
Abstract
Verrucous carcinoma is a rare form squamous cell carcinoma which appears similar to a wart. When it occurs in the feet, it can be easily misdiagnosed. It rarely metastasizes or recurs posttreatment. We report a case of a septuagenarian with recurrence of verrucous carcinoma diagnosed within 6 months at the site of previous treatment. Unique features in our patient’s clinical presentation include his advanced age, being nondiabetic, and the rapid recurrence of carcinoma.
Verrucous carcinoma is a rare form of low-grade squamous cell carcinoma with cauliflower-like lesions appearing similar to a wart.”
Case Report
A 74-year-old man presented with a thick eschar and a lesion to the dorsal right-foot great toe approximately 2 to 3 months after undergoing surgery (Figure 1). A biopsy, which was too superficial, revealed hyperkeratosis and parakeratosis consistent with the superficial portion of a verruca vulgaris; however, because the deeper component could not be visualized, verrucous carcinoma could not be ruled out. The patient at that time declined an additional biopsy and treatment for verruca, instead adopting a wait-and-see approach while self-treating the area with petroleum jelly.

Thick eschar to dorsal right great toe 3 months postoperatively.
After 7 months with no improvement, the patient returned for another biopsy, which was again too superficial. He continued to treat the lesion with petroleum jelly and hydrogen peroxide, and the malodor persisted. A third biopsy later that same month was confirmed by a dermatopathology tissue examination to be verrucous carcinoma (Figure 2). The following month, he was scheduled for Mohs micrographic surgery for a primary squamous cell carcinoma (verrucous carcinoma) of the right great toe and dorsal foot. He underwent a right-foot great-toe amputation and split-thickness skin graft (STSG; Figures 3 and 4). The patient had partial graft loss postoperatively, and patch grafting was performed in the tub room. Upon bolster take-down 2 days following this procedure, the patient again had partial graft loss, and he was scheduled for right foot debridement, STSG, and wound vac placement for approximately 4 weeks later.
Verrucous carcinoma is a rare form of low-grade squamous cell carcinoma with cauliflower-like lesions appearing similar to a wart.

Right foot lesion after dematopathology tissue examination confirmed verrucous carcinoma. Photo taken prior to Mohs procedure.

Right great-toe amputation and split-thickness skin graft.
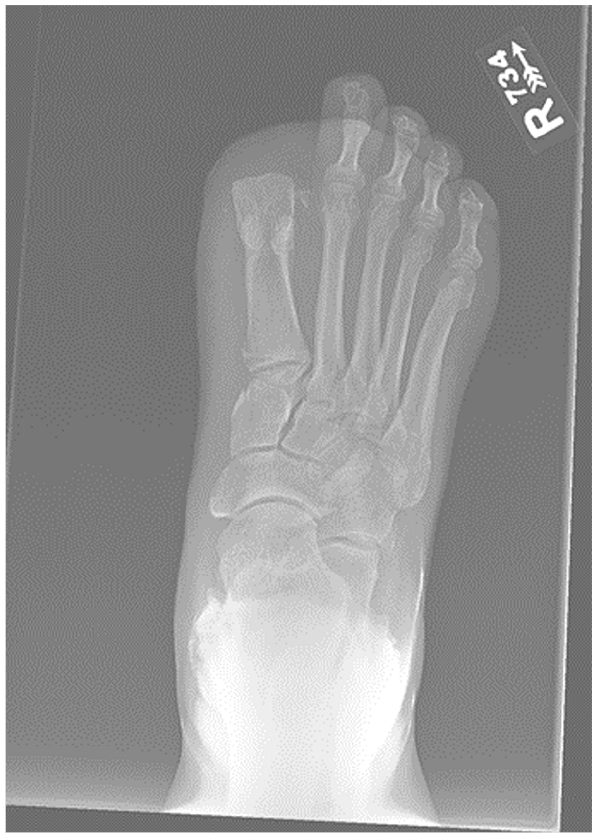
Radiograph of right great-toe amputation.
The patient was discharged from clinic with greater than 95% graft take and followed up weekly for 3 weeks postoperatively. Three months after his last follow-up, the amputation site had not completely healed. Physical examination revealed a small, cauliflower-shaped ulcer on the distal/plantar edge of the skin graft on the right foot. A 4-0 punch biopsy was performed on the amputation site and revealed epidermal hyperplasia with parakeratosis and downward-pushing borders, consistent with a recurrent verrucous carcinoma. Upon diagnosis, dermatology recommended midfoot amputation. One month later, the patient underwent transmetatarsal amputation (Figure 5). At that time, surgical pathology revealed ulcerated skin with pseudoepitheliomatous hyperplasia and no malignancy identified.
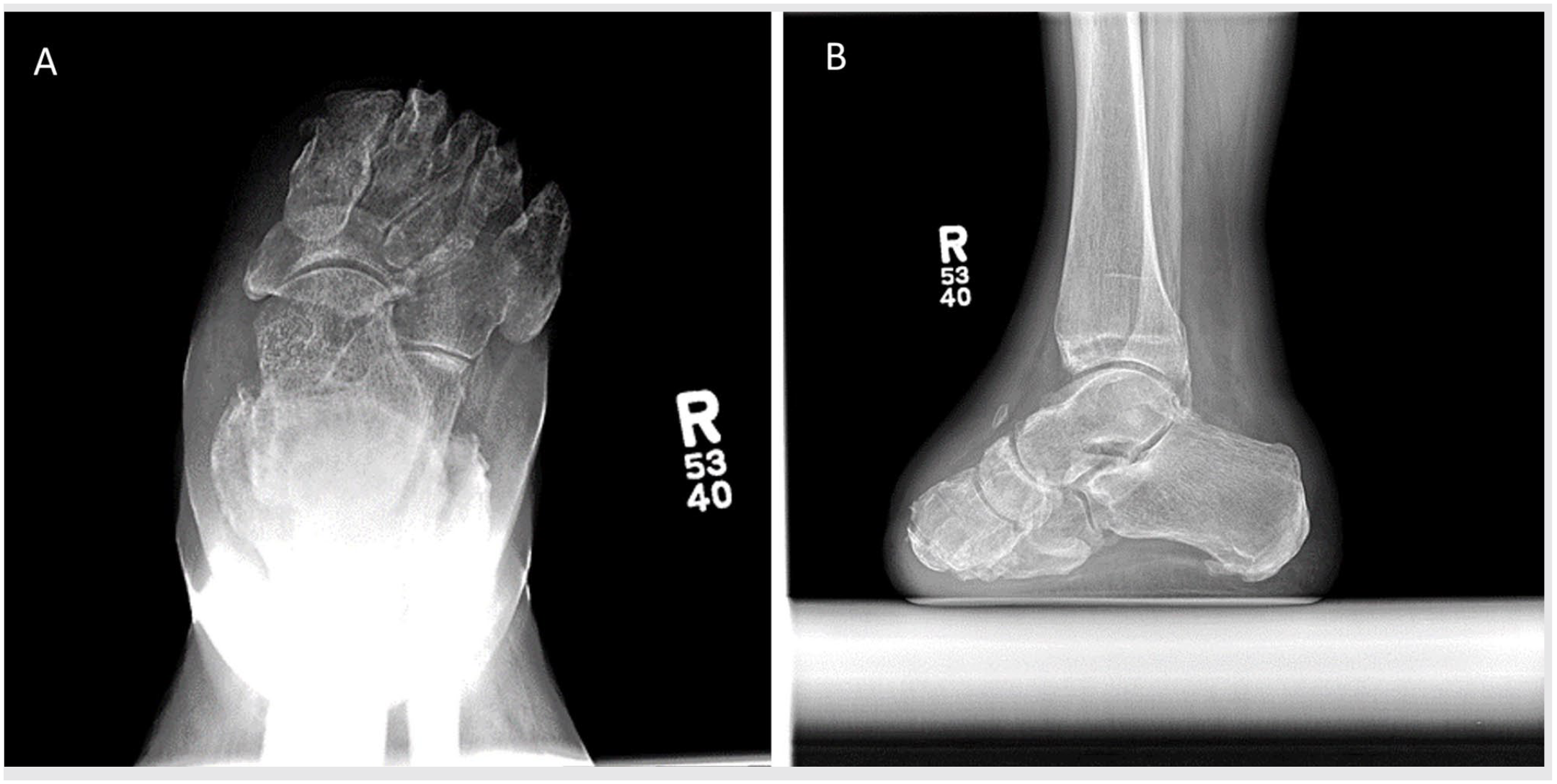
Radiograph of right foot transmetatarsal amputation: (A) anteroposterior, (B) lateral.
Discussion
Verrucous carcinoma is a rare form of low-grade squamous cell carcinoma with cauliflower-like lesions appearing similar to a wart. 1 It occurs in the oropharynx, genitalia, and feet, 2 and rarely metastasizes or recurs posttreatment. When patients present to clinic with these lesions, they are frequently misdiagnosed as warts or corns, leading the provider to treat the lesions with a topical cream for the presumed wart or corn. The locations of most common occurrence for verrucous carcinoma are the sole and ball of the foot. As such, these lesions can go undetected for years, especially when clinicians leave the feet unexamined. The carcinoma can also masquerade as other conditions, causing misdiagnosis of the lesions as actinomycosis, verruca plantaris, pseudoepitheliomatous hyperplasia, and plantar fibromatosis. Patients with verrucous carcinoma rarely experience metastasis and their survival rates are excellent.
Clinicians should be extremely vigilant about observing the appearance of a patient’s foot. If any suspicious-looking soft-tissue lesions (eg, warts, callus, corns) with unusual color, shape, texture, odor, or size are noted, a biopsy or referral to dermatology should be scheduled immediately. Most lesions appear to develop at surgical scar sites; our patient developed such a lesion at his amputation site. 3
Competency in obtaining a punch biopsy is critical to minimizing the risk of a misdiagnosis from the dermatopathology report. When obtaining a punch biopsy, the 2 or 3-mm punch biopsy instrument is gently pressed onto the skin area of concern. To ensure that both dermal and subcutaneous tissue is taken, rotate the punch biopsy instrument clockwise/counterclockwise and make a cut down to the level of the subcutaneous fat/tissue. Once done, gently pull out the biopsy instrument and use forceps and scissors to remove the biopsy sample and place into formalin.
The optimal approach to treat verrucous carcinoma is a wide, local surgical excision, 4 because it is difficult to intraoperatively differentiate between cancerous and noncancerous tissue. 1 Plastic surgery techniques used to cover the resultant surgical defect include full-thickness skin graft or radial forearm free flap. 1 Our patient received a STSG, but, despite wide excision, the cancer recurred. Several previously published surgical techniques, such as electrodessication, cryotherapy, and laser ablation, have been associated with a high rate of verrucous carcinoma recurrence. 4
The Mohs technique involves precise dissection using a microscope, which assists in total tumor excision while conserving most of the normal tissue structure, and has a history of being successful for patients with verrucous carcinoma. In clinical scenarios of high cancer recurrence, potential treatments include multiple surgical excisions of the tumor, toe/partial ray amputation, and below-knee amputation. 2 Most of the amputations result from the tumor invading soft tissue and/or bony involvement. As a foot and ankle specialist, this case highlights the need for vigilance, as squamous cell carcinoma can be easily misdiagnosed and can recur rapidly. Biopsies should be obtained immediately in cases of highly suspicious or unusual skin lesions, as dermatopathology reports are key to obtaining a correct diagnosis so that the patient can receive appropriate care in a timely manner by a multidisciplinary team of providers.
Footnotes
Authors’ Note
Work for this study was performed at The University of Texas Medical Branch, Galveston, TX.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: V.K.P. is a consultant for Stryker Orthopaedics as well as an editor for Lippincott Williams and Wilkins Publishing. The other authors have no conflicting interests to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.