
Abstract
Background
The aim of the study was to evaluate the clinical and functional outcomes following suturing of sheath of peroneal tendons to the calcaneal plate as an innovative technique for reduction of peroneal tendon instability (PTI) accompanying calcaneal fracture surgically treated via extensile lateral approach (ELA).
Methods
In a retrospective comparative study, among 245 operatively treated calcaneal fractures through ELA, we had 33 cases with PTI who underwent relocation of the peroneal tendons with ethibond suture in a figure-of-8 shape, passed through 2 parts of sheath of peroneal tendons and stitched to the calcaneal plate. Of the 33 cases, 12 were evaluated in the experimental group. Twelve surgically treated calcaneal fractures without PTI were matched as the control group. The outcome of the patients was assessed by American Orthopaedic Foot & Ankle Society (AOFAS) Ankle-Hindfoot Scale, Foot Function Index (FFI) percentage, Visual Analog Scale (VAS) pain, changes in Tegner activity level, maximal peroneal muscles strength testing, modified Star Excursion Balance Test (mSEBT), and triple hop for distance (THD) test. For the last 3 tests, the difference between operated and normal feet was calculated for each patient and this difference was compared between the 2 groups.
Results
There was no statistically significant difference between the 2 groups for AOFAS Ankle-Hindfoot Scale (P = .09), FFI percentage (P = .12), VAS pain (P = .73), changes in Tegner activity level (P = .87), maximal peroneal muscles strength testing (P = .45), mSEBT (P > .05), and THD (P = .87) tests. We had a case with point tenderness on retromalleolar groove and 4 cases with paresthesia in the territory of the sural nerve in the experimental group in contrary to one case of sural nerve paresthesia in the control group (P = .31).
Conclusions
Relocation of peroneal tendons in PTI accompanying calcaneal fractures by fixing sheath of peroneal tendons to the calcaneal plate could be an acceptable procedure with good outcomes but may have increased chance of sural nerve injury.
Levels of Evidence:
Therapeutic, Level III: Retrospective
“We introduce an innovative surgical technique to stabilize the peroneal tendons in the retromalleolar groove by suturing of sheath of peroneal tendons instead of peroneal tendons to the calcaneal plate during ELA.”
Introduction
Calcaneal fractures are rare injuries with annual incidence of 11.5 per 100 000 people. Men are affected about 2.5 times more than women. Displaced intra-articular calcaneal fracture is the most common type.1 -4 Recently, operative reduction and fixation of displaced calcaneal fractures have become more popular in order to achieve anatomical joint reduction and restoration of the shape and height of the calcaneus. 5 Operative management of displaced calcaneal fractures is a technically demanding procedure which is better to be done by an experienced surgeon. There are potential complications following surgical treatment of displaced calcaneal fractures including wound breakdown, superficial and deep infections, subtalar and calcaneocuboid joint degenerative arthritis, varus or valgus malalignment and other malreductions, sural nerve neuritis, peroneal tendon tenosynovitis and stenosis, prominent hardware, hardware breakage, muscle atrophy and weakness, and joint stiffness.6 -8
One of the important associated injury with displaced calcaneal fractures which may be easily missed is peroneal tendon instability (PTI) from its anatomical position in the retromalleolar groove. 9 The overall prevalence of PTI accompanying calcaneal fractures is 11.6% to 29.3%.9 -12 The peroneal tendons are restricted in a fibro-osseous tunnel in the retromalleolar groove covered by a fibrotic superior peroneal retinaculum (SPR). At the time of injury, harshly displaced lateral wall of the calcaneus can hit the fibula tip. If the released energy would be high enough, it could lead to tear of SPR or bony avulsion of SPR.8,13 Although bony avulsion of SPR or fibular fleck sign is radiographically obvious in ankle radiographs 13 or computer tomography (CT) scan, SPR integrity must be checked before wound closure by intraoperative peroneal retinaculum intactness testing. 11
The usual surgical technique to reduce the peroneal tendons in the retromalleolar groove is incising longitudinally on the posterior ridge of the lateral malleolus and fixing the SPR or bone avulsion to its anatomical position by a suture anchor or passing sutures to the bone, pull out suture technique.8,14 The other 2 described techniques for relocation of the peroneal tendons in extensile lateral approach (ELA) of the calcaneus are fixing the peroneal tendons to the calcaneal plate 15 or elevating the lateral fasciocutaneous flap over the anterior part of the fibula tip and direct repair of the SPR to the retromalleolar groove by a suture anchor. 11
To the best of our knowledge, there is no clinical comparative study in the literature to elucidate the functional outcome of surgically treated calcaneal fractures with relocation of peroneal tendons in their anatomical position. In this study, we introduce an innovative surgical technique to stabilize the peroneal tendons in the retromalleolar groove by suturing of sheath of peroneal tendons instead of peroneal tendons 15 to the calcaneal plate during ELA. Also, we compared the clinical and functional outcomes of the cases treated by this surgical technique with a group of matched cases of displaced calcaneal fractures without PTI who underwent open reduction and internal fixation (ORIF) through ELA.
Materials and Methods
After approval of the study by the ethic committee of the university in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments (research ethics certificate approval ID: IR.SUMS.MED.REC.1398.477) in a retrospective comparative study, all consecutive calcaneal fractures that underwent ORIF by the senior author (A.R.V.) were reviewed from April 2015 to April 2019. Inclusion criteria were unilateral closed displaced intra-articular calcaneal fracture or displaced calcaneal body fractures surgically treated through ELA with PTI without fibula fleck sign. Ten months was considered as the minimum follow-up period. Exclusion criteria were bilateral calcaneal fractures, open calcaneal fractures, sanders type IV calcaneal fractures, calcaneal fractures with primary subtalar arthrodesis, concomitant lower limb fracture or previous surgeries, simultaneous spinal fracture with cord injuries, sinus tarsi approach or minimally invasive surgeries, SPR bony avulsion approved in the preoperative CT scan, postoperative wound breakdown, postoperative infection, patients suffering from balance disorder, and patients refused to participate in the research. The eligible cases were asked to have a visit for assessing the clinical and functional outcomes after getting an informed written consent. Based on the subjects in the experimental group, the control group was selected among patients who underwent ORIF of calcaneal fracture through ELA without intraoperatively approved PTI. It was tried to match the control group to the experimental group regarding gender, age, follow-up period, and the number of displaced fractured fragments of the posterior facet of calcaneus observed intraoperatively, Sanders Classification. 16 Our aim to select these cases for the control group was to evaluate any possible complications or unfortunate consequences related to our new surgical technique such as decrease in strength of the peroneal tendons, reduction in range of motion of the ankle joint and/or subtalar joint, increase in pain score, and so on. These complications might be the result of adhesions of the peroneal tendons to the surrounding tissues after suturing the sheath of peroneal tendons to the calcaneal plate. Therefore, we decided to compare our cases with a matched group that underwent ORIF via ELA without PTI, instead of comparing with the usual surgical technique for relocation of the peroneal tendons via a separate incision on posteroinferior of the lateral malleolus.
Surgical Technique
Under general or spinal anesthesia, in lateral decubitus position, after inflating the tourniquet, through ELA to the calcaneus, a full-thickness fasciocutaneous flap was elevated from lateral wall of the calcaneus by subperiosteal dissection. In our technique, we do not extend the vertical limb more than the fibula tip, proximally, and it is just anterolateral to the Achilles tendon to reduce the risk of injury to the lateral calcaneal artery. The horizontal limb is made at the junction of the glabrous and non-glabrous skin, extended to the calcaneocuboid joint. After ORIF of the calcaneal fracture with a lag screw and a locking calcaneal plate on lateral wall, based on the standard steps of ORIF of calcaneal fracture, 17 PTI was checked by inserting a surgical curve clamp in the sheath of peroneal tendons from distal and sliding it proximally to the retromalleolar groove. By forcing the peroneal tendons anteriorly, anterior dislocation was recognized. In most cases, the empty retromalleolar groove could be touched by a clamp, and crossing of the peroneal tendons on anterior of fibula tip was obvious (Figure 1). In cases with PTI, no. 2 ethibond suture, in a figure-of-8 shape, was passed through 2 parts of the sheath of peroneal tendons (Figure 2). We assured that no part of peroneal tendons was caught by gliding the tendons distally. After milking the tendons from anterior part of the lateral malleolus to the retromalleolar groove, first the proximal suture and then the distal one were tied, and sheath of peroneal tendons was fixed to the plate, either in an empty screw hole or around frame of the calcaneal plate (Figure 3). Finally, the reduction of peroneal tendons was approved again by passing the curved clamp to the directory of the peroneal tendons and checking the stability of peroneal tendons in the retromalleolar groove (Figure 4).
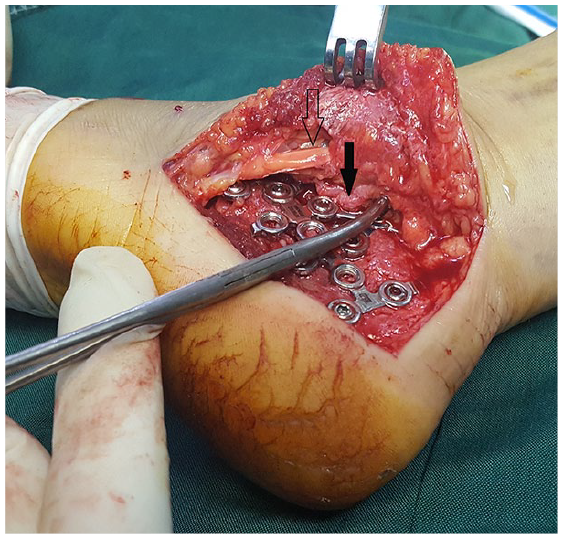
Touching the empty retromalleolar groove by a clamp and crossing of the dislocated peroneal tendons (empty arrow) on anterior of fibula tip (solid arrow).
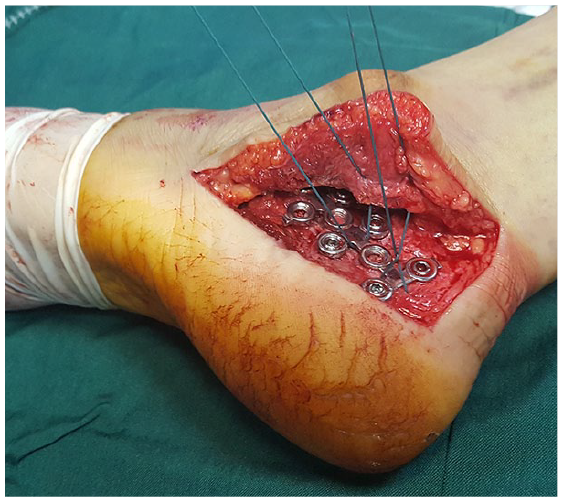
Passing of ethibond sutures through peroneal tendon sheath and calcaneal plate frame.
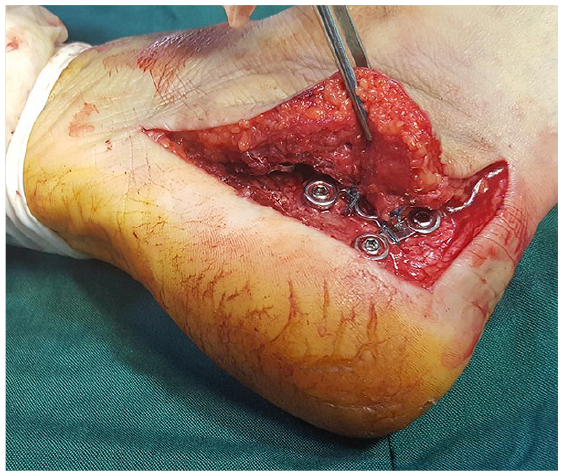
Tying the sutures.
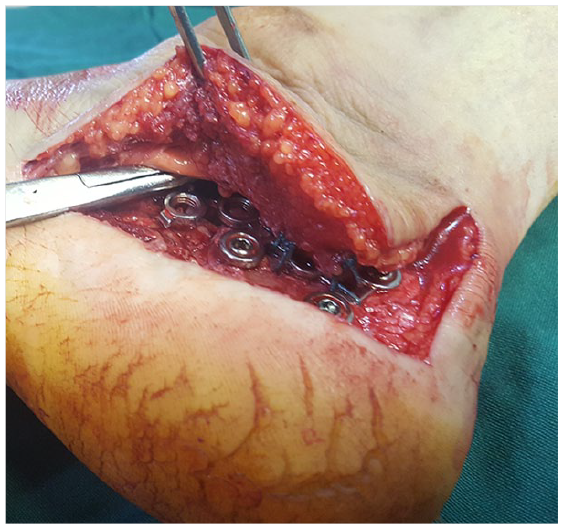
Approving the reduction of peroneal tendons by inserting and sliding the curved clamp in the directory of peroneal tendons.
After closing the fasciocutaneous flap and skin over a drain, short leg cast was applied. After 6 weeks, the cast was changed to posterior short leg slab, and physiotherapy was started. At 12 weeks following the surgery, the patient was permitted to have full weight-bearing with high-top shoes.
Clinical Assessment
The patients were evaluated using American Orthopaedic Foot & Ankle Society (AOFAS) Ankle-Hindfoot Scale, Foot Function Index (FFI) percentage, Visual Analog Scale (VAS) pain, and Tegner activity level.18,19 For Tegner activity level, the changes between before injury and at the follow-up visit were calculated. Furthermore, the swelling on lateral of the calcaneus in comparison to the uninjured side, any paresthesia in the territory of the sural nerve, and point tenderness on posterior of lateral malleolus on the peroneal tendons were evaluated.
Functional Examination
The patients were asked for functional tests including maximal peroneal muscles strength testing, modified Star Excursion Balance Test (mSEBT), and triple hop for distance (THD) test. The former was done using Biometrics DataLOG (Biometrics DataLOG MWX8, Gwent, UK) handheld dynamometer with MyoMeter M550 connected to evaluate the strength of peroneal muscles. Channel sensitivity was set on 3 mVdc, with sampling rate of 50, and excitation output was 2000 mV. To do the strength testing, the patient lied supine on the table. Both legs were isometrically examined. At first, the uninjured leg was tested for which the leg was fixed and the MyoMeter was put at the lateral border of the foot. The patient was asked to exert the maximal possible force to the device while the foot is in plantarflexed and everted position. The first test was done only for familiarization. Then, 3 repetitions were taken, each held for 5 seconds, and 30 seconds of interval was given between repetitions. Then, the injured leg was tested using the same procedure. The peak torque in kilogram produced during each test was recorded, and the maximum peak torque was used for analysis. 20
After 5 minutes of rest, mSEBT was taken for which triple strip meters pointing to anterior, posteromedial, and posterolateral, starting from the same point, were attached on the ground. The patient stood at the cross site of the triple meters with hands on hips and the navicular bone of the testing lower limb above the cross point. At first, the uninjured side was tested with the other leg pointing to each mentioned directions, respectively. They had 6 familiarization practices in each direction and then 3 repetitions of the main test. The tested foot had to be in complete contact with the ground, and the patient was told not to remove any part of the foot, especially the heel, from the ground during the test. If they lost their balance or their hands detached from the hip, the test would be considered as wrong and it would be repeated until an errorless test was performed. They could have 5 to 10 seconds of rest between each repetition, and 15 to 30 second interval was given between different directions. The mean distance reached in 3 main trials of each direction in centimeter was calculated. The tests were repeated for injured limb as well. 21
The last test was the THD test, in that the patient stood one legged before the starting point of a 6 meter strip with injured foot above the ground. The hands could move freely during the test. After 2 trials of practice, 2 main tests were taken, and the maximum distance reached after 3 executive hops was recorded. The average between 2 main tests in centimeter was recorded. If the patients’ hands touched the wall or if the other foot touched the ground, the test was taken again. The injured limb was also tested the same. 22
Statistical Analysis
Data analysis was performed in SPSS version 16 using Chi-square and Fisher exact test for categorical variables. Independent t test was used to compare the mean between 2 groups when normality assumptions were met; otherwise, Mann-Whitney U test was used. P value ≤.05 was considered statistically significant.
For functional variables, the difference of mean value between injured and uninjured limbs for each patient was measured. Then, the analysis was done for the calculated differences, between the experimental group and the control group.
Results
Among 245 operatively treated calcaneal fractures through ELA, 33 cases had PTI approved by intraoperative SPR intactness testing. Of the 33 cases who underwent suturing of sheath of peroneal tendons to the calcaneal plate, only 12 cases were accepted to participate in this survey or be eligible. Demographic data and the results of clinical and functional outcomes are reported in Tables 1 and 2.
Demographic Data and Outcome of All Patients in the Experimental Group.
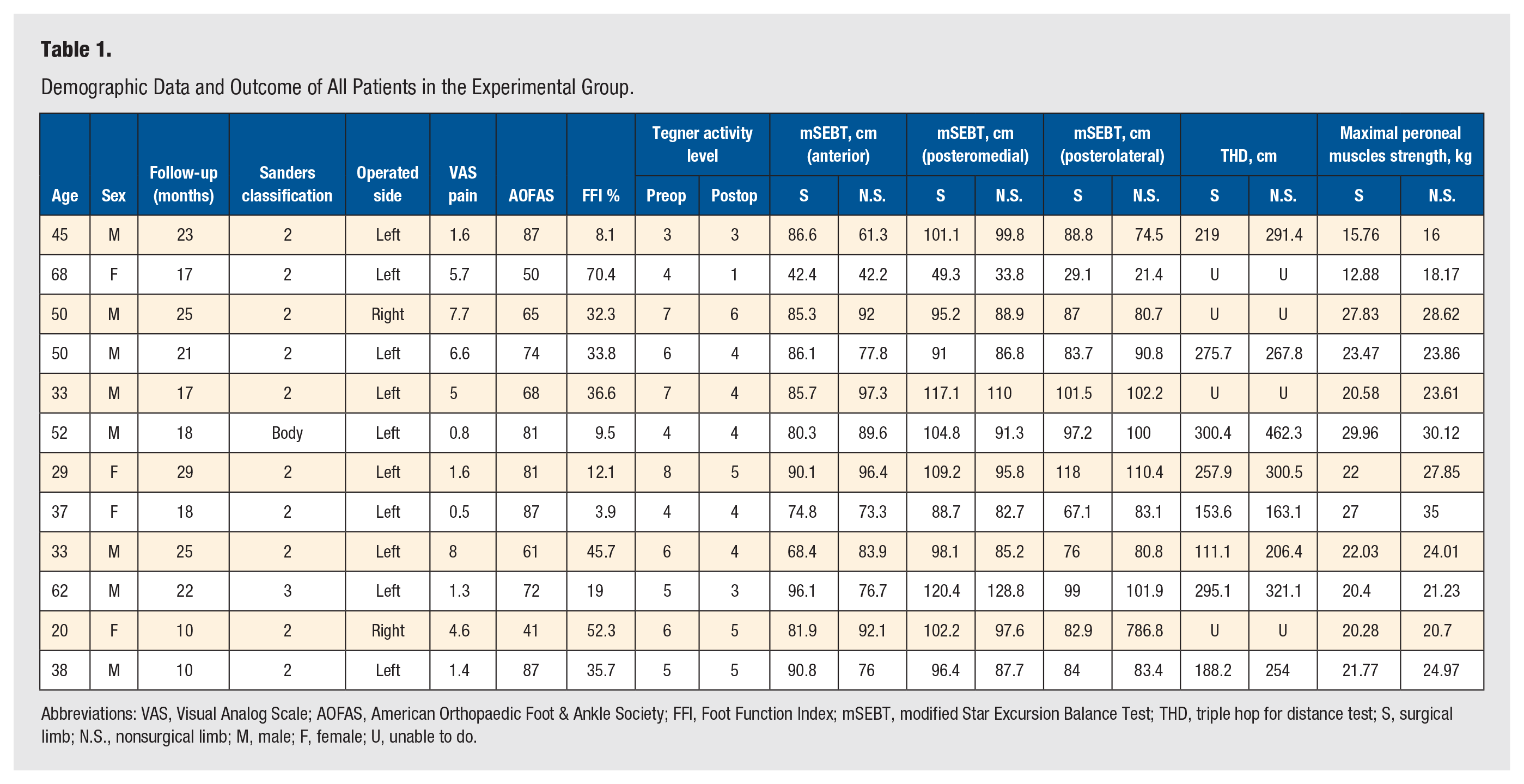
Abbreviations: VAS, Visual Analog Scale; AOFAS, American Orthopaedic Foot & Ankle Society; FFI, Foot Function Index; mSEBT, modified Star Excursion Balance Test; THD, triple hop for distance test; S, surgical limb; N.S., nonsurgical limb; M, male; F, female; U, unable to do.
Demographic and Outcome of All Patients in the Control Group.
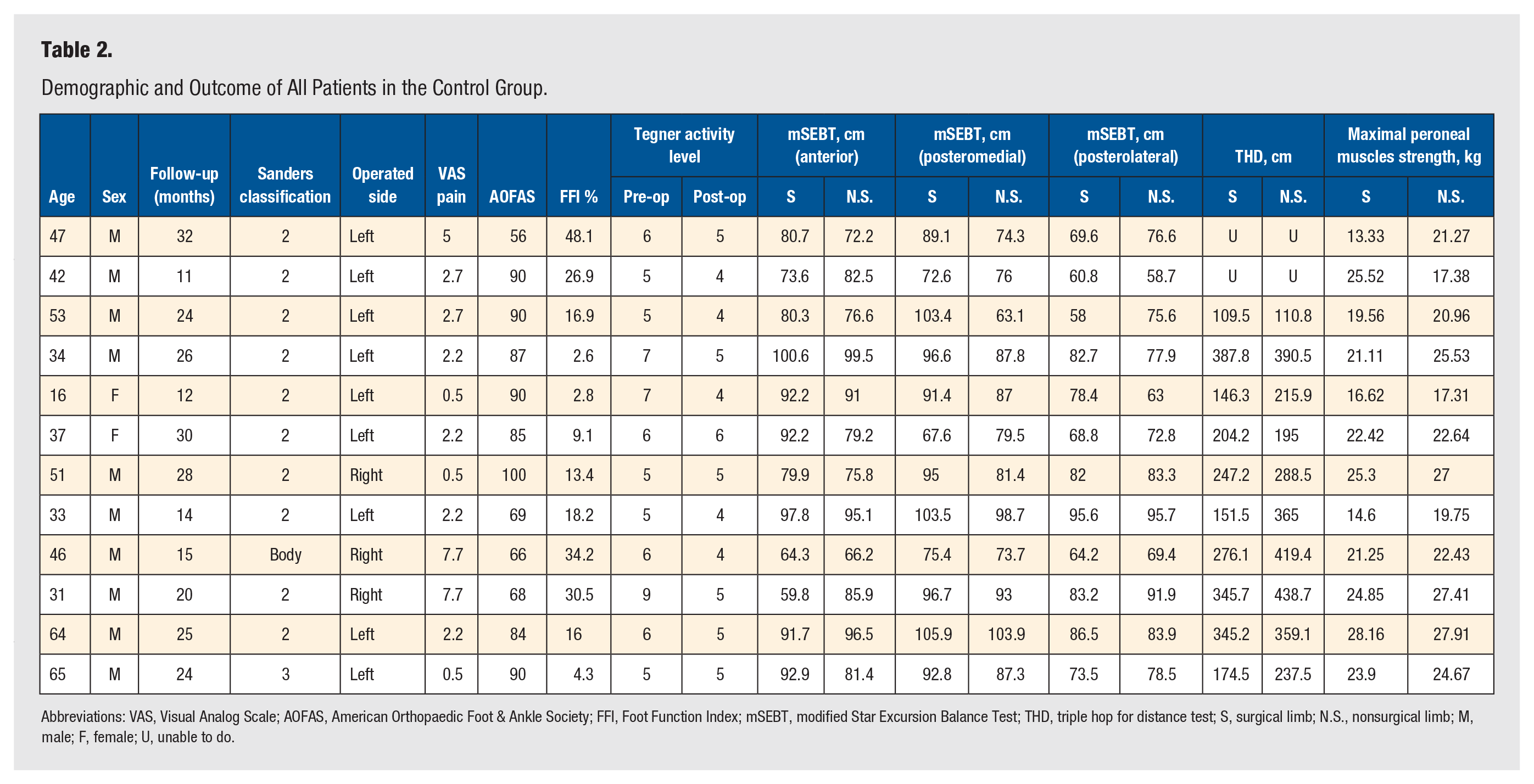
Abbreviations: VAS, Visual Analog Scale; AOFAS, American Orthopaedic Foot & Ankle Society; FFI, Foot Function Index; mSEBT, modified Star Excursion Balance Test; THD, triple hop for distance test; S, surgical limb; N.S., nonsurgical limb; M, male; F, female; U, unable to do.
In each group, there were 10 Sanders type II, a case of Sanders type III, and a calcaneal body fracture with intact posterior facet. There were 8 (66.7%) men in the experimental group and 10 (83.3%) men in the control group (P = .64). Mean age of the patients in the experimental group was 43.1 ± 14.0 years and in the control group was 43.3 ± 14.2 years (P = .98). Also, mean follow-up visit for the experimental group was 19.6 ± 5.8 months and for the control group was 21.8 ± 7.2 months (P = .43) (Table 3). Therefore, the patients in both groups were statistically matched.
Baseline Characteristics of Matched Groups.
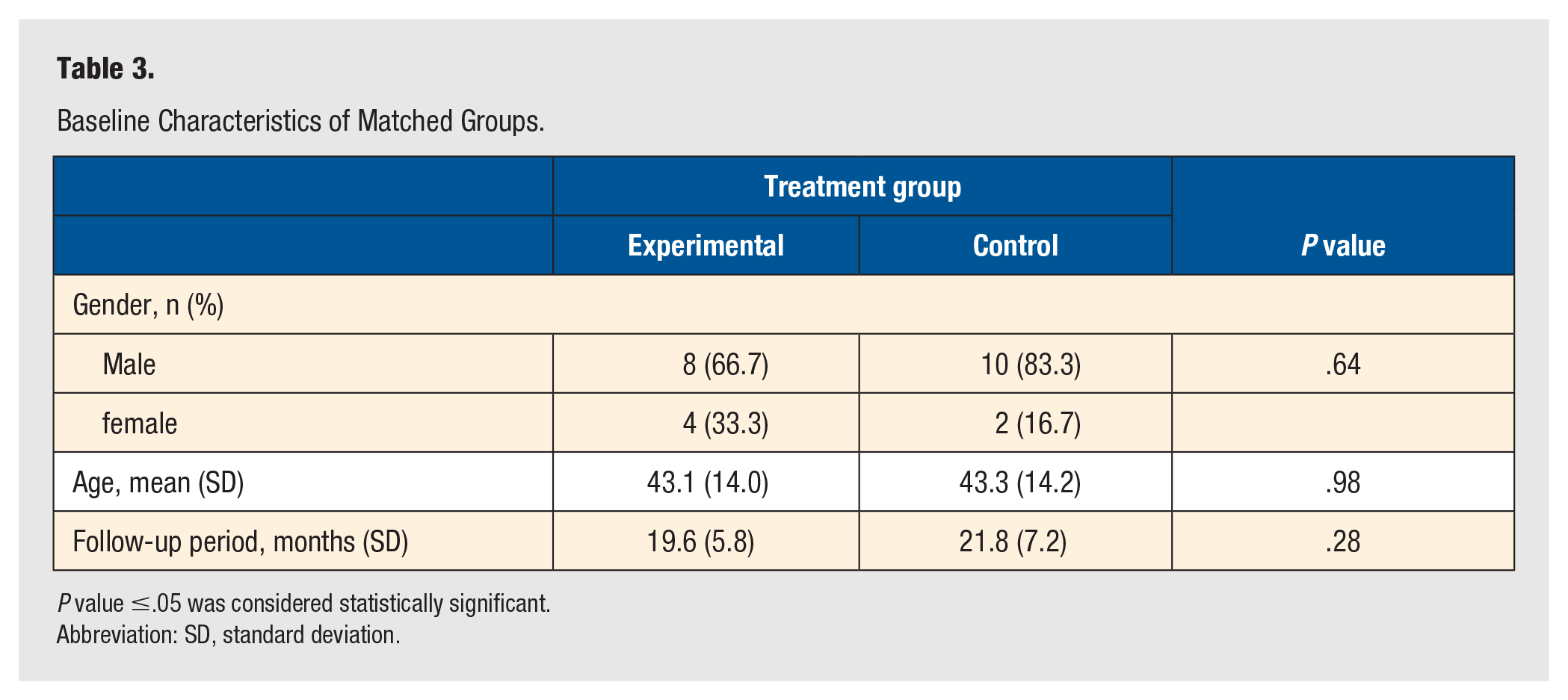
P value ≤.05 was considered statistically significant.
Abbreviation: SD, standard deviation.
Ten cases in the experimental group (83.3%) and 7 cases in the control group (58.3%) had swelling on lateral side of the calcaneus in comparison to the uninjured side (P = .37). Moreover, 4 cases in the experimental group (33.3%) and 1 case in the control group (8.3%) had paresthesia in the territory of the sural nerve (P = .31). Only 1 case in the experimental group had point tenderness on posterolateral of lateral malleolus on the peroneal tendons.
The postoperative clinical assessment showed that the VAS pain (P = .73), AOFAS Ankle-Hindfoot Scale (P = .09), FFI percentage (P = .12), and changes in Tegner activity level (P = .87) were not statistically significant between the 2 groups. Furthermore, our analysis indicated that the differences in functional tests of injured and uninjured legs were not statistically significant between the control and the experimental groups (Table 4).
Clinical and Functional Outcomes of Both Treatment Groups.
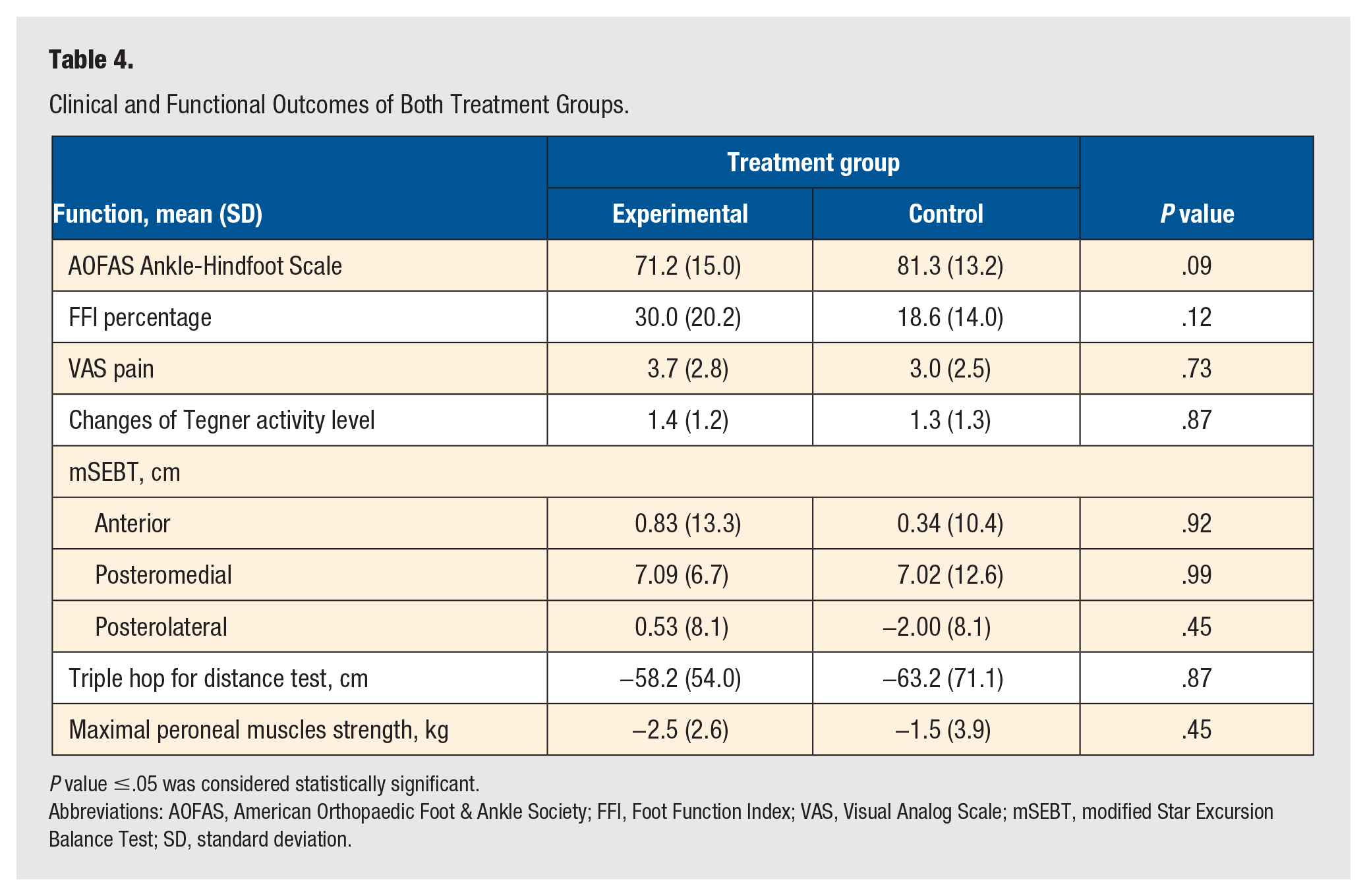
P value ≤.05 was considered statistically significant.
Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; FFI, Foot Function Index; VAS, Visual Analog Scale; mSEBT, modified Star Excursion Balance Test; SD, standard deviation.
Discussion
Combination of displaced calcaneal fractures and PTI is an entity in foot and ankle surgeries that needs more researches to clarify the best surgical technique and the final outcomes, especially nowadays by increasing the tendency of orthopaedic surgeons to treat displaced intra-articular calcaneal fracture operatively. The timely diagnosis and treatment of PTI during ORIF of displaced calcaneal fractures are very important to have a good outcome. Up to about 53% of PTI associated with calcaneal fracture are initially misdiagnosed or overlooked.9,12 Untreated PTI can lead to peroneal muscles atrophy and shortening with final result of ankle instability, weakness, and chronic pain. 23 Notably, an asymptomatic untreated case of PTI approved by magnetic resonance imaging, 4 years after ORIF of a calcaneal fracture, has been reported in the literature. 9
Several studies tried to accurately diagnose PTI accompanying calcaneal fractures by reviewing preoperative CT scan or ankle radiographs.9,11,12 Obviously, fleck signs from posterolateral of fibula tip, indicative of SPR avulsion fracture, are easier to detect in x-ray-based modalities. Increasing fracture severity according to the Sanders classification, calcaneal fracture dislocation, enlarged heel width, and soft tissue swelling at lateral malleolar level had direct correlation with increased probability of PTI.9,11 -13 On the other hand, age, open versus closed calcaneal fractures, and excessive lateral wall displacement are not associated with intraoperative approving of PTI. 11 Although CT scan has been considered the standard preoperative method to diagnose PTI, 9 it appears that the preoperative CT scan and radiographs are not reliable enough to diagnose all PTI accompanying displaced calcaneal fractures, especially SPR ruptures without bony fragment.11,24 The gold standard is intraoperative SPR intactness testing, 25 as described in the surgical technique.
We believe that anatomical reduction of the calcaneus by achieving the normal calcaneal shape, height, and Bohler angle may disclose any undiagnosed PTI in the preoperative CT scan. This is in contrary to what was explained by Mak and colleagues 14 They contended that decompression of calcaneal fracture would relocate the peroneal tendons. It is notable to consider the probability of PTI accompanying calcaneal body fractures without posterior facet involvement.
Either nonoperative or operative treatments have been described for PTI after sport injuries.23,26 Five main categories have been explained for surgical treatment of PTI with good results, including SPR repair and reattachment with or without suture anchor, SPR reconstruction, rerouting procedures by transpositioning of peroneal tendons under the calcaneofibular ligament, bone block procedure, and groove-deepening or a combination of the above procedures.27 -30 There is no superiority of one method to the others, and the surgical decision should be individualized. 27
In PTI accompanying calcaneal fractures, relocation of the peroneal tendons during ORIF of a calcaneal fracture is an essential part of the surgery. There are several reported surgical techniques in the literature, but the routine and most frequently used approach is incising the posterior part of the fibula tip after closing the ELA to restore the tension on the soft tissue envelope on lateral of the calcaneus (dual-incision approach). 14 After relocating the peroneal tendons, primary repair of SPR or reattachment of SPR to the posterolateral ridge of fibula tip by a suture anchor or pull out suture technique should be done. 8 We excluded cases with this approach from our study because it is our preferred technique for PTI with bony fleck sign. Ketz and colleagues 11 introduced fixation of SPR to the retromalleolar groove with an interosseous suture anchor though ELA. They extended the exposure and elevated the lateral flap to anterior part of the fibula tip to relocate the peroneal tendons. They did not describe the clinical outcomes or postoperative complications, but considerably, the risk of injury to lateral calcaneal artery may be higher in comparison to our technique. Moreover, in a surgical technique tip, Ehrlichman and colleagues 15 presented relocation of PTI in the retromalleolar groove by suturing around the peroneal tendons using no. 0 Vicryl. They tied the suture in an empty screw hole of the calcaneal plate. Although they did not report any outcome for their technique, there are several disadvantages. The most important, we think, is that fixation of the peroneal tendons to the calcaneal plate is a tenodesis of peroneal tendons; however, they stated that the suture was loose. In addition, using an absorbable suture may increase the inflammation process during its absorption course; hence, this would lead to fibrosis with final result of excursion loss of the peroneal tendons. We fixed the sheath of the peroneal tendons instead of the peroneal tendons to the calcaneal plate.
Based on our analysis, there were no statistical differences for all outcome variables between the experimental and the control group; however, by looking at Table 4, we found that AOFAS Ankle-Hindfoot Scale, FFI percentage, and VAS pain were better in the control group. The main reason may be the number of cases in each group. It should be considered that matching more cases in this trial would be very difficult and we hope it could be done in the upcoming researches. Furthermore, we believe that calcaneal fractures accompanying PTI usually have a higher energy trauma with lesser clinical outcome scores.
We thought that peroneal tendon strength would become weaker than the uninjured limb after ORIF of calcaneal fractures through ELA, due to adhesions of the tendons to the calcaneal plate during the healing phase. Moreover, it was important for us to find out whether suturing the sheath of peroneal tendons would lead to more adhesions of the peroneal tendons with loss of their power in comparison to the cases without PTI. This was the main reason we compared these 2 groups, instead of including cases with standard dual-incision approach. Based on our results, this theory was approved by reduction in strength of peroneal tendons of about 1.5 ± 3.9 kg in the case group and 2.5 ± 2.6 kg in the experimental group; however, our analysis did not reveal any significant differences between groups for the strength of peroneal tendons. Although we tried our best to match the control group to the experimental group, the most important weak point in this study was uncontrollable quality and quantity of physiotherapy sessions following the surgery between groups with definite direct effect on the power of tendons. Other limitations are retrospective nature of our research, limited postoperative follow-up, and assessing of the cases by the same individual.
The main advantage of our technique is approaching by a single incision without needing to extend the standard ELA. The disadvantage would be sural nerve injury which was seen more in the experimental group than the control group.
In conclusion, relocation of peroneal tendons in PTI accompanying calcaneal fractures by fixing sheath of peroneal tendons to the calcaneal plate could be an acceptable procedure with good outcomes but may have increased chance of sural nerve injury.
Footnotes
Acknowledgements
This article has been obtained from a thesis (registered no. 98-01-01-20790) submitted to the Shiraz University of Medical Sciences in partial fulfillment of the requirement for the degree of specialty in orthopaedic surgery. The project is sponsored by Bone and Joint Diseases Research Center, Shiraz University of Medical Sciences.
Authors’ Contributions
A.R.V. contributed to the conception and design of the work, operated the patients, reviewed the images, drafted the paper, and revised it critically for important intellectual content study. B.H. contributed to the design of the work, took the photos, asked the patient for follow-up visit, analyzed the data, and drafted the paper. S.K. and A.A. contributed to the data acquisition, examined the patients at the follow-up visit, and drafted the paper. Z.S. analyzed the data and drafted the paper. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was financed by Shiraz University of Medical Sciences (grant number: 98-01-01-20790).
Ethical Approval
This study was performed after the approval of the study by the ethical committee of Shiraz University of Medical Sciences in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments (Approval ID: IR.SUMS.MED.REC.1398.477). All methods in this retrospective study with human participants were carried out in accordance with the relevant guidelines and regulations. The need for written informed consent was waived by Shiraz University of Medical Sciences ethics committee due to retrospective nature of the study.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Availability of Data and Material
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.