
Abstract
Background
Total ankle arthroplasty (TAA) is an increasingly popular option for end-stage ankle arthritis. Americans over the age of 80 years grew to 16.7 million in 2010, but there are scarce data assessing the outcomes of octogenarians undergoing TAA. This study evaluated (1) perioperative factors, (2) 30-day postoperative complications compared to a nonoctogenarian cohort, and (3) independent risk factors for adverse outcomes.
Methods
A national database registry was queried for patients who had undergone primary TAA. This yielded 1113 patients, under (n = 1059) and over (n = 54) age 80 years. Demographics and perioperative data were compared using Fisher’s exact, χ2, and independent-samples t tests. Logistic and Poisson regressions were used to calculate odds ratio (OR) of complications and independent risk factors.
Results
The octogenarian cohort had longer in-hospital length of stay (1.9 vs 2.5 days, P < .0001). Octogenarians were not significantly more likely to develop any complication (OR = 1.32; 95% confidence interval = 0.29-6.04; P = .722), or increased number of complications (OR = 1.18; 95% CI = 0.27-5.18; P = .820). Octogenarians had significantly increased risk of being discharged to rehab/skilled nursing (OR = 6.60; 95% CI = 2.16-20.15; P < .001) instead of home.
Conclusion
Although the elderly population may carry inherent risk factors, octogenarians do not present an increased risk of short-term complications following TAA.
Levels of Evidence
Therapeutic, Level III: Retrospective cohort study.
Age has been shown to be an independent risk factor for perioperative morbidity and mortality in patients undergoing major surgery.
The number of Americans over the age of 80 grew from 13.4 million to 16.7 million from 2000 to 2010. 1 In 2007, over one third of all inpatient surgical procedures were performed on patients older than 65 years.2,3 Furthermore, an estimated 14% of surgeries done in an ambulatory setting between 2000 to 2010 were on patients over the age of 75. 4 The rising demand for surgical interventions in this elderly population necessitates an appropriate preoperative risk stratification with consideration for perioperative complications. Yoshihara and Yoneoka compared in-hospital complication and mortality rates of patients age 80 years and older, undergoing elective major orthopaedic surgery, to those between the ages of 65 and 79 years. 5 They found that the overall in-hospital complications and mortality rates were significantly higher for octogenarians undergoing spinal fusion, total hip, and total knee arthroplasty, compared with patients between 65 and 79 years old. Furthermore, the in-hospital complication rate increased with increasing number of medical comorbidities. 5 Age has been shown to be an independent risk factor for perioperative morbidity and mortality in patients undergoing major surgery. 6 Octogenarians may require additional consideration when determining the risk and benefit of a surgical procedure. This has been analyzed in the literature when considering octogenarian patients for other total joint replacements like knee, hip, and shoulder.7-11 Total ankle arthroplasty (TAA) is becoming an increasingly more prevalent option for end-stage arthritis, yet there is a paucity of literature evaluating the risk in the octogenarian age group undergoing TAA.
TAA is becoming an increasingly popular option for end-stage ankle joint disease as an alternative to ankle arthrodesis, previously the standard of care.12-14 Singh and Ramachandran 15 assessed time trends in TAA utilization rates in the US population. They found a 670% increase in TAA utilization rate over a 13-year period from 1998 to 2010. 15 In comparison to other orthopaedic procedures, the increase in utilization rate during this time was 200% and 50% higher than those of total knee and total hip arthroplasty, respectively. They also noted the TAA utilization rates for patients 80 years or older increased 7- to 10-fold, consistent with trends showing an increase in age of patients undergoing TAA.15,16 While initial attempts at TAA were met with high complication and failure rates, newer generations of implants and associated improved outcomes have led to a rapid increase in treatment of end-stage ankle arthritis.17-20 Ankle arthrodesis leads to a significant loss of ankle motion and is known to alter gait mechanics, restricting patient activity.21,22 Difficulties in ambulation and balance are the most common cause of falls and severe injuries in the elderly.23,24 In a TAA, replacement of the ankle using a prosthesis provides the advantage of preserving motion, resulting in improvements in gait, protection of the surrounding joints, and reduction of limp.25,26 Although increased mortality and readmission rates for octogenarians have been documented after total joint arthroplasty, there is a paucity of literature evaluating this population following primary TAA.
Given the rising popularity of TAA, and the increasing demand of joint arthroplasty for octogenarians, further investigation of the potential risks is paramount. Despite previous studies suggesting age as a major risk factor for early in hospital mortality, the elderly population should not be excluded as operative candidates. 5 Given the scarce data on early postoperative outcomes in the elderly undergoing TAA, the purpose of this study was to evaluate perioperative and short-term postoperative outcomes in octogenarians and to better understand risk factors. This study employed a prospectively collected national database to compare 30-day postoperative outcomes of patients age 80 years and older undergoing primary TAA patients to a younger cohort. Specifically, we assessed (1) perioperative factors; (2) 30-day postoperative complications compared to a nonoctogenarian cohort; and (3) independent risk factors for adverse outcomes.
Methods
Database
This study utilized the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. The purpose of this database is to advance the quality of care delivered to the surgical patient. Data are collected from over 700 participating hospitals, by trained clinical reviewers, including demographics, comorbidities, diagnoses in International Classification of Disease 9th and 10th revisions (ICD-9, ICD-10) codes, surgery in Current Procedural Terminology (CPT) codes, and surgical outcomes through 30 days postoperatively.
Study Population
The NSQIP database was queried to identify all patients who underwent primary TAA as defined by the CPT code 27702, from January 1, 2007, to December 31, 2017. 27 A total of 1113 patients were identified and then further subdivided by their age leading to 1059 patients in the nonoctogenarian cohort and 54 in the octogenarian cohort.
Patient Demographics
Demographic parameters included age, sex, race (White, Black, other), body mass index (BMI) categories (<24.9 kg/m2, 25 to 29.9 kg/m2, 30 to 34.9 kg/m2, 35 to 39.9 kg/m2, and >40 kg/m2), smoking status, diabetes (none, oral agents, insulin dependent), functional status, and Modified Charlson (MC) score (0, 1, ≥2). The MC score includes the following comorbidities and assigned values: chronic obstructive pulmonary disease (1 point), congestive heart failure (1 point), renal failure/end-stage renal disease (2 points), on a ventilator (2 points), ascites (3 points), and cancer (6 points). The MC score has had similar efficacy when compared to the original Charlson Comorbidity Score.28-30
Perioperative and Postoperative Factors
Perioperative factors collected include anesthesia type (general, regional/local/other), American Society of Anesthesiologists (ASA) scores (1, 2, 3, 4), operative time, and hospital length of stay (LOS). Postoperative factors collected include discharge destination and complications. Complications collected included the following: superficial incisional surgical site infection, deep incisional surgical site infection, organ space infection, wound dehiscence, pneumonia, urinary tract infection, deep vein thrombosis, renal insufficiency, transfusion, stroke, cardiac arrest, myocardial infarction, pulmonary embolism, unplanned re-intubation, on ventilator for more than 48 hours, acute renal failure, sepsis, and septic shock.
Independent Risk Factors for Adverse Outcomes
Adverse outcomes evaluated were occurrence of postoperative complication, prolonged LOS, and discharge to rehab/skilled nursing. Postoperative complications included those listed above. Prolonged LOS was defined by the patient spending greater than 5 days in the facility. Discharge disposition was either to home or to a rehab/skilled nursing facility.
Statistical Analysis
All statistical analyses were performed with SPSS version 26 (IBM Corporation). Patient demographics and perioperative data were compared using Fisher’s exact test and χ2 test for categorical variables, and independent samples t test for continuous variables. Logistic and Poisson regressions were used to calculate odds ratios (ORs) and confidence intervals (CIs) of any complications, number of complications, and independent risk factors. Tests were deemed significant with a P value less than .05 or, where applicable, a Bonferroni-Holm correction was done to determine an adjusted P value of .005.
Results
Demographics
The nonoctogenarian cohort included 1059 patients with a mean age of 63 years (range = 21-79 years), while the octogenarian group included 54 patients with a mean age of 83 years (range = 80-87 years). Both cohorts were composed of similar ratios of males to females. Racial distribution was also similar among the cohorts. When compared to the nonoctogenarian group, the octogenarian group had more patients with a BMI less than 24.9 kg/m2 (13.6% vs 25.9%) or 25 to 29.9 kg/m2 (35.1% vs 46.3%), while having fewer patients with BMI greater than 30 kg/m2 (P = .008). The octogenarian group also had more patients with a MC score of 1 (2.5% vs 7.4%) or greater than 2 (0.2% vs 1.9%, P = .006). The octogenarian cohort had fewer patients who were functionally independent (98.1% vs 94.4%, P = .028). The octogenarian group had less smokers (8.7% vs 3.7%, P = .311) and more nondiabetics (86.8% vs 96.3%, P = .116; Table 1).
Demographics of Octogenarian and Nonoctogenarian Patients Undergoing Primary Total Ankle Arthroplasty.
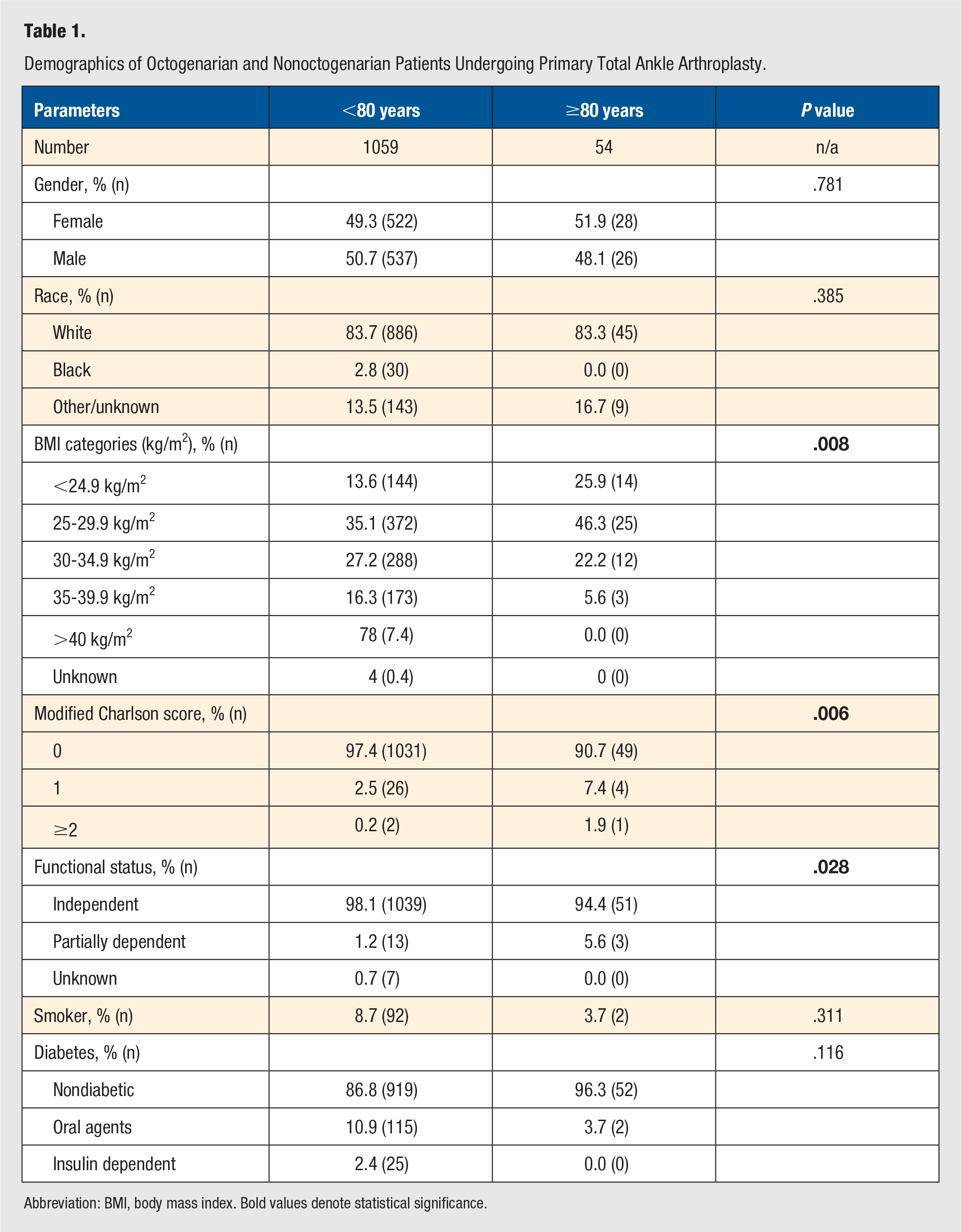
Abbreviation: BMI, body mass index. Bold values denote statistical significance.
Perioperative Factors
When compared to the nonoctogenarian group, the octogenarians were less likely to receive general anesthesia (89.8% vs 75.9%, P = .005). The octogenarians had higher ASA scores than the nonoctogenarians, but this did not reach statistical significance (P = .078). Octogenarians had shorter mean operative times (156.5 vs 146.0 minutes, P = .195), but significantly longer LOS (1.9 vs 2.5 days, P < .0001; Table 2).
Perioperative Factors of Octogenarian and Nonoctogenarian Patients Undergoing Primary Total Ankle Arthroplasty.
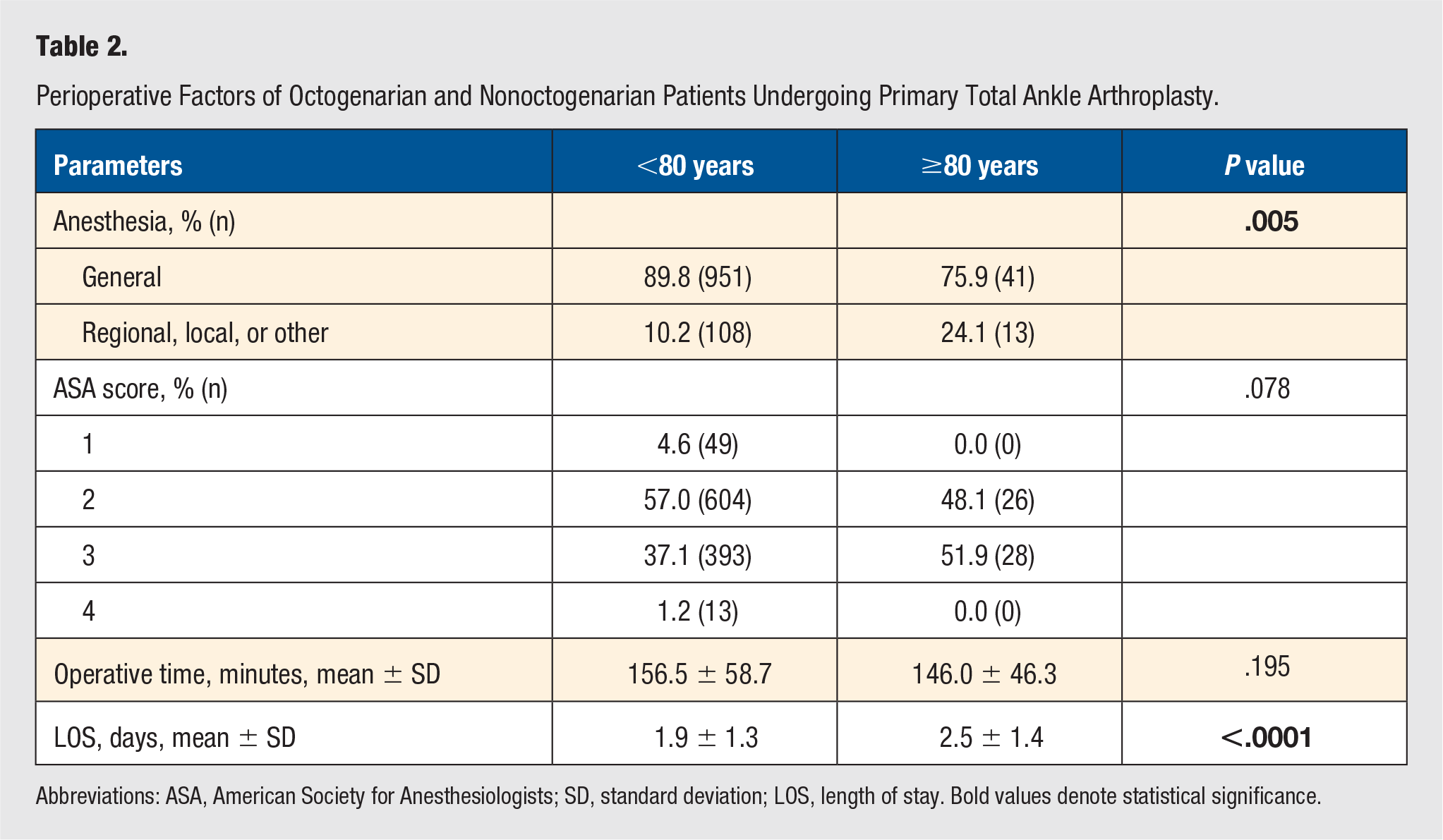
Abbreviations: ASA, American Society for Anesthesiologists; SD, standard deviation; LOS, length of stay. Bold values denote statistical significance.
Postoperative Complications
The octogenarian cohort had higher incidence of postoperative complications (3.7% vs 2.4%). Nevertheless, while controlling for sex, race, BMI category, and MC score, those patients greater than 80 years of age were not at significantly higher risk to develop any complication (OR = 1.32; 95% CI = 0.29-6.04; P = .722). Additionally, the octogenarian cohort was not at significantly higher risk of increased number of complications (OR = 1.18; 95% CI = 0.27-5.18; P = .820; Table 3).
Risk of Postoperative Complications of Octogenarian Compared to Nonoctogenarian Patients Undergoing Primary Total Ankle Arthroplasty (This Includes Risk of Any Complication and Accounts for Increasing Number of Complications per Patient) a .
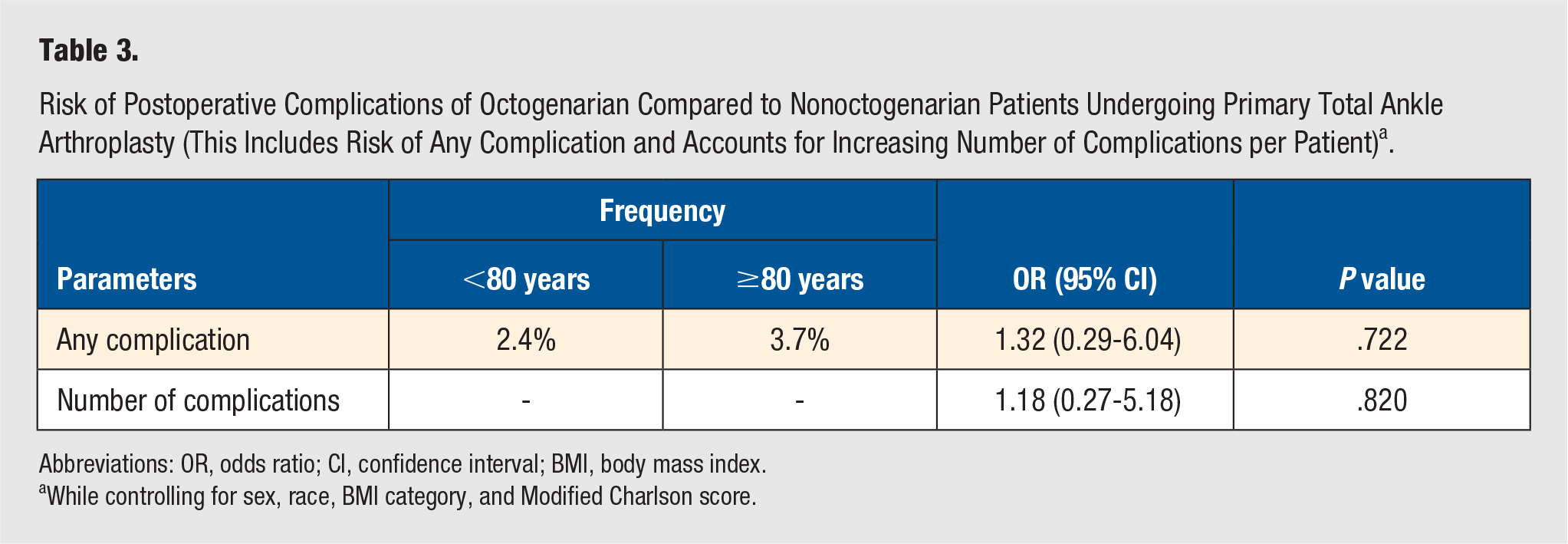
Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index.
While controlling for sex, race, BMI category, and Modified Charlson score.
Independent Factors of Adverse Outcomes
Analyzing the parameters in Table 4 independently, octogenarian was not a significant risk factor for development of any postoperative complication (OR = 1.66; 95% CI = 0.17-15.91; P = .521). Among all evaluated risk factors for complications, diabetes most closely approached statistical significance; insulin dependent patients having higher odds (OR = 5.33; 95% CI = 0.52-54.16; P = .038) of a complication than those taking oral agents (OR = 3.66; 95% CI = 0.84-15.88; P = .011).
Independent Risk Factors of Adverse Outcomes.
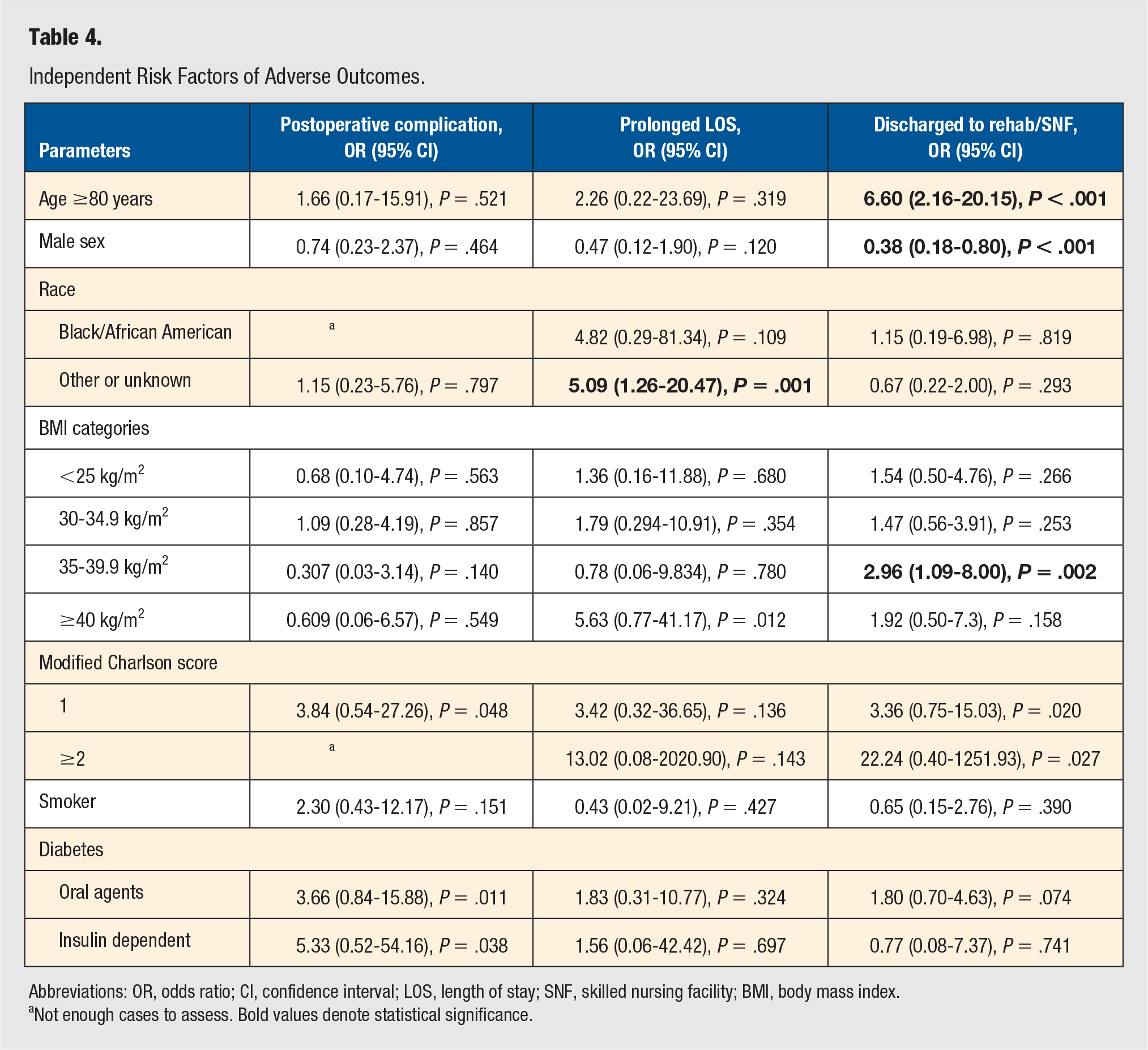
Abbreviations: OR, odds ratio; CI, confidence interval; LOS, length of stay; SNF, skilled nursing facility; BMI, body mass index.
Not enough cases to assess. Bold values denote statistical significance.
Octogenarians had increased odds of prolonged LOS (OR = 2.26; 95% CI = 0.22-23.69; P = .011) but this did not reach statistical significance. The patient’s race was found to be a risk factor, with those listed as other or unknown being significantly more likely to have a prolonged LOS (OR = 5.09; 95% CI = 1.26-20.47; P = .001). Patients with a BMI greater than 40 kg/m2 had an increased risk of prolonged LOS which closely approached but did not reach statistical significance (OR = 5.63; 95% CI = 0.77-41.17; P = .012).
Being an octogenarian was found to be a significant risk factor for discharge to a rehab/skilled nursing facility instead of home (OR = 6.60; 95% CI = 2.16-20.15; P < .001). Those patients with a BMI of 35 to 39.9 kg/m2 were also at significantly increased risk (OR = 2.96; 95% CI = 1.09-8.00; P = .002), while other BMI categories did not have as large of a risk or reach statistical significance. Male patients were found to be at a decreased risk of being discharged to a rehab/skilled nursing facility (OR = 0.38; 95% CI = 0.18-0.80; P < .001; Table 4).
Discussion
Utilization of TAA as treatment for end-stage arthritis in elderly patients has increased, paralleling the increasing demand for elective total joint arthroplasty in the knee, hip, and shoulder. Specifically, in the octogenarian age group there has been a 7- to 10-fold increase of TAA in recent decades as it continues to be an enticing alternative to ankle arthrodesis.15,16 Despite surgical advancements and improved outcomes in recent generations of implants, there is a lack of literature evaluating the risk of adverse events after TAA in octogenarians. As the number of primary TAAs continue to rise, identifying the impact of age on early postoperative outcomes is essential. Octogenarian patients undergoing TAA, despite having significantly higher MC scores, were not at a significantly higher risk for any, or increased, perioperative or postoperative complications when compared to a younger cohort. The octogenarians had a significantly longer hospital LOS. Additionally, when looking at independent risk factors for prolonged LOS, octogenarians had increased odds, but this did not reach statistical significance. Despite their advanced age and higher preoperative risk profile, octogenarian patients may not be at the perceived risk for perioperative and early postoperative adverse events. The results of this study reflect the perioperative complications in the elderly following TAA, and the importance of other risk factors aside from advanced age.
Although our study relied on a large amount patient data, certain limitations need to be considered. First, there are limitations inherent to the NSQIP database. The NSQIP database collects data for the first 30 postoperative days, limiting long-term data analysis. In addition, the database does not collect data on quality outcomes, such as pain and functional scores. Evaluating functional outcomes of octogenarians would expand the validity of our study. CPT codes are used to identify patients in the NSQIP database, and when potential miscoding is considered, incomplete patient capture is a risk. In addition, misclassification of data is a concern when using database information. NSQIP data entry is done by surgical clinical reviewers, medical professionals, and misclassification of data is reduced with their use of the ACS NSQIP Data Definition Committee. Although low, it is important to mention the less than 1.8% interrater reliability disagreement within ACS NSQIP. 27 Our sample size, while stemming from an extensive database, would benefit from further patient cases. This is an intrinsic limitation when studying TAA, because even with the growth noted, there are still limited number of cases performed annually. 31 Last, the short follow-up time stays consistent with our intended focus; however, long-term data may demonstrate divergence of outcomes when comparing these cohorts. To the best of our knowledge, this is the first study evaluating early postoperative outcomes in octogenarians undergoing primary TAA. With consideration that this study is based on all available database cases and the number of octogenarians undergoing TAA, along with the literature, is limited, an a priori power analysis was not conducted. Performing a post-hoc power analysis on results that are not significant (octogenarian risk of any 30-day complication) would inherently reflect low power. This is potentially due to Type II error, or that the effect size of the octogenarian factor is too small to detect with available populations. Noting the larger effect size of other factors influencing postoperative complications (none significant after new threshold set by Holm-Bonferroni adjustment) and the effect size of the octogenarian factor on discharge disposition, the effect size of octogenarians on 30-day postoperative complications may be small and less clinically relevant than previously suspected. Therefore, the investigators believe that a power analysis would not provide further clarity of our results. Despite the limitations, this study broadens our understanding of risk factors of this expanding procedure.
The current literature contains limited studies on the impact of age on patients undergoing primary TAA; however, our results are consistent with these smaller studies. Demetracopoulos et al conducted a prospective study, from June 2007 to July 2011, examining the effect of age on outcomes of 395 patients undergoing primary TAA. When comparing 3 age groups (less than 55, 55 to 70, greater than 70 years), they found no difference in wound complications and clinical outcomes with a mean 3.5-year follow-up. They also found no difference in the need for reoperation or revision surgery. 32 However, it is important to note their study differed in the length of follow-up. Tenenbaum et al performed TAA on a consecutive series of 21 patients older than 70 years followed by another series of 21 patients between 50 and 60 years. At minimum 1-year follow-up, they found equivalent improvements in clinical and gait outcomes among the 2 age groups. 33 Our study showed slightly higher incidence and odds of complications in the octogenarian group undergoing primary TAA, but this did not reach statistical significance. Furthermore, our study demonstrates the impact of a patient being an octogenarian, as an independent risk factor for development of complications, is not as influential as an increased MC score or being an insulin-dependent diabetic.
Prior orthopaedic literature has demonstrated age as an independent risk factor for postoperative complications. Easterlin et al used the 2005 to 2009 NSQIP database to evaluate the effect of age on short-term complications on elderly patients undergoing primary total knee arthroplasty. They found that early postoperative complications began to significantly increase starting at age 70, with mortality rates highest for those age 85 years and older. 34 Nevertheless, the surgical stress the patient undergoes varies with different procedures, and patient selection criteria may differ across subspecialties. While our study did not find age above 80 years to be a significant independent risk factor for postoperative complications, octogenarian patients had higher odds of discharge to rehab/skilled nursing instead of to home. Yoshihara and Yoneoka, using the 2000 to 2009 National Inpatient Sample, studied the trends of in-hospital outcomes on patients over age 80 undergoing elective major orthopedic surgeries. Unlike our results, which showed no significant difference among the different age groups, their study demonstrated significantly higher overall in-hospital complication and mortality rates of the octogenarian patients when compared to the matched younger cohort. 5 The authors stated that the differences observed, although significant, were small. Given the lack of data focused on TAA outcomes, it is presumptive to extrapolate results from other studies, of different orthopaedic subspecialties, to foot and ankle surgery. Despite previous literature suggesting age to be a major risk factor for postoperative complications, many of these studies analyzed orthopaedic procedures other than TAA.
As our elderly population expands, our understanding of the risks and benefits of orthopaedic procedures must expand with it. TAA can improve a patient’s quality of life, but with limited data, we must strive to better optimize surgical indications. Despite previous literature suggesting age as an independent risk factor for postoperative and perioperative complications in patients undergoing orthopaedic procedures, this should not dissuade consideration for elective TAA in elderly patients. Our intent was to evaluate short-term outcomes in octogenarians undergoing elective TAA and provide a better understanding of the surgical risk in these patients. With higher MC scores and higher ASA scores, one may hypothesize higher postoperative complication rates. While the octogenarians had slightly higher incidence and odds of complications when compared to the younger population, there was no significant difference between the cohorts. Furthermore, octogenarian patients, as an independent risk factor for complications, had lower odds than other parameters, like MC score and insulin-dependent diabetes. When looking at independent risk factors for prolonged LOS, age 80 or greater was not a significant risk factor. However, octogenarians, and those with a BMI of 35 to 39 were significantly more likely, and males were significantly less likely, to be discharged to a rehab/skilled nursing facility instead of home. Orthopaedic surgeons may use this information when indicating elderly patients with end-stage arthritis for TAA and while discussing patient expectations and risks. Future studies extending the early follow-up to intermediate and long-term outcomes will only strengthen the literature on TAA. Prospective studies with a larger octogenarian population would provide longitudinal data to expand our current understanding, and further examine the long-term risks and benefits of the elderly undergoing TAA.
Supplemental Material
Hoenig_Power – Supplemental material for Short-Term Outcomes of Primary Total Ankle Arthroplasty in Octogenarians: A National Database Analysis
Supplemental material, Hoenig_Power for Short-Term Outcomes of Primary Total Ankle Arthroplasty in Octogenarians: A National Database Analysis by Matthew Partan, Nicholas Frane, Cesar Iturriaga, Prashant Matai and Adam Bitterman in Foot & Ankle Specialist
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Bitterman reports stock from ROM3 Rehab, outside the submitted work; and American Orthopaedic Foot and Ankle Society: Board or committee member; American Osteopathic Academy of Orthopedics: Board or committee member; and New York State Society of Orthopedic Surgeons: Board or committee member. The other authors do not disclose an conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Informed Consent
Not applicable.
Trial Registration
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.