
Abstract
Hallux valgus is a common progressive forefoot deformity. Although open techniques have shown good outcomes, no technique has been shown to be superior to other techniques. The current third generation of minimally invasive Chevron–Akin (MICA) technique features a percutaneous procedure with a stable internal fixation. The technique used in this study resulted in stable internal fixation; however, 1 screw was used in intramedullary fashion in the majority of cases. The purpose of this study is to review the early outcomes of MICA. Electronic Health Records (EHR) were queried for patients who underwent MICA to treat hallux valgus (HV) deformity, by a single surgeon. The primary clinical outcomes assessed were visual analog pain score (VAS), rate of revision surgery, and recurrence. Radiographic outcomes were assessed including pre and postoperative hallux valgus angle (HVA), intermetatarsal angle (IMA), and bony foot width. The secondary outcomes included postoperative complications. A total of 91 feet underwent MICA to correct symptomatic HV deformity. The mean age of this cohort was 53.63 ± 15.42 years, mean body mass index (BMI) of 26.81 ± 6.21 kg/m2, mean follow-up of 6.33 ± 6.39 months and 87 feet belonged to female patients. Patients showed significant improvement in VAS and radiographic outcomes at final follow-up, with a mean improvement of 10.70° ± 6.42°, 2.39° ± 3.55°, and 5.30 mm ± 4.23 mm for the HVA, IMA, and bony foot width, respectively. Two patients (2.2%) required revision surgery for nonunion and removal of symptomatic hardware. One patient had a second metatarsal fracture treated nonoperatively. No feet had recurrence, hardware loosening, infection, or scar hypersensitivity. The current study reported on early outcomes for MICA. This technique appears to be effective and safe with no failure of fixation in our patients. We showed in our short-term follow-up, MICA led to significant improvement in pain and radiographic scores.
“MICA osteotomy led to significant clinical and radiographic improvements at short term.”
Introduction
Hallux valgus (HV) is a common progressive forefoot deformity that can become painful and may result in an associated lesser toes abnormality. A trial of conservative approach can be used in symptomatic patients. If this approach does not alleviate symptoms, surgical correction is indicated. Although traditional open techniques have shown good outcomes, no technique has been shown to be superior and 15% of patients have procedure-related complications 1 including pain, stiffness, and slow recovery.
Minimally invasive techniques have been found to result in smaller scars, quicker recovery, and greater postoperative range of motion. 2 Minimally invasive (MIS) percutaneous hallux valgus techniques have progressed over multiple generations. The current third generation of hallux valgus minimally invasive Chevron–Akin (MICA) technique developed by Vernois and Redfern 3 features a percutaneous osteotomy (Chevron–Akin) with a stable internal fixation.
The purpose of this study is to report the early outcomes of MIS Chevron–Akin osteotomy for symptomatic hallux valgus deformity performed by a single surgeon.
Methods
This is a retrospective study of consecutive patients who underwent a minimally invasive Chevron–Akin procedure to treat symptomatic hallux valgus deformity between July 2018 and June 2021. Institutional review board (IRB) approval was obtained for this study. All surgeries were performed by a single fellowship-trained foot and ankle orthopedic surgeon at a single academic institution. Exclusion criteria included patients younger than 18 years old, previous hallux valgus and/or bunionectomy surgery, congenital deformities, and peripheral neuropathy.
A chart review was performed to collect patient demographics including age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) classification score, tobacco use, diabetes mellitus, other comorbidities, surgical details, and associated lesser toes deformities. The ASA score is an assessment of patient’s overall preoperative health based on five classes (I–V). The primary outcomes included visual analog pain score (VAS), rate of revision surgery, and recurrence/loss or failure of correction.
Radiographic outcomes, assessed on weightbearing anteroposterior foot radiograph, included pre- and postoperative hallux valgus angle (HVA), intermetatarsal angle (IMA), and bony foot width. The measurements were performed by two of the authors on two separate occasions on digital films.
The HVA was the angle between a line drawn down the long axis of the first metatarsal shaft and another line drawn along the hallux proximal phalangeal shaft. The IMA was the angle between a line drawn down the long axis of the first metatarsal shaft and another line down the long axis of the second metatarsal shaft. Bony foot width was the distance measured between the most medial point of the first metatarsal head and the most lateral point of the fifth metatarsal head.
The secondary outcomes included postoperative complications: infection, scar hypersensitivity, hardware irritation, malunion, nonunion, loss of correction, hardware loosening, removal of hardware, and metatarsal fracture.
The severity of the hallux valgus deformity was defined as mild (HVA 15°-20° and/or IMA 9°-14°) in 28 feet (30.8%), moderate (HVA 20°-40° and/or IMA 14°-20°) in 62 feet (68.1%) and severe (HVA ≥40° and/or IMA ≥20°) in 1 (1.1%).
Surgical Technique
The patient is placed on the surgical table with the feet at the end of the table. An ankle Esmarch tourniquet, a mini-C arm and lead gloves are used. Prior to performing the osteotomy, the guide pin for the cannulated screw is inserted from proximal (the base of the first metatarsal) to distal (just proximal to the osteotomy site). Anteroposterior (AP) and lateral fluoroscopic views are obtained to confirm that the starting point avoided the first tarsometatarsal joint. This is an intramedullary pin; hence, it should not pierce the far cortex. It has to aim slightly lateral on the AP view and to be central on the lateral view. Then, the chevron osteotomy is performed as described by Vernois and Redfern. The osteotomy level is, determined on fluoroscopy, at the flare of the metatarsal neck.
A Shannon burr 20 × 2.2 mm (Novastep®) is used. The burr should be directed distally and plantarly (10° in both planes) to avoid shortening. The starting point is central on the sagittal plane and the burr is passed from medial to lateral cortex followed by the plantar then the dorsal cut. Once the chevron osteotomy is completed, the lateral head translation is performed. A reduction probe is introduced into the proximal shaft segment. The surgeon, with one hand, maintains the head well aligned in the sagittal plane, while the probe is used to push the head laterally with their other hand. The toe pronation is corrected then the guide pin is advanced into the metatarsal head. The guide pin is measured then over drilled, and a flanged head cannulated screw (Novastep®) is inserted while the surgeon maintains the reduction maneuver. The final position of the screw is confirmed on radiographs then the guide pin is removed. A lateral percutaneous soft tissue release is performed if necessary.
The correction is assessed, and a percutaneous Akin osteotomy is performed as needed. A guide pin is inserted from the medial base of the big toe proximal phalanx at a 45° angle aiming toward the lateral phalangeal cortex. The pin position is confirmed on AP and lateral fluoroscopic views. A 12 × 2 mm Shannon burr is used. The burr is introduced from medial dorsal and under fluoroscopy the wedge cut is completed. The lateral cortex is kept intact. The wedge is then closed manually and the guide pin is inserted through the lateral cortex, measured, advanced into the first webspace and temporarily held with a clamp. The osteotomy is fixed with 1 flanged head screw (Figure 1).

(A) Preoperative AP foot radiograph. (B and C) MICA Postoperative AP and lateral radiographs. Although in this case the medial prominence was not shaved, patient had no related symptoms postoperatively. It is recommended that this should be addressed at the time of surgery (D) AP radiograph at 9-months follow-up.
The 20 × 2.2 mm Shannon burr is used to remove the excess of bone at the proximal medial wall of the first metatarsal bone.
The portals are closed with silk sutures then a compressive soft dressing is applied and the patient is allowed to fully bear weight in a flat rigid postoperative shoe.
Statistics
All statistical analyses were performed using SPSS 24 (IBM Corp, Armonk, NY). Data are presented using the mean, standard deviation, and range for continuous variables and counts with percentages for categorical data. Wilcoxon Sign-Rank test and paired t-test were used to compare the means of continuous variables. The level of significance was set at 5% (P < .05).
Results
Patient Cohort
A total of 91 feet (80 patients) were included in the study with a mean follow-up of 6.3 ± 6.39 months. The median age was 53.63 ± 15.42 years (range 17-93), the mean body index (BMI) was 26.81 ± 6.21 kg/m2 (range 16.20-46.30), 23 (25.27%) patients met the definition of obesity (BMI > 30 kg/m2), the mean American Society of Anesthesiologists (ASA) score was 1.93 ± 0.55, and 87 (95.60%) of the included feet belonged to female patients. Forty-one patients had right foot hallux valgus correction and 38 had a left foot correction, whereas 11 had bilateral corrections.
Nine (8.9%) feet were performed without Akin osteotomy, 36 (39.5%) feet underwent concomitant lesser toe Weil osteotomy, and 17 (18.6%) underwent concomitant hammer toe(s) correction. Eighty-four (93.3%) feet had the chevron osteotomy fixed with 1 metatarsal screw (Table 1).
Clinical and Demographic Characteristics of the Studied Population.

Hallux valgus category: Mild (HVA 15°-<20° and/or IMA 9°-<14°); Moderate (HVA 20°-<40°, and/or IMA 14°-20°); Severe (HVA ≥ 40° and/or IMA ≥ 20°). The more severe of the 2 angles was used to represent the hallux valgus category.
Abbreviations: ASA, American Society of Anesthesiologists; HVA, hallux valgus angle; IMA, intermetatarsal angle.
Radiographic and Clinical Outcomes
The study group had a mean preoperative HVA of 22.05 ± 6.30 (range 3-40)°, a mean preoperative IMA of 11.51 ± 3.50 (range 4-21)°, and a bony foot width of 90.1 ± 5.60 (range 78-105.8) mm. These significantly improved postoperatively to a mean HVA of 11.35 ± 5.52 (range 0-29)°, a mean IMA of 9.12 ± 3.54 (range 2-16)°, and a mean bony foot width of 84.81 ± 6.15 (range 72-101.5) mm (P < .001).
The visual analogue scale (VAS) significantly improved from a preoperative value of 5.01 ± 1.83 (range 2 – 10) to a postoperative value of 1.36 ± 1.82 (range 0-8) (P <.001) (Table 2).
A Comparison of Pre and Postoperative Radiographic and Clinical Outcomes.
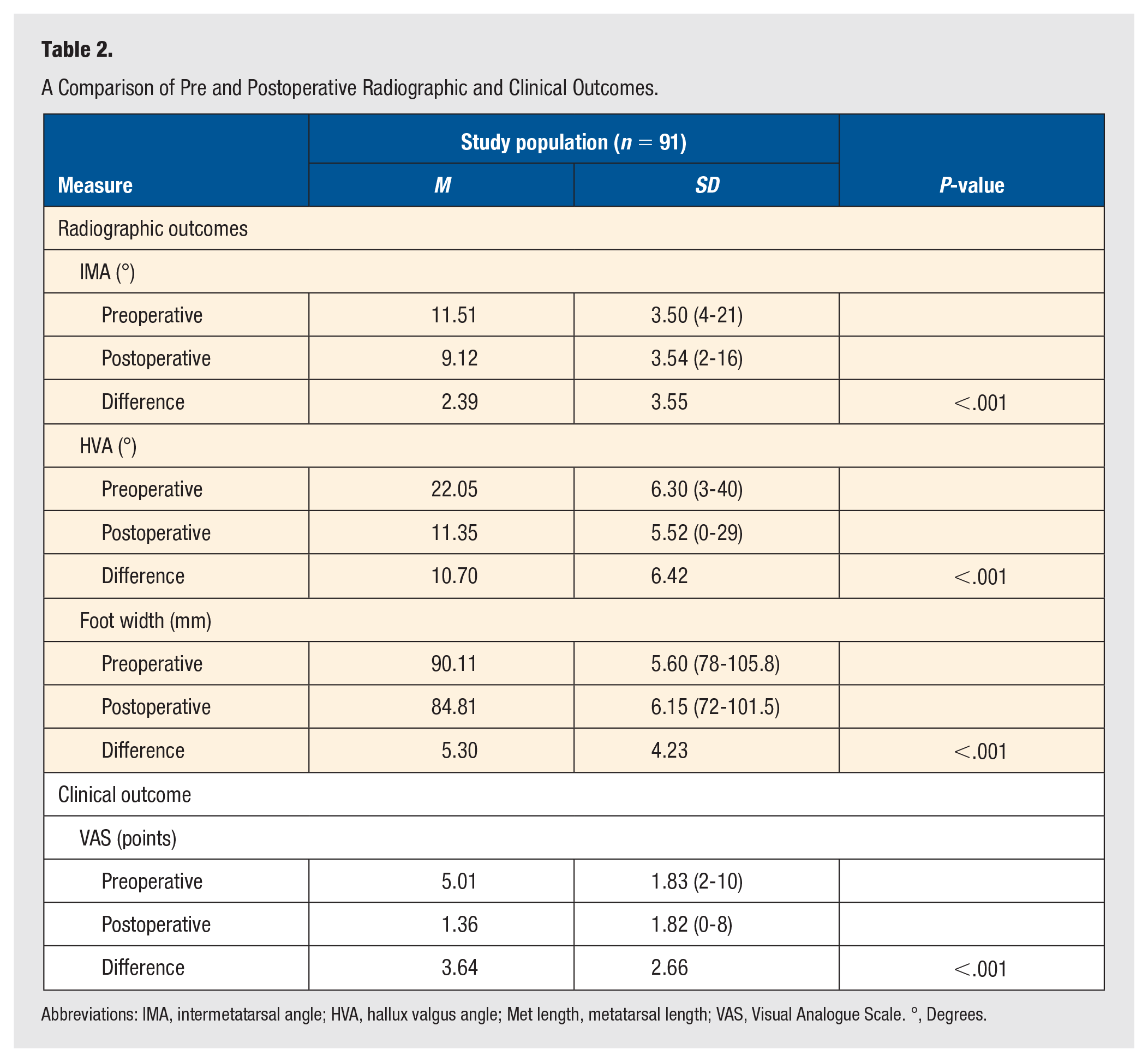
Abbreviations: IMA, intermetatarsal angle; HVA, hallux valgus angle; Met length, metatarsal length; VAS, Visual Analogue Scale. °, Degrees.
Complications
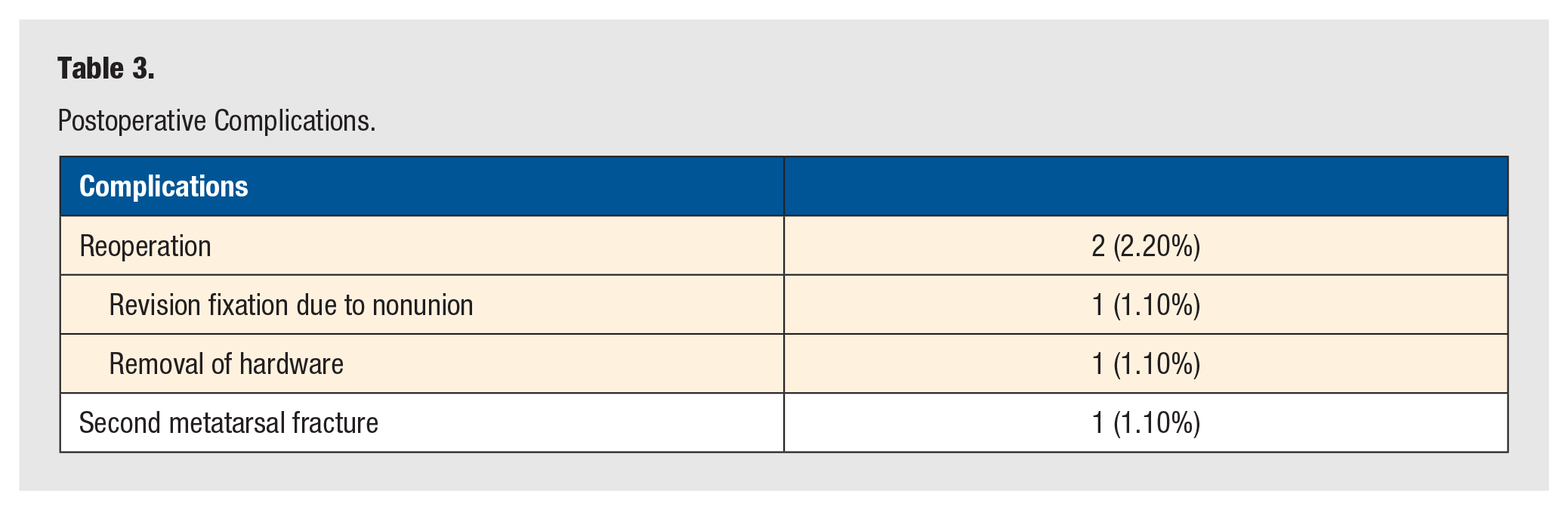
There were 2 reoperation (2.2%). One (1.1%) patient required hardware removal due to hardware irritation and 1 (1.1%) patient required a revision surgery due to metatarsal osteotomy symptomatic nonunion at 7 months postoperatively. The nonunion was observed in a 49 year old woman with mild hallux valgus deformity and no specific risk factors. One patient (1.1%) had a second metatarsal postoperative fracture that healed with conservative treatment and did not affect the recovery process. There were no cases of failure, recurrent deformity, hallux varus, infection, scar hypersensitivity, or hardware loosening (Table 3).
Postoperative Complications.
Discussion
The first surgical hallux valgus correction was done by Gernet in 1836. Reverdin in 1881 described a subcapital closing wedge osteotomy to correct the deformity. In the 1940s, early reports of percutaneous hallux valgus correction were published. Then, by the 1960s, early power equipment for minimally invasive osteotomy with intraoperative fluoroscopy were available for use. 4 The Reverdin technique revived by Isham 5 in 1991 is considered the first generation of percutaneous minimally invasive hallux valgus correction. It involved an intraarticular medial wedge closing osteotomy, oriented from dorsal distal to plantar proximal, an akin osteotomy and a percutaneous lateral release without internal fixation. The author reported, in a 5 year study, on 1000 cases with 90% excellent and 10% good outcomes. The second-generation MIS technique was described in 1993 by Bösch et al. 6 It involved a percutaneous hallux valgus distal osteotomy with a Kirshner wire fixation. Magnan et al, 7 in a review of 118 mild-to-moderate hallux valgus cases, at a mean follow-up of 35.9 months, reported 91% satisfaction rate and 2.5% recurrence rate. An oblique distal osteotomy was performed using a thin 2.23-mm micromotorized bone cutter. A 2-mm K-wire was inserted from distal, just medial to the metatarsal head, to proximal into the metatarsal shaft. All the radiographic parameters significantly improved postoperatively.
Kadakia et al 8 reported, in a review of 13 patients with hallux valgus treated by a percutaneous metatarsal shaft osteotomy, a dorsally angulated alignment in 9 patients (69%). However, the authors used a mini-incision approach, a saw for the osteotomy and 2 Kirschner wires capturing the metatarsal head and shaft for fixation.
The current third-generation MIS technique was developed by Vernois and Redfern. 9 It is a technique that combined stable internal fixation used in the scarf osteotomy and the principles of the minimally invasive technique. The authors found, in a review of 341 patients treated with percutaneous chevron osteotomy (Akin osteotomy was performed in 90% of the cases), a satisfaction rate of 95% (good/excellent results), with 7 patients required secondary surgery for recurrence due to failed primary fixation. The radiographic parameters significantly improved. The mean IMA was 14.5° preoperatively and 5.5° at last follow-up. The mean HVA was 33.7° preoperatively and 7.3° at the last follow-up.
The present study showed that minimally invasive Chevron–Akin osteotomy for a symptomatic hallux valgus deformity leads to significant improvement in clinical and radiographic outcomes at 6 months follow-up. The mean preoperative HVA and IMA improved from 22.05° and 11.51° to 11.35° and 9.12°, respectively. The mean preoperative bony foot width improved from 90.1 to 84.8 mm postoperatively. In our technique, 2 main modifications to be highlighted. First, the use of an intramedullary (without breaching the first metatarsal lateral cortex) screw in all cases. The thought here was to avoid any soft tissue complications in the first webspace with any lateral cortex screw prominence. Second, the use of a single screw in most cases as opposed to 2 screws in the traditional MICA technique. We felt that we could achieve adequate and stable fixation with this technique.
Other outcome studies on minimally invasive hallux valgus surgery reported similar results.10 -12 Lee et al compared third-generation percutaneous Chevron–Akin osteotomy to open scarf osteotomy, 25 patients were included in each group. HVA and IMA significantly improved from 31° to 7.6° and 15.6° to 6.4°, respectively, in the minimally invasive group. No major complication was reported, and 6 patients required hardware removal. The radiographic and clinical outcomes were comparable to those in the SCARF osteotomy group. 1 Holme et al, 13 in review of 40 patients treated with third-generation MICA for hallux valgus, found at 1-year follow-up improvement in HVA and IMA from preoperative values of 32° and 13° to 12° and 7° postoperatively, respectively. Lewis et al reported on a single surgeon two year follow-up of 292 cases third-generation MICA for a hallux valgus deformity. The authors found significant improvement in functional scores, however the radiographic follow-up was not routinely extended beyond 6 weeks. The overall complication rate was 21.3%—these were divided into three grades based on the severity and requirement of reoperation. The recurrence rate was 0.9% (3 cases) and some of the other reported complications included screw removal in 6.3% (21 cases), deep infection requiring washout in 1.2% (4 cases), flexor hallucis longus tendon injury in 1.5% (5 cases), transfer metatarsalgia in 0.9% (3 cases), and intraoperative conversion to open surgery in 0.6% (2 cases). 14 Mikhail et al 9 reported a total complication rate of 8.4% (23 cases) including 2 cases of nonunion (0.7%). In this study, we observed a low complication rate of 3.30% (3 cases). Complications included 1 hardware removal, 1 revision of nonunion, and 1 case of second metatarsal fracture successfully treated nonoperatively.
First metatarsal shortening is a concern with hallux valgus surgery; however, it remains unclear how much shortening leads to transfer metatarsalgia. Jung et al 15 showed, in a cadaveric study, that a first metatarsal shortening of 5 to 10 mm is necessary to cause an increased plantar pressure under the second and lesser metatarsals. Nakagawa et al 16 found an increased risk of transfer metatarsalgia when the first metatarsal is shortened more than 3 mm. Nishikawa et al 17 found, in a review of 29 patients with hallux valgus corrected with a Lapidus procedure, that first metatarsal shortening leads to decreased lower extremity functional scale.
The use of a Shannon burr to perform the subcapital osteotomy could lead to metatarsal shortening. The burr is of 2 mm diameter and will cut 2 to 2.5 mm of bone. This could be avoided by directing the tip of the burr in a 10° to 20° distally on the coronal plane and 10° planarly on the sagittal plane. If the metatarsal was lengthened, then the burr could be reintroduced to remove more bone. 18
The limitations of this study included the retrospective study design without a control group to compare our results to open hallux valgus surgery. Another limitation is the follow-up duration, we investigated the early outcomes of MICA; hence, a longer follow-up is needed to comment on long-term outcomes. The lack of calibrated radiographs for parameters measurement and not including a sesamoid position is also a limitation.
Conclusion
This study reported on early outcomes for MICA HV correction. This technique appears to be effective and safe with no failure of fixation in our patients. We showed in our short-term follow-up, MICA technique led to significant improvement in pain and radiographic scores. Future randomized trials with long-term follow-up are needed to validate the outcomes of minimally invasive techniques. Future randomized trials with long-term follow-up are needed to validate the outcomes of minimally invasive techniques.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.G.P. receives research support from Biomet, Integra, Pacira, and Zimmer; is a board or committee member for the American Orthopaedic Association, and American Orthopaedic Foot and Ankle Society; is a paid consultant for Additive Orthopaedic, Arthrex, Inc, Integra, Pacira, Solana, Sonoma Orthopedics, Stryker, and Wright Medical Technology, Inc.; is a paid presenter or speaker for Pacira; receives IP royalties from Arthrex, Inc, Integra, Orthohelix, and Solana; receives publishing royalties from Jaypee Publishers, SLACK Incorporated, and Wolters Kluwer Health—Lippincott Williams & Wilkins; receives financial or material support from Jaypee Publishers, SLACK Incorporated, and Wolters Kluwer Health—Lippincott Williams & Wilkins; and receives stock or stock options from Extremity Medical, Invuity, and Nextremity Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was not sought for the present study because all data collected was available in the public domain.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.