
Abstract
Introduction
Sleep Apnea (SA) is a common sleep disorder that increases postoperative morbidity. There is limited research on how SA influences outcomes following operative fixation of ankle fractures. Therefore, the aim of this study was to determine whether patients who undergo surgical fixation for bimalleolar ankle fractures have higher rates of medical complications and health care expenditures.
Methods
A retrospective review from January 1, 2005 to March 31, 2014 was conducted using the parts A and B Medicare Data from PearlDiver database. Patients with and without SA on the day of the primary open reduction and internal fixation (ORIF) of their bimalleolar ankle fractures were queried using the International Classification of Diseases, Ninth Revision codes. Welch’st-tests were used to compare costs of care. A multivariate binomial logistic regression model was used to calculate the odds ratio (OR) of adverse events. A P-value <.001 was considered statistically significant.
Results
There were 20 560 patients (SA = 3150; comparison cohort = 17 410) who underwent ORIF for bimalleolar ankle fractures during the study period. Sleep apnea patients were found to have significantly higher rates and odds of 90-day medical complications (21.42% vs 7.47%, OR: 3.11, P < .0001) and 90-day costs of care ($7213.12 vs $5415.79, P < .0001).
Conclusion
This research demonstrates an increased risk of postoperative medical complications and health care costs among patients with SA undergoing ORIF for bimalleolar ankle fractures.
Level of Evidence
Therapeutic, Level IV: Retrospective
Keywords
Whether perioperative management of patients with sleep apnea who were undergoing open reduction and internal fixation for bimalleolar ankle fractures decreases the risk of morbid complications and reduces the health care expenditures.”
Introduction
Ankle fractures are among the most prevalent traumatic orthopaedic injuries encountered in the emergency department in the United States and are among the most common fractures requiring surgery.1-3 The incidence of ankle fractures is estimated to be 187 per 100 000 people—a 163% increase over the past 30 years with no evidence of future decline. 4 Research has shown that the routine management of patients sustaining operative ankle fractures results in approximately more than $367 million of annual excess economic burden in the United States and negatively impacts patients’ lives in debilitating ways. 5 Bimalleolar ankle fractures account for 60% of all ankle fractures and a subset of these patients sustaining these injuries are often admitted directly from the emergency room for surgical management, while most can generally be reduced and discharged. 6 The most prevalent treatment method for bimalleolar ankle fractures is open reduction and internal fixation (ORIF) which has been shown to be more efficacious than nonoperative treatment, but is associated with a high incidence of perioperative and postoperative complications. 5
The number of patients undergoing ORIF procedures for bimalleolar ankle fractures has been steadily increasing, paralleling the observed increase in the prevalence of these injuries. 6 In turn, it is important to understand the risks of complications that arise from treating these injuries which are costly and can adversely affect patient outcomes. Sleep apnea (SA) is one of the most common sleep-related breathing disorders, characterized by intermittent episodes of partial or complete upper airway obstruction during sleep and is associated with various health-related consequences.7-9 It is estimated that at least 25 million adults in the United States are affected by SA.7-9 The prevalence of SA is expected to increase substantially, secondary to the increasing incidence of obesity—a risk factor for developing SA. 10 Research has shown that SA is associated with poor bone mineralization, immune dysregulation, osteoarthritis, and an increased risk of postoperative complications.11-13 Prior research has shown that SA increases health care costs and the risk of 90-day complications following orthopaedic surgery.14-16 However, the association of SA in patients undergoing ORIF for bimalleolar ankle fractures has not been thoroughly elucidated. 16 With the rising prevalence of SA and expected increase of bimalleolar ankle fractures, large sample size studies investigating the association of this condition in patients who undergo ORIF for these injuries are warranted.7-9,17
Therefore, the aim of this study was to analyze a large nationwide administrative claims database to determine the association of SA on outcomes following ORIF for bimalleolar ankle fractures within the Medicare beneficiaries. Specifically, this study analyzed whether SA patients undergoing surgical fixation for bimalleolar ankle fractures have higher rates of medical complications and health care expenditures. Based on prior research, we hypothesize that SA is associated with worse outcomes and higher health care–related costs for treating these injuries.
Materials and Methods
A retrospective level III case-control query from January 1, 2005 to March 31, 2014 was performed using the 100% parts A and B Medicare claims database from PearlDiver (www.pearldiverinc.com, PearlDiver Technologies, Fort Wayne, Indiana). These years were chosen as they are the standard years provided within the Medicare claims of the PearlDiver database.
While the Medicare claims database consists of parts A to D, these parts of the Medicare claims were analyzed as parts A and B represent coverage for inpatient/hospital and outpatient/medical coverage, respectively. The subscription-based platform allows primary investigators to identify patients’ populations of interest either through parts A and B of the Medicare claims or by using a private payor system known as Mariner. In total, both data sets hold more than 100 million patients and have been used extensively for orthopaedic-related research.14,18-21 Information from the database is aggregated and analyzed through the use of a syntax-based language by using International Classification of Disease, Ninth Revision (ICD-9), ICD-10, Current Procedural Terminology (CPT), National Drug Codes, and Diagnostic-Related Group codes. 22 Research variables available to primary investigators include complications, discharge dispositions, health care costs, and other metrics of interest. Information is subsequently downloaded as a Microsoft Excel (Microsoft Corporation, Redmond, Washington) spreadsheet for further data analysis. As the downloaded information is devoid of patient identifiers, the study was exempt from the approval and review process by our institution’s Institutional Review Board.
The database was initially queried for those patients who had either an open or a closed bimalleolar ankle fracture using ICD-9 diagnostic codes 824.4 (bimalleolar fracture, open) and 825.5 (bimalleolar fracture, closed). Patients who underwent ORIF for these injuries were identified using CPT code 27814 (open treatment of bimalleolar ankle fractures, includes internal fixation when performed). 23 Patients who have SA were identified using ICD-9 diagnostic codes 327.20 to 327.29, in addition to 780.57. These codes were used as they have been used previously in prior published investigations.15,16,24,25 To ensure patients were not counted twice in the database, the “FIRST_COMMAND” syntax was utilized to ensure only patients who had these diagnoses and procedures the first time were included within the investigation. The study cohort consisted of those patients who underwent ORIF for bimalleolar ankle fractures with SA, while those patients without SA served as the comparison cohort in the investigation. In addition, as patients may enter and leave the Medicare claims, the “ACTIVE” syntax command was utilized to only identify patients who had an active enrollment 90 days prior to 180 days after the procedure. This would ensure that our study cohort was homogenous and does not introduce any potential bias within the investigation. No exclusion criteria were used.
In this retrospective analysis, 90 day medical complications, day of surgery expenditures, and global 90 day health care expenditures were compared among patients with and without SA who underwent ORIF for bimalleolar ankle fractures. Baseline demographics of the 2 cohorts compared included age, sex, and prevalence of comorbid conditions such as alcohol use disorder, arrhythmias, body mass index (BMI), congestive heart failure, coagulopathy, depressive disorders, diabetes mellitus, hypertension, hypothyroidism, iron deficiency anemia, liver failure, peptic ulcer disease, peripheral vascular disease, renal failure, rheumatoid arthritis, valvular disorders, and pathologic weight loss. These comorbid conditions were chosen as they comprise aspects of the 2 most commonly utilized comorbid indices in orthopaedic research—the Charlson comorbidity index and Elixhauser comorbidity index (ECI).26-29 In addition to comparing individual prevalence of the comorbid conditions, a mean ECI score was computed for the 2 cohorts. Ninety-day medical complications assessed included acute kidney injuries, cerebrovascular accidents, deep vein thromboses, myocardial infarctions, episodes of ileus, pneumoniae, pulmonary emboli, respiratory failure, and venous thromboemboli. Day of surgery and 90-day health care costs were compared between the 2 cohorts using reimbursement data as it is a more accurate predictor of what providers are paid through the insurance companies.30-32 Economic information is aggregated in the database starting from the time of the initial procedure and continuing up to a time interval chosen by the principal investigators. For this study, 90 days were chosen for medical complications and reimbursement analyses as it corresponds to the global fee period for set in place by the Centers for Medicare and Medicaid Services, as done in previously published investigations using the same database.30-32 Health care costs from the database are aggregated by using a time interval at the discretion of the investigators and all additional costs which patients may have incurred during the time interval are tabulated. These costs may include additional physician visits, diagnostic tests, medication refills, and other health care–related expenses.30,33
Data Analyses
Statistical analyses were performed using the open programming language known as R (R, Foundation for Computational Statistic, Vienna). Baseline demographics of the 2 cohorts were compared using Pearson chi-square analyses or Fisher exact test, when applicable for the latter. PearlDiver provides age as a categorical variable starting with patients less than or equal to the age of 64 years and older than the age of 65 years with 5-year age increments. For the continuous variables in the study, Welch’s t tests were used to compare mean ECI scores and health care costs for the day of surgery and global period. To determine the association of SA on medical complications, a multivariate binomial logistic regression model was constructed to calculate the odds ratio (OR) and 95% confidence interval (95% CI) for each of the different complications. The regression model was adjusted for age, sex, geographic region, and the following comorbid conditions which have been shown to be prevalent within patients who have SA: alcohol use disorder, chronic obstructive pulmonary disease, general anxiety disorder, diabetes mellitus, hyperlipidemia, hypertension, obesity—defined as a BMI >30 kg/m2, and tobacco use.34-38 This method of data analysis was chosen as it has been done in previously published investigations utilizing the same database.39-41 To minimize the probability of a type I error and due to the ease of finding statistical differences with large administrative data sets, a Bonferroni correction was performed and a P value <.001 was considered to be statistically significant. 42
Results
Patient Demographics
The final query yielded 20 560 patients who underwent ORIF for bimalleolar ankle fractures who did have SA (n = 3150) and did not have SA (n = 17 410; Figure 1). Study group patients were generally younger than the age of 64 years (38.83%) and represented the largest cohort with respect to age followed by those patients between the ages of 65 and 69 years (30.13%), whereas patients younger than the age of 85 years represented the smallest cohort (1.78%; Table 1). Female patients were more likely to have the SA condition compared with their male counterparts (61.65% vs 38.35%; Table 1). When analyzing prevalence of comorbid conditions, SA patients had higher rates of arrhythmias (47.65% vs 31.30%, P < .0001), obesity (18.29% vs 5.31%, P < .0001), morbid obesity—defined as a BMI >40 kg/m2 (3.40% vs 2.25%, P < .0001), congestive heart failure (42.57% vs 21.79%, P < .0001), depressive disorders (57.52% vs 33.47%, P < .0001), and other comorbid conditions (Table 1). This greater prevalence of comorbid conditions found within the study cohort is further exemplified by SA patients having significantly higher mean ECI scores compared with their counterparts (8 vs 4, P < .0001; Table 1).
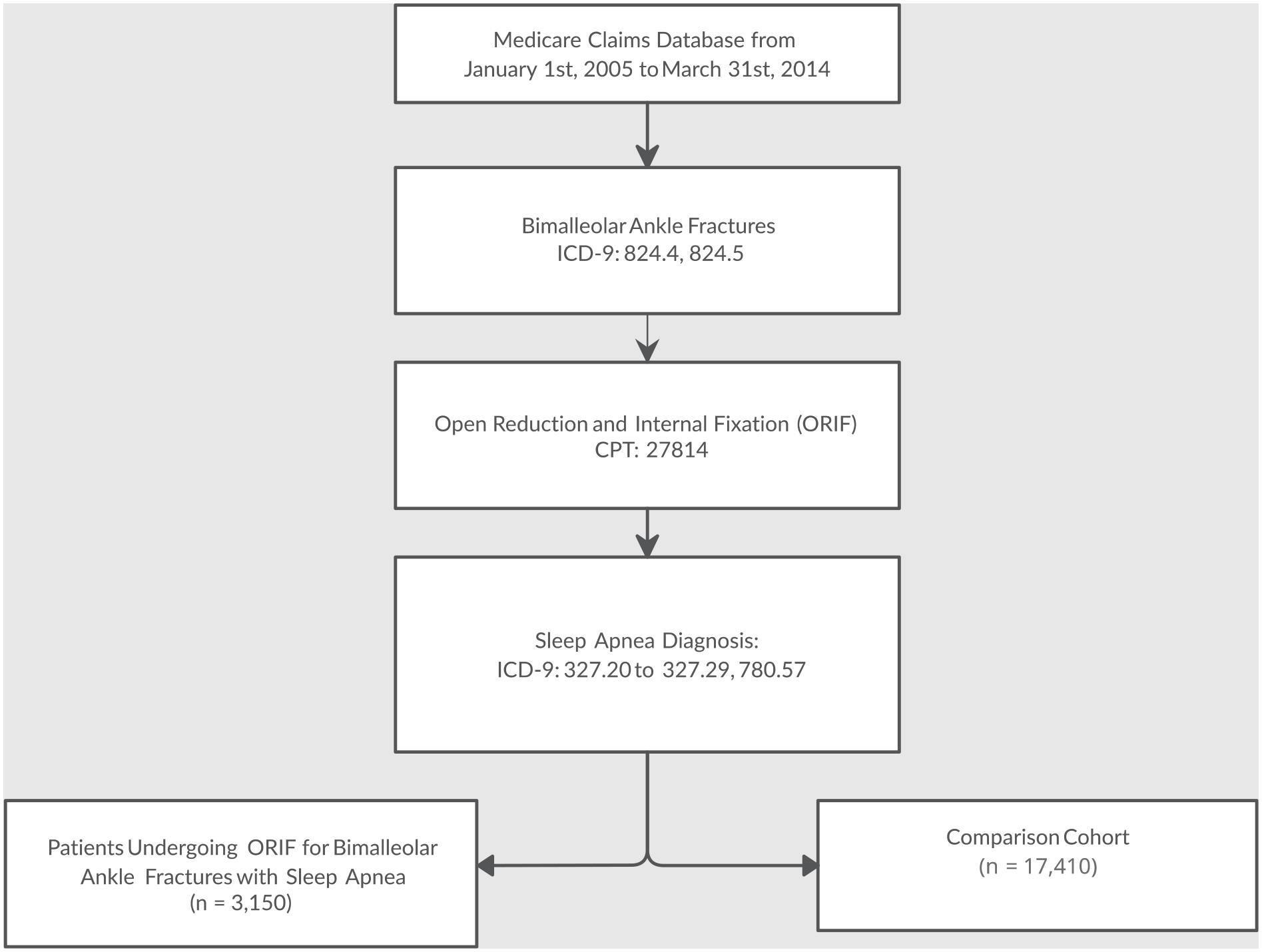
STROBE diagram demonstrating final cohorts within the investigation.
Comparison of Baseline Demographics of Patients With SA (n = 3150) and Without SA (n = 17 410) Undergoing Open Reduction and Internal Fixation of Bimalleolar Ankle Fractures.
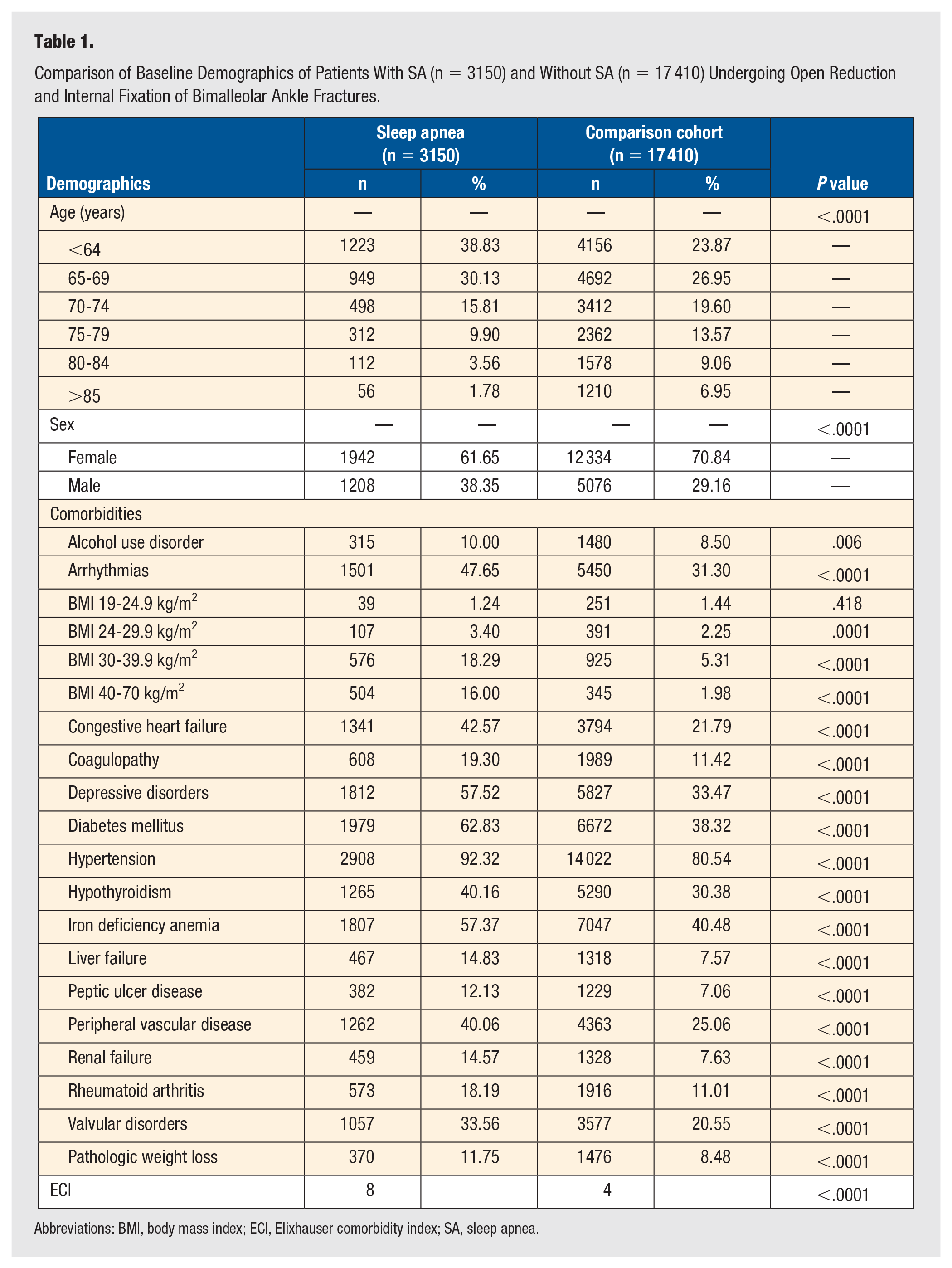
Abbreviations: BMI, body mass index; ECI, Elixhauser comorbidity index; SA, sleep apnea.
Medical Complications and Health Care Expenditures
Study group patients were found to have significantly higher frequency and odds (21.42% vs 7.47%, OR: 3.11, 95% CI: 2.78-3.48, P < .0001) of developing adverse events within 90 days following the index procedure. Specifically, SA patients had higher odds of developing pneumoniae (6.70% vs 1.77%; OR: 3.27, 95% CI: 2.66-4.01, P < .0001), cerebrovascular accidents (1.33% vs 0.45%; OR: 2.78, 95% CI: 1.83-4.18, P < .0001), pulmonary emboli (1.02% vs 0.39%; OR: 2.75, 95% CI: 1.71-4.35, P < .0001), acute kidney injuries (6.25% vs 1.82%; OR: 2.67, 95% CI: 2.17-3.27, P < .0001), respiratory failures (0.60% vs 0.20%; OR: 2.13, 95% CI: 1.12-3.91, P = .0001), and other complications compared with their counterparts (Table 2).
Multivariate Binomial Logistic Regression Comparing Rates of 90-Day Medical Complications Among Sleep Apnea Patients and the Comparison Cohort Undergoing Open Reduction and Internal Fixation for Bimalleolar Ankle Fractures.
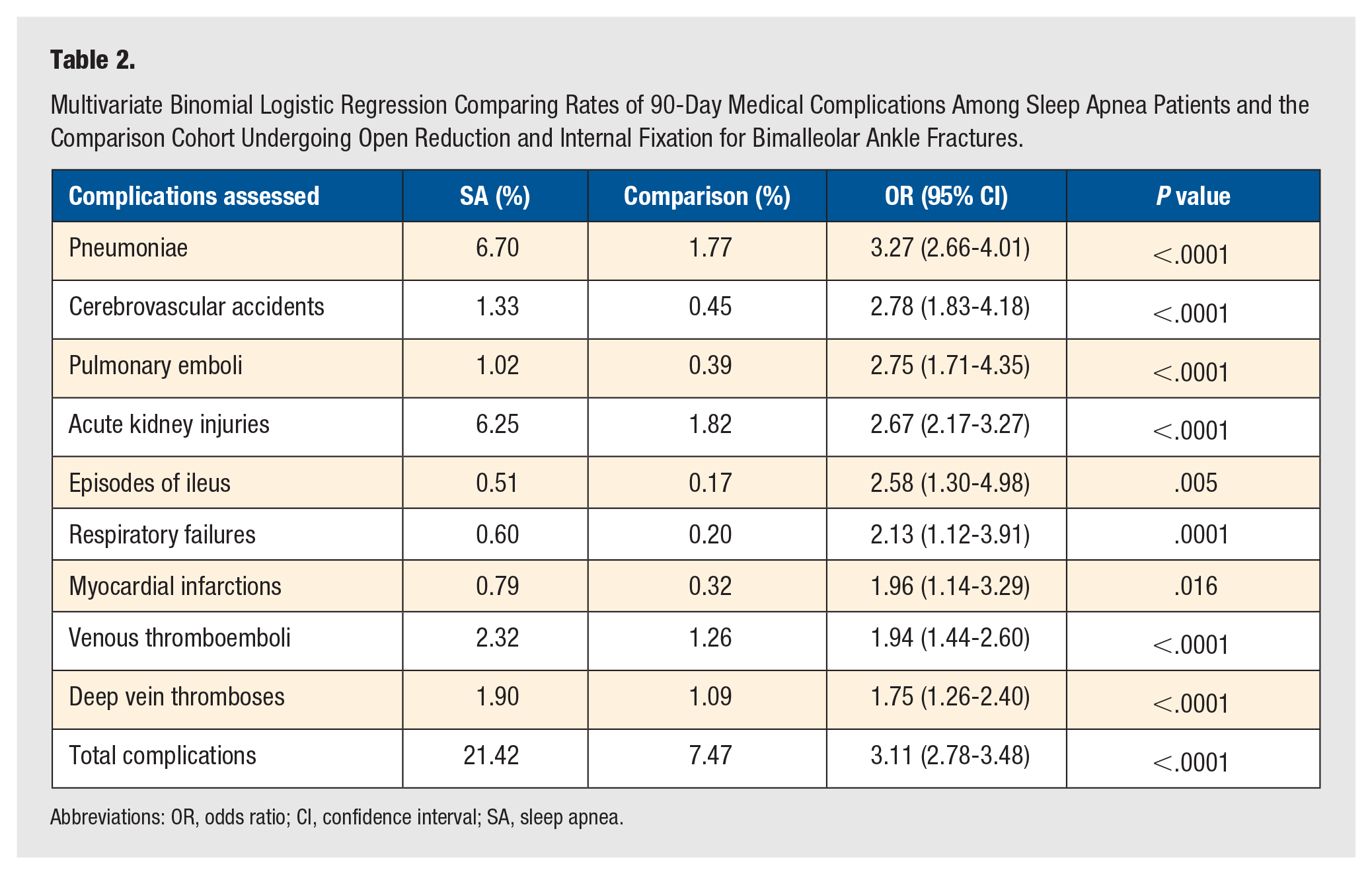
Abbreviations: OR, odds ratio; CI, confidence interval; SA, sleep apnea.
When comparing health care expenditures between the 2 cohorts, SA patients were found to have significantly higher day of surgery ($3642.51 vs $3287.96, P = .026) in addition to total global 90-day episode of care costs ($7213.12 vs $5415.79, P < .0001) compared with their counterparts following ORIF for bimalleolar ankle fractures.
Discussion
The prevalence, morbidity, and economic burden of SA have been steadily increasing and are projected to continue to this trend in the coming years. 7 Concomitant with this trend is the rise of ORIF for patients who sustained a bimalleolar ankle fracture. 5 While ORIF has shown to be an effective means for treating these fractures, it does not come without complications. 17 As such, it is of great importance to identify modifiable risk factors that may reduce complications to improve patient outcomes and reduce health care expenditures. This research shows that SA is a significant risk factor for postoperative medical complications following ORIF for bimalleolar ankle fractures. Patients with SA undergoing operative treatment of these injuries had higher rates of complications and health care expenditures within 90 days following the index procedure.
This retrospective analysis demonstrated that SA leads to higher rates of adverse events within 90 days following the index procedure, including pulmonary- and vascular-related complications. Specifically, SA patients were found to have significantly higher odds of developing pneumoniae (OR: 3.27, P < .0001), cerebrovascular accidents (OR: 2.78, P < .0001), and pulmonary emboli (OR: 2.75, P < .0001). In a retrospective case-control study, Gupta et al 43 demonstrated that patients with SA undergoing total joint arthroplasty had a significantly higher overall incidence of postoperative complications including respiratory instability and cardiac compromise secondary to postoperative episodic hypoxemia compared with their matched cohorts. D’Apuzzo and Browne 44 analyzed the Nationwide Inpatient Sample database of 258 445 patients who underwent revision total hip and knee arthroplasty between 2006 and 2008 and found that SA is associated with more episodes of hypoxia, higher rates of pulmonary emboli, and increased inhospital mortality. Golub et al 14 found their SA cohort had significantly higher frequency and odds of developing complications (72.66% vs 43.85%; OR: 1.57, P < .0001) after adjusting for baseline covariates within their investigation. The higher risk of pneumoniae among patients with SA may be attributed to increased risk for aspiration and impaired immunity. In SA, episodic airway collapse and impaired upper airway sensation and swallowing reflex may facilitate aspiration of pathogen containing pharyngeal contents into the lower respiratory tract. 45 Sleep fragmentation and hypercapnia observed among patients with SA have also been shown to impair innate immunity and may also contribute to this increased susceptibility to pneumoniae. 46 With respect to vascular-related complications, studies have shown SA to meet the requirements of Virchow’s triad, making patients susceptible to developing thrombotic-related complications.47,48
The higher rates of complications observed could explain the higher incremental costs found in the study group patients. For instance, this study demonstrated patients who had SA were found to have significantly higher frequency and odds of developing thromboembolic complications compared with their comparison cohort. Studies have shown that the treatment of adverse events like pulmonary emboli and deep vein thromboses may an incur an additional $17114 and $9345, respectively.49,50
Postsurgical complications pose a significant risk of harm to patients either directly through the occurrence of the complication itself or indirectly through increased length of stay in the hospital environment. Therefore, to improve outcomes and reduce costs, it is necessary to recognize factors, like the presence of SA, that may be associated with an increased risk of adverse outcomes. Managing these factors begins with identifying the patient with SA, either through nocturnal polysomnography which is the gold standard but can be difficult to implement in a patient following traumatic injuries or through validated questionnaires such as the Snoring, Tired, Observed, Pressure-Body mass over 35 kg/m2, Age above 50 years, Neck circumference, and Gender survey, American Society of Anesthesiologists checklist, and the Berlin questionnaire. The latest guidelines and practice statements by the Society of Anesthesiologists, the American Academy of Sleep Medicine, and the Society of Anesthesia and Sleep Medicine recommend routine screening for SA using the aforementioned screening questionnaires during preoperative assessment.51-54 These guidelines suggest that patients with SA may require additional vigilance during the perioperative management of their airway and recommend the judicious use of anesthetic agents and opioid medications.52,54 In addition, encouraging the use of continuous positive airway pressure (CPAP) during the postoperative period is also recommended. 52 Research has shown that the use of CPAP significantly reduced the rate of postoperative complications and also decreased the hospital length of stay among patients undergoing hip or knee replacements. 55 Other studies that investigated the efficacy of CPAP utilization also support its use in reducing postoperative medical complications and hospital length of stay among patients with SA.56-58
The current investigation is not without limitations. Large-volume databases such as the PearlDiver database used in this research provide robust information about patients enrolled within a private insurance or the Medicare claims. 59 However, it is not without errors as electronic miscoding is an inherent limitation of using a national patient database. In addition, this research only studied Medicare data which may not represent a true cross-sectional depiction of SA patients within the United States. Patients with SA commonly have other comorbidities which along with complications and adverse events may be underreported and not have been analyzed within this investigation. 60 A confounding variable which was not able to be controlled for was whether study group patients were utilizing CPAP treatment for their SA, which could potentially have impacted the results of this investigation. In addition, the investigation was unable to determine whether patients received general anesthesia or regional anesthesia, which could have potentially confounded the results of the investigation; however, this can serve as the basis for future prospective studies. Furthermore, the diagnosis of SA is made through a formal analysis via a sleep study. It is possible that patients in the comparison cohort may not have received a diagnosis of SA which could potentially underestimate the results of the investigation. In addition, it is possible that patients who sustained a bimalleolar ankle fracture may have sustained other traumatic injuries which could have confounded the results of this study. Furthermore, the lack of other studies analyzing the association of SA on outcomes following ankle fractures makes it difficult to determine whether the results of our studies coincide with other investigators. While PearlDiver is generally utilized to query for inpatient procedures, many bimalleolar ankle fractures are treated in the outpatient setting, which potentially introduces observer bias within the study. Similarly, additional granular variables such as the Injury Surveillance Score (ISS) were not available for patients to determine whether polytrauma patients or higher ISS scores had any correlation with the dependent variables measured within this study, but can certainly serve as the basis for future prospective studies. Despite these limitations, the study provides adequate information for orthopaedic surgeons and other health care professionals to adequately educate patients who are undergoing surgical fixation for their bimalleolar ankle fracture.
Conclusion
This study demonstrates that operative fixation of bimalleolar ankle fractures in patients with SA is associated with a higher risk of medical complications and higher health care expenditures. The risk of serious postoperative complications is nearly 3 times greater in patients who have SA than those who do not. Based on the results of this study, it is important to identify SA among patients undergoing ORIF of their ankle fractures to reduce the high risk of morbidity associated with this patient population. Orthopaedic surgeons can help mitigate these risks by optimizing the intraoperative use of anesthetic and narcotic agents which may exacerbate apneic episodes. In addition, orthopaedists should counsel and encourage the use of CPAP throughout the postoperative period and consider minimizing the use of analgesics that depress the respiratory system. The appropriate perioperative management of patients with SA may therefore decrease the risk of morbid complications and reduce health care expenditures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.