
Abstract
The medial ankle ligamentous complex, which includes the deltoid, talocalcaneal, and calcaneonavicular ligaments, functions to provide stability to the medial ankle. Injuries to the deltoid ligament can lead to medial-sided ankle pain, subsequent instability, and posttraumatic osteoarthritis given the altered biomechanics of the ankle joint. After completing a thorough physical examination, imaging modalities such as stress radiographs and magnetic resonance imaging can be used to confirm the diagnosis. Acute injuries to the deltoid ligament should be managed conservatively with a short course of immobilization. For patients with continued pain and instability following a regimen of nonoperative management, surgical intervention can be considered. Primary repair using suture anchor fixation to the medial malleolus can be utilized if sufficient tissue remains. However, if reconstruction is necessitated, autograft or allograft can be utilized in several described techniques.
Keywords
“Deltoid ligament injuries have also been described in association with fractures of the lateral malleolus.”
Background
Ankle ligament injuries are among the most common injuries in the United States, occurring at a rate of 2.15 per 1000 person-years. 1 The vast majority of these occur on the lateral ankle; however, approximately 5% of ankle sprains involve the deltoid ligament. 1 Given the infrequent nature of these injuries, pathology on the medial side of the ankle is often neglected by orthopaedic providers. As little as 0.5% of deltoid ligament injuries will undergo surgery; however, chronic medial ankle instability may eventually undergo surgical intervention. 2
Recent consideration has been given to injury of the medial ankle ligamentous complex as a source of pathology leading to ankle instability. 3 Although the incidence in the general population has not been well described, Hintermann et al 4 reported a deltoid ligament injury rate of 40% in patients undergoing arthroscopy for lateral ankle instability. Deltoid ligament injuries have also been described in association with fractures of the lateral malleolus. 5 The purpose of this article is to provide a review of the current literature regarding medial ankle instability to highlight relevant anatomy, clinical evaluation, and management strategies.
Anatomy and Biomechanics
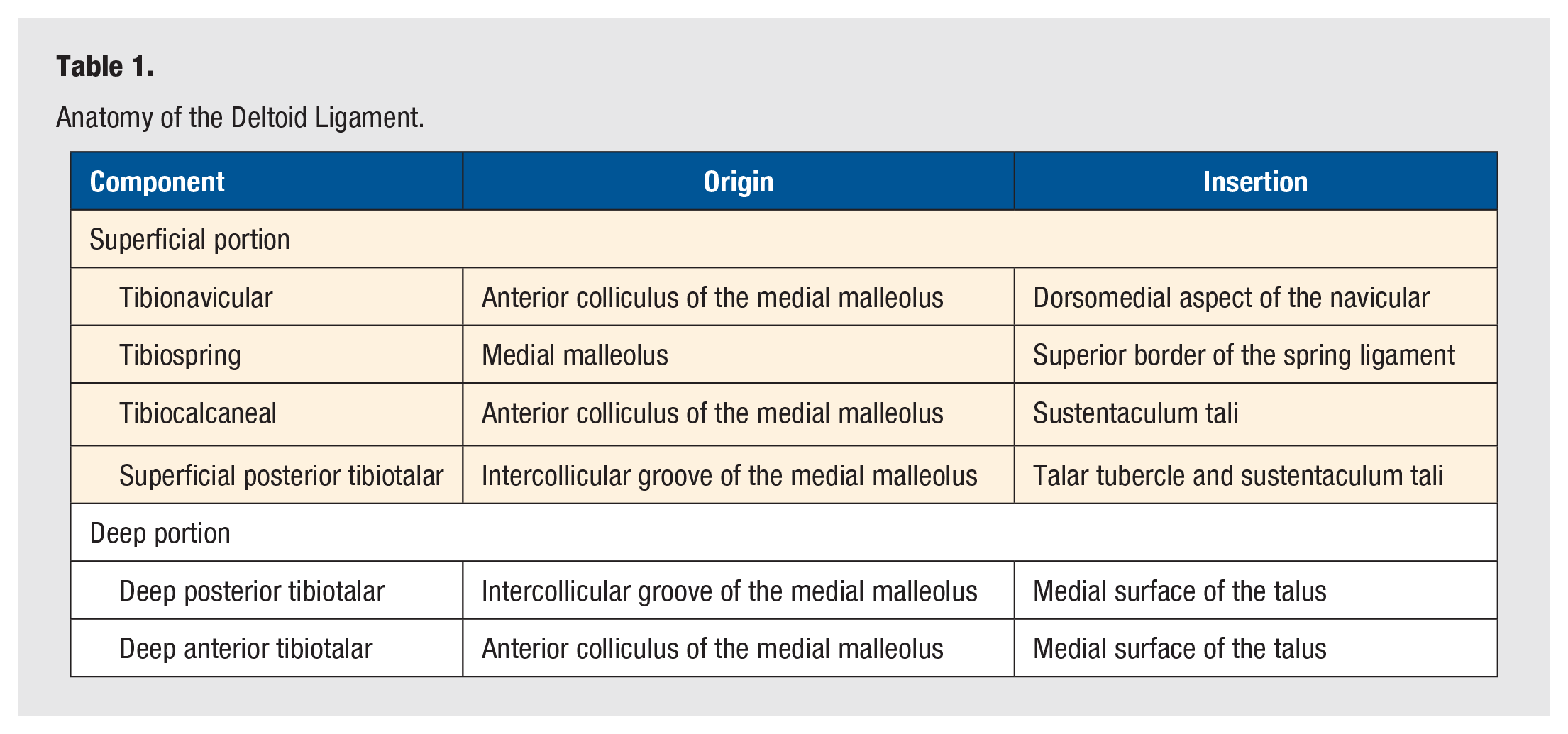
The deltoid ligament is a strong, broad ligament that stabilizes the medial aspect of the ankle joint complex. Although variations exist in anatomical descriptions, the deltoid ligament is generally considered to have superficial and deep components formed by multiple thickenings in a common capsular band. Figures 1 and 2 depict the anatomical origins and insertions of each of the superficial and deep deltoid components. In their examination of 40 ankle specimens, Milner and Soames 6 observed 4 superficial components and 2 deep components. The origin and insertion points for each of these are summarized in Table 1. Because portions of the superficial deltoid insert onto the calcaneonavicular (or spring) ligament, the spring ligament complex also helps stabilize the medial ankle joint, which can contribute to pathology when it is incompetent. 7
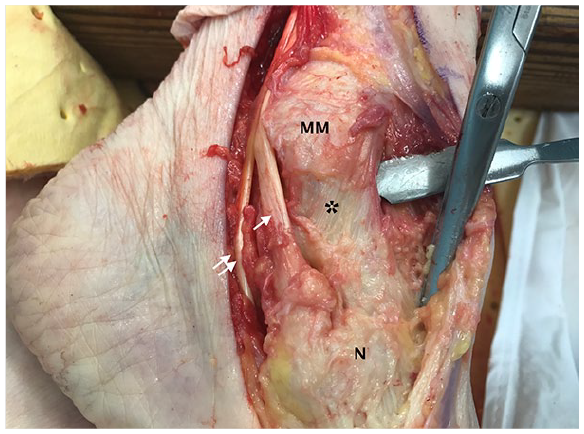
Superficial deltoid ligament: The superficial deltoid (*) originating on the anterior inferior aspect of the medial malleolus (MM) has a broad insertion on the navicular (N), plantar calcaneonavicular ligament, and sustentaculum tali of the calcaneus. The posterior tibialis tendon (single arrow) is shown coursing posterior to the medial malleolus and inserting on the navicular tuberosity. Flexor digitorum longus tendon (double arrow) is also shown.
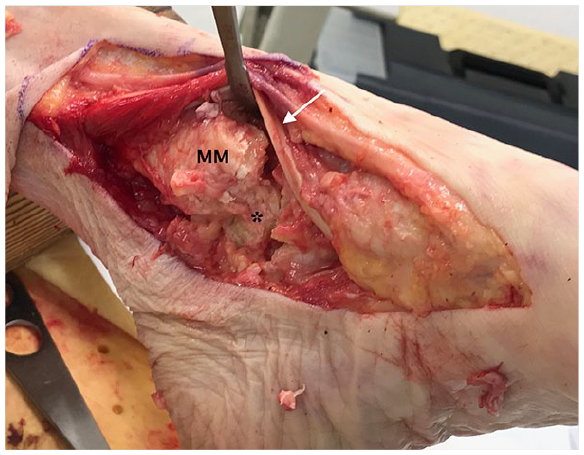
Deep deltoid ligament: The deep deltoid (*) lies deep to the superficial deltoid (excised). It originates on the posterior aspect of the anterior colliculus, intercollicular groove, and posterior colliculus of the medial malleolus (MM) and inserts on the medial aspect of the talus. Here, the posterior tibialis and flexor digitorum longus tendons are reflected anteriorly (white arrow).
Anatomy of the Deltoid Ligament.
The term medial ankle ligamentous complex is defined by the deltoid ligament, talocalcaneal ligament, and calcaneonavicular ligament. This complex provides a variety of important tasks that allow for maintenance of normal biomechanics at the ankle joint. The deltoid ligament in particular is essential to stability, with the deep deltoid primarily restraining talar translation, whereas the superficial deltoid primarily resists talar rotation. In a cadaver study, sectioning of the deep deltoid allowed for an increase of medial clear space to 3.7 mm, compared with less than 2 mm in intact specimens. 8 More recent studies have concluded that both superficial and deep components are equally responsible for resisting valgus tilting of the talus. 9 Using an osseoligamentous preparation of ankle specimens, Rasmussen et al 9 showed that the deep portions of the deltoid ligament rupture in external rotation, without involvement of the superficial portion. Finally, pronation of the talus is limited by both the superficial and deep components of the deltoid ligament, with secondary support provided by the talocalcaneal ligament.9,10 Pathological translation and rotation of the talus within the mortise can lead to altered ankle biomechanics and symptoms of instability. Medial ankle sprains have been shown to develop osteoarthritis on a rate even faster than lateral sided injuries and, thus, warrant careful evaluation. 11
Clinical Presentation
Diagnosis of a medial-sided ankle injury begins with obtaining and performing a thorough history and physical exam. An acute injury to the medial ankle ligaments following ankle trauma typically results in symptoms such as pain and swelling of the ankle with inability to bear weight. Isolated deltoid ligament injuries are uncommon but are typically the result of either a valgus stress or external rotation injury. They have also been associated with lateral ligament injuries and fibula fractures. In the setting of isolated lateral malleolar ankle fractures, approximately 40% of patients can have deltoid ligament disruption. 12 Chronic injuries present with history of an initial injury that is followed by anteromedial ankle pain, recurrent instability events, or feelings of “giving way.” In advanced cases, lateral sided pain can result from subfibular impingement secondary to hindfoot valgus.
On examination, skin around the medial and lateral sides of the ankle is inspected for swelling and ecchymosis. Inspection should be performed in both the standing and seated positions. Hindfoot alignment should also be inspected and any valgus tilting observed. Palpation of the medial, lateral, and syndesmotic ligamentous structures should be performed. Patients typically report tenderness over the deltoid ligament. In conjunction with hindfoot valgus tilt, pain can be elicited in the subfibular area and sinus tarsi. An external rotation drawer test should be performed and compared with the contralateral side. The affected ankle will demonstrate an increased amount of laxity with this maneuver.
An anatomically based classification for medial ankle instability has been proposed. 13 Type 1 lesions are described as a proximal avulsion of the tibionavicular or tibiospring ligaments; type 2 lesions demonstrate a midsubstance tear of these same structures; and type 3 lesions appear as a distal avulsion.
Standard 3-view weight-bearing radiographs of the ankle should be obtained. Some authors have advocated for the use of valgus stress radiographs of the ankle to identify medial instability, although wide variations and differences of up to 19° side to side in noninjured patients make this difficult to interpret. 4 Currently, the value of gravity stress views in diagnosing deltoid ligament injuries has not been established in the clinical setting. Magnetic resonance imaging (MRI) is a useful modality for identifying ligament injuries about the ankle, and its use in identifying injury to the lateral ligament and spring ligament complexes has been well established. 14 Figure 3 shows a coronal MRI image of chronic damage to the deltoid ligament. However, the usefulness of MRI in defining clinically relevant medial instability has not yet been investigated. In instances of suspected medial instability based on history and examination, arthroscopic evaluation can be performed to not only identify deltoid injuries, but also associated cartilage and lateral ligamentous disruptions requiring operative intervention. In one study, cartilage lesions were found in 98% of ankles with deltoid injuries. 4
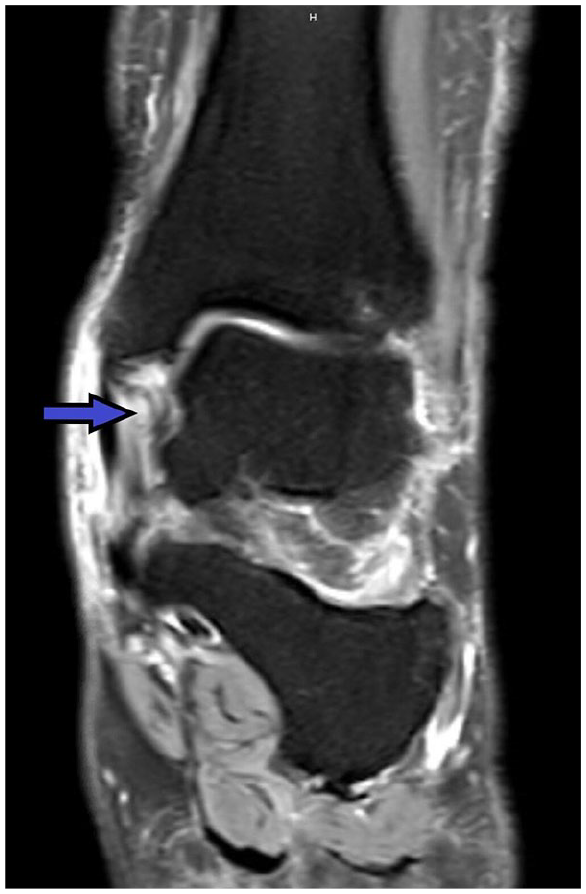
T2-weighted coronal magnetic resonance image demonstrates edema and hyperintensity of the deltoid ligament, indicating ligament chronic injury and attenuation. Photo courtesy of Talusan PG.
Nonoperative Management
Management of acute deltoid injuries should utilize a treatment algorithm similar to that of acute lateral ligament sprains. A standard course of nonoperative management begins with a period of rest and immobilization, typically in a cast or walking boot, for 1 to 3 weeks until pain and swelling subside. The patient may then be transitioned into a lace-up ankle stabilization brace and begin a course of physical therapy focusing on proprioceptive training as well as strengthening. Normal activities are then resumed at 8 to 12 weeks after injury. 3
Similar to lateral ligament injuries, surgical management is reserved for patients with continued symptom instability after a dedicated course of nonoperative management. Pijnenburg et al 15 reported a statistically significant improvement in clinical results with surgical repair of lateral ligament tears; however, these results were comparable in acute and delayed repairs. Given that surgery itself carries inherent risk, they recommended a trial of conservative therapy prior to pursuing surgical intervention. These authors recommend a period of 4 to 6 months of conservative management that includes physical therapy as well as insole orthotics with medial arch support to correct valgus hindfoot alignment.
Operative Management
Surgical management of deltoid ligament injury focuses on restoring medial ankle stability through ligament repair or reconstruction. Arthroscopic techniques to address deltoid ligament insufficiency have been described but are not currently utilized by the authors.
Primary Repair
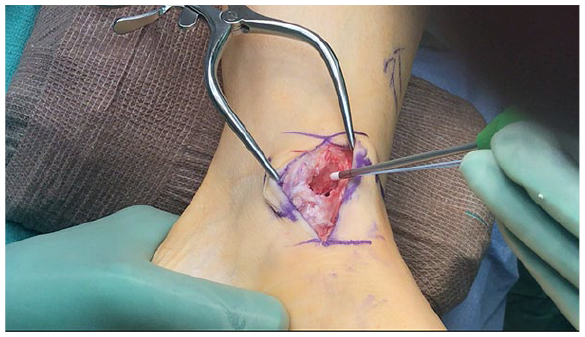
If the injured and/or attenuated deltoid is of sufficient quality to hold sutures, the superficial deltoid ligament can be repaired based on the location of the tear. A 4- to 8-cm gently curved incision is centered just posterior to the tip of the medial malleolus aiming at the medial aspect of the navicular bone. The subcutaneous tissue is divided in line with the incision, and the location of the tear is identified. If no tear is identified and the instability is the result of an attenuated ligament, the ligament complex is sharply removed from the tip and anterior portion of the medial malleolus. The bony origin on the distal and anterior portion of the medial malleolus is roughened to a bleeding surface with a burr, rongeur, or rasp. The authors’ preferred method is to place a suture anchor on the anterior and distal portions of the medial malleolus, as depicted in Figure 4. The sutures are passed through the ligament in a mattress fashion to imbricate the ligament.
For type 1 lesions, 1 or 2 suture anchors can be placed 6 mm above the tip of the malleolus and sutured using the surgeon’s preferred technique.
Reconstruction
If the deltoid tissue is not amenable to repair, several methods of reconstruction have been described.16-23 Two of the most commonly used techniques by the authors are described below. Deland et al 17 described a reconstruction using a peroneus longus transfer. The peroneus longus tendon is transected proximal to the cuboid tunnel, and the proximal portion is tenodesed to the peroneus brevis. A tunnel is drilled with a k-wire from the lateral aspect of the talar neck medially through the talar body. A second tunnel is drilled in the tibia from the tip of the medial malleolus at a 60° angle to the lateral cortex at the distal third of the tibial shaft. The tendon is secured in the tunnels using staples and nonabsorbable suture on the free ends and bone grafting interposition.
Haddad et al 19 described a technique in which a tunnel was placed from medial to lateral in the talar body using a drill and a second tunnel placed in the calcaneus, anterior to the sustentaculum, in a similar fashion. A split allograft was secured to the anterior tibia using a spiked washer and screw, and 1 arm each was passed into each tunnel and secured using a suture button.
The authors’ postoperative course consists of 4 weeks non–weight-bearing followed by 4 weeks of protected weight-bearing in a CAM boot. The first 2 weeks are spent in a short leg splint immediately postoperatively, which is changed to a CAM boot at 2 weeks postoperatively. Transition to an ASO brace occurs at 8 weeks postoperatively. Physical therapy for motion, proprioception, strengthening, and gait training begins around 8 weeks postoperatively. Patients are typically allowed to return to full activities at 6 months postoperatively if doing well.
Outcomes
Table 2 provides an overview of several studies that examined the outcomes of surgical management of medial ankle instability. The first study was presented by Hintermann et al 3 in 2004, with the same cohort of 52 patients being described in 2 subsequent articles by the same group.7,13 Their cohort underwent joint evaluation and repair of the deltoid ligament with suture anchors. They looked at American Orthopaedic Foot and Ankle Society (AOFAS) hindfoot scores and found an improvement in score from a mean of 42.9 preoperatively to 91.6 at a mean of 4.4 years postoperatively.
Outcomes of Surgical Therapy for Medial Ankle Instability.
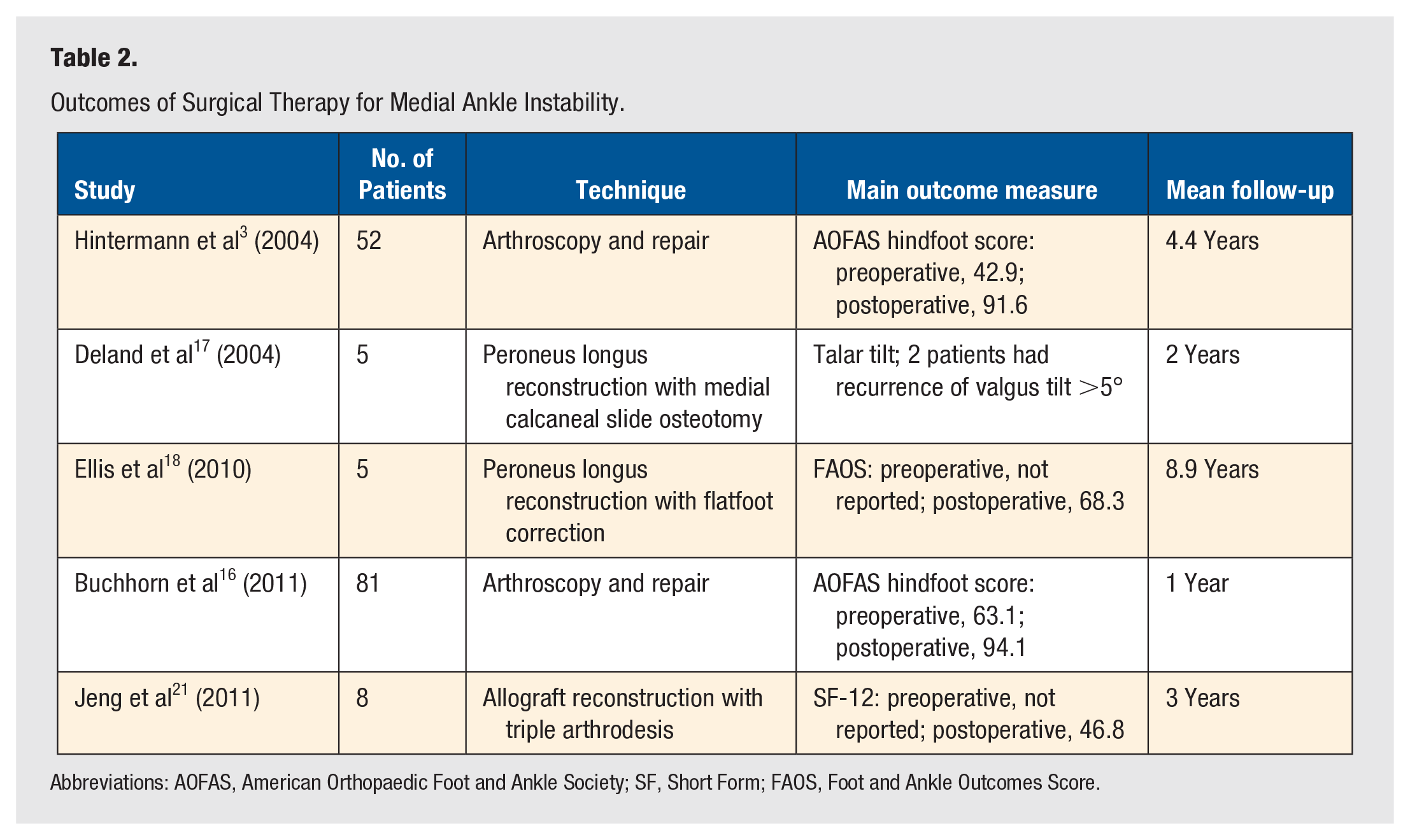
Abbreviations: AOFAS, American Orthopaedic Foot and Ankle Society; SF, Short Form; FAOS, Foot and Ankle Outcomes Score.
Buchhorn et al 16 in 2011 again looked at 81 patients who underwent arthroscopy and deltoid ligament repair using suture anchors. They also looked at AOFAS hindfoot score and found an improvement in score from a mean of 63.1 preoperatively to 94.1 at a mean of 12 months postoperatively. Deland et al, 17 Ellis et al, 18 and Jeng et al 21 all had small cohorts describing deltoid ligament reconstruction in the setting of flatfoot correction. Their outcomes measures and follow-up varied widely.
Conclusion
Deltoid ligament injury is relatively uncommon compared with lateral ligament injury, but its presence can significantly affect management strategies and patient outcomes. It is important to consider deltoid ligament injury in patients who present with instability and medial sided symptoms. When these injuries are neglected, instability resulting from the altered ankle mechanics can lead to associated pathology and early osteoarthritis. Standard and advanced imaging techniques in addition to ankle arthroscopy can be used to identify deltoid ligament injury as well as concomitant ankle pathology. A trial of nonoperative management should always be attempted before proceeding to surgical management. Intraoperatively, if native deltoid tissue is not amenable for primary repair, the surgeon can perform a reconstruction via reconstruction using allograft or autograft tendon. Robust outcomes data for operative management of these injuries are lacking, and this warrants further evaluation.
Footnotes
Acknowledgements
None
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.