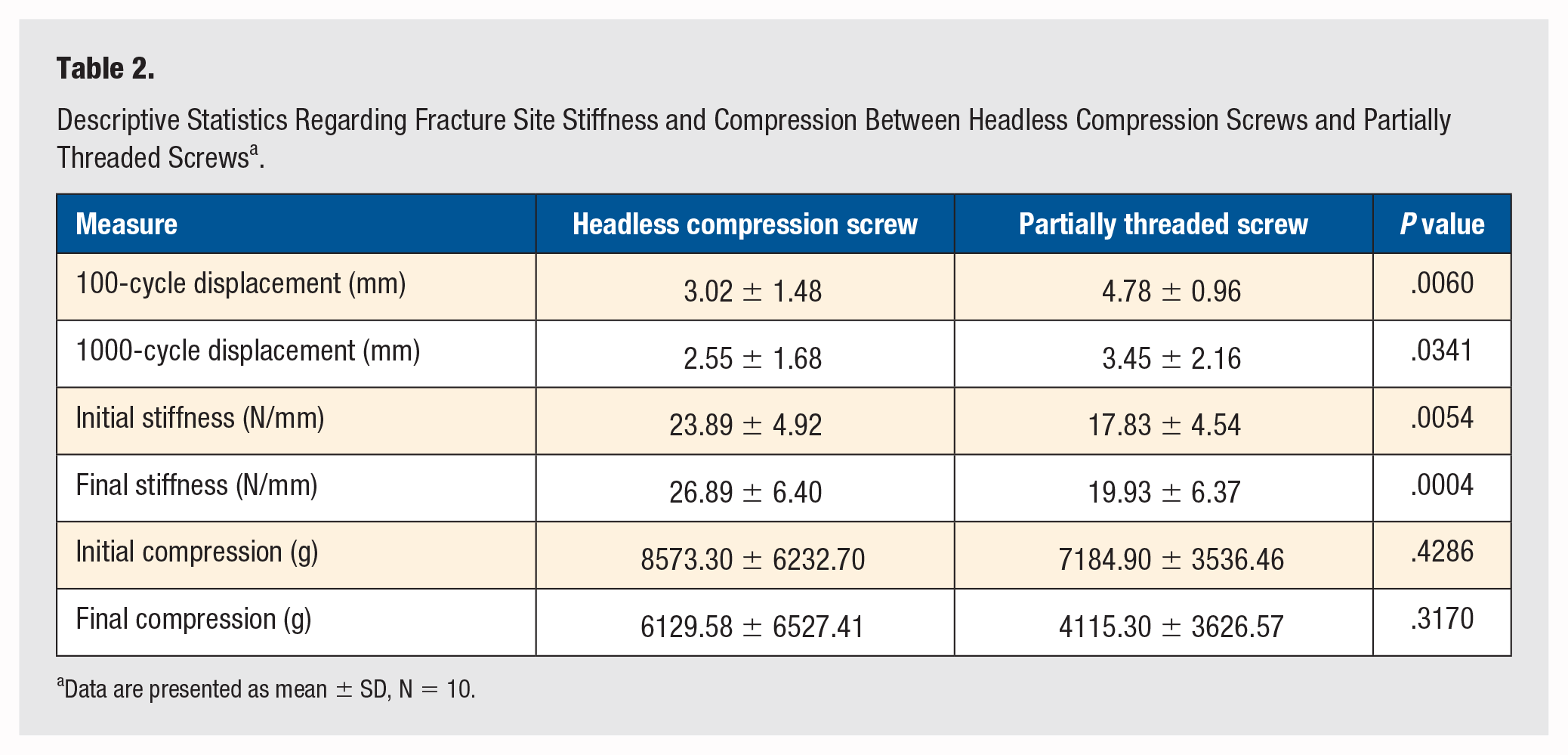
Data are presented as mean ± SD, N = 10.
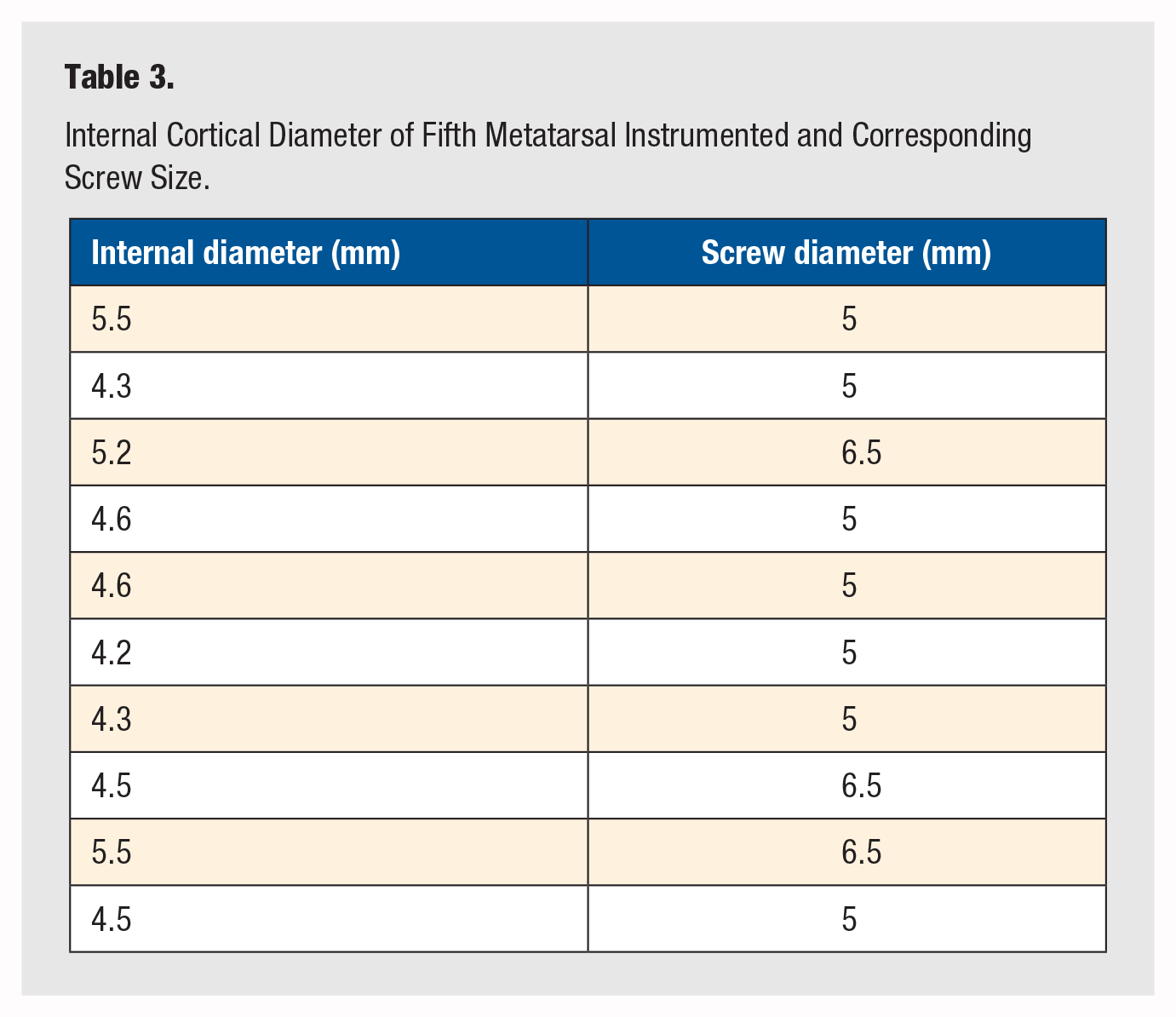
Internal Cortical Diameter of Fifth Metatarsal Instrumented and Corresponding Screw Size.
There were statistically significant differences in 100-cycle displacement (P = .0060), 1000-cycle displacement (P = .0341), initial stiffness (P = .0054), and final stiffness (P = .0004). The headless compression screw fixations sustained significantly less displacement and were significantly stiffer than the partially threaded screw fixations. The headless compression screws also exhibited higher initial and final fracture site compression, although not statistically significant (Figure 3).
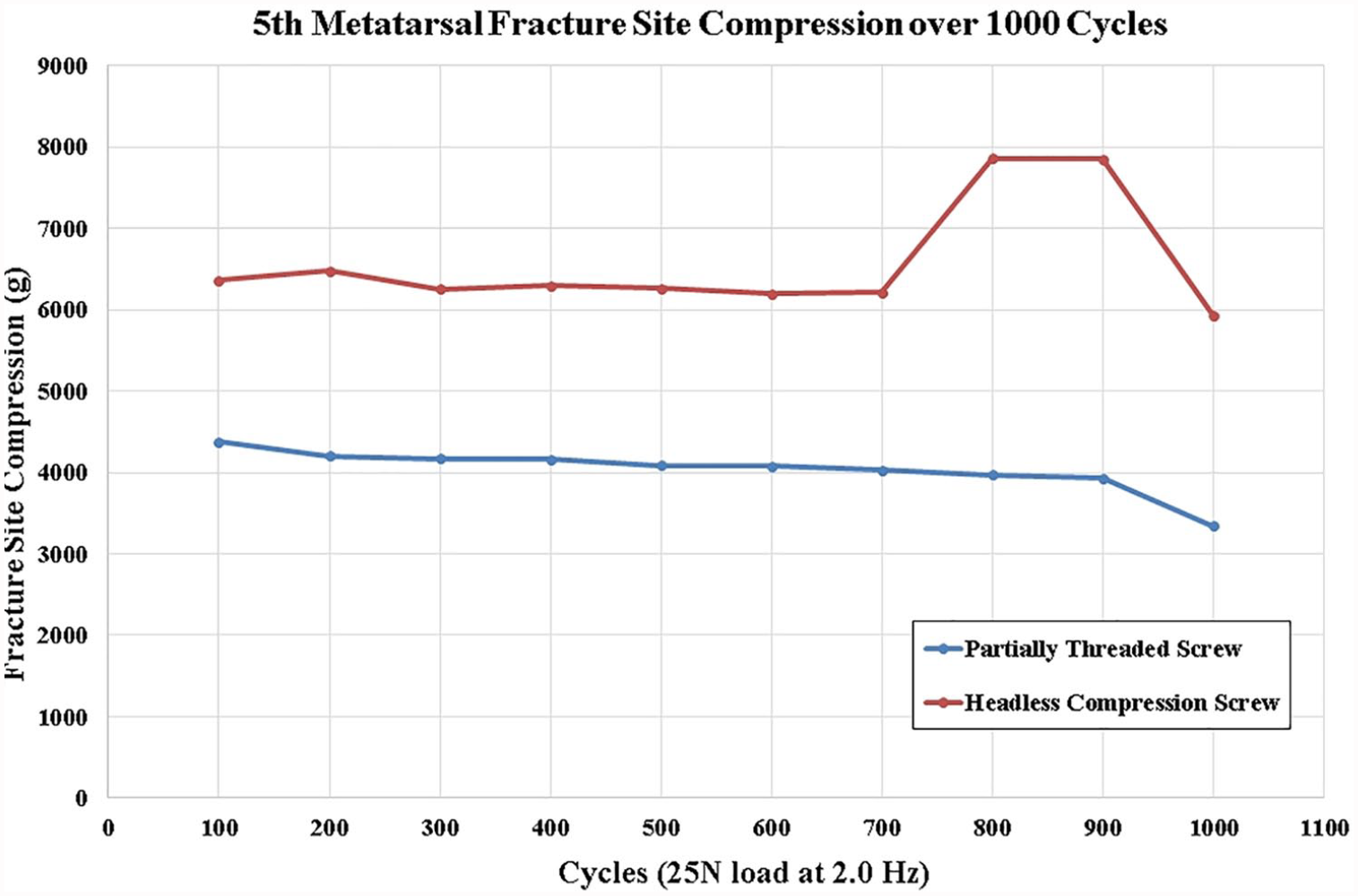
Average fracture site compression during cyclic loading.
Discussion
In this study, we show that headless compression screws achieve a greater amount of fracture-site stiffness versus conventional, partially threaded screws. Our results differ from a similar biomechanical study in which conventional, partially threaded screws were found to be superior to variable-pitch, fully threaded headless compression screws in terms of fracture-site compression and angulation. 13 A large difference between our study and Orr’s was that our headless compression screws were of either the same diameter or larger (by 0.5 mm) than the partially threaded screws used, whereas in the study by Orr, the partially threaded screws were the same size or larger (by 1.5 mm) than the variably threaded screws. Considering that stiffness increases by radius to the fourth power, this change could lead to a significant difference in stiffness that is independent of screw fixation or design. Orr’s justification in using different sized screws was based on 2 biomechanical studies showing that 4.5 and 5.5 mm cannulated partially threaded screws had no difference in load to failure and that the Acutrak 4/5 had equivalent bending stiffness to a 6.5-mm partially threaded screw.14,18 However, in both of those studies, there was no cyclic loading; thus, those results may not have been applicable for this experiment.
The choice of screw size used was also different than prior studies. We sequentially tapped the canal until a snug fit was found, in contrast to using internal cortical diameter. Although this introduced a portion of subjectivity to the methodology, we believe this better represents how screws will be sized in the operating room. Looking at the final screw diameters used, we observed that internal cortical diameter is a poor predictor of final screw diameter, and may lead to undersizing the screw used (Table 3).
Another interesting result was that displacement after 1000 cycles was measured as less than the initial 100-cycle displacement. We surmise that the unilateral loading caused “settling” of the fracture fragments into a more stable position; stiffness improved once the intramedullary bone contacted the smooth shank of the screw. Additionally, in the headless compression group, fracture-site compression increased briefly between 800 to 900 cycles. Looking at the data, this was due to a spurious reading for one of the screws that skewed the average. If these data are excluded, then the peak disappears.
There are several limitations to this study. Our cadaveric sample represented a population older than patients typically treated for this fracture pattern. The number of samples is small. Although most Jones fractures are transverse, the osteotomy created by a saw does not represent a physiologic fracture pattern. Furthermore, we only tested 1000 cycles and did not account for fracture healing. Our biomechanical model is oversimplified and is lacking a rotation moment on the fracture, which has been shown to occur due to the pull of the peroneus brevis. 19
Qualitatively, one insight gained through this study was that headless compression screws seem to provide the most benefit in osteopenic bone. The headless compression screw was able to obtain a larger amount of purchase and distribute load in the proximal fragment, whereas the partially threaded screw head would bury itself in the proximal fragment without obtaining fracture-site compression. To our knowledge, there has not been a comparison of compression strength of headless compression screws and conventional screws in an osteoporotic fracture model, and will be subject of future research.
In conclusion, in a cadaveric model, headless compression screws achieve greater fracture-site stiffness compared to partially threaded screws for Jones fracture fixation. The results here may guide surgeons considering choice of implants in fixation of proximal fifth metatarsal fractures. When considering prior studies, it appears that, regardless of implant chosen, the largest possible screw should be used when performing operative fixation of Jones fracture via an intramedullary screw technique.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Informed Consent
Not applicable.
Trial Registration
Not applicable.