
Abstract
Background
With emerging evidence supporting functional rehabilitation for Achilles tendon ruptures (ATRs), this study sought to evaluate the treatment trends for patients sustaining an acute ATR and whether gender and age may influence the rates of operative repair.
Methods
A retrospective database review identified ATRs from 2010 through 2019. Patients were then stratified into three cohorts based on age (18-30, 30-45, and 46 and older), separated by gender, and then assessed whether patients were treated operatively or not. Cochran-Armitage Trend test was performed to analyze the trends of operative management. Chi-square analyses were performed to assess whether the proportion of patients who received operative management in each age cohort differed from 2010 to 2019. Logistic regression analyses were performed to assess whether gender influenced treatment.
Results
Over the previous decade, the total rates of operative treatment for ATR significantly decreased (18.3%-12.3%, P < .0001). Each individual age cohort experienced a proportional decrease in operative management when comparing 2010 with 2019 (all P < .0001). Within all age cohorts, males were significantly more likely to receive operative treatment for an ATR over the previous decade (odds ratios: 2.63-3.22). Conclusion. Overall rates of operative management for ATR decreased across all cohorts likely due to previous studies providing evidence of similar results between operative and nonoperative managements. Over the previous decade, males were demonstrated to be far more likely than females to undergo operative management. Why females are less likely to receive an operation for ATR is likely multi-factorial and requires further exploration.
Level of Evidence:
Level III: Retrospective comparative study
. . . this article set out to characterize the trends of treatment in ATR patients and identify whether age or gender may influence rates of operative repair.”
Introduction
Acute rupture of the Achilles tendon is one of the most common tendon injuries in the adult population and one of the most commonly treated injuries by orthopaedic surgeons with increasing incidence over the last few decades. 1 The overall incidence of an Achilles tendon rupture (ATR) increased from 2.1 per 100 000 person years in 1979 to 21.5 per 100 000 person years in 2011. 2 In Ontario, Canada, the highest incidence was reported in males ages 30 to 39 at 57.0 per 100 000 person years. 3 Lemme et al 4 reported a significant increase in ATR from 1.8 per 100 000 person years in 2012 to 2.5 per 100 000 person years in 2016 in the US population with 77.1% occurring in men. As more evidence supports nonoperative management with functional rehabilitation for ATRs, the trending characteristics of this evidence has not been elucidated.3,5,6
While operative repair of the Achilles tendon may decrease the rate of re-rupture, it has also led to more complications compared with nonoperative management, which has been reported to have similar outcomes and less complications.5,7,8 A study by Ochen et al 7 compared outcomes of operative versus nonoperative treatment of acute ATR demonstrating that operative treatment was associated with a significant reduction in re-rupture rate compared with nonoperative treatment. In addition, operative repair of ATR has also led to earlier return to work in select populations and better functional outcomes when evaluated by 2 different jump tests and 1 muscular endurance test.9,10 In a study performed by Lantto et al, 11 comparative outcomes between operative and nonoperative management noted surgery restores calf muscle strength over the entire range of the ankle joint, as well as better quality of life in terms of physical functioning and bodily pain. Conversely, evidence suggests nonoperative management with functional rehabilitation, early weight bearing, and early active mobilization produces similar outcomes and fewer complications when compared with operative treatment.7,8,12,13
There is continuous data comparing treatment selection and outcomes as well as support for nonoperative management with functional rehabilitation and early mobilization for ATR. Given this evidence, this article set out to characterize the trends of treatment in ATR patients and identify whether age or gender may influence rates of operative repair.
Methods and Materials
Data Source
Patient records were retrospectively reviewed using the PearlDiver database (PearlDiver, Inc, Fort Wayne, IN), which is a large nationwide commercially available administrative claims database consisting of roughly 144 million patients derived from across multiple insurance provider groups in the United States. This study used the “MLExtr” dataset, a sub-dataset of the 144 million patients that specifically contains patient records pertaining to procedures or diagnoses of the lower extremity. Patient data were queried from this dataset using Current Procedural Technology (CPT) and International Classification of Diseases (ICD), Ninth Revision and Tenth Revision (ICD-9/ICD-10) codes. Institutional review board exemption was granted through our institution as the provided data were deidentified and compliant with the Health Insurance Portability and Accountability Act.
Patient Selection
Utilizing both ICD-9 and ICD-10 diagnostic codes, patient data were initially queried for a diagnosis of ATR. As this study sought to capture the trends of operative management over the previous decade, data collection was narrowed to include the beginning of 2010 through 2019. After identifying patients who were diagnosed with an ATR from 2010 through 2019, data were queried to determine whether they underwent operative repair for their ATR injury within 6 weeks from initial injury. The two CPT codes used to identify operative treatment of an ATR included CPT-27650 (Repair, primary, open or percutaneous, ruptured Achilles tendon) and CPT-27652 (Repair, primary, open or percutaneous, ruptured Achilles tendon; with graft [includes obtaining graft]). If patients did not have one of the two CPT codes associated with their ATR within 6 weeks after the initial rupture, they were deemed to have undergone nonoperative treatment. Identified patients were then stratified by age (ages 18-30, 31-45, and 46 and older) and then further divided by gender (male or female). 14 In addition to characterizing the overall trends in management for an ATR, subgroup analyses were performed to determine the trends in ATR treatment for the following: (A) males, (B) females, (C) patients aged 18 to 30, (D) patients aged 31 to 45, and (E) patients aged 46 and older. Patients who had a concurrent diagnosis of Achilles tendonitis were excluded to ensure only patients with an ATR were being studied. In addition, the study decided to exclude patients under the age of 18 as ATRs in the pediatric population are rare and typically involve a different mechanism of injury ared to adults. 15 The ICD codes used in this study are included in Supplemental Appendix Table A1.
Statistical Analysis
Statistical analysis was performed using R statistical software (R Project for Statistical Computing, Vienna, Austria) integrated within the PearlDiver software and Microsoft Excel (Microsoft Corporation, Redmond, WA) with the XLStat statistical package add-on (Addinsoft Inc., New York, NY) with an α level set to 0.05. Trend analyses were performed with the Cochran-Armitage Trend test to evaluate the 2-tailed null hypothesis that the overall, male, and female rates of operative management for ATR remained constant (ie, did not increase or decrease), and whether age impacted the proportional trend of operative treatment. Within each age cohort, a chi-square analysis was performed to determine whether the proportion of patients receiving an operation in 2010 was statistically different from those receiving an operation in 2019. In addition, logistic regression analysis was used to calculate adjusted odds ratios (OR) with corresponding 95% confidence intervals (CI) to assess whether males or females were more likely to receive operative treatment for ATR. Elixhauser Comorbidity Index (ECI), diabetes mellitus, and tobacco use were controlled for to decrease their confounding effects on the overall health of the Achilles tendon and treatment choice.16,17
Results
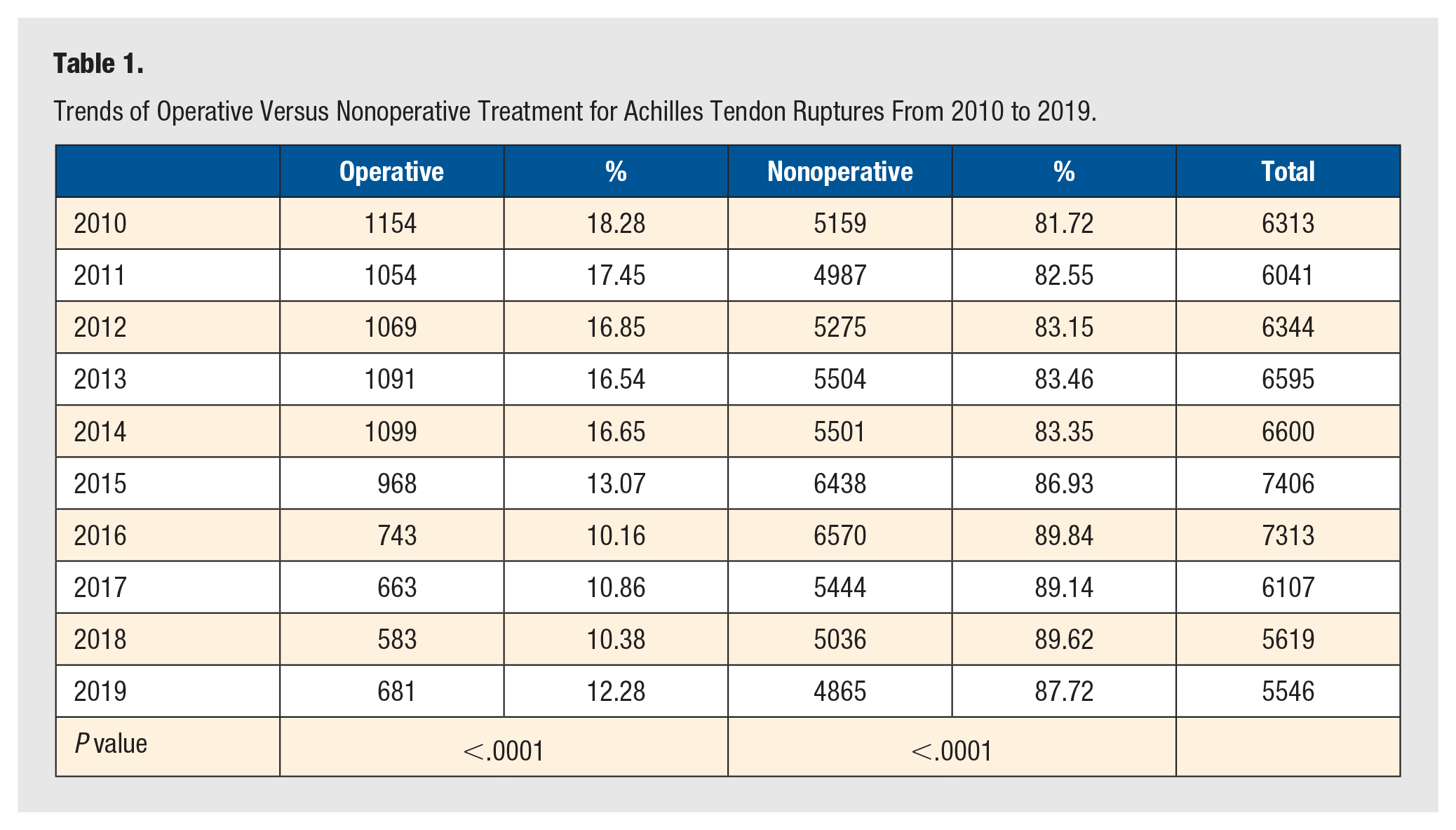
A total of 63 884 patients experienced ATR injuries from 2010 through 2019: 3852 aged 18 to 30, 14 888 aged 31 to 45, and 45 144 aged 46 and over. There were 9105 (14.3%) adult patients who received an operation within 6 weeks their initial ATR injury, and 54 779 (85.7%) adult patients who did not undergo operative treatment within 6 weeks. As outlined in Figure 1 and Table 1, trend analysis demonstrated that the proportion of operative management decreased significantly over the previous decade (18.3%-12.3%, P < .0001). In addition, the steepest decline in operatively managed patients occurred from 2014 to 2015 with a 78.5% decrease in operations during this year.
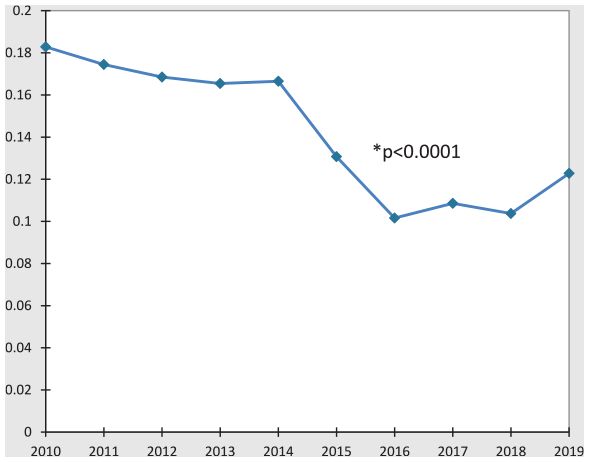
Proportional trend of operative treatment for Achilles tendon ruptures from 2010 to 2019.
Trends of Operative Versus Nonoperative Treatment for Achilles Tendon Ruptures From 2010 to 2019.
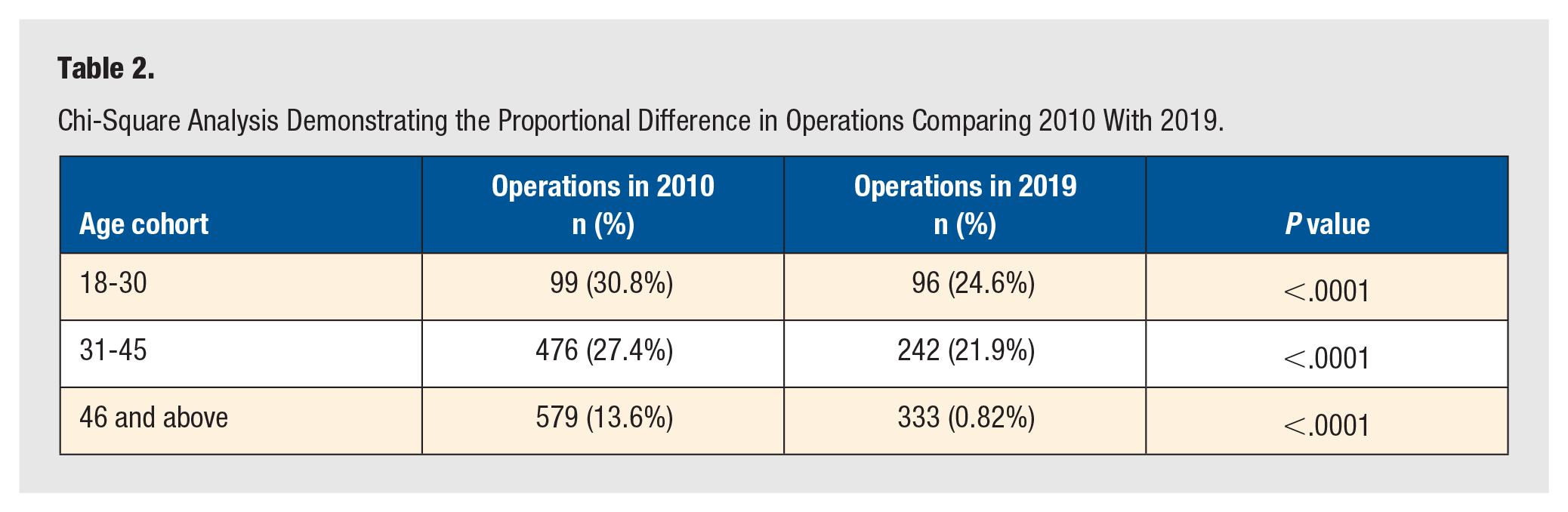
Trend analyses demonstrated that the proportion of operative compared with nonoperative treatment decreased significantly in both males and females (25.8%-21.4% and 9.0%-5.7%, respectively, both P < .0001) (Figure 2A and 2B). With respect to gender, the rates of operative treatment decreased by 83.1% in males and 63.1% in females. In each individual age cohort, the proportion of operatively managed patients significantly decreased when comparing 2010 with 2019 (age 18-30: 30.8% vs. 24.6%, age 31-45: 27.4% vs. 21.9%, age 46 and older: 13.6% vs. 8.2%, all P < .0001) (Table 2). However, among the patients who did receive operative treatment, the proportion of operative patients aged 18 to 30 significantly increased (8.6%-14.3%, P < .0001), the proportion of operative patients aged 31 to 45 significantly decreased (41.3%-36.1%, P < .0001), and the proportion of operative patients aged 46 and older remained relatively constant (50.2% vs. 49.6%, P = .593) (Figure 3).
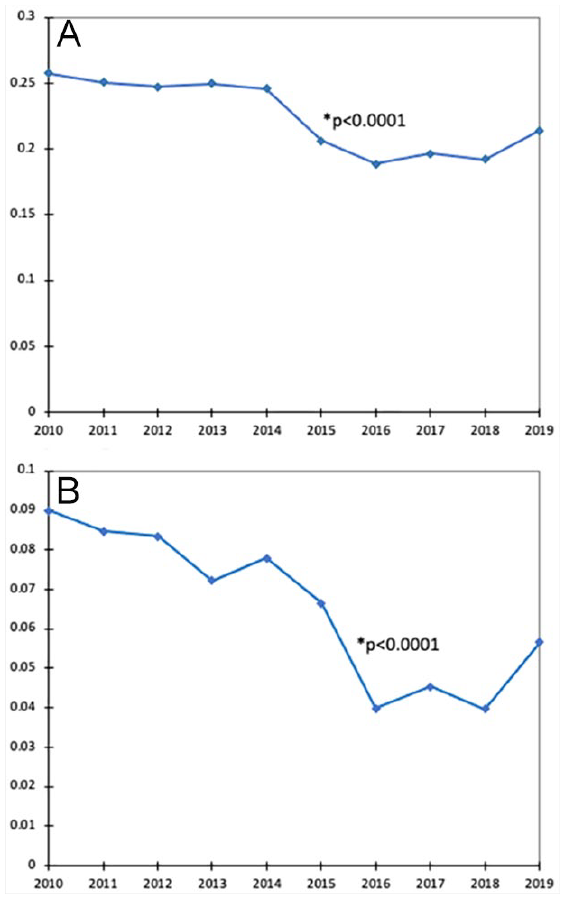
(A) The trend of operative management for Achilles tendon ruptures in males. (B) The rates of operative management for Achilles tendon ruptures in females.
Chi-Square Analysis Demonstrating the Proportional Difference in Operations Comparing 2010 With 2019.
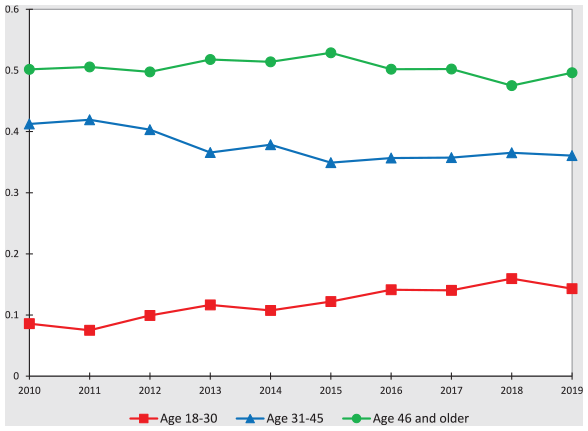
Among operative patients, the trends demonstrating the proportion of operative management and the influence of age.
As outlined in Table 3, gender analyses controlling for ECI, diabetes mellitus, and tobacco use revealed that males in all cohorts were significantly more likely to receive operative treatment for an ATR over the previous decade. In patients aged 18 to 30, a total of 796 (76.2%) males who received operative management (OR: 2.63, CI: 2.24-3.10). Among patients aged 31 to 45, a total of 2818 (81.5%) males received operative management (OR: 3.22, CI: 2.93-3.55). A total of 3372 (73.7%) male patients who were 46 and older received operative treatment for their ATR (OR: 3.21, CI: 2.99-3.44).
Odds Ratio Comparing Which Gender in Each Age Cohort Was More Likely to Undergo Either Operative Treatment Throughout the Decade.
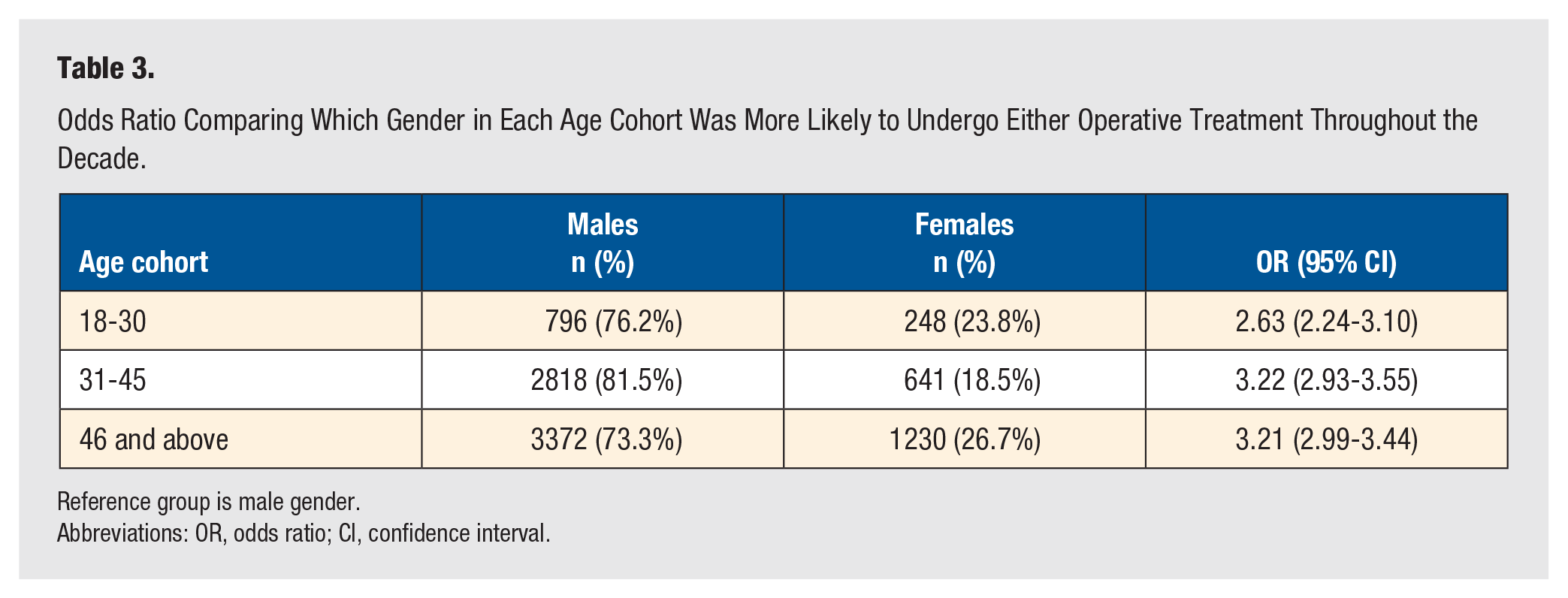
Reference group is male gender.
Abbreviations: OR, odds ratio; CI, confidence interval.
Discussion
Overall, from 2010 through 2019, there was decline in operative repair of ATR (18.3%-12.3%, P < .0001); a trend demonstrated in several other studies as well.1,3,5,18,19 A multicenter, randomized control by Willits et al 8 compared outcomes of ATRs who underwent nonoperative management with functional rehabilitation to operative treatment reporting that all measured outcomes of nonoperative management were acceptable and clinically similar to those of operative treatment while avoiding the complications associated with operative management. In addition, a meta-analysis of randomized trials comparing functional rehabilitation with early range of motion demonstrated that re-rupture rates were equal for operative and nonoperative patients, and the increased risk of having a complication other than a re-rupture in the operative group (risk difference 15.8%) may outweigh the increased risk of re-rupture in the nonoperative group if functional rehabilitation is not an option (risk difference 8.8%). 9 Given the convincing evidence supporting functional rehabilitation for ATR, the trends presented in the present study align with a decreased pursuit of operative management over the previous decade.
Age is a common consideration when indicating and offering surgery for many orthopaedic conditions. Using an animal model, Pardes et al 20 reported numerous alterations in Achilles tendon properties with increased age, including inferior material properties, increased ankle joint passive stiffness, and decreased propulsion force during locomotion. This could explain the varying rates of ATRs with the 46 and older cohort experiencing 70.7% of ATR injuries in the present study. Also reflected in this study is the influence of age in operatively managed ATRs with the increase in the proportion of operative management among the 18 to 30 cohort, and the decrease in the proportion of operative management among the 31 to 46 cohort. Older populations have been demonstrated to have less successful Achilles tendon repairs with higher rates of complications following both operative and nonoperative management. 21 A previous study by Hussien et al 22 reported, specifically for Achilles tendon repair, patients who returned with a postoperative surgical infection had a significantly higher mean age compared with patients with no postoperative surgical infection (53.66 ± 13.53 and 45.48 ± 14.27 years, respectively), and each additional year of age increases the likelihood of developing a surgical infection by a factor of 1.0303 (P = .03). Conversely, Maffulli et al 13 suggested percutaneous repair under local anesthesia for acute rupture of the Achilles tendon in patients older than 65 years provided good results in terms of postoperative ATR scores (ATRS), calf circumference, and isometric plantar flexion strength.
The present study demonstrated a significant difference in patients receiving operative treatment, with males being more likely to receive surgery for an ATR across all age groups. One potential explanation for males being more likely to receive an operation for ATR could be attributed to the differences in outcomes between genders following surgery. Silbernagel et al 23 reported females had significantly more symptoms after operative treatment compared with males at both 6 (mean ± SD ATRS, 59 ± 24 vs. 73 ± 19) and 12 months (74 ± 27 vs. 86.5 ± 17); however, this association was not present in the nonoperative group. In addition, it has been reported that females are historically more inclined to pursue less dynamic activities in this age range which could account for the discrepancy in incidence; however, this cultural gap is closing rapidly with more female sports available and participation increasing. 24 Studies done during the Covid-19 pandemic have especially highlighted the continued disproportionate household responsibilities of females who therefore may not undergo surgical repair even if offered.25,26 Similar to the present study, Huttunen et al 6 previously reported a proportional decrease in operatively managed ATR patients from 2001 to 2012 from 43% to 28% in males and 34% to 22% in females; however, the difference in operative rates between genders would benefit from further studies.
There are several limitations for this study. As the PearlDiver database only provides data on a specific group of patients during a certain time period, sampling bias is present. With the onset of ICD-10 codes in 2015, and manual examination and selection of both ICD-9 and ICD-10 codes for this study, there is a potential of coding discrepancies when selecting ICD-10 codes that corresponded with ICD-9 codes. However, to reduce this potential limitation, a coding translator was used to ensure that selected ICD-10 codes corresponded correctly with ICD-9 codes. Although the PearlDiver database contains over 144 million patient records and includes patients insured by all payers (ie, commercial health plans, Medicare, Medicaid, and other government insurance plans), it must be acknowledged that the results presented may not reflect the US population as a whole or the population with ATR receiving operative or nonoperative treatment. However, compared with prior datasets provided by PearlDiver that were limited to Medicare-only and/or single commercial carriers, the current dataset includes all payers and has significantly improved national representation. The main goal of this study was to identify trends in ATRs and management; therefore, the results of this study do not ascertain prospective information such as outcomes and complications of operative versus nonoperative management. As a claims based database prevents the authors from accurately quantifying a patient’s activity level, it is impossible to determine a patient’s level of activity which may have influenced the surgeon’s decision as to whether the patient is or is not a suitable surgical candidate. Although logistic regression analyses comparing the likelihood of operative management between males and females controlled for ECI, diabetes, and tobacco use, other known and unknown confounders could have influenced the results. While this study attempted to capture patients who underwent operative management for ATR in the acute stage (ie, 6 weeks), it does not account for patients who may have failed nonoperative management and received an operation beyond this time frame. Last, when performing a study using a database system that relies on patient claims, there is the possibility of human error created from incorrect medical billing coding input. However, in a study from the Centers for Medicare and Medicaid Services (CMS), such instances of incorrect medical billing input only occur in about 1.0% of overall payments, thus this would likely have minimal impact on the results of this study. 27
Conclusion
Overall rates of operative management for ATR decreased across all cohorts likely due to previous studies providing evidence of similar results between operative and nonoperative managements. Over the previous decade, males were demonstrated to be far more likely than females to undergo operative management. Why females are less likely to receive an operation for ATR is likely multi-factorial and requires further exploration.
Supplemental Material
sj-docx-1-fas-10.1177_19386400221102745 – Supplemental material for Rates of Operative Management for Achilles Tendon Rupture Over the Last Decade and the Influence of Gender and Age
Supplemental material, sj-docx-1-fas-10.1177_19386400221102745 for Rates of Operative Management for Achilles Tendon Rupture Over the Last Decade and the Influence of Gender and Age by J. Heath Wilder, Sione A. Ofa, Olivia C. Lee, Naomi E. Gadinsky, Ramon F. Rodriguez and William F. Sherman in Foot & Ankle Specialist
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Consent was not applicable to this study as this study utilized a HIPAA compliant deidentified patient database.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.