
Abstract
Background
The Trabecular Metal (Zimmer Biomet, Warsaw, IN) total ankle arthroplasty (TAA) system uses a lateral approach with a fibular osteotomy to gain access to the tibiotalar joint and a sagittally curved tibial component. This is the first TAA system to laterally approach the ankle, and few studies have explored outcomes associated with this implant. This study aimed to report the 5-year clinical and radiographic outcomes as well as the survivorship of the implant.
Methods
Over a 3-year period, 2 fellowship-trained foot and ankle surgeons used this implant system to treat 38 end-stage arthritic ankles. Reoperation and revision data were collected from all patients (100%) as part of the local prospective database. Patients completed the Foot and Ankle Outcome Score (FAOS) questionnaire preoperatively and at each annual follow-up visit; scores for a minimum of 5 years were available for 28 (73.7%) patients. A radiographic analysis compared postoperative coronal and sagittal alignment in weightbearing radiographs at a minimum of 5 years with that at 3 months postoperatively, as well as cyst or lucency formation, which was available for 21 patients (55.3%).
Results
At 5 years, there were 3 revisions (7.9%) and 9 reoperations (23.7%). Reoperations included 4 fibular hardware removal and 5 medial gutter debridement procedures. The FAOS significantly improved for all domains (P < .05). Implant positioning did not significantly change between 3 months and 5 years postoperatively.
Conclusion
Our 5-year results in this small series using this unique prosthesis showed good overall survivorship (92.1%) and a reoperation rate of 23.7%, along with clinically significant improvement in patient-reported outcomes.
Levels of Evidence:
Level IV: Retrospective case series
“This study of the 5-year follow-up after lateral Trabecular Metal TAAs describes a survivorship of 92.1% with a reoperation rate of 23.7% and 1 case of amputation (2.6%). There were excellent clinical outcomes, with improvements in patient-reported outcomes that exceeded the MCID in all domains.”
Introduction
Total ankle arthroplasty (TAA) has been developed historically through an anterior approach for visualization of the medial-lateral aspects of the joint while having limited access to the posterior aspect. Many previous outcome studies on midterm survivorship and clinical outcomes of anteriorly approached TAA systems have been conducted, demonstrating overall favorable outcomes but significant rates of tibial osteolysis and wound complications.1 -5 The Trabecular Metal TAA system (Zimmer Biomet, Warsaw, Indiana) introduces a lateral approach to TAA to potentially address these issues,6,7 while presenting other benefits that can affect postoperative outcomes and implant survivorship.
Additional benefits of a laterally based TAA include the ability to remove the fibular hardware and to use a prior fibular incision, which are both likely to be present since a substantial proportion of patients with posttraumatic ankle arthritis have already had a fibula fracture operatively treated with the lateral approach. The lateral approach encounters only the superficial peroneal nerve, which is typically more anteriorly located, and thus avoids injury to anterior neurovascular bundles and the extensor tendons’ iatrogenic bowstring effect. In addition, implantation through a lateral incision allows the tibial component to be curved in the sagittal plane while visualizing the center of rotation and as such can reduce the amount of bone resection. The curved nature of the tibial component following the trabecular lines, along with the use of trabecular metal that has not been used previously, may influence the osteointegration process to reduce the rate of tibial osteolysis. 6 Finally, the use of an alignment guide and foot holder may help control varus and valgus deformities.
While having these proposed benefits, a lateral approach may also present new issues such as difficulty with coronal plane adjustment and gutter debridement, especially of the medial gutter. In addition, in cases where an old lateral incision is used, there may be increased difficulty in the approach due to the presence of scar tissue and adhesions. The various benefits and drawbacks of the lateral approach may influence long-term outcomes of the trabecular metal TAA system; however, few studies have reported the midterm outcomes of this implant. 8 It is essential to evaluate the midterm survivorship, clinical outcomes, and radiographic outcomes of this TAA system to understand the effects of the changes in approach and implant design and determine its utility and safety in clinical practice. Therefore, the goal of this study was to report on the 5-year clinical and radiographic outcomes of this prosthesis as well as the survivorship of the implant with the hypothesis that this was a safe treatment option for end-stage ankle arthritis (ESAA), comparable to other TAA systems currently available.
Methods
Between February 2013 and March 2016, the Trabecular Metal TAA (Zimmer Biomet) system was used through a lateral approach. Two fellowship-trained foot and ankle surgeons offered this surgery as part of the standard of care for ankle arthritis. The indication for a surgery was symptomatic ESAA that failed conservative treatment, which included activity modification, nonsteroidal drugs, brace, physical therapy, shoe-wear modification, and steroid injections to the ankle. All patients were given the option of ankle fusion versus replacement. The final decision was made in a shared decision-making process, influenced by age, range of motion, level of activity, alignment, adjacent deformity, and patients' expectations.
Thirty-eight consecutive patients who underwent a TAA with the trabecular metal system using a lateral approach were included in this study. As part of the local foot and ankle database, demographic information including age, sex, side, and body mass index (BMI) was recorded. Surgery-specific information including component sizes and concurrent procedures was also gathered. As seen in Table 1, the cohort consisted of 38 patients (45% female) with an average age of 64 years (95% CI: 61-67) and average BMI of 28 kg/m2 (95% CI: 26-30). Concurrent procedures done with TAA, listed in Table 1, include medial malleolar prophylactic fixation in 9 patients (23.7%), Achilles lengthening in 7 patients (18.4%), medializing calcaneal osteotomy in 10 patients (26.3%), and Broström-Gould lateral ligament repair in 7 patients (18.4%). This study received approval from the steering committee of an institutional review board (IRB)-approved foot and ankle registry (IRB #2013-038) at the authors’ institution.
Baseline Demographic Characteristics.
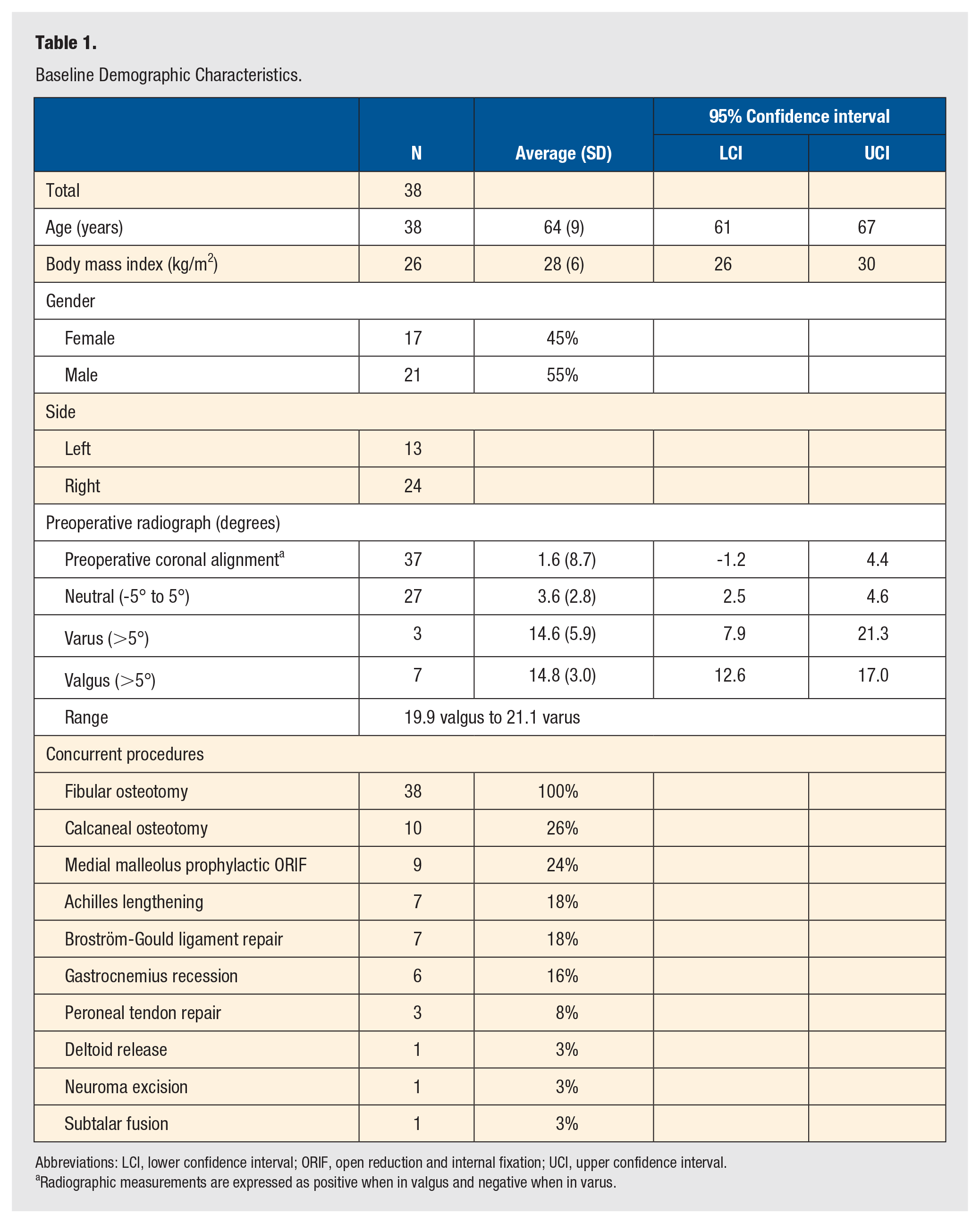
Abbreviations: LCI, lower confidence interval; ORIF, open reduction and internal fixation; UCI, upper confidence interval.
Radiographic measurements are expressed as positive when in valgus and negative when in varus.
Revision, Reoperation, and Complications
The primary outcome of this study was survivorship of the implant, defined as the need for revision of one of the metallic components of the ankle prosthesis or conversion to an ankle arthrodesis. Further chart review recorded the reoperations or the hardware related to the lateral approach. Reoperation was defined as a subsequent surgery that did not include removal of one of the metallic components for any reason related to pain at the ankle or to improve alignment of the ankle or foot. Complications were recorded using the standardized Canadian Orthopaedic Foot and Ankle Society coding system. 9
Surgical Technique
Most cases were performed as joint cases with both surgeons present in the room to operate and assist interchangeably to ensure a similar technique. Surgery was performed with the patient supine. A lateral incision was made over the fibula. A fibular osteotomy was performed obliquely in a proximal-to-distal fashion. The osteotomy would go up to approximately the level of the syndesmosis. The anterior ligaments would then be severed, and the fibula would be rotated posteriorly. The ankle was then exposed along the talar neck and tibia. The lower leg was then put into the foot holder and positioned so that a mortise view of the ankle could be obtained and that the anterior portion of the talar strip was parallel with the grid and the tibial shaft was parallel with the rod and grid. The axis of rotation would be determined by making a small arthrotomy medially and inserting a small osteotome perpendicular to the foot holder. When there was severe varus deformity that did not warrant adequate reduction to achieve a parallel joint line, a medial-side incision was used to release the deltoid ligament. Sizing of the implant was then done, the drill guide was placed, and drill holes were made in the talus and tibia. The joint surfaces were swept with the burr. The rail hole guides were placed with a spreader pin. Once these were confirmed to be in good position under fluoroscopy, they were pinned, and the rail holes were made. The guides were then removed, and the trials were placed. After testing the range of motion, a gastronomies recession or Achilles tendon lengthening would be performed if increased dorsiflexion was desired. When necessary, a calcaneal osteotomy, either medial or lateral side, was determined to neutralize heel alignment. The final components were then placed with the inserters. The fibular osteotomy was then fixed with a one-third tubular nonlocking plate. Notably, bone cement was not used during implantation.
Radiographic Outcomes
The authors routinely ordered weightbearing anteroposterior (AP), mortise, and lateral view radiographs of the ankle preoperatively, 3 months after the surgery, and then at every subsequent follow-up, which generally includes visits at 6 months, 1 year, 2 years, and 5 years after the surgery. The radiographs were analyzed by a senior musculoskeletal radiologist with a foot and ankle subspecialty. Well-accepted reliable measurements, as previously described by Usuelli et al, 10 were performed on each set of radiographs taken. The coronal alignment angle was measured on the AP radiograph (alpha angle [α]), meanwhile the tibial slope (beta angle [ß]) and talar slope angle (gamma angle [γ]) were measured on the lateral-view radiograph. The earliest radiograph to assess for weightbearing alignment was available at the 3-month time. Initial weightbearing postoperative radiographs were taken on average 2.6 (95% CI: 2.2-3.0) months after the index surgery. A significant change in the tibial or talar components was described as a change of at least 5° in angulation. Radiographs at the 5-year mark were available for patients who presented for follow-up and accepted to undergo radiographs. A total of 21 patients (55.3%) had completed 5-year radiographs. Measurements from the first weightbearing radiographs at 3 months and the last radiographs at 5-year follow-up were compared.
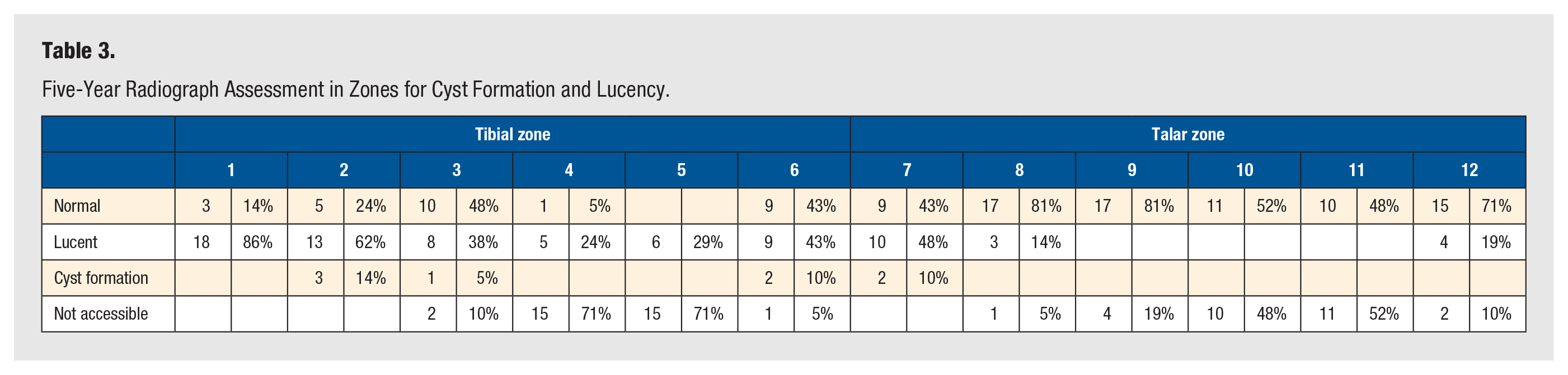
Each 5-year radiograph was reviewed by a foot-and-ankle musculoskeletal fellowship-trained attending radiologist to assess for lucency or cystic formation. Zones previously described in the literature 11 were described as “normal,” “lucent” (<2-mm radiolucent line), or “not accessible” in cases where it was hidden by the plate.
Patient-Reported Outcomes
All patients were included in the local foot and ankle database and were sent surveys prospectively as part of the Foot and Ankle Orthopaedic Registry at the authors’ institution. The surveys included the Foot and Ankle Outcome Score (FAOS), a patient-reported outcome that has been validated to evaluate ankle arthritis patients. 12 The FAOS consists of 5 domains: pain, activities, sports and recreation, quality of life (QOL), and other symptoms. In this scale, a higher value represented a more favorable outcome. FAOSs for each patient were collected once preoperatively and at the 1-year, 2-year and 5-year follow-up visits. A total of 28 patients (73.7%) had completed a 5-year survey. Ten patients did not complete postoperative surveys despite receiving 3 reminder calls. Improvements in the FAOS score were also compared with previously published minimal clinically important differences (MCIDs) for foot and ankle pathology.13,14 The MCIDs for each of the domains are 25.3 for pain, 11.2 for symptoms, 2.0.0 for functional, 36.8 for sports, and 32.7 for QOL.13,14
Postoperative Management
The standard of care at this institution is to have follow-up appointments at 2 weeks, 6 weeks, 3 months, 6 months, and annually. The patients were placed in a well-padded splint for the first 2 weeks after surgery. They were then immobilized further in a removable orthopaedic boot for an additional 4 weeks. Patients were allowed weightbearing 6 weeks after the surgery with the boot on and initiated outpatient physical therapy from that moment. Patients could ambulate without the boot progressively after 6 weeks postoperatively.
Statistical Analysis
A Kaplan-Meier survival analysis was used to illustrate the survivorship of the implant up until the latest point of follow-up. A prosthesis was considered to have a failure event when a revision of the metal component of the tibial or talar was taking place. A paired t test was used for all data that were normally distributed. Analysis of variance (ANOVA) was used to test for differences between the preoperative, 1-year, 2-year, and 5-year FAOS scores. Minimal clinically important differences for the FAOS were used to determine clinical significance of FAOS improvements. 14 Statistical significance was reached when P values are <.05 in all tests. Analyses were performed with Microsoft Excel (Microsoft, Redmond, Washington) and SPSS statistics (SPSS Inc., Chicago, Illinois).
Results
Radiographic Outcomes
The average preoperative coronal alignment was 1.6° (standard deviation: 8.7) valgus, with most patients (27, 73.0%) having a neutral alignment between 5° of varus and valgus. Three patients had more than 5° of varus, and 7 patients had more than 5° of valgus coronal alignment (Table 1 and Figure 1). Changes from immediate postoperative to latest radiographic outcomes including alpha angle, beta angle, and gamma angle are shown in Table 2, demonstrating no significant differences in any angle between the 2 time points. In Table 3, we note that a total of 6 patients had cyst formation. Zone 2 was the most common (3 patients), followed by zone 6 and 7 who had 2 cases each. Two patients had cyst formation in 2 zones.
Radiographic Parameters.
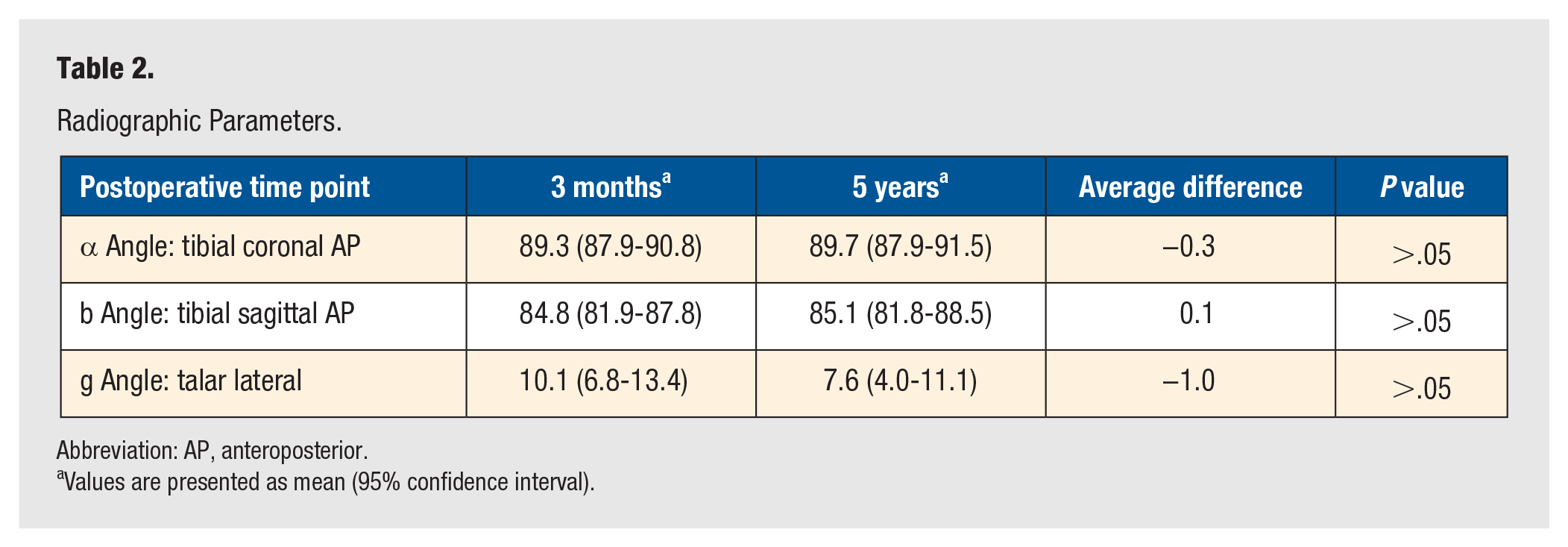
Abbreviation: AP, anteroposterior.
Values are presented as mean (95% confidence interval).
Five-Year Radiograph Assessment in Zones for Cyst Formation and Lucency.
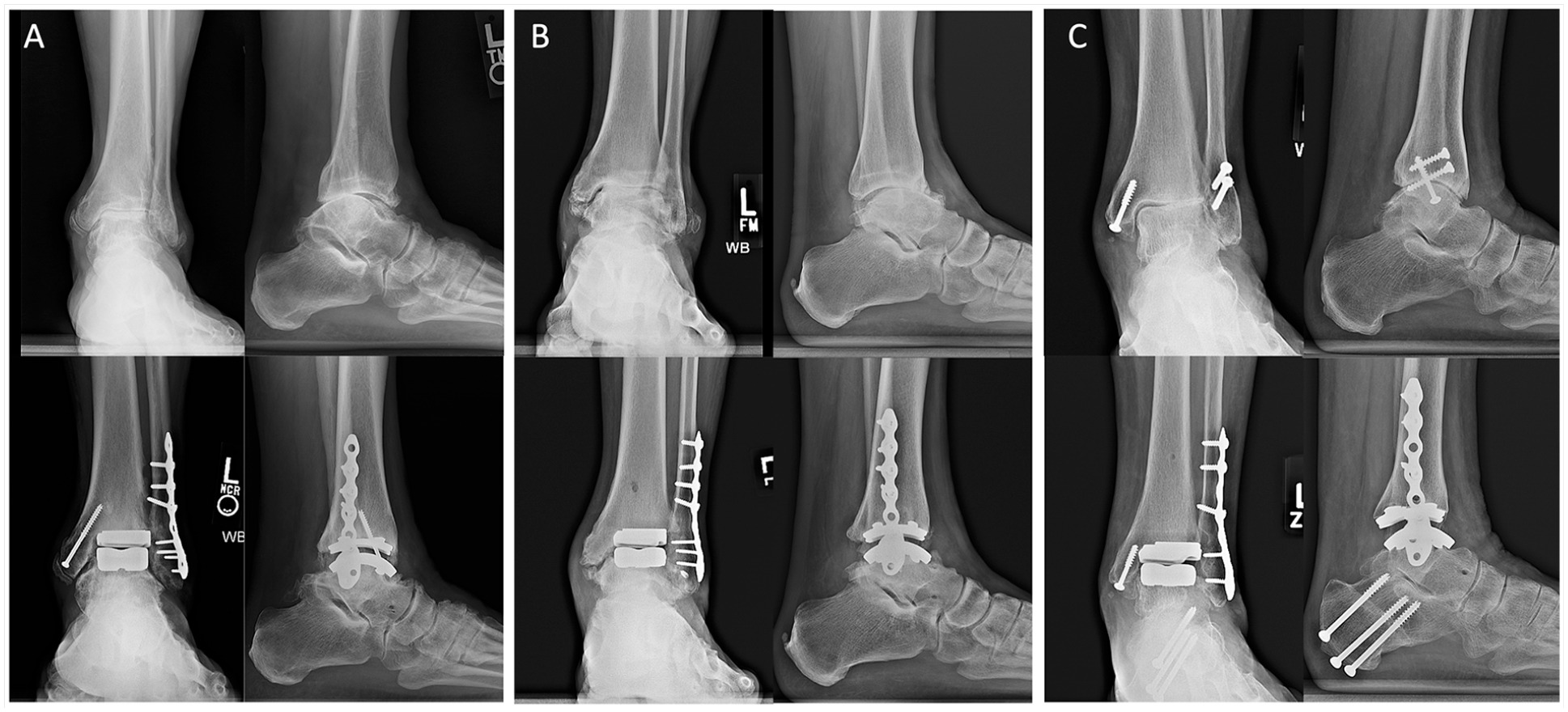
Anteroposterior and lateral radiographs of the ankle in 3 patients (A, B, and C) before and after the trabecular metal total ankle arthroplasty.
Patient-Reported Outcomes
The patient-reported outcomes can be visualized in Table 4. Every 5-year postoperative component of the FAOS was significantly different than the preoperative score. The ANOVA demonstrated significant differences between preoperative scores and 1-year, 2-year, and 5-year scores for all domains (P < .05). There were no significant differences between the 1-year, 2-year, and 5-year scores for any domain. Each average of the differences was superior to the previously published MCID.2,15 As reported in Table 4 as well, for each individual component, more than 50% of patients were above the MCID. As seen in Figure 2, the postoperative outcomes seemed to plateau after 1 year, with a slight tendency for improvement.
Patient-Reported Outcomes Before and After Surgery.
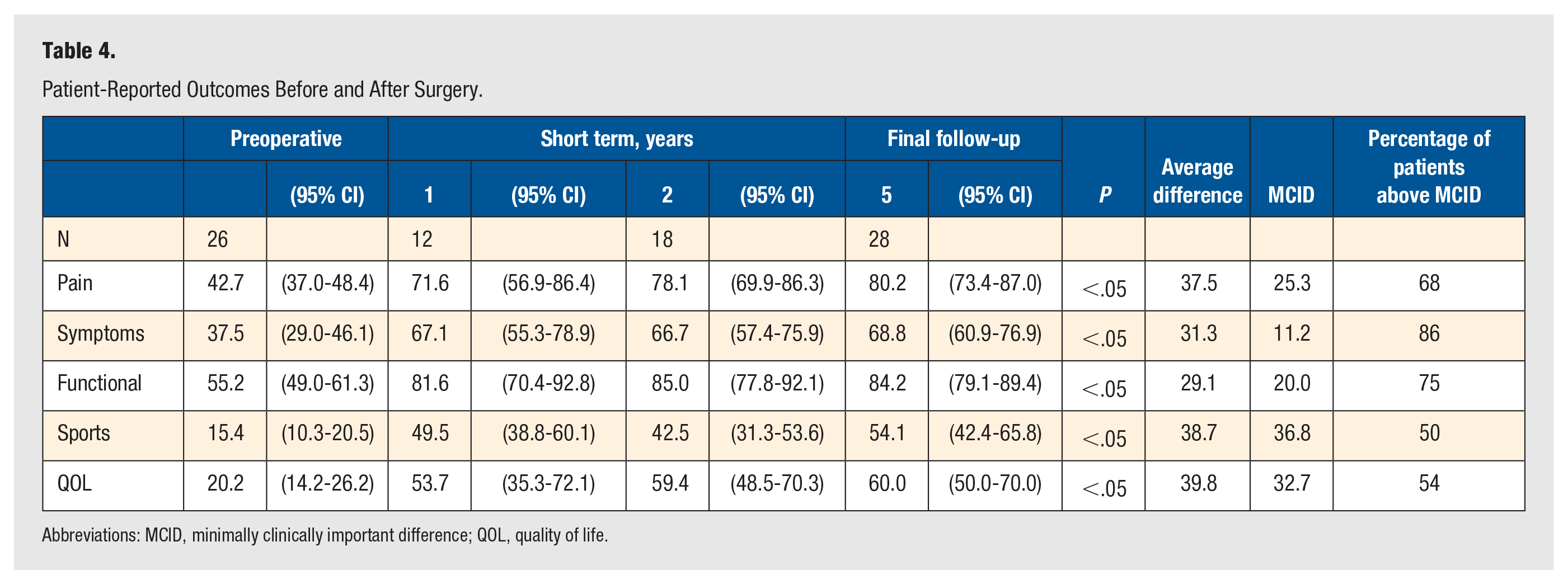
Abbreviations: MCID, minimally clinically important difference; QOL, quality of life.
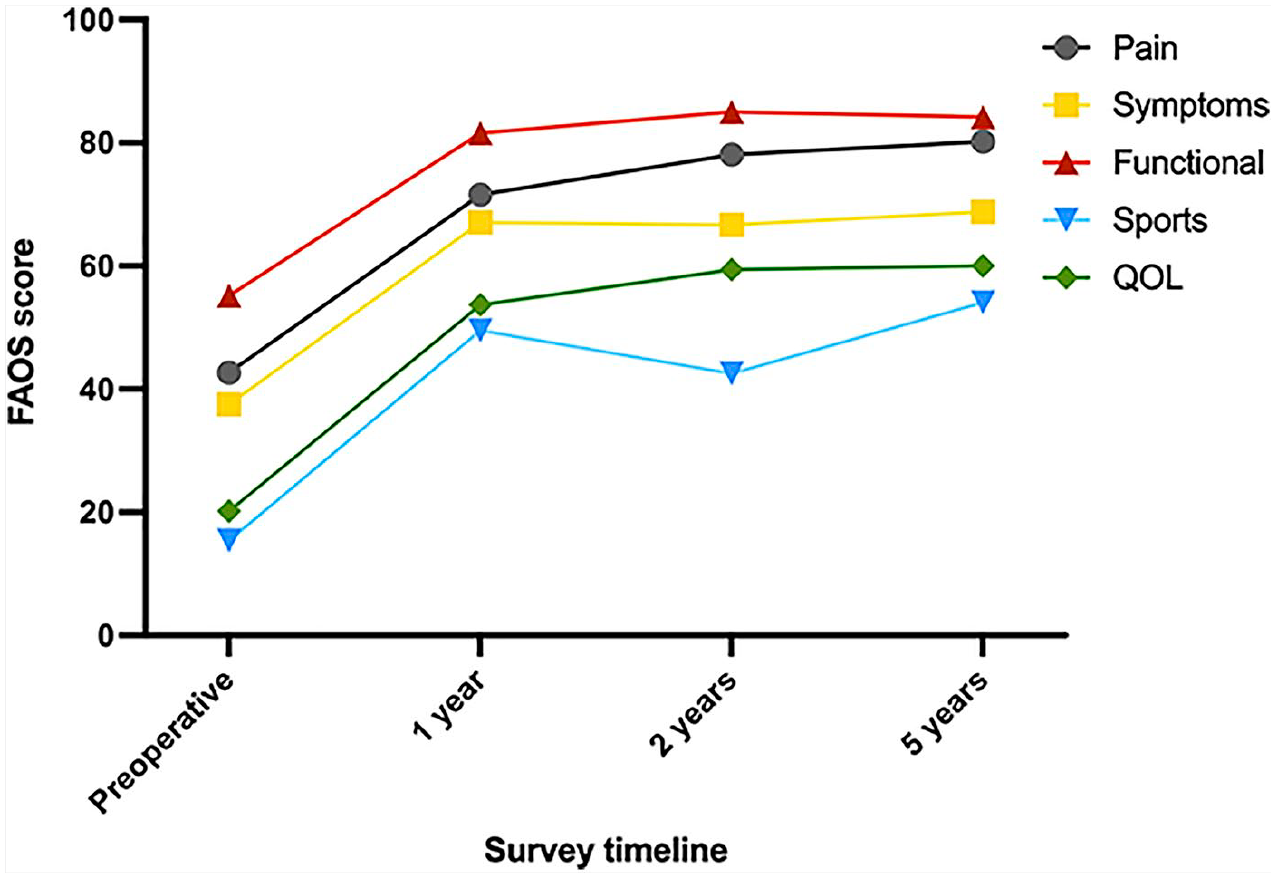
FAOS domains before and after surgery. ANOVA demonstrated significant differences between preoperative scores and 1-year, 2-year, and 5-year scores for all domains. There were no significant differences between the 1-year, 2-year, and 5-year scores for any domain.
Survivorship
Implant survivorship was found to be 92.1% with a 5-year minimum follow-up in this cohort (Figure 3). Revision and reoperation events are shown in Table 5. The 3 events (7.9%) where the implant was extracted were at 12 (2 cases) and 15 months postoperatively. One patient underwent below-the-knee amputation due to recurrence of methicillin-susceptible Staphylococcus aureus (MSSA) infection with a chronic wound (amputation rate 2.6%). A second patient had an infection detected with joint aspiration that grew methicillin-resistant Staphylococcus aureus (MRSA) 12 months after the index procedure and was treated with a 2-stage revision to an INBONE II, which remained in place 5 years after the revision. A third patient had a revision only of the tibial component at 15 months for a symptomatic loose tibial component and no radiographic ingrowth. This patient went on to have the lateral hardware removed at 18 months and a definitive revision to another implant. Other secondary reoperations included 4 fibular hardware removals and 5 medial gutter debridement procedures. A supplementary anterior approach was used for all revisions and gutter debridement procedures.
Reoperations and Revisions Per Patient.
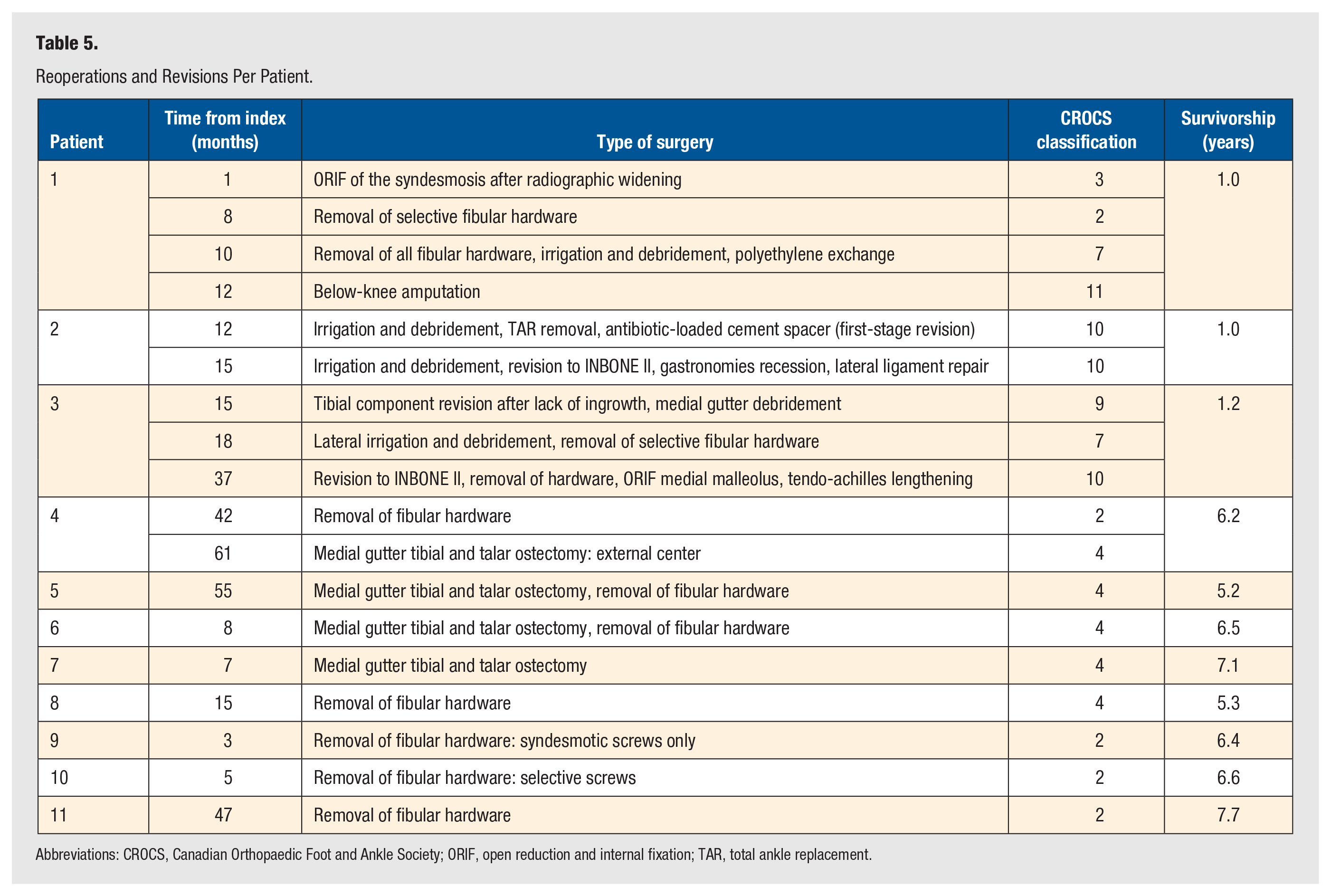
Abbreviations: CROCS, Canadian Orthopaedic Foot and Ankle Society; ORIF, open reduction and internal fixation; TAR, total ankle replacement.
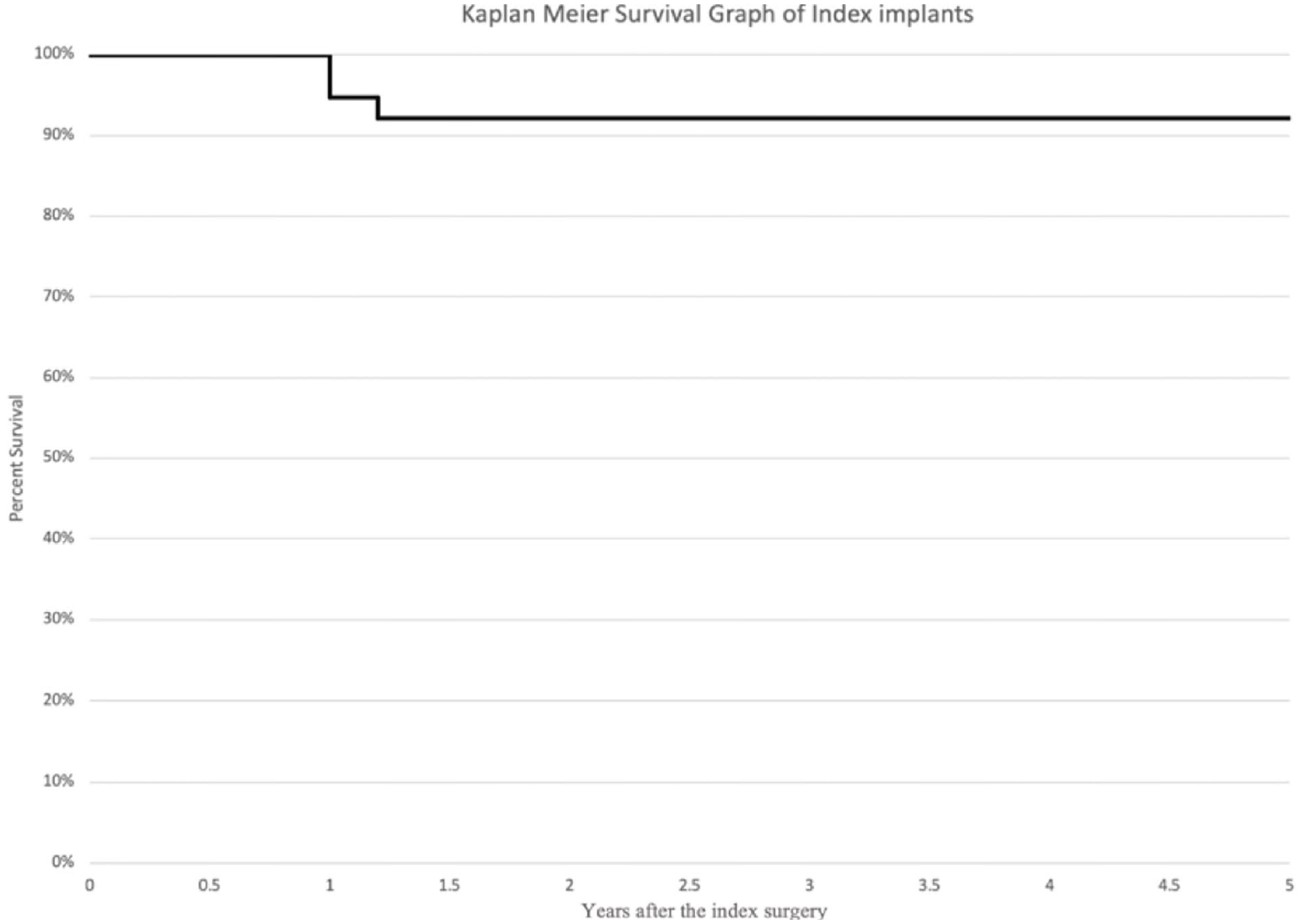
Kaplan-Meier curve demonstrating the survivorship to revision of the trabecular metal implant up to 5 years postoperatively.
Discussion
This study describes a retrospective analysis of a prospectively enrolled cohort of patients treated with a trabecular metal TAA performed through a lateral approach. The cohort demonstrated a 92.1% implant survivorship and clinically significant improvement in patient-reported outcomes above the MCID. This study is only the second to report the clinical improvement with patient-reported outcomes and radiographic outcomes at the minimum 5-year time point. 16 This evidence is essential in increasing the knowledge and understanding or this prosthesis to help guide other clinicians and future TAR development.
Using the FAOS across all domains, the difference between the preoperative and 5-year score was above the MCID, indicating that the use of this replacement is a reasonable treatment of ESAA.12,17,18 These results were consistent across all time points, indicating a promising midterm prognosis if a patient is doing well 1 or 2 years after surgery. For patients contemplating undergoing a lateral TAA, this information can be useful when discussing postoperative expectations and for shared decision-making.
This implant demonstrated a good 5-year survivorship of 92.1% in this study, which is in accordance with findings from previous short-term studies on the trabecular metal implant.15,16,19,20 Only one other minimum-5-year study that has been conducted by Tiusanen et al 8 reported an implant removal rate of 2.9%, indicating excellent implant survivorship. The consistently high survivorship rate found in the literature suggest that the use of the trabecular metal and curved designed tibia may aid in the osteointegration process of the prosthesis.
In fixed-bearing implants, a stable bone-implant interface is necessary because there can be difficulty in perfecting rotational alignment when inserting the implant, and there will most likely be shear forces when loading the ankle postoperatively as the prosthesis seeks congruity. It is possible that the use of trabecular metal in the prosthesis allows the stable interface and bony ingrowth to occur; however, there are scant data on the use of trabecular metal in TAA as this is the first ankle prosthesis to use this material. Studies investigating the use of trabecular metal in total knee replacement have found low rates of aseptic loosening and solid fixation despite early migration of the implant at both 2 and 5 years postoperatively.21,22 In addition, a retrospective study by Girerd et al 23 on the use of trabecular metal tantalum cones in 51 revision total knee arthroplasties demonstrated radiographic osteointegration of all cones. These findings, combined with our survivorship for the trabecular metal TAA, suggest a faster and more solid osteointegration process for this material, which may explain our outcomes.
While our good survivorship outcomes support that the properties of trabecular metal may allow for solid osteointegration, periprosthetic cysts did develop in 6 patients. Due to the small number of patients who underwent 5-year radiographic follow-up, the exact percentage of periprosthetic cyst development at 5 years for the entire study population could not be determined. However, a short-term to midterm follow-up study by Kormi et al 15 found a low osteolysis rate of 10% with this trabecular metal TAA system, which is actually much lower than those reported in midterm studies of other implants such as the Salto Talaris (21.2%) and INBONE II (18.2%).1,4 The lower rate of cyst formation for the trabecular metal implant supports the idea that the use of this material may benefit overall osteointegration of the prosthesis, as previously discussed. However, the use of trabecular metal and a curved tibia still did not completely prevent cyst formation, demonstrating that the problem of osteolysis is still one that needs to be further addressed in future implant designs.
Notably, there was a significant reoperation rate of 23.7% in this study, most commonly for medial gutter impingement. There is concern that the lateral approach is the main cause of this complication as there can be difficulty addressing the medial gutter during the index TAA. However, when performing the reoperation through an anterior approach, the medial gutter was able to be thoroughly debrided, and there was resolution of symptoms in all cases. The combination of low rates of implant removal and osteolysis, along with the high incidence of medial gutter impingement for this implant, introduces an interesting discussion on the trade-off between these complications. While a lateral approach may improve implant survival and osteointegration, surgeons may encounter a higher rate of medial gutter impingement, possibly requiring the consideration of prophylactic gutter resection.
This study has several limitations. One of the most significant limitations of the study was the number of patients who responded to the annual patient-reported outcome survey, which can be explained by the fact that some patients lost interest in participating in the research survey and that only 21 of 38 patients had final radiographs. However, this study includes 5-year survivorship and reoperation rates obtained from all individuals treated with trabecular metal TAA during the study period. Another limitation is this does represent the initial series using this procedure for the surgeons involved. A third limitation is that the surgeons did not use the manufacturer-recommended surgical technique by not exposing the medial gutter with an anteromedial approach and had issues, as others have reported, with medial gutter impingement. A fourth limitation with interpreting this series is the types and rates of concomitant procedures are different from those reported by others. This series had a relatively high rate of medial displacement calcaneal osteotomies and medial malleolar prophylactic fixation. Finally, due to the relatively small number of patients and the lack of radiographic follow-up in all patients, we were unable to analyze the factors associated with implant failure, reoperations, and cyst development. Because previous research has demonstrated a correlation between the postoperative alignment and the medial or lateral location of periprosthetic cyst formation in TAAs with standard flat cut tibial implants, 24 it would be of great value to determine if a similar correlation exists in this curved tibia trabecular metal TAA system in future studies.
Conclusion
This study of the 5-year follow-up after lateral trabecular metal TAAs describes a survivorship of 92.1% with a reoperation rate of 23.7% and 1 case of amputation (2.6%). There were excellent clinical outcomes, with improvements in patient-reported outcomes that exceeded the MCID in all domains. This study is the second to report on the 5-year outcome of this implant and supports its use, recognizing the possible benefits of good implant fixation and osteointegration while acknowledging the drawbacks of increased rates of medial gutter impingement.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Scott Ellis reports receiving consulting fees from Stryker/Wright Medical, Paragon 28, and Vilex; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Stryker/Wright Medical and Paragon 28; participation on the Data Safety Monitoring Board or Advisory Board of Stryker/Wright Medical; having a leadership or fiduciary role in other board, society, committee, or advocacy group, paid or unpaid—other financial or nonfinancial interests: Wright Medical Technology provides research support. Constantine Demetracopoulos reports receiving royalties or licenses from Exactech; consulting fees from Exactech, RTI, Medshape, and In2Bones; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing, or educational events from Exactech—speakers bureau. Jonathan Deland reports receiving royalties or licenses from Zimmer Biomet and Arthrex; consulting fees from Zimmer Biomet and Arthrex; and has patents planned, issued, or pending with Zimmer Biomet, Arthrex, and Lima—not yet on market; has stock or stock options in Wright Medical; and other financial or nonfinancial interests in Lima Corporate—unpaid consultant. Carolyn Sofka reports receiving royalties or licenses from Lippincott Williams & Wilkins and consulting fees from OSSIO Ltd. All other authors declare no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Foot and Ankle Registry Steering Committee of the authors’ institution (IRB #2013-038).
Informed Consent
Written informed consent was obtained from all subjects of this study.
Trial Registration
Not applicable, because this article does not contain any clinical trials.