
Abstract
Introduction
The promising data from Ankle Arthroplasty are consequence of the evolution of instruments and implants. Recent studies have shown good results in the short and intermediate follow-up, in addition to high patient satisfaction. The aim of this study is to present the results obtained with 49 cases treated with the Infinity total ankle prosthesis in 2 South America countries.
Methods
This is a case series of 48 patients (27 women and 22 men), treated with 49 Infinity prostheses in Brazil and Colombia. They underwent surgical treatment between April 1, 2016, and January 18, 2020. We used the visual-analogue pain scale (VAS), the AOFAS score for ankle and hindfoot and the measurement of range of motion (ROM) in the pre- and post-surgical period. The radiological evaluation was performed on ankle radiographs in anteroposterior and lateral views, obtained in orthostasis, measuring the parameters suggested by Hintermann. Average follow-up was 4 years.
Results
VAS reduced from an average of 7.94 to 1.98; AOFAS increased from 28.02 to 83.16 and ROM increased from 11.45 to 28.08. Distal Tibial Slope is higher for higher improvements in VAS and lower for higher improvements in AOFAS and ROM. We observed 4 wound infections, 1 intra-op medial malleolus fracture. No bone cysts, tibial or talar components subsidence, polyethylene component wear or failure were observed. No salvation procedures were required in this series.
Discussion
This study results corroborates literature data showing great improvements in pain, functional pattern, and movement.
Conclusion
Infinity Ankle Arthroplasty is a safe and reproducible procedure with good outcomes at a short-term follow-up.
Level of evidences:
4 - Case series
“Infinity Ankle Arthroplasty is a safe and reproducible procedure with good outcomes at a short-term follow-up.”
Introduction
The treatment of ankle osteoarthritis, a disease that affects about 6% of the population, 1 is a topic of great interest among foot and ankle surgeons. Much of this interest comes from the improvement of the total ankle arthroplasty (TAA) techniques over the last few years, allowing promising results. TAA was introduced in the 1970s, 2 but only in the last decade its use has increased considerably. 3
On the other hand, ankle arthrodesis, considered as the gold standard in the treatment of osteoarthritis of any etiology has been questioned, mainly due to the overload generated in neighboring joints with a consequent deterioration in patient’s functional quality of life. 4
The promising data from TAA are consequence of the evolution of instruments and implants. As a result, the use of restricted implants was replaced by less restricted implants and mobile platforms with 2 or 3 components, getting closer to the biomechanics and kinematics found in normal ankles, with survival rates of approximately 80% in 10 years. 5 - 7
Recent studies have shown good results in short and intermediate follow-up, in addition to high patient satisfaction. 8 However, the main concerns remains around longevity and revision rates. 9
The aim of this study is to present the results obtained in 49 cases treated with the Infinity total ankle prosthesis in 2 South America countries (Brazil and Colombia).
Methods
Between April 1, 2016, and January 18, 2020, 49 total ankle arthroplasties were performed in 48 patients, 27 women and 22 men (55% and 45% respectively). The surgeries took place in 4 different hospitals in Brazil and Colombia. The sample consisted of data collected from the 48 patients who underwent surgery. All patients were reassessed in February 2020 for clinical and radiographic data. The average follow-up was 4 years. This study was approved by our institution ethical committee and all patients signed an informed consent.
Patients’ ages varied between 29 and 78 years (mean 60.2 years). In all, 27 surgeries were performed on the right side and 22 on the left side. Most cases were diagnosed as post-traumatic arthrosis (35 cases, 71%). There were also 6 cases (12%) of primary arthrosis, 5 of rheumatoid arthritis (10%), 2 of hemophilic arthritis (4%), and 1 case of gouty arthritis (2%). On average, patients suffered from such conditions for 8.5 years (minimum 2 years and maximum 30 years).
In clinical evaluation, we used the visual-analogue pain scale (VAS), the AOFAS score for ankle and hindfoot 10 and the measurement of range of motion (ROM) in the pre- and post-surgical period. The radiological evaluation was performed on ankle radiographs in anteroposterior and lateral views, obtained in orthostasis, measuring the parameters suggested by Hintermann et al (Figure 1) 11 - 13 :
- Misalignment (a) Tibial component too short, too lateralized or medialized with angular deviation greater than 5 degrees and (b) Very small or very large talar component, placed at an angle greater than 10 degrees. In the ideal placement, the talar component should be located 5% in front of the tibial component.
- Alpha angle—Angle measured between the anatomical axis of the tibia and the articular surface of the tibial component of the prosthesis on the weight-bearing AP view (normal = 90 degrees).
- Beta angle—Angle measured between the anatomical axis of the tibia and the articular surface of the tibial component of the prosthesis, on the weight—bearing lateral view—(normal = 85 degrees).
- Theta angle—Angle obtained between the line passing through the anterior and posterior ends of the talar component of the prosthesis and the line that touches the upper edge of the navicular and the upper eminence of the posterior tuberosity of the calcaneus on the weight—bearing lateral view—normal = 20 degrees.
- Distance “a”—Distance in millimeters measured between the anterior end of the talar component of the prosthesis and the line that touches the upper border of the navicular and the upper eminence of the posterior tuberosity of the calcaneus on the weight-bearing lateral view.
- Distance “b”—Distance in millimeters measured between the posterior end of the talar component of the prosthesis and the line that touches the upper border of the navicular and the upper eminence of the posterior tuberosity of the calcaneus on the weight-bearing lateral view.
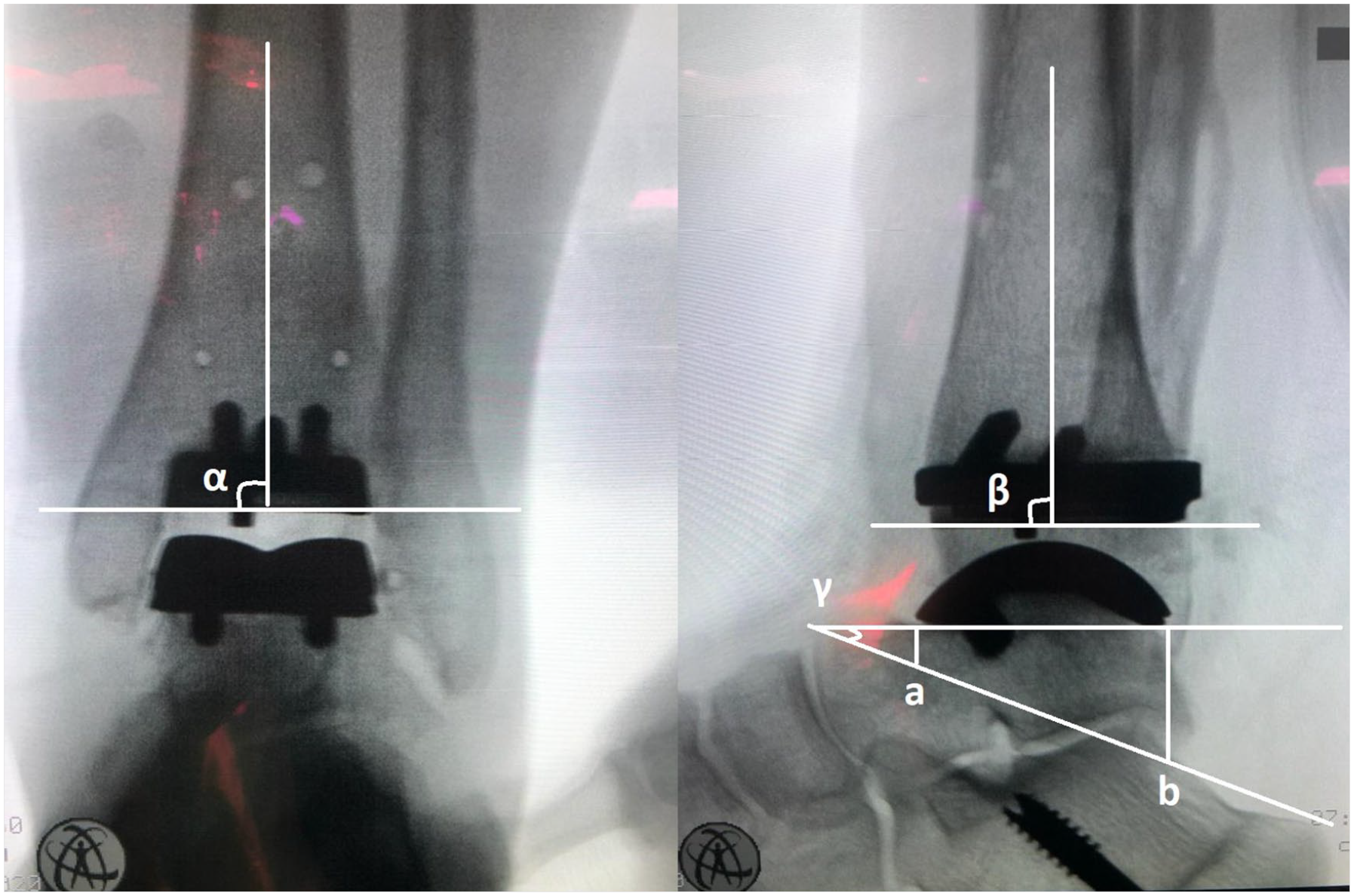
Left: Ap Post-op TAA image showing Alpha angle. Right: Lateral Post-op TAA image showing Beta and Theta angle, distance “a” and “b.”
Distal Tibial Slope were collected in the pre- and postoperative period. It is worthy to mention that post-operative tibia slope is the same as beta angle. Alpha, beta, theta angles and “a” and “b” distances were collected only in the postoperative period. Real mobility of the ankle, defined as the range of motion measured between the tibial and talar components on weight-bearing lateral radiographs in maximum flexion and extension were also measured.
We used the “three weeks” criterion to consider the integrity of the soft tissue envelope in the ankle region and to determine the occurrence of surgical wound complications. 14
Finally, outcome flaws were recorded: periprosthetic cysts, talar radiolucency, tibial radiolucency and wear. Radiolucency lines were defined as dark lines, of variable width, that appear around the prosthetic components.
For correlation between radiographic parameters and functional outcome, the Pearson’s correlation test was used for cases in which the normal distribution of variables was discarded (at a significance level of 5%) and the Spearman correlation test for the other cases. This test makes no assumptions about the distribution of variables. For the correlation between observational failures and radiographic parameters, Student’s t-test was used for variables with normal distribution and the Wilcoxon point sum test (also known as Mann-Whitney) for the others. The normality test used was Jarque-Bera and the software was R 3.6.3.
Results
Descriptive Statistics of the Sample Variables.
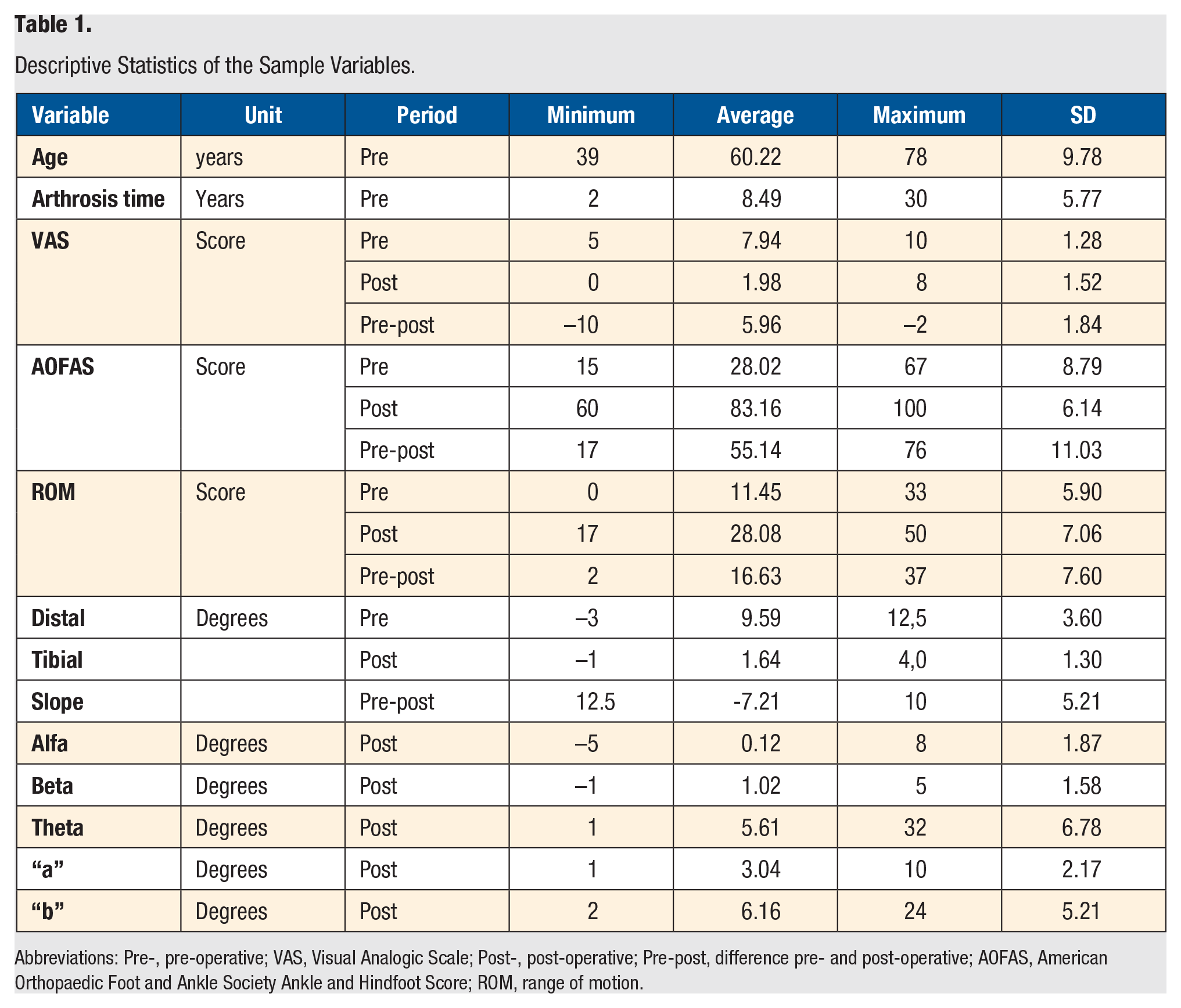
Abbreviations: Pre-, pre-operative; VAS, Visual Analogic Scale; Post-, post-operative; Pre-post, difference pre- and post-operative; AOFAS, American Orthopaedic Foot and Ankle Society Ankle and Hindfoot Score; ROM, range of motion.
Table 2 shows the functional outcomes pre- and post-operative comparison. VAS reduced from an average of 7.94 to 1.98; AOFAS increased from 28.02 to 83.16 and ROM increased from 11.45 to 28.08. All these results were statistically significant (p<0.001).
Functional Outcomes: Pre- and Post-Operative Comparison.
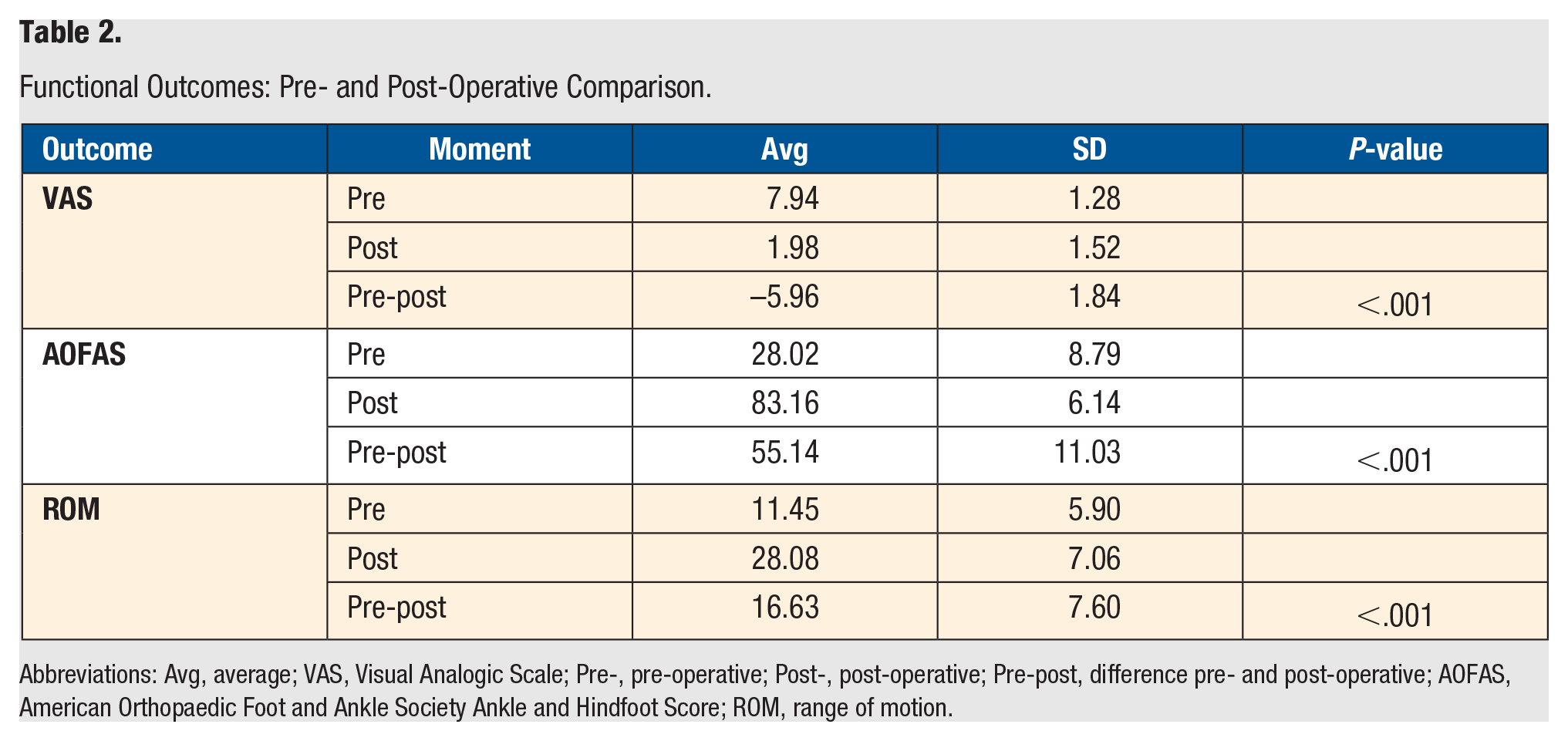
Abbreviations: Avg, average; VAS, Visual Analogic Scale; Pre-, pre-operative; Post-, post-operative; Pre-post, difference pre- and post-operative; AOFAS, American Orthopaedic Foot and Ankle Society Ankle and Hindfoot Score; ROM, range of motion.
Table 3 summarizes the results of the statistical tests for the radiographic parameters that were measured before and after surgery in relation to the functional outcomes. It was observed that clinical outcomes (VAS, AOFAS and ROM) were directly influenced by the distal tibial slope. Distal Tibial Slope is higher for higher improvements in VAS and lower for higher improvements in AOFAS and ROM.
Relationship Between Distal Tibial Slope and Clinical outcomes.
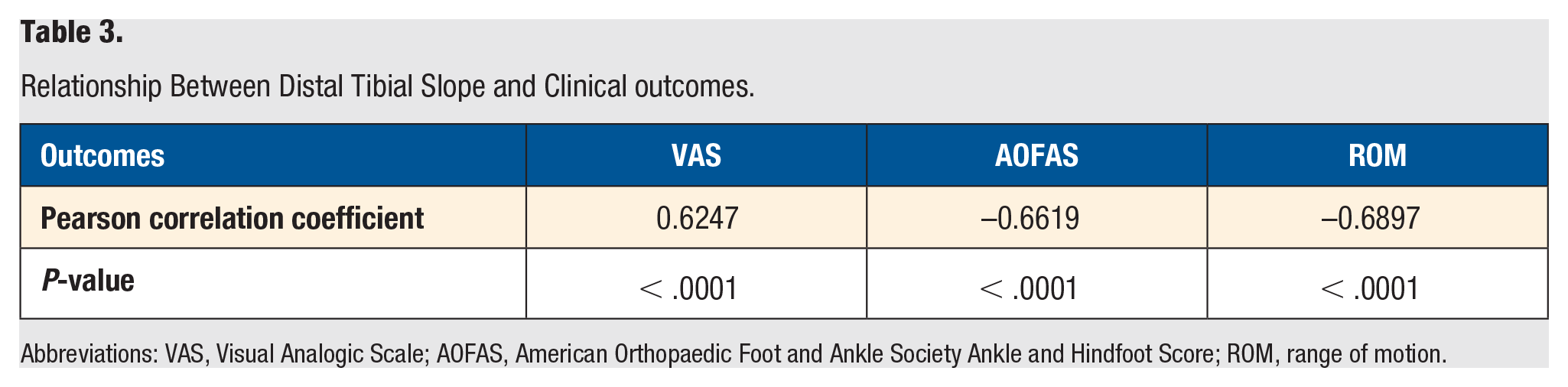
Abbreviations: VAS, Visual Analogic Scale; AOFAS, American Orthopaedic Foot and Ankle Society Ankle and Hindfoot Score; ROM, range of motion.
Table 4 describes the associations between functional outcomes (VAS, AOFAS and ROM pre/post-op difference) and post-operative angles (a, b, alpha, beta and theta). There is a correlation between beta angle and AOFAS: the higher the difference between pre and postop AOFAS the lower the beta angle is. No other association were found with a 5% significance level.
Relationship Between Functional Outcomes (VAS, AOFAS and ROM Pre-Post-Op Difference) and Radiographic Angles.
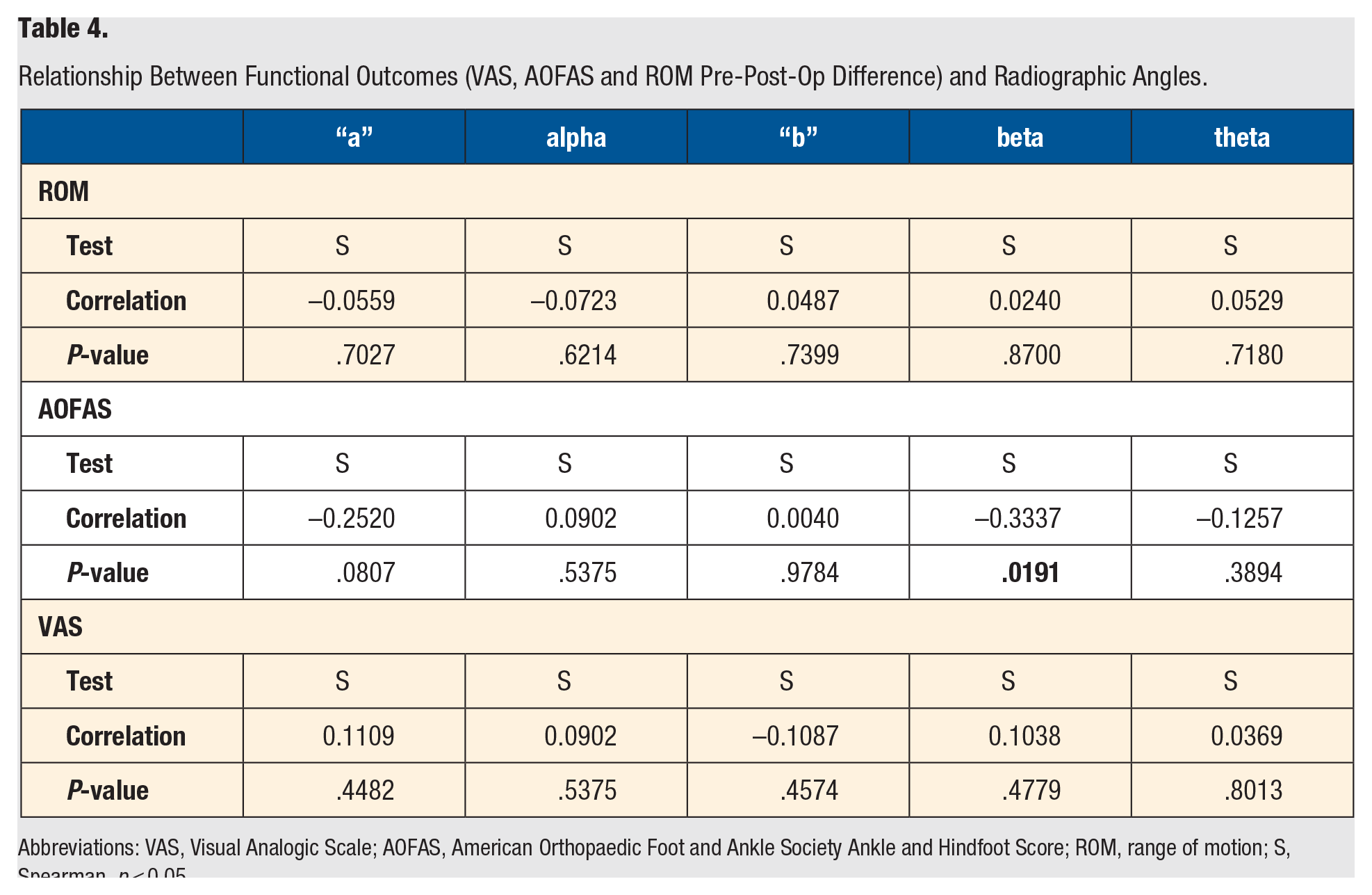
Abbreviations: VAS, Visual Analogic Scale; AOFAS, American Orthopaedic Foot and Ankle Society Ankle and Hindfoot Score; ROM, range of motion; S, Spearman. p < 0.05.
Only one patient suffered an intra-op medial malleolus fracture, which was treated at the same time with a compression screw. Regarding surgical wounds, 4 surgeries (8%) presented skin incision edges necrosis and 2 presented extensive soft tissue necrosis around the surgical incision. One of them required free skin-grafting and the other required a vascularized flap. In all other 44 surgeries, no complications of any type were observed. No bone cysts, tibial or talar components subsidence, polyethylene component wear or failure were observed. No salvation procedures were required in this series.
Discussion
Unlike other lower limb arthrosis, osteoarthrosis (OA) of the ankle has joint trauma as its main etiological factor, especially malleolar fractures, chronic ankle instability and distal tibial fractures. 12 In our sample, it is observed that 35 cases (71%) were diagnosed as post-traumatic OA, ratifying the rate already established in iterature. 13
To facilitate therapeutic decision-making, Hintermann et al, proposed a staged treatment algorithm, according to factors to be evaluated in each patient. According to this algorithm, TAA is indicated for patients with severe OA, severe daily pain, high functional limitation, of any etiology, with good bone quality, with adequate alignment of the lower limbs or slight asymmetry, stable articulation, elderly age range and absence of serious systemic comorbidities. Also, according to this algorithm, arthrodesis is reserved for patients with severe OA, severe daily pain, high functional limitation, of any etiology, with good bone quality, with adequate alignment of the lower limbs or slight asymmetry, stable articulation, elderly and young adults age range and absence of serious systemic comorbidities. 12 The aspect that would influence the most the choice of TAA in relation to arthrodesis would be the possibility of restoring the functional range of motion, taking into consideration the elimination of pain and the improvement in quality of life that could be achieved in both procedures.12,15,16
It is important to emphasize that the precise selection of patients is essential for the success of this procedure. And contraindications include osteonecrosis, severe peripheral vascular disease, peripheral neuropathy, recent or previous joint infection, severe ligament instability, major misalignment of the lower limb and poor bone quality. 17
The subjective and objective assessment of patients to TAA shows, in general, satisfactory results, good improvement of functional scores, ROM and real mobility. 8 In this study VAS reduced from an average of 7.94 to 1.98; AOFAS increased from 28.02 to 83.16 and ROM increased from 11.45 to 28.08. This corroborates literature data showing great improvements in pain, functional pattern and movement. 16
When evaluating radiographic parameters, Nery C et al 8 did not detect significant differences between alpha, beta and theta angles and distances “a” and “b,” which had small variations, located within the acceptable limits. In this study, we found a correlation between beta angle and AOFAS: the higher the difference between pre and postop AOFAS the lower the beta angle is. This could lead us to infer that lower beta angle could allow more ankle mobility in dorsiflexion with possible better function and ankle movement. No other association were found with a 5% significance level.
It was also found in this study a correlation between post-operative Distal Tibial Slope (beta angle) and the clinical outcomes VAS, AOFAS Ankle and Hindfoot Score and ROM. Distal Tibial Slope is higher for higher improvements in VAS and lower for higher improvements in AOFAS scores and ROM. This is the first time, at our best effort, that this correlation is found in literature. This may occur because patients with lower ROM (higher tibial slope) tend to present less pain and patients with higher ROM (lower tibial slope) tend to present better function.
Despite the promising results, TAA still has high complication rates compared to knee and hip arthroplasties. 18 Intraoperative complications are due to difficulties in aligning the components, bone cuts and fractures of the malleoli. Postoperative complications are related to dehiscence of the surgical incision and infection.3,8,19,20 In the long term, the biggest complication is aseptic loosening of the tibial or talar components, followed by stress fractures and capsular retraction.21,22 Corroborating with the current literature, we observed in our sample the occurrence of one medial malleolus fracture intraoperatively. 23 We also observed 4 (8%) superficial wound problems, and 2 deep wound problems, requiring further surgery for treatment. In the other 44 surgeries, no complications and/or misalignment were observed.
The literature is abundant when reporting outcome flaws, such as cysts, tibial or talar radiolucency (subsidence), wear or failure on the prostheses,3,29. However, none of the patients in our sample had these failures nor a salvage procedure so far. This may be explained for our short follow-up.
This study has several limitations such as its small sample size, short-term results and retrospective study design. Therefore, long-term follow-up studies, with larger samples are necessary to further correlate traditional radiographic parameters and functional outcomes in patients undergoing TAA.
Conclusion
Infinity Ankle Arthroplasty is a safe and reproducible procedure with good outcomes at a short-term follow-up.
Footnotes
Author Contributions
All authors made substantial contributions to all of the following: the conception and design of the study, acquisition of data, analysis and interpretation of data; drafting the article and revising it critically for important intellectual content. All authors have approved the final article should be true and included in the disclosure.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Daniel Baumfeld, Caio Nery and Santiago Guerrero are Consultant/Speaker for Arthrex, Inc (USA). Caio Nery and Santiago Guerreiro are Consultant/Speaker for Wright Medical Tiago Baumfeld is Speaker for Medartis Ricardo Fernandes has no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.