
Abstract
Background
There remains no clear consensus on patient satisfaction and functional outcomes following synthetic cartilage implant (SCI) implantation for hallux rigidus. The purpose of this study was to review our experience at a single academic institution using an SCI for treatment of hallux rigidus.
Methods
A retrospective review was performed of patients who underwent the SCI procedure for treatment of hallux rigidus between January 2017 and May 2019. Functional outcomes were evaluated using Patient-Reported Outcome Measures Informational System (PROMIS)-10 scores as well as a survey investigating patient satisfaction, self-reported clinical improvement, and changes in sporting ability. Patients were divided into satisfied versus unsatisfied subgroups, and between-group differences in preoperative variables and complications were reviewed. A total of 90 patients (96 implants) were included in this study. The mean follow-up time was 26.4 months.
Results
In all, 81.2% of patients reported that their foot was “much improved” (55.2%) or “improved” (26.0%) since undergoing the SCI procedure, whereas a slightly lower percentage, 74.0%, stated that they were “extremely satisfied” (41.7%) or “satisfied” (32.3%) at final follow-up. Patients were able to tolerate higher impact sporting activities after the procedure, and 75.0% of patients stated they would have the same surgery again. PROMIS-10 T-scores averaged 54.2 points for physical health and 57.4 points for mental health. Only 2.1% of patients required conversion to arthrodesis. Significant differences between the satisfied versus unsatisfied subgroups were found in preoperative corticosteroid injection use (21.1% vs 41.1%, respectively; P = .029) and preoperative VAS pain score (8.2 vs 7.1, respectively; P = .036).
Conclusion
The SCI procedure can be a viable option for treating hallux rigidus with high satisfaction overall, increased sport activity levels, and a very low revision rate. However, maximizing patient satisfaction may require more careful consideration of preoperative prognosticators and extensive patient counseling to ensure realistic expectations for recovery time and individual outcome.
Level of Evidence:
Level IV: Retrospective case series
“Cheilectomy with or without proximal phalanx osteotomy has demonstrated good clinical outcomes for treatment of low-grade hallux rigidus.”
Introduction
Degenerative arthritis of the first metatarsophalangeal (MTP) joint, which is known as hallux rigidus, is the most common arthritic condition of the foot and affects 1 in 40 people older than 50 years in the United States. 1 The first metatarsal plays a critical role in the mechanics of the foot and bears up to 119% of body weight during the gait cycle, particularly during the push-off phase. 2 Any pathology, including arthritis, that induces pain or loss of joint motion may negatively affect the biomechanics of this joint and result in functional disability and decreased quality of life for patients.
The progression of first MTP joint arthritis is characterized by destruction of articular cartilage, periarticular inflammation, joint space narrowing, and periarticular osteophyte formation, all of which contribute to limited joint mobility. 3 These arthritic changes result in increased friction and tension between the metatarsal head and proximal phalanx, which in turn translate to increased pain with motion across the narrowed arthritic joint. Thus, avoidance of excessive MTP joint movement has long been a key strategy of nonsurgical hallux rigidus management, with therapies ranging from stiff-soled or rocker bottom shoes to orthotics such as carbon fiber footplates. Although nonoperative strategies should certainly be trialed in patients first presenting with symptomatic hallux rigidus, Grady et al 4 reported a modest 55% success rate of conservative care alone, which included shoe modification, orthotics, and corticosteroid injections.
Symptomatic patients who fail conservative management should be considered for surgery. Cheilectomy with or without proximal phalanx osteotomy has demonstrated good clinical outcomes for treatment of low-grade hallux rigidus.5-9 However, for advanced stage hallux rigidus (grade IIIb or IV), Coughlin and Shurnas 10 recommend arthrodesis instead. First MTP joint arthrodesis has long been considered the gold standard of hallux rigidus treatment because of its reliability in relieving pain and achieving excellent functional outcomes for patients11-14; however, sacrifice of first MTP joint mobility is an inevitable consequence of the procedure. Rising concern over altered postoperative forefoot biomechanics, reduced capacity for certain activity types, and restricted footwear selection has fueled the search for surgical treatments capable of mitigating pain while preserving joint motion, such as hemiarthroplasty or total joint arthroplasty with silicon, metal, and ceramic implants.15-17 Unfortunately, multiple implant arthroplasties have demonstrated high rates of failure as a result of implant fragmentation, loosening, and wear debris.18-21
In 2016, the United States Food and Drug Administration approved a new option for hallux rigidus treatment: a small (8-10 mm) polyvinyl alcohol (PVA) hydrogel-based implant (Cartiva; Wright Medical, Memphis, TN) designed to act as a joint spacer via implantation into the metatarsal head with 1 to 2 mm of distraction. 22 Unlike previous prostheses, this new synthetic cartilage implant (SCI) had a water content, compressive modulus, and tensile strength all comparable to healthy human articular cartilage.23,24 The multicenter Cartiva MOTION Study Group reported very encouraging results regarding the efficacy and safety of this implant, with pain relief and functional outcomes comparable to first MTP joint arthrodesis at 2 years of follow-up and excellent implant survivorship at midterm follow-up.25,26 Several recent studies investigating SCI implantation, however, have failed to match the favorable outcomes of the Cartiva MOTION Study Group.3,27,28 Cassinelli et al 27 notably reported presence of mild pain, physical dysfunction, and only “neutral” patient satisfaction at postoperative follow-up of 18.5 months.
To date, there remains a shortage of information regarding patient satisfaction and functional outcomes following SCI implantation for hallux rigidus treatment in the United States. Further independent research from multiple non–industry-funded groups may be required to fully characterize the efficacy and safety of this attractive treatment option. The purpose of this study was to review our experience at a single academic institution using an SCI for treatment of hallux rigidus.
Methods
Approval was obtained from our institutional review board prior to the initiation of this study, and verbal informed consent was obtained from all patients before the study. All patients who received an SCI for treatment of hallux rigidus at a single academic institution with 1 of 3 foot and ankle fellowship-trained orthopaedic foot and ankle surgeons between January 2017 and May 2019 were reviewed. Patients chosen for this study met the following inclusion criteria: (1) 18 years of age or older, (2) diagnosed with hallux rigidus, (3) underwent SCI (Cartiva) procedure, and (4) at least 1 year out from surgery at the time of study initiation. Patients who had prior SCI procedure for hallux rigidus or underwent PVA hydrogel implantation for lesser MTP joints were excluded from this study.
Charts were reviewed for perioperative patient data, including age at surgery, sex, body mass index (BMI), smoking status, diabetes mellitus, rheumatoid arthritis, history of prior hallux surgery, history of corticosteroid injections prior to and after the index surgery, presence of preoperative sesamoiditis symptoms, implant size, and additional procedures performed at the time of the index surgery. Preoperative weight-bearing anteroposterior and lateral radiographs of the foot were reviewed to assess intermetatarsal angle (IMA), hallux valgus angle (HVA), and hallux rigidus grade as defined by the Coughlin and Shurnas 10 grading system. All complications, including reoperation, infection, and wound problems were reviewed for each patient.
To evaluate post-SCI patient satisfaction, self-reported clinical improvement, and changes in sporting ability, a questionnaire was designed with the following core queries: (1) How would you describe your foot now compared to before the surgery? (2) How satisfied are you with the outcome of the procedure you had done? (3) Would you have the same surgery again under the same circumstances? Answer choices to the first 2 questions were based on a 5-point Likert scale, whereas patients indicated “yes,” “no,” or “unsure” for the third. Preoperative and postoperative pain Visual Analog Scale (VAS) score and Patient-Reported Outcome Measures Informational System (PROMIS)-10 scores were also collected for each patient to better quantify clinical improvement. Patients were asked to describe their exercise and other physical activities before and after the surgery, which were categorized as “low-impact,” “mid-impact,” and “high-impact” 29 activities based on conventions set forth by Usuelli et al. 29 Using these definitions, low-impact activities focus on stretching, breathing, or slow movements and require only body weight weight-bearing (eg, yoga, pilates, swimming, bicycling); midimpact activities include moderate-intensity movements such as dance and Zumba; and high-impact activities involve contact sports, forceful ground impact, or intense weight-bearing (eg, volleyball, football, rugby). The questionnaire was administered via telephone survey by an author who was not involved in perioperative patient care. The full survey template including the complete survey results and PROMIS-10 questionnaire can be found in Appendixes A and B (Supplemental material, available online), respectively.
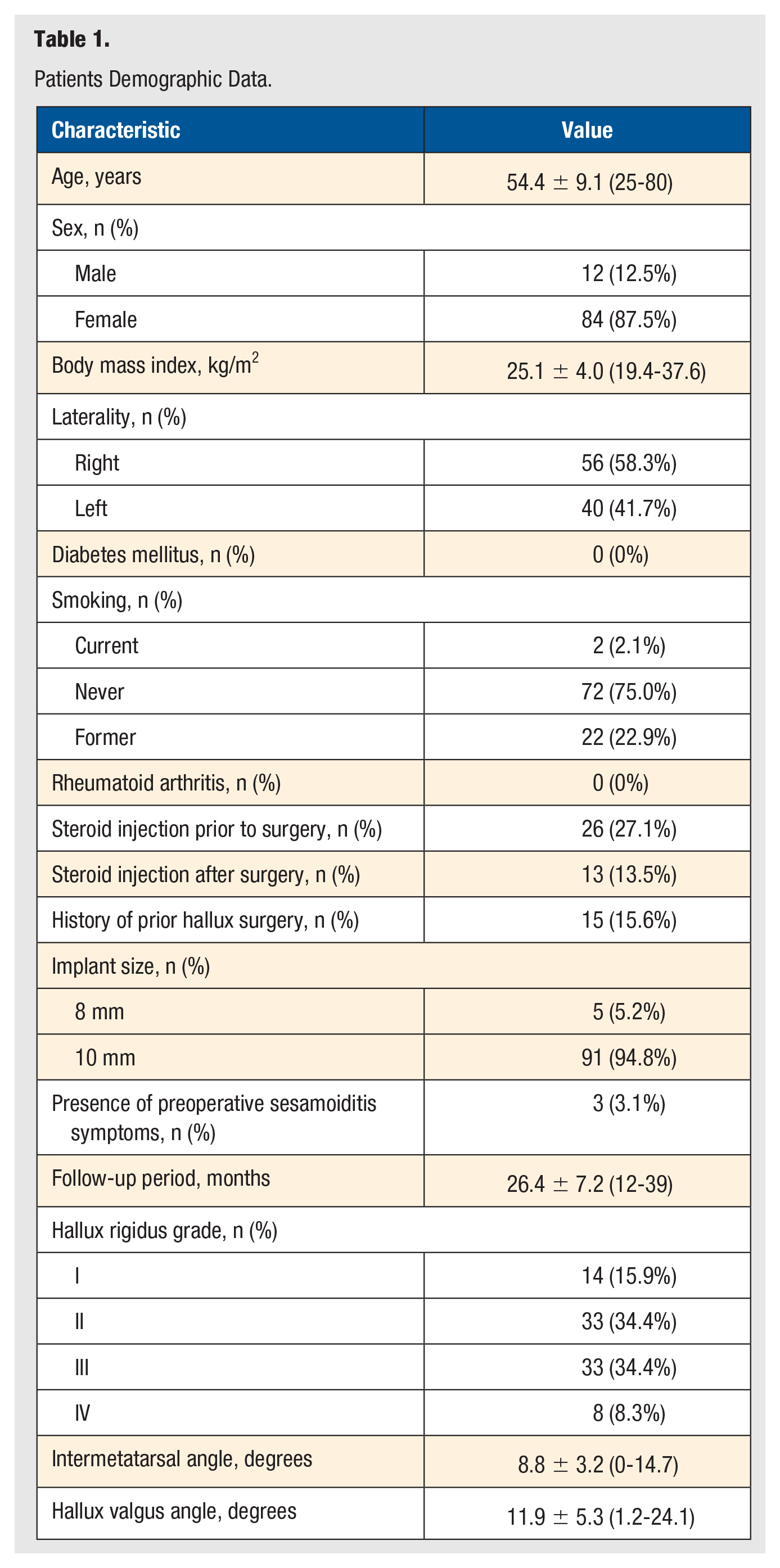
A total of 116 consecutive patients (124 implants) were included in this study initially, but 2 patients (4 implants) declined to join the study, and 24 patients (24 implants) could not be reached for the survey. Finally, a total of 90 patients (96 implants) were included in this study: 12 (12.5%) men and 84 (87.5%) women (Table 1). The mean age at the time of surgery was 54.4 ± 9.1 years (range, 27 to 74). Cohort BMI averaged 25.1 ± 4.0 kg/m2 (range, 19.4 to 37.6). The mean follow-up period was 26.4 ± 7.2 months (range, 12 to 39). Review of preoperative foot radiographs identified 14 cases of grade I (15.9%) hallux rigidus, 33 cases of grade II (34.4%), 33 cases of grade III (34.4%), and 8 cases of grade IV (8.3%). Mean preoperative IMA was 9.3° ± 2.5° (range, 2.9° to 14.7°), and mean HVA was 11.9° ± 5.3° (range, 1.2° to 24.1°).
Patients Demographic Data.
The standard operative technique for SCI implantation, which has been described in previous publications,25,30,31 was used in this study. A longitudinal incision through the skin was made over the dorsal first MTP joint, and the extensor hallucis longus tendon was identified, mobilized, and retracted. A dorsal capsulotomy was created, and the head of the metatarsal was exposed subperiosteally. The great toe was then placed in maximum plantar flexion using a McGlamry retractor to mobilize the joint if necessary. The dorsal osteophytes of the metatarsal head were removed, and the edges of the head were smoothed with a rongeur. Osteophytes on the dorsal aspect of the proximal phalanx were also removed if necessary. After using the sizer to ensure adequate room to place a properly sized SCI (8 or 10 mm), a guide pin was placed. A reamer was used to create the cavity for the implant. An appropriately sized SCI was placed using the implant delivery tube and seated in the first metatarsal head approximately 1 to 2 mm proud relative to the adjacent native cartilage. Great toe mobility was assessed to ensure full range of motion (ROM) without impingement. A thin layer of bone wax was placed over the exposed dorsal metatarsal bone. Layered closure of the capsule, and subsequently the skin, was performed. A compression soft dressing was applied along with a postoperative shoe. Patients were permitted to bear weight as tolerated in the postoperative shoe and begin ROM exercises at 1 week postoperatively. At 2 weeks postoperatively, sutures were removed, and patients could return to wearing their regular shoes as pain and swelling permitted.
SPSS software (version 21.0; IBM, Armonk, NY) was used for all statistical analyses. Data are presented as means and SDs. The Student t-test was used for between-group comparisons of continuous or continuous ranked data such as age, BMI, VAS pain score, IMA, and HVA. The χ2 test or Fisher exact test was used to compare categorical variables such as smoking, implant size, corticosteroid injection prior to the index surgery, presence of preoperative sesamoid symptoms, hallux rigidus grade, and sports impact level. The level of statistical significance was set as P <.05.
Results
More than 80% of patients reported an improvement in their symptoms after being treated with SCI for hallux rigidus, with 55.2% (53/96) of patients describing their foot as “much improved” and 26.0% (25/96) as “improved.” When asked if they would choose to have the surgery again under the same circumstances, 75% (72/96) of patients answered “yes,” whereas 22.9% (22/96) responded “no” and 3.1% (3/96), “not sure.” As a corollary to this question, patients were asked if they would recommend the same surgery to family or friends who were in a similar situation. To this, 69.8% (67/96) of patients responded “yes,” 17.7% (17/96), “no,” and 12.5% (12/96), “not sure.” In terms of satisfaction with their clinical outcomes, 41.7% (40/96) of patients described themselves as “extremely satisfied,” 32.3% (31/96) as “satisfied,” 8.3% (8/96) as “neutral,” 8.3% (8/96) as “unsatisfied,” and 9.4% (9/96) as “extremely unsatisfied.” Only 6 patients (6.3%) reported that they would have undergone first MTP joint arthrodesis rather than synthetic cartilage implantation had they known the results they have now ahead of time.
For more granular evaluation of the time frame over which patients experience clinical improvement, we stratified the postoperative recovery period into 4 different time frames: 0 to 3 months, 3 to 6 months, 6 to 12 months, and 12+ months. Overall, 57.3% (55/96) of patients stated that they first noticed improvement from their preoperative baseline within postoperative 3 months; 15.6% (15/96) noted improvement starting within 3 to 6 months, 7.3% (7/96) within 6 to 12 months, and 3.1% of patients (3/96) after 12 months. Unfortunately, 12 patients out of 96 did not note any improvement in their symptoms after surgery. The time to “new normal” was even longer: 25.0% (24/96) of patients reported reaching this state within 3 months, 17.7% (17/96) within 3 to 6 months, 34.4% (33/96) within 6 to 12 months, and 10.4% (10/96) in more than 12 months; 10 patients responded that they had not achieved a new normal feeling since the operation. The key survey results are shown in Table 2.
Key Results of the Survey Investigating Patient Satisfaction and Their Clinical Status.
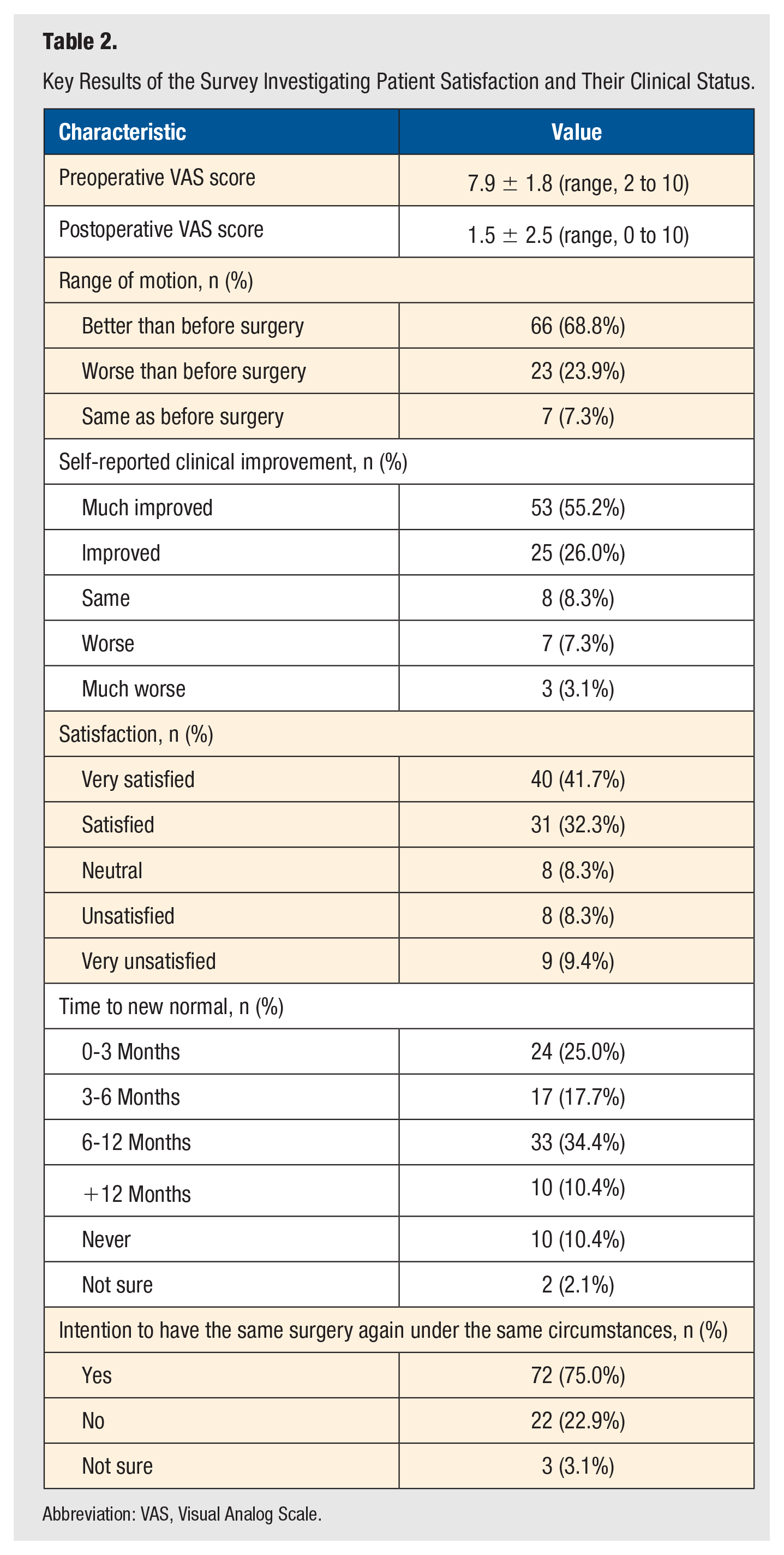
Abbreviation: VAS, Visual Analog Scale.
At final follow-up in this study, PROMIS-10 physical health T-scores averaged 54.2 ± 8.3 points (range, 26.7-67.6), which corresponds to a label of “very good” (from excellent, very good, good, fair, and poor). 32 PROMIS-10 mental health T-scores averaged 57.4 ± 7.8 (range, 31.3 to 67.6), corresponding to a label of “excellent.” For reference, the average T-score for the overall US population is 50, and our cohort’s comparatively high T-scores reflect their satisfaction with their clinical outcomes following the SCI procedure, as corroborated by the survey responses. VAS pain scores also demonstrated significant improvement from 7.9 ± 1.8 (range, 2 to 10) preoperatively to 1.5 ± 2.5 (range, 0 to 10) postoperatively (P < .001).
Preoperatively, 92.7% of patients (89/96) in this study reported participating in sports or other types of physical activity: 59.4% (57/96) partook in low-impact activities, 17.7% (17/96) in midimpact activities, and 15.6% (15/96) in high-impact activities. After the SCI procedure, 97.9% (94/96) of patients in our cohort were able to resume participation in sports and physical activities, with a slight increase in the impact levels that patients were able to tolerate after surgery (Table 3). This is reflected by the shift toward midimpact and high-impact activities postoperatively: 57.2% (55/96) reported participating in low-impact activities, 18.8% (18/96) in midimpact activities, and 20.8% (20/96) in high-impact activities. However, this change in sport impact levels from preoperative to postoperative did not reach statistical significance (P = .498).
Preoperative and Postoperative Level of Sports Activity.
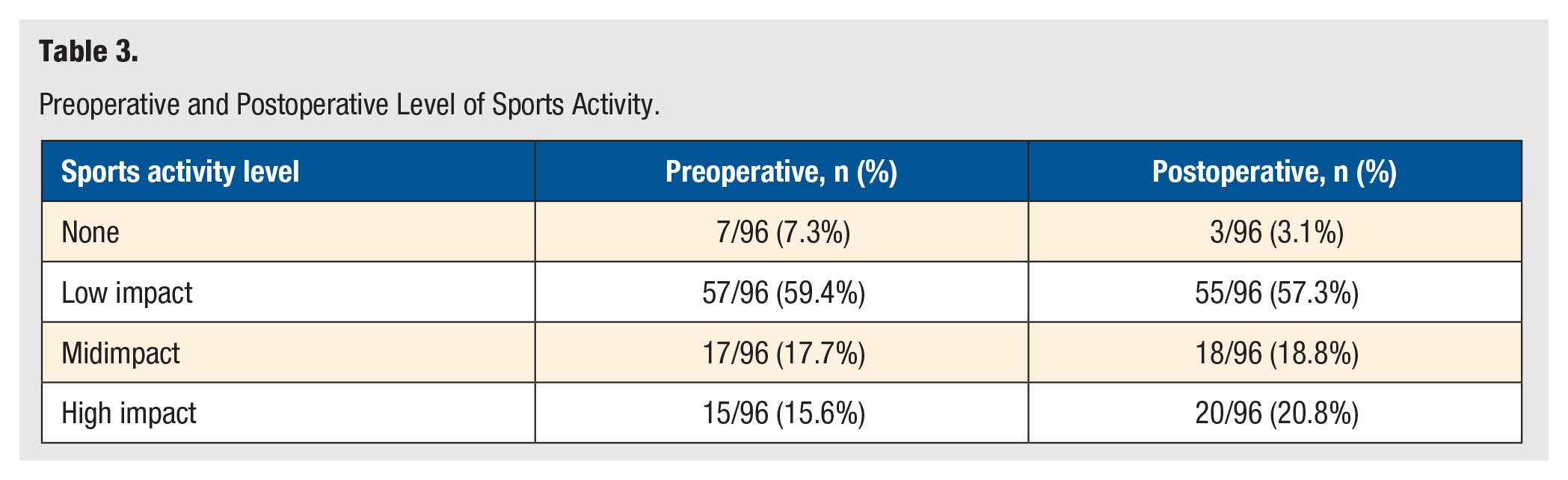
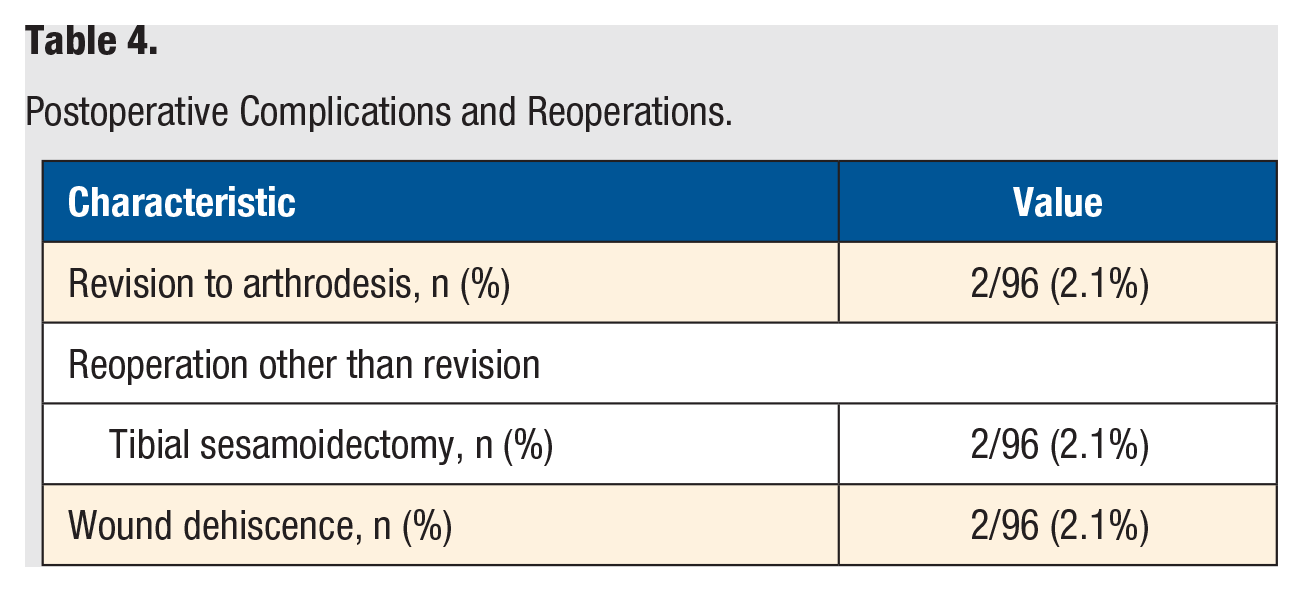
Table 4 summarizes the postoperative complication and reoperation data for the cohort in our study. Only 2 out of 96 patients (2.1%) required implant removal and conversion to arthrodesis, which took place an average of 18 months after the index surgery (one at 13 months and the other at 23 months). Apart from arthrodesis, reoperations on the affected foot included 2 cases of tibial sesamoidectomy procedures, which were performed for pain over the sesamoid area refractory to corticosteroid injections and metatarsal pads. Overall, we observed a very low complication rate in our cohort, with the only postoperative complications being 2 cases of superficial wound dehiscence, which were both managed with dressing changes only and resolved without antibiotic therapy or any additional procedures. There were no infection complications in our study.
Postoperative Complications and Reoperations.
Patients were divided into 2 subgroups based on the degree of their satisfaction: a “satisfied” group (n = 71, those responding “extremely satisfied” and “satisfied”) and an “unsatisfied” group (n = 17, those responding “unsatisfied” and “extremely unsatisfied”). Patients with “neutral” satisfaction (n = 8) were excluded from this subgroup analysis. We observed statistically significant differences in the rate of preoperative corticosteroid injections and preoperative VAS pain score between the 2 subgroups (P < .029 and P < .036, respectively; Table 5).
Comparison of Variables Between the Satisfied Group and the Unsatisfied Group.
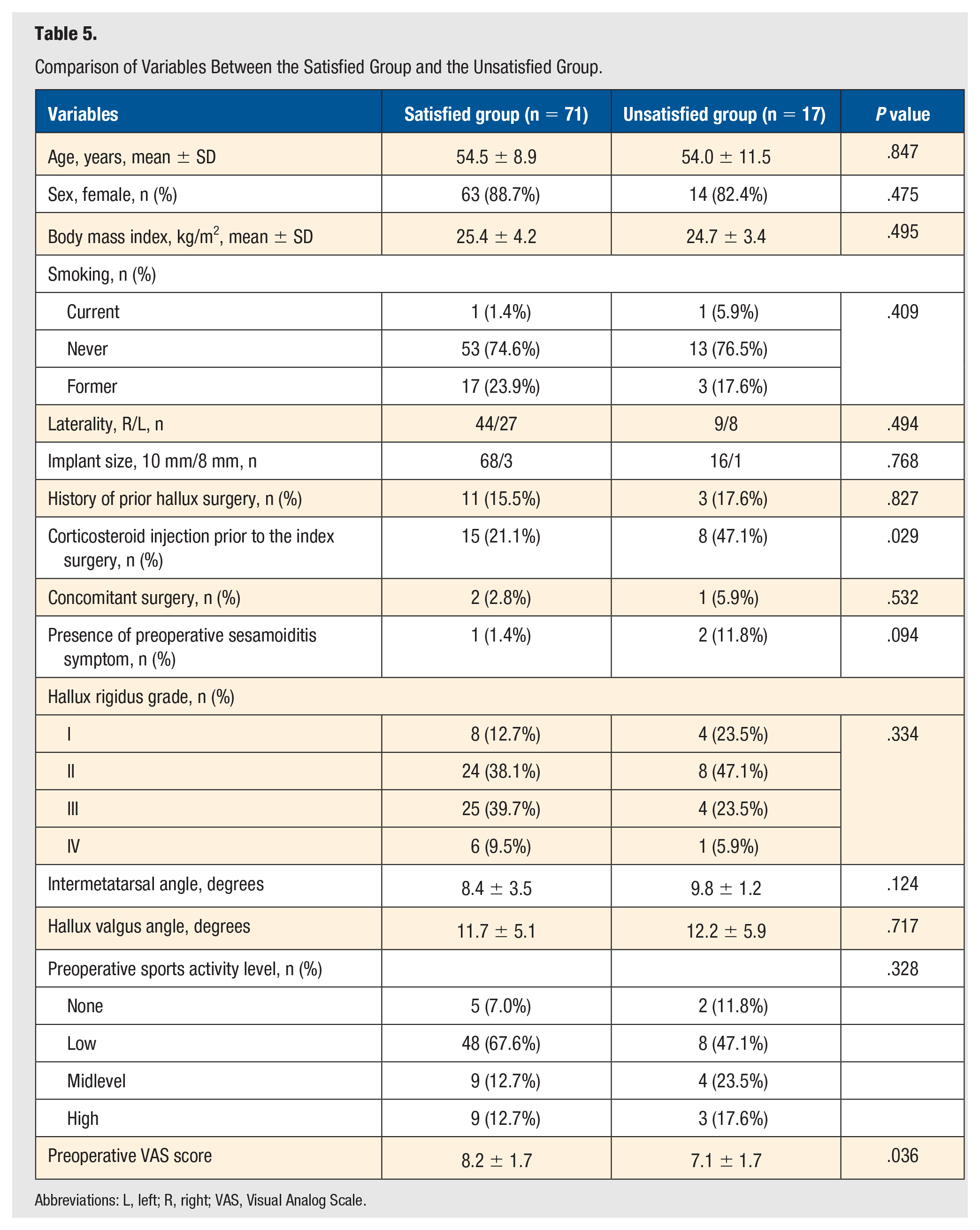
Abbreviations: L, left; R, right; VAS, Visual Analog Scale.
Discussion
This study reviewed our experience with synthetic cartilage implantation for treatment of hallux rigidus at a single academic institution. Overall, patients endorsed high levels of satisfaction and self-reported clinical improvement following the procedure. More than 80% of patients described their foot as “much improved” or “improved” at final follow-up, with 41.7% (40/96) of patients reporting feeling “extremely satisfied” and 32.3% (31/96) feeling “satisfied” with their outcome. 75.0% (72/96) of patients stated that they would have the same surgery again. PROMIS-10 T-scores averaged 54.2 points for physical health and 57.4 points for mental health, reflecting the cohort’s overall high satisfaction with their clinical outcomes. Only 2 patients (2/96, 2.1%) in this cohort converted to arthrodesis at 13 and 23 months. All these findings reflect the viability of the SCI procedure as an effective treatment option for hallux rigidus, with high patient satisfaction and excellent clinical outcomes.
Interestingly, we noted some discrepancy between patients’ self-reported clinical improvement and their overall satisfaction with the SCI. Although it would be reasonable to assume that patients who described their foot as “much improved” or “improved” would also be “extremely satisfied” or “satisfied,” the overall satisfaction rate was in fact lower than the self-reported improvement rate. In all, 81.2% of patients described their foot as “much improved” or “improved,” whereas only 74.0% reported that they were “extremely satisfied” or “satisfied.” Based on the survey results and further patient discussions, the relatively lower satisfaction rate may be largely explained by longer postoperative recovery times than patients initially expected, though the causes of this discrepancy are multifactorial. Although more than 50% of patients had reported improvement from their preoperative baseline within 3 months, 50% of patients required more than 6 months to reach a state that they described as their “new normal,” and 10 patients (10.4%) required more than 1 year before reaching this state. Furthermore, even patients who did indicate satisfaction with the procedure responded that they would hesitate to recommend SCI to their family or friends because of the extended recovery time. Also, 75.0% of patients stated that they would have the surgery again themselves, whereas only 69.8% stated that they would recommend it to others.
Additionally, although 17 patients (17.7%) described themselves as “unsatisfied” or “highly unsatisfied,” only 6 of these patients stated that they wished they had undergone first MTP joint fusion instead. The remainder stated that the loss of great toe mobility was incompatible with their lifestyle and would be unlikely to ever consider proceeding with arthrodesis. Of note, 23.5% of the unsatisfied patients (4/17) nonetheless described their foot as “much improved” or “improved” after the procedure and cited the source of their ongoing dissatisfaction not as a lack of improvement but as unfulfilled expectations as to what the implant would deliver (eg, total absence of pain, unimpaired return to high-impact activities, comfort in high-heeled shoes). These findings highlight not only the utmost importance of first MTP joint mobility for many patients, but also the different factors that may drive patients to pursue SCI versus first MTP joint arthrodesis in the first place. Although SCI may greatly benefit patients with symptomatic hallux rigidus who highly value first MTP joint mobility, it is impossible to overstate the importance of thorough preoperative discussion between physician and patient to ensure appropriate expectations for both length of recovery and final outcome.
Through a multicenter randomized controlled trial, the Cartiva MOTION Study Group reported that the SCI (Cartiva) showed equivalent pain relief and improved function when compared with the gold standard, first MTP joint arthrodesis, for advanced hallux rigidus. A total of 9.2% (14/152) of Cartiva cases resulted in conversion to a successful arthrodesis at 2 years of follow-up. 25 They also reported excellent outcomes in a midterm case series following a cohort of the survivors of the original multicenter randomized controlled trial, with 84% implant survivorship at a mean of 5.8 years of follow-up; 93.4% of patients reported that they would have the same surgery again. 26 In contrast, the single-surgeon cohort study by Cassinelli et al 27 reported a less optimistic rate of only 66% (42/64) of patients who would elect to have the SCI procedure again. The differing results between these 2 studies may stem from a myriad factors: study level (I vs IV), national demographic (Canada and the United Kingdom vs the United States), duration of follow-up (5.8 years vs 18.5 months), and so on. Compared to our study’s satisfaction rate of 74.0%, the study by Cassinelli et al reports that only 37.5% of patients described themselves as “extremely satisfied” or “satisfied.” Although the Cartiva MOTION Study Group has been diligent in producing studies that investigate the clinical outcomes of synthetic cartilage implantation for hallux rigidus, we observe that, thus far, there are very few non–industry-funded independent research groups that have done the same.3,27 Our current study represents a single-center investigation of clinical outcomes following a large number of SCI implantations. The results demonstrate high patient satisfaction overall, with a very low revision rate in our cohort of 2.1%. Given that further research from different groups is required before the clinical outcomes of this novel procedure can be fully understood, our hope is that the results of this study may be of benefit to orthopaedic surgeons seeking a more comprehensive understanding of patient satisfaction and outcomes of this procedure.
Notably, there has been a paucity of information on how SCI affects patients’ ability to tolerate sports and other physical exercise. Although the Cartiva MOTION Study Group included the Foot and Ankle Ability Measure (FAAM) Sports Scale as one of their outcome measures, there was no description of specific exercises that patients could tolerate before and after the surgery.25,33-35 Recently, Brandao et al 3 compared patient participation in various sports after arthrodesis versus Cartiva hemiarthroplasty for hallux rigidus and found no significant difference in FAAM sports scale between the 2 procedures. The most common physical activities enjoyed by patients after Cartiva hemiarthroplasty were “walking” (63%), “gym sports” (48%), and “running sports” (11%). However, because the scope of the Brandao et al study was limited to postoperative activities, any changes in exercise ability from patients’ preoperative baseline were unable to be determined. In this study, we observed that 100% of patients were able to return to activities with the same or higher impact level that they engaged in before surgery. Although more patients reported participating in midimpact or high-impact activities after the procedure compared with before, this difference did not reach statistical significance.
Appropriate patient selection is essential for ensuring successful outcomes following the SCI procedure. Goldberg et al 33 examined the association between patient factors and outcomes of first MTP joint SCI hemiarthroplasty versus arthrodesis and found similar success rates between the 2 procedures irrespective of gender, age, BMI, hallux rigidus grade, or preoperative symptom duration. Baumhauer et al 36 demonstrated the weak correlation between first MTP joint mobility, VAS pain score, and intraoperative cartilage loss to hallux rigidus grade, suggesting that clinical signs and symptoms, rather than radiographic parameters, should guide treatment. In concordance with these previous studies, we did not find a statistical difference in any preoperative variables, including hallux rigidus grade, age, BMI, gender, and smoking status, between our satisfied and unsatisfied subgroups. However, there were significant differences in the rate of corticosteroid injection prior to SCI and preoperative VAS pain score between the 2 subgroups. Both patients (2/96) who eventually converted to arthrodesis had corticosteroid injections before the index surgery. Obviously, we cannot conclude that corticosteroid injections negatively affect clinical outcomes or patient satisfaction after the SCI procedure, as a result of both insufficient sample size of our study and the various confounding factors that may drive patients to pursue corticosteroid therapy prior to surgery. More research is needed to fully characterize the relationship between corticosteroid injections and clinical outcomes of SCI procedure for hallux rigidus. Regarding the association between preoperative pain score and patient satisfaction, the satisfied subgroup reported higher preoperative VAS scores than the unsatisfied subgroup (8.3 vs 7.2; P < .05) but significantly lower postoperative VAS pain scores (0.5 vs 5.2; P < .001). The change in VAS score from preoperative to postoperative was markedly higher in the satisfied group compared with the unsatisfied group (7.7 vs 1.9; P < .001).
Limitations
There are several limitations to our study. First, this is a retrospective study with inherent susceptibility to bias and no control group. Second, patients were asked during the survey to evaluate their previous clinical status as well as their status at present. Because this information relies on patient memory, the possibility of memory decay bias or recall bias must be acknowledged. Third, our follow-up period was relatively short. Finally, we admit that there are few objective parameters in this study, such as postoperative radiographs or physician-evaluated ROM, that were used to characterize the effects of SCI. As we assume that patient satisfaction is a more meaningful clinical outcome than any radiographic parameter, patients who express satisfaction with the procedure are not followed with routine radiographic imaging at our institution.
Conclusion
Patients who received an SCI for hallux rigidus demonstrated high satisfaction overall, with increased sport activity levels and a very low revision rate. PVA hydrogel implant hemiarthroplasty can be a viable option for treatment of hallux rigidus; however, maximizing patient satisfaction may require more careful consideration of preoperative prognosticators, including steroid injection history as well as careful preoperative patient counseling to ensure realistic expectations regarding both recovery time and individual outcome.
Supplemental Material
sj-docx-1-fas-10.1177_19386400211001993 – Supplemental material for Patient Satisfaction Following Hallux Rigidus Treatment With a Synthetic Cartilage Implant
Supplemental material, sj-docx-1-fas-10.1177_19386400211001993 for Patient Satisfaction Following Hallux Rigidus Treatment With a Synthetic Cartilage Implant by Wonyong Lee, Carol Wang, Dan Prat, Keith L. Wapner, Wen Chao and Daniel C. Farber in Foot & Ankle Specialist
Supplemental Material
sj-docx-2-fas-10.1177_19386400211001993 – Supplemental material for Patient Satisfaction Following Hallux Rigidus Treatment With a Synthetic Cartilage Implant
Supplemental material, sj-docx-2-fas-10.1177_19386400211001993 for Patient Satisfaction Following Hallux Rigidus Treatment With a Synthetic Cartilage Implant by Wonyong Lee, Carol Wang, Dan Prat, Keith L. Wapner, Wen Chao and Daniel C. Farber in Foot & Ankle Specialist
Footnotes
Declaration of Confliction Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Keith L. Wapner, MD, reports being a consultant for Wright Medical, outside the submitted work. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.