
Abstract
Objective
We sought to assess whether the presence of an os peroneum is correlated with cavovarus foot alignment in patients without a neurologic explanation for their foot shape. We hypothesized that a large os peroneum would increase the power of the peroneus longus and lead to a forefoot-driven, hindfoot varus deformity.
Materials and Methods
This was a retrospective cohort study conducted at a single institution and reviewed patients with 3 weightbearing views of the foot on plain radiography. Patients were characterized into having either no os peroneum (235), a small os peroneum (18), or a large os peroneum (23). The control group included the first 101 of the 235 patients without an os peroneum based on a power analysis of the primary outcome, which was the difference in the mean Meary’s angle (lateral talo-first metatarsal angle) between groups. The kite angle (anterior-posterior [AP] talocalcaneal angle), as well as 4 other angles were measured as secondary outcomes.
Results
Those with a large os peroneum had on a mean 7.7° (P < .01) more apex dorsal angulation of Meary’s angle than controls, and a kite angle 4.2° varus to that of the control group. There were no differences between the small os peroneum and control groups.
Conclusion
These findings add to the existing literature surrounding the etiology of cavovarus foot shape and link the presence of an ossified os peroneum, an oftentimes incidental radiographic finding, to cavovarus foot deformity in those without an underlying neurologic diagnosis.
Levels of Evidence:
Therapeutic, Level III: Retrospective Case-Control
Introduction
Cavovarus foot shape may cause a wide range of clinical conditions, such as osteoarthritis of the midfoot, subtalar joint, or ankle; lateral ankle joint instability; pathology of the peroneal tendons; plantar fasciitis; and foot pain. 1 It has been suggested that 62% to 75% of those with bilateral cavus foot deformity may be able to attribute this foot shape to some sort of neurological entity—including upper motor neuron disorders, peripheral nerve injury, or primary myopathies. However, cavovarus foot lacking a definitive neurologic diagnosis typically has their foot deformity labeled as idiopathic. 1
The os peroneum is an accessory ossicle of the foot typically located at the level of the calcaneocuboid joint within the peroneus longus tendon present in 5% to 26% of the population. 2 When large or fractured, this may lead to tendinosis or tenosynovitis of the peroneus longus tendon. 3 In addition, Taniguchi et al 4 noted the association between peroneal tendon tears and a cavovarus foot. To explain these findings, we hypothesize that a large os peroneum increases the power of the peroneus longus. Given its attachment at the base of the first metatarsal, this may lead to a forefoot-driven, hindfoot varus deformity. The association between an os peroneum and the cavovarus foot has yet to be characterized in the literature.
With this study, we aim to add to the literature surrounding idiopathic cavovarus foot deformity by evaluating whether the presence of a radiographically evident os peroneum is associated with the development of cavovarus foot shape.
Materials and Methods
Study Design and Participants
After institutional review board approval, we retrospectively identified eligible patients via a CPT (current procedural terminology) code search (73630) at our institution to find patients who had an outpatient clinic visit involving 3 weightbearing radiographs of the foot within the last 10 years at our institution. Patients were chosen in random series, from multiple different clinic locations as to increase generalizability. Patients 18 and older were included in this study. Exclusion criteria included prior surgery intended to address any underlying foot deformity, any hardware obscuring the view making it difficult to measure the foot, patients with Charcot arthropathy, Charcot-Marie-Tooth disease or other noted neurologic disorder, rheumatoid arthritis, or any amputation of the digits.
Study Procedures
The oblique view was used to characterize the presence or absence of an os peroneum, which is most apparent (if present) on this view. The length and width of the os peroneum were measured using this oblique view. The lateral view was then used to measure the depth of the os peroneum. The length, width, and depth were multiplied to give an estimate of the volume of the os peroneum. If the os peroneum was bipartite or multipartite, the sum of the parts was reported as the volume.
When the necessary number of patients in the control group was reached (101), subsequently, only those radiographs with an os peroneum were measured. So, though 276 radiographs were reviewed in total to amass a study cohort of 23 patients (23/276, 8.3%) with a large os peroneum, not all of the reviewed radiographs were included in study. The overall proportion of a radiographically evident os peroneum was 41/276 (14.9%).
Six angles were measured using the same protocol outlined by Taniguchi et al, 4 which was used as the reference standard for this study. Classification of cavus feet is not universal, but Meary’s angle (the angle drawn between the axes of the first metatarsal and that of the talus) is one common method.1,5,6 An angle that is 5 degrees or greater apex dorsal has been cited in the literature to signify a cavus foot deformity. 1 The angle created between the axes of the talus and the calcaneus on the anterior-posterior (AP) radiograph (the AP talocalcaneal or “kite angle”) has previously been used to appreciate hindfoot varus. An angle less than 25 degrees has been cited to signify a varus foot deformity. 1 These 2 angles have historically been used to measure cavovarus. 7 Based on more recent literature attempting to quantify cavovarus foot deformity, 4 other angles may give insight into the shape of a foot radiographically: the calcaneal pitch, the lateral talocalcaneal angle, 8 the AP talo-first metatarsal angle and the talonavicular coverage angle.4,9 An overview of these angles and their standard measurements was available to image interpreters before the study. 10 The protocol in Taniguchi et al used the 6 angles that were most appropriate for this analysis, and therefore, its protocol was used as a reference.
We used the lateral radiograph to measure 3 angles: the lateral talocalcaneal angle, the lateral talo-first metatarsal (Meary’s) angle, and the calcaneal pitch (Figure 1A, from Taniguchi et al 4 ). The AP radiograph was used to measure the talonavicular coverage angle, the AP talocalcaneal (kite) angle, and the AP talo-first metatarsal angle (Figures 1B and 1C, adopted from the work of Taniguchi et al 4 ).
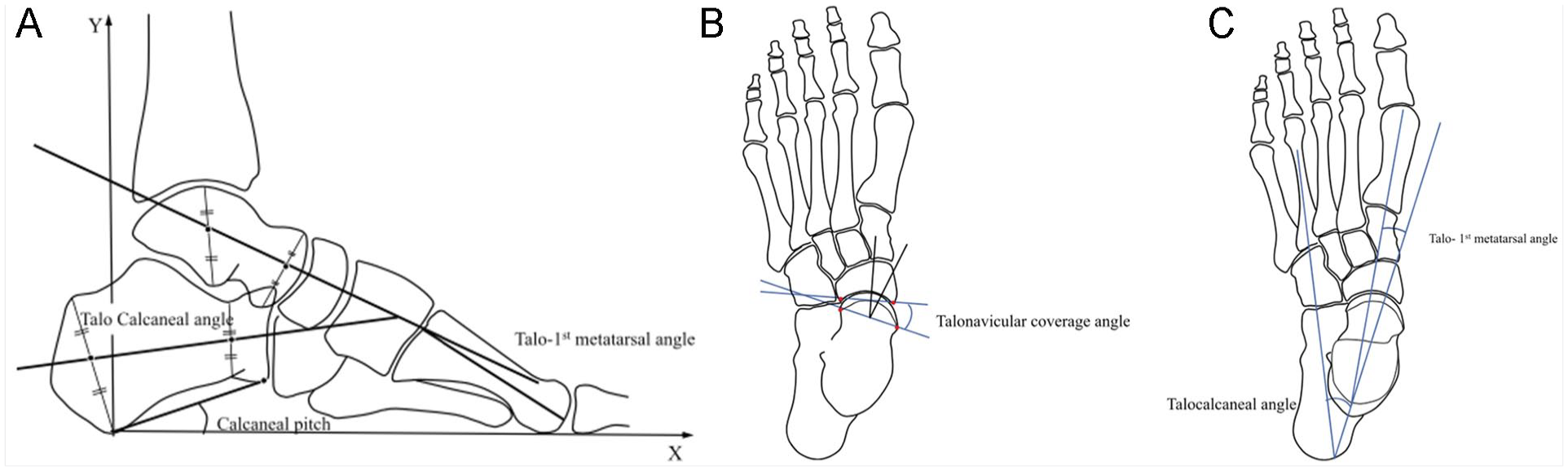
(A) Calcaneal pitch, talocalcaneal angle, and talo-first metatarsal angle measured on lateral radiographs. (B) Talonavicular coverage angle measured on an anteroposterior radiograph. (C) Talo-first metatarsal angle and talocalcaneal angle measured on anteroposterior radiographs.
Statistical Analyses
Categorical variables were summarized as counts and percentages and were compared between treatment groups using chi-square tests. Continuous data were described as mean values and standard deviations (SDs), and were compared between treatment groups using Student’s t test. We report both unadjusted and adjusted results. The adjusted results use a multivariate linear regression to control for patient-specific characteristics—body mass index (BMI), age, and sex. The results of the adjusted model are presented as beta values, which represent the number of degrees of difference of the small and large os peroneum groups as compared with the control group, and are reported with an associated 95% confidence interval (CI). All analyses were performed using R statistical software, version 3.5.3 (R Foundation for Statistical Computing, Vienna Austria).
Outcome Variables
The primary outcome was specified as Meary’s angle, based on prior research showing it as a reliable indicator of cavovarus deformity.1,5,6 Sample size was determined based on a power analysis of this outcome. It was determined that 23 patients in the treatment group and at least 100 in the control group were needed order to evidence a 4-degree difference between groups in Meary’s angle with α = 0.05. The secondary outcome was the other 5 angles measured.
A board-certified orthopaedic surgeon as well as an MD candidate with 4 years of musculoskeletal radiology experience were both involved in image interpretation.
Results
Patient Characteristics
Of the 142 included patients, 41 had an os peroneum and 101 did not; 100 mm3 was defined because it was the median measured value of volume for the sample population (first 20 patients measured). In the end, 18 had what was characterized as a small os peroneum (< 100 mm3), and 23 had a large os peroneum (> 100 mm3).
Baseline characteristics of these groups are included in Table 1. Overall, the patients were predominantly female (102/142, 72%). Those with a large os peroneum tended to be older (average age, 64 years) as compared with the both the small group (55 years) and the control group (49 years) (P < .01). There were not differences in sex or BMI between groups. The mean volume was 422 mm3 in the large group and 54 mm3 in the small group.
Demographics.
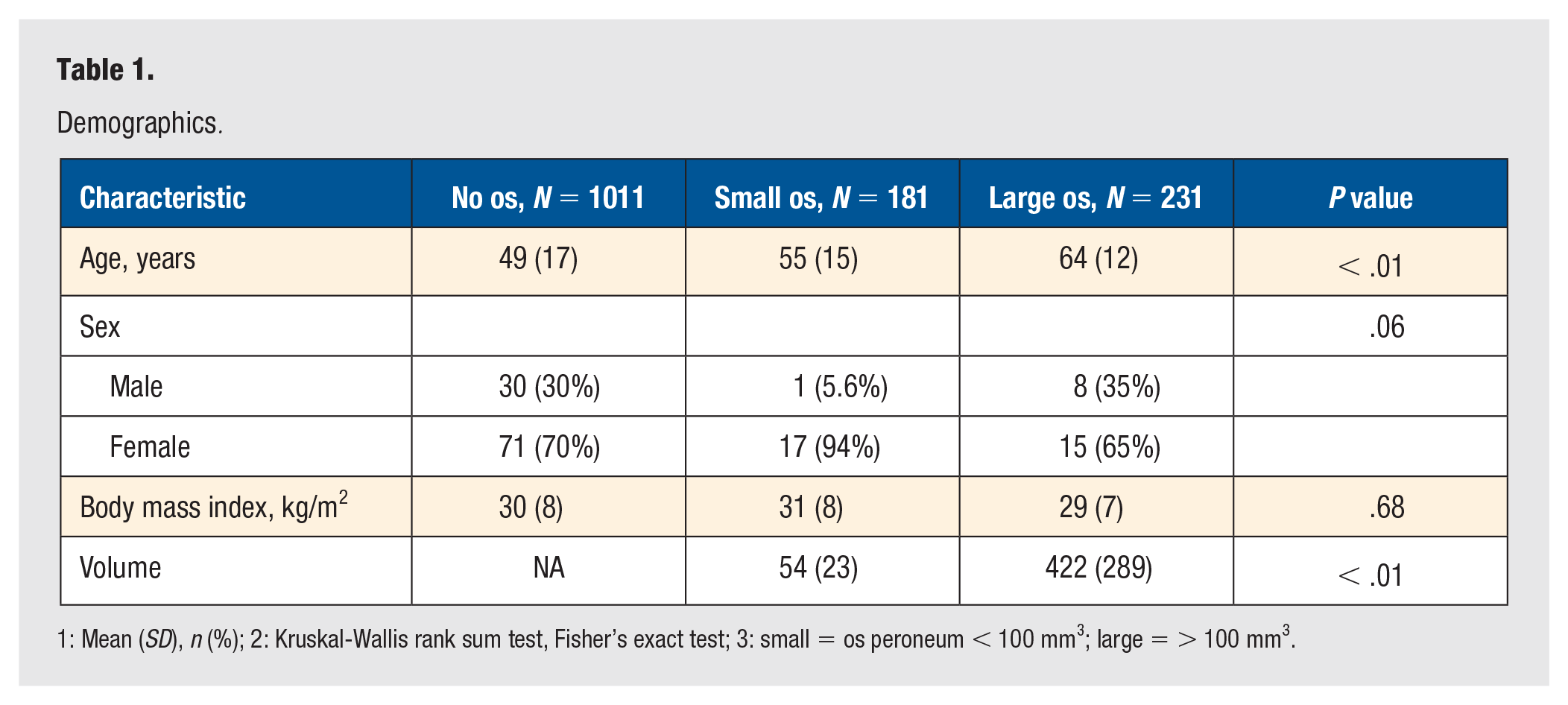
1: Mean (SD), n (%); 2: Kruskal-Wallis rank sum test, Fisher’s exact test; 3: small = os peroneum < 100 mm3; large = > 100 mm3.
Primary Outcome
Meary’s angle was significantly different between groups in the unadjusted analysis (P = .01) (Table 2). The large group showed a mean of −1° (SD = 7) as compared with the control group (−6°, SD = 8), with negative angles signifying apex plantar (planus). When a linear regression was used to adjust for differences in age, sex, and BMI, the large group was on average 7.7° more apex dorsal as compared with controls (95% CI = 4.0-11.4, P < .01) (Table 3).
Unadjusted Results.
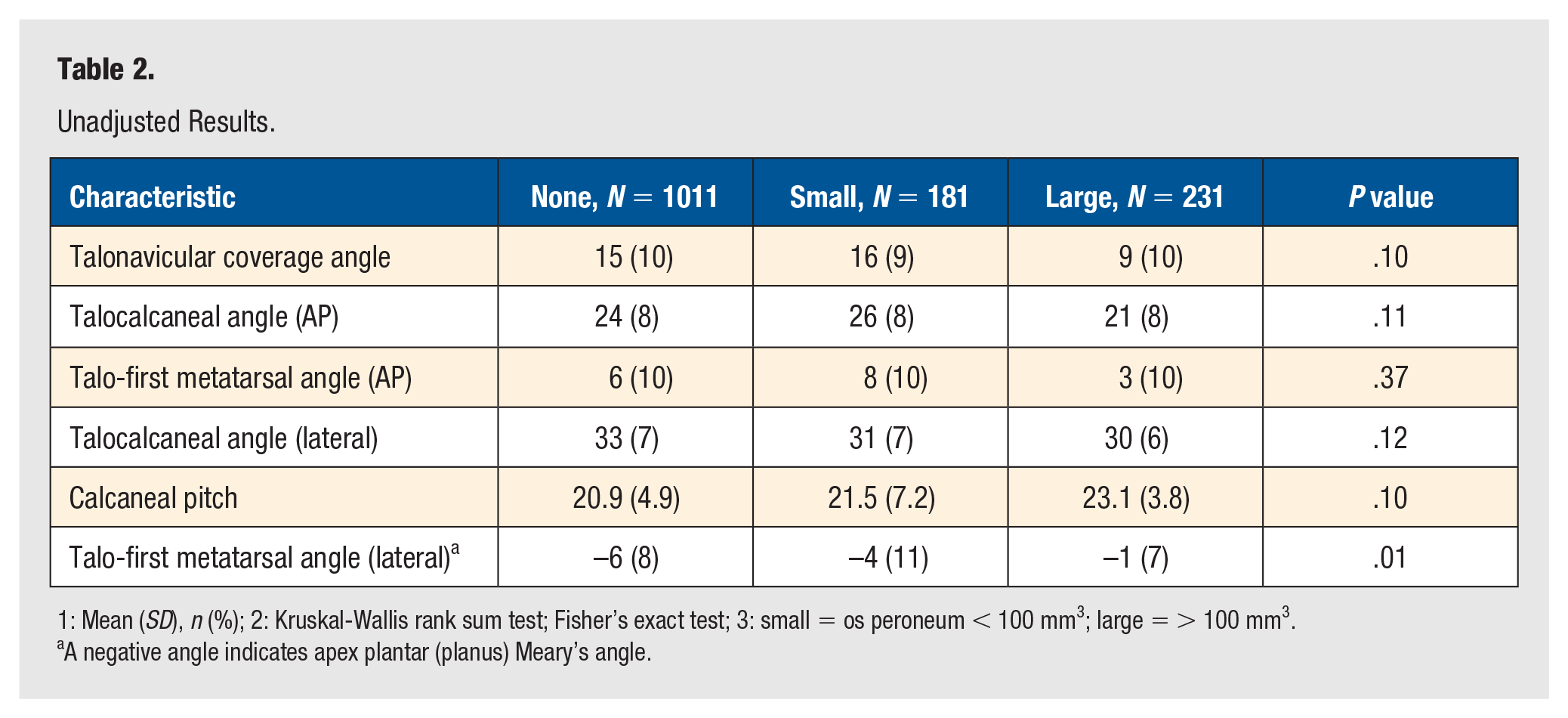
1: Mean (SD), n (%); 2: Kruskal-Wallis rank sum test; Fisher’s exact test; 3: small = os peroneum < 100 mm3; large = > 100 mm3.
A negative angle indicates apex plantar (planus) Meary’s angle.
Adjusted Results.
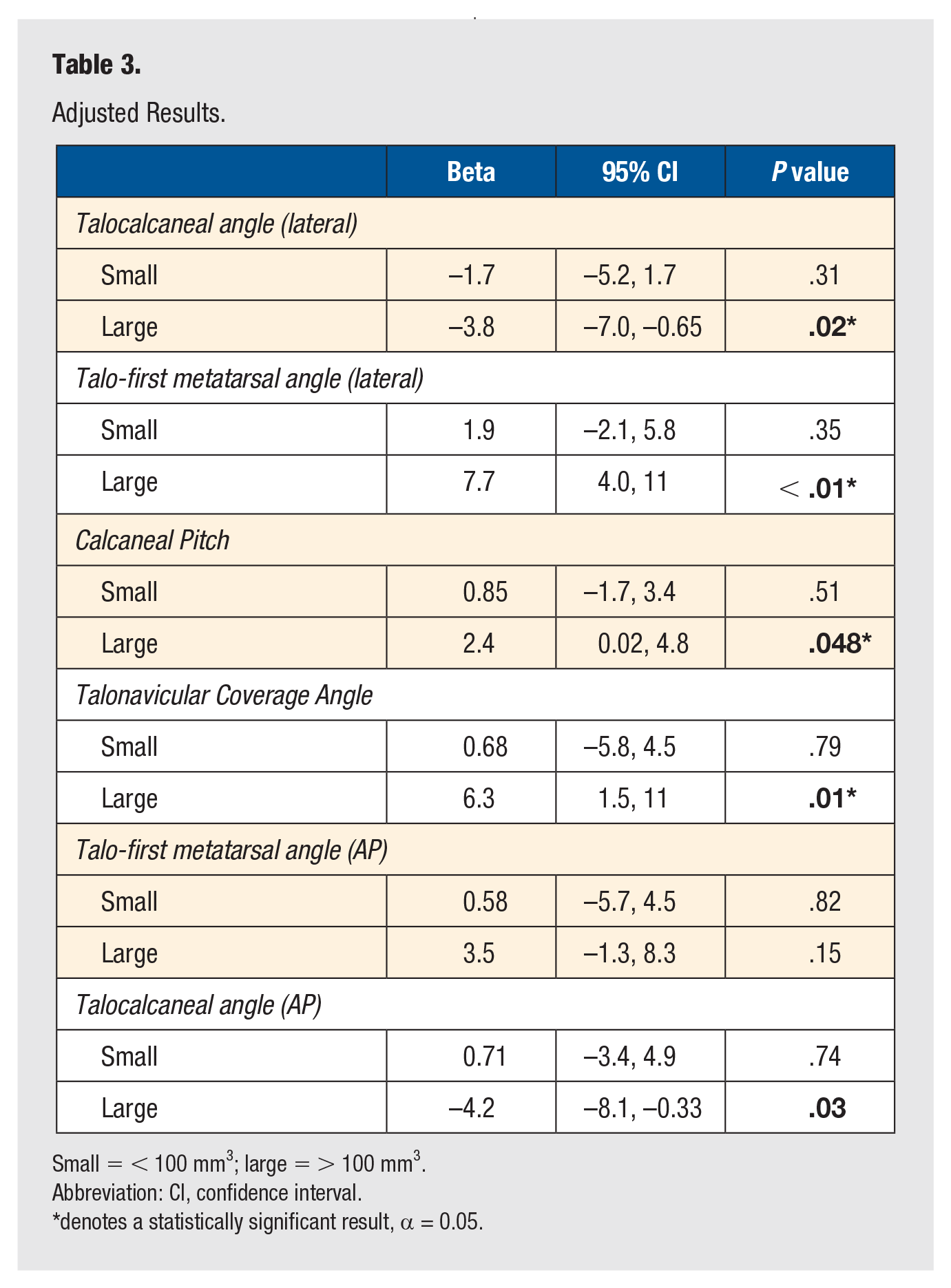
Small = < 100 mm3; large = > 100 mm3.
Abbreviation: CI, confidence interval.
denotes a statistically significant result, α = 0.05.
Secondary Outcomes
No secondary outcomes were significantly different between groups in the unadjusted analysis. However, after linear regression, on average, the lateral talocalcaneal angle was 3.8° less than controls (P = .02), and the calcaneal pitch was 2.4° greater than controls (P = .048). The talonavicular coverage angle was 6.3° greater than controls (P = .01), and the kite angle was 4.2° less than controls (P = .03). No difference was observed between groups in the AP talo-first metatarsal angle.
Discussion
We found that the foot with a large os peroneum (> 100 mm3) is more likely to be both cavus (Meary’s angle difference of 7.7°, P < .01, adjusted analysis) and varus (kite angle difference 4.2°, P = .03, adjusted analysis). It is also notable that an os peroneum < 100 mm3 does not predispose patients to developing a more cavovarus foot shape. Figure 2 shows the results of the unadjusted analysis, demonstrating the tendency of those with a large os peroneum to have a cavovarus foot shape. To our knowledge, this is the first study to show the association between an os peroneum and differences in foot shape.
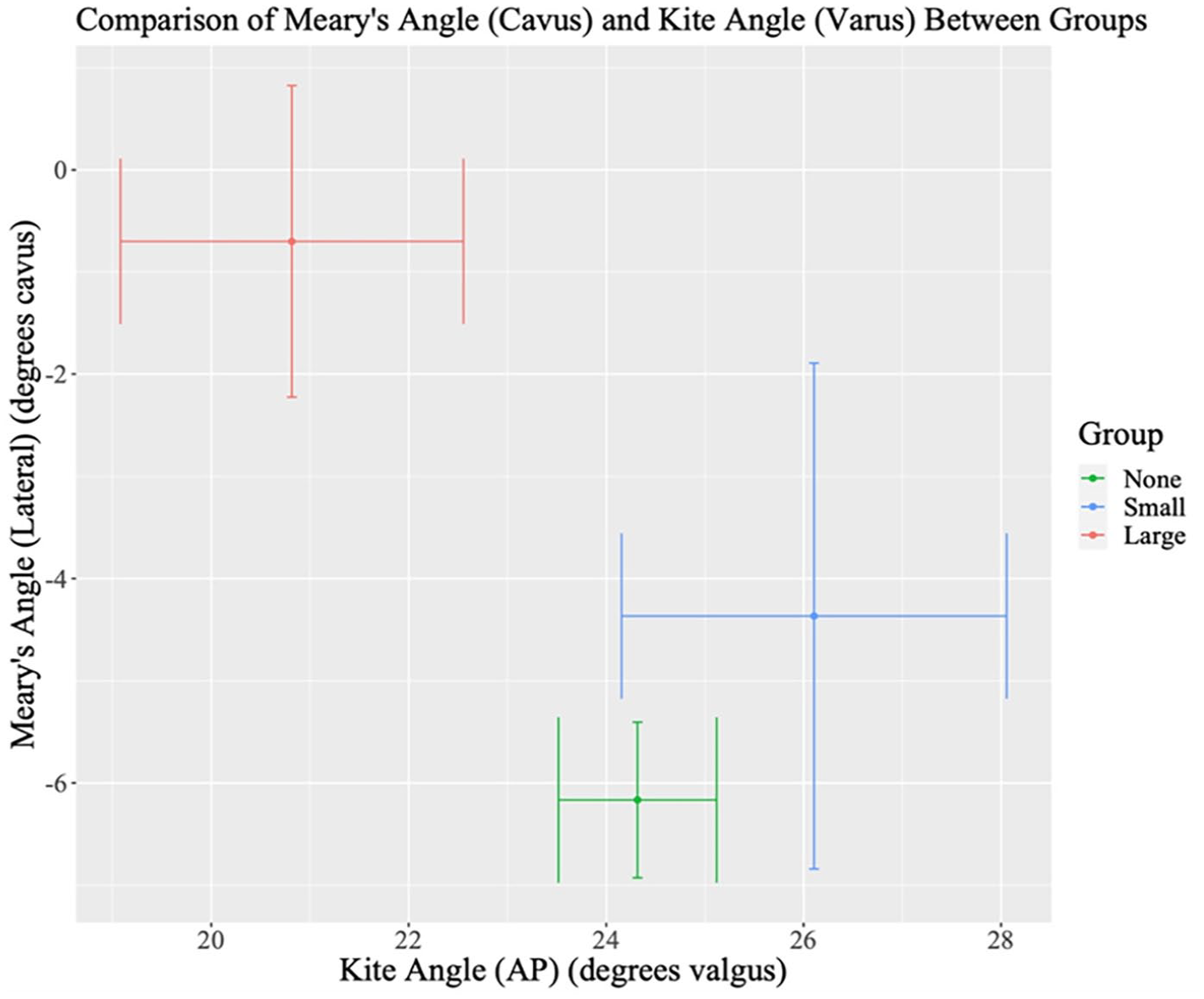
Cavus of the foot is represented as positive angles on the y-axis (mean Meary’s angle), and is compared with valgus alignment, represented as higher angles on the x-axis (mean kite angle).
Previously, the os peroneum has been demonstrated to be associated with peroneus longus tears, 3 and Sammarco et al 11 noted the relatively high incidence of an os peroneum in those with operatively treated peroneal longus tears (6/14, 43%). In addition, there are data to show an association between peroneal tendon tears and cavovarus foot shape. 4 Taniguchi et al found differences in the calcaneal pitch, as well as AP talo-first metatarsal and AP talonavicular coverage angles between the control group and those with peroneal tendon tears. Our study did not find a difference in the AP talo-first metatarsal angle between groups but does agree with the tendency of the study group to have a cavovarus foot, evidenced by significant differences in the other 5 measured angles.
This study brings into light the clinical relevance of a perhaps incidental radiographic finding. Previously, the os peroneum has been associated with lesions of the peroneal tendon. In addition, painful os peroneum syndrome (POPS) (with pain lateral to the cuboid in the context of an os peroneum) is a recognized clinical entity.2,12 However, even in the absence of pain or obvious lesion to the peroneal tendon, the os peroneum could have clinical significance in its contribution to a patient’s foot shape.
One additional finding was that the group with a large os peroneum was significantly older (mean, 64 years) than the control group (mean, 49 years) (P < .01), and could signify that the os peroneum tends to ossify with time, and therefore more likely to be radiographically evident in older patients. There is cadaveric evidence to support that all humans have some evidence of at least a fibrocartilaginous os peroneum, though only some have a bony component to this structure. 13
We acknowledge that “os peroneum” is somewhat of a misnomer, as it has been written in the literature that everyone has a histologically evident “os peroneum,” though most often, it is a band of fibrocartilage embedded within the tendon that never ossifies. Therefore, we must clarify that our study aims to determine whether specifically the ossification of this segment of tendon is associated with cavovarus foot deformity, and we do recognize that most believe that there are microscopic and macroscopic differences in this region of the tendon regardless of whether it is calcified and visible on radiographs or not.
In summary, these data might indicate that tendon strain from an ossified os peroneum could be a significant contributor to the development of cavovarus foot deformity. Another possible explanation is the reverse, in which the cavovarus foot may cause strain on the peroneus longus and in turn lead to more rapid ossification of the os peroneum. While an alternative hypothesis is that ossification of the os peroneum occurs as a response to degeneration or weakness of the tendon, these data argue against this—a weaker peroneus longus tendon would tend to leave the foot in planovalgus, rather than the tendency toward cavovarus we observed. Future study may make use of magnetic resonance imaging (MRI) or ultrasound to characterize any inflammation in the peroneal tendon that may be caused by a radiographically identified os peroneum—thereby assessing more directly the quantity of the strain on the peroneal tendon imposed by large os peroneum. In addition, quantifying the degree of patient symptomology based on the presence of both os peroneum and/or cavovarus foot deformity could help elucidate the clinical significance of this result.
Strengths and Limitations
There are several strengths to this study. First, a pre-study power analysis ensured that we included an adequate patient number. Also, the measurement of the volume of the os peroneum allowed us to see the differences between small and large os peroneums. A rigorous methodology that included measuring 6 angles per patient, and a linear regression analysis to control for factors, such as BMI, age, and sex helped to further delineate differences between groups. The margin of error in radiographic measurement is a limitation of this study. The intraobserver class coefficient was 0.93. Though this is an excellent score for the intraobserver reliability in the measurement of radiographs, it shows that there is still possibility of error that occurred in the measuring process. Error was attempted to be minimized using a previously documented, detailed measurement technique and involvement of a board-certified foot and ankle orthopaedic surgeon in the measuring process. Limitations include the significant difference in age between groups, which we attempted to control for in our linear regression analysis. Though, as in any retrospective analysis, residual confounding may exist. This was a single-institution study that used patients being seen for a variety of causes by multiple providers.
Implication
With this study, we add to the existing literature surrounding the etiology of cavovarus foot shape and provide a possible alternative explanation for cavovarus foot deformity in those with a radiographically identified large os peroneum without a known neurologic explanation for their foot shape.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from an ethics committee or institutional review board. IRB number 15972 from the Henry Ford Health System IRB.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.