
Abstract
Background
Surgeons rely on intraoperative fluoroscopy to assist in placement of implant components during total ankle arthroplasty (TAA). Parallax alters the direction of an object when viewed from two different points, resulting in image distortion. The purpose of this study was to evaluate parallax/distortion in intraoperative fluoroscopic images during TAA.
Methods
A retrospective review of all TAAs performed by two surgeons (R.W.M. and B.S.) from August 2019 to April 2023 were reviewed. Intraoperative fluoroscopic anteroposterior (AP) ankle views were evaluated for any obvious parallax image distortion. Cases with obvious parallax distortion were included for angular evaluation of AP intraoperative fluoroscopic and first postoperative plain films. The tibia was marked at 2-centimeter intervals to create zones from the proximal stem of the implant. The anatomical axis of the tibia (AAT) was drawn at the mid-diaphysis. The anatomic lateral distal tibial angle (aLDTA) and anatomic axis deviation (AAD) were measured for each zone.
Results
A total of 22 TAAs were performed during the study period. Four cases were excluded due to inadequate imaging, leaving a total of 18 TAAs for review. We found 6 of 18 (33.3%) cases had obvious parallax distortion. We found the average aLDTA was 90.9° (84°-101°). At the most proximal tibial zone, the average aLDTA was 94° (91°-101°). We found the average AAD was 4.7 (0.5-17.2) mm. The AAD ranged from 0.5 to 17.2 mm lateral to 0.8 to 8.2 mm medial. Postoperative plain film radiographs displayed a normal aLDTA and an AAT centered within the ankle joint.
Conclusion
Parallax can distort the appearance of the tibia on fluoroscopic images. Deviation from the normal aLDTA and anatomical axis should be anticipated. Surgeons should be aware of the potential impact of parallax and ways to mitigate these effects.
Keywords
“The apparent shift of anatomical landmarks caused by parallax/distortion can potentially result in angular deviation and linear displacements of implant components.”
Introduction
Arthritis at the ankle joint is a debilitating condition resulting in pain, limited mobility, and reduced quality of life. End-stage ankle arthritis can be difficult to treat. Compared to arthritis in the hip or knee, which are usually primary osteoarthritic processes, ankle arthritis is much more commonly posttraumatic. 1 After failing conservative measures, the two main surgical options include arthrodesis or total ankle arthroplasty (TAA). Traditionally, ankle arthrodesis has been the “gold standard” for surgical correction of ankle arthritis. However, newer-generation replacement devices have shown promising outcomes in treating end-stage ankle arthritis.
The first functional TAA was performed by Lord and Maroote in 1973. 2 Total joint replacement is an attractive option for treating ankle arthritis as it allows for a pain-free joint while maintaining motion. Although major advances in prosthetic design have allowed for significant improvement in survivorship of over 90% at 5 to 10 years,3,4 there remains a 19.7% overall risk of complications and a 7.9% risk of reoperation. 5 Multiple factors are involved in a successful outcome with TAA, including patient selection, prosthetic design, the severity of the deformity, soft-tissue balancing, bone stock, and surgical technique.
Errors in surgical technique can lead to malalignment of the prosthesis. A malpositioned prosthesis can lead to impingement, increased risk of subsidence, and component loosening. 6 One potential cause for prosthesis malalignment is inadequate fluoroscopic imaging of the tibial axis. 7 Although fluoroscopic utilization is an indispensable tool for surgeons, particularly when performing a TAA, it is important to recognize potential imaging distortion that can occur. Parallax is the apparent difference in direction of an object when visualized from two different points that are not in a straight line with the object. 8 Differences in parallax/distortion can be noted on comparison of intraoperative fluoroscopic images and postoperative plain film radiographs. The apparent shift of anatomical landmarks caused by parallax/distortion can potentially result in angular deviation and linear displacements of implant components.
Literature on total knee and total hip arthroplasties has emphasized the effects of parallax/distortion.9 -12 However, no literature has focused on the effect of parallax/distortion on TAAs. It is essential for surgeons to be aware of the parallax phenomenon and its potential implications in TAA surgery. Therefore, the purpose of this study was to evaluate the prevalence and degree of parallax/distortion in intraoperative fluoroscopic images during TAA.
Materials and Methods
A retrospective review of all TAAs performed by two surgeons (R.W.M. and B.S.) between August 2019 and April 2023 were reviewed. All surgeries were performed at a single institution (OhioHealth Grant Medical Center, Columbus, OH) from August 2019 to April 2023.
Two types of modern TAAs were utilized during the study period. Fixed-bearing implants were utilized, either with or without an intramedullary stem. Patients underwent either a TAA using the INBONE prosthesis (Wright Medical Technology, Arlington, TN) or the INFINITY prosthesis (Wright Medical Technology, Arlington, TN).
Patients were excluded if they were ≤18 years old, or if the intraoperative fluoroscopic images and/or first postoperative plain films were unable to be obtained for review. Cases that met the inclusion criteria were included for review. Intraoperative fluoroscopic images obtained on patients undergoing TAA were compared to the first-postoperative-visit plain films for any obvious parallax/distortion. We defined obvious parallax/distortion as any gross curvature or warping of anatomical structures on intraoperative images compared to plain films. Images were viewed on Synapse Enterprise Imaging (Fujifilm, Lexington, MA) and printed for analysis. Standard anteroposterior (AP) radiographic views were evaluated. If any obvious parallax/distortion was noted, angular measurements were performed for further evaluation (Figure 1).
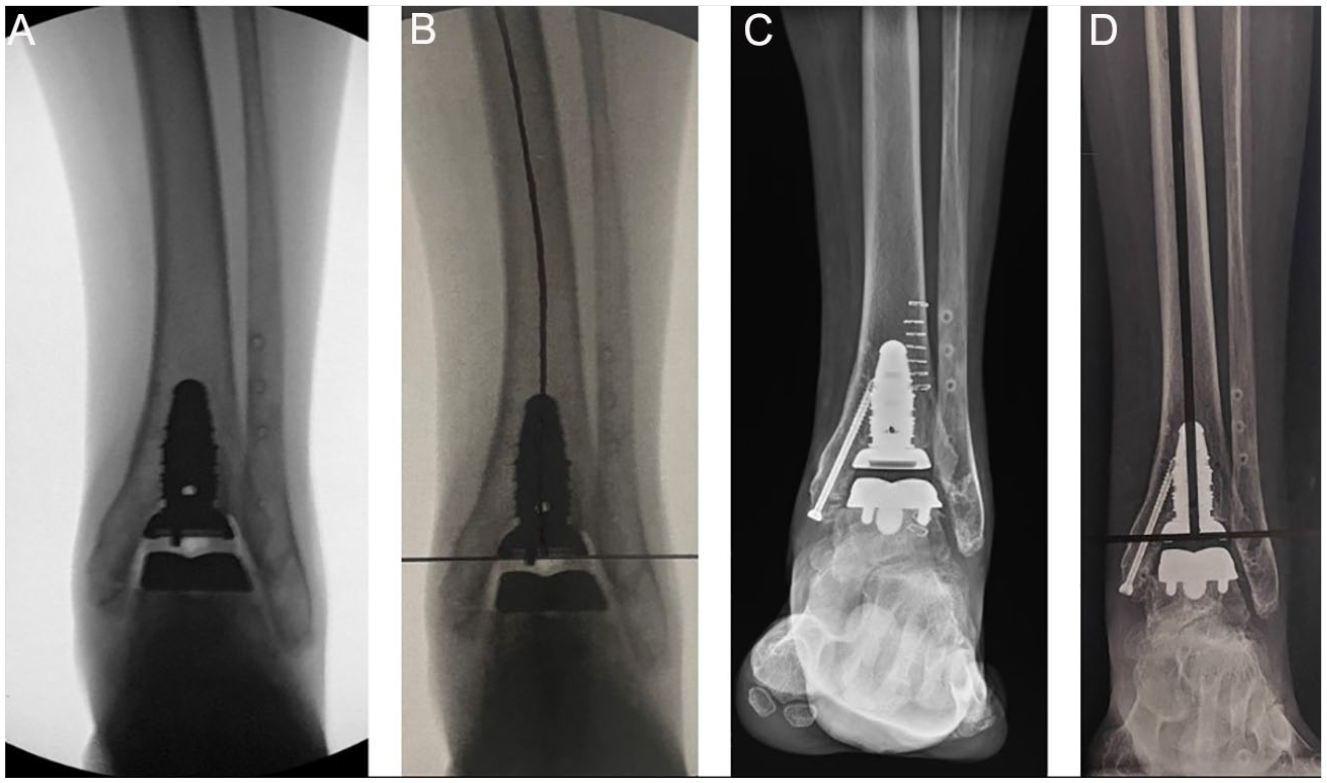
Radiographic images of “TAA 1.” (A) Intraoperative fluoroscopic anteroposterior image prior to medial malleolar fixation. (B) Printed version of the same fluoroscopic anteroposterior image with the mid-diaphysis of the tibia drawn for reference. Note the significant parallax/distortion appreciated at the proximal tibia. (C) Postoperative anteroposterior radiograph of the same patient. (D) Printed version of the same postoperative radiograph with the mid-diaphysis of the tibia drawn for reference. One can appreciate the lack of parallax/distortion of the tibia.
Intraoperative fluoroscopic images with obvious parallax/distortion, and the corresponding first postoperative plain film AP radiographic views, were imported into Photoshop 2024, version 25.4 (Adobe, San Jose, CA). Lines were drawn for the respective angles listed below and were measured utilizing the ruler tool. Measurements were performed by 2 investigators (R.G. and Z.P.H.). If there was discrepancy between measurements, a third investigator was utilized (J.R.B.). A horizontal line was drawn at the distal tibial tray to represent the distal tibial component. A red dot was placed at the center of this line to represent the center of the tibiotalar joint. The tibia was marked at 2-centimeter intervals from the proximal stem of the implant to create tibial zones. Tibial zones were labeled in sequential order from distal to proximal. The anatomical axis of the tibia (AAT) was drawn at the mid-diaphysis of each respective zone (Figure 2). The anatomic lateral distal tibial angle (aLDTA) and anatomic axis deviation (AAD) were measured for each segment. The aLDTA was measured as the angle between the AAT and the articular surface of the tibia, or tibial component. The AAD was measured as the amount of deviation, either medially or laterally, from the center of the tibiotalar joint (Tables 1 and 2).
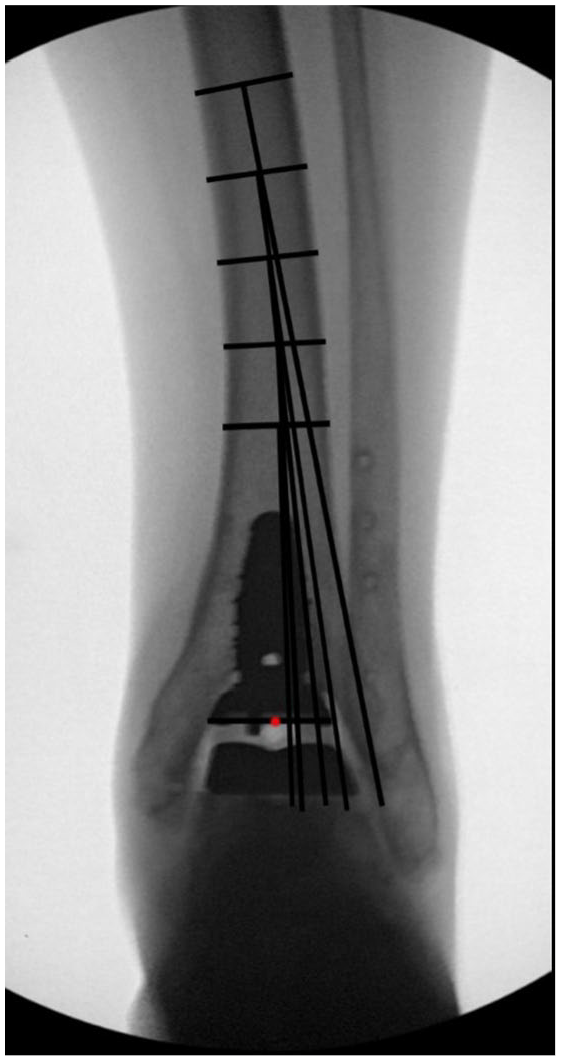
Intraoperative fluoroscopic anteroposterior image of “TAA 1.” Horizontal line at distal tibial component, with a red circle representing the center of the tibiotalar joint. Tibial zones were marked at 2-centimeter intervals, in sequential order from distal to proximal, from the proximal stem of the implant. The AAT was drawn at the mid-diaphysis of each zone. The aLDTA and AAD were measured from the AAT of each zone.
The aLDTA measured at each 2-centimeter zone from the proximal stem of the implant.
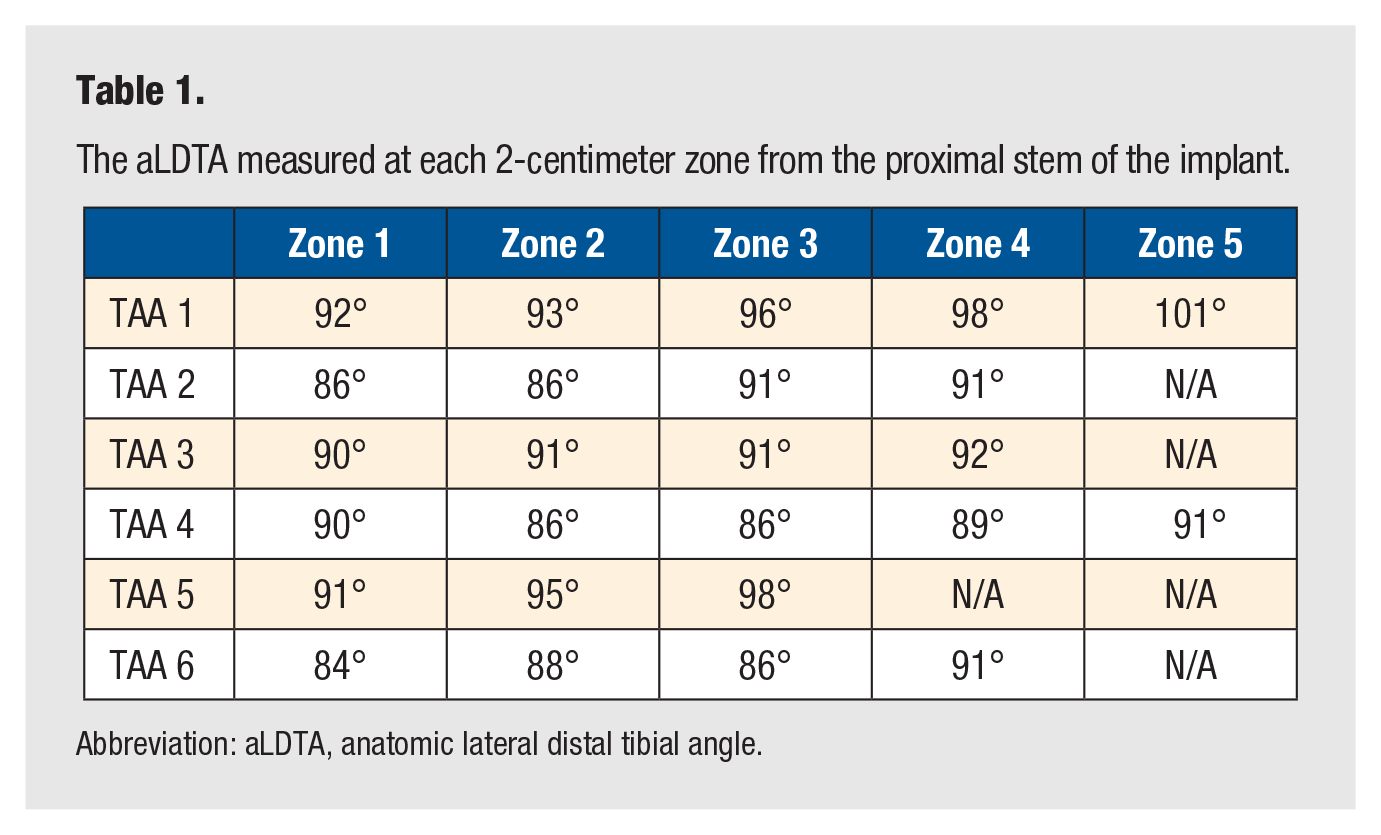
Abbreviation: aLDTA, anatomic lateral distal tibial angle.
The AAD at the tibiotalar joint measured at each 2-centimeter zone from the proximal stem of the implant.
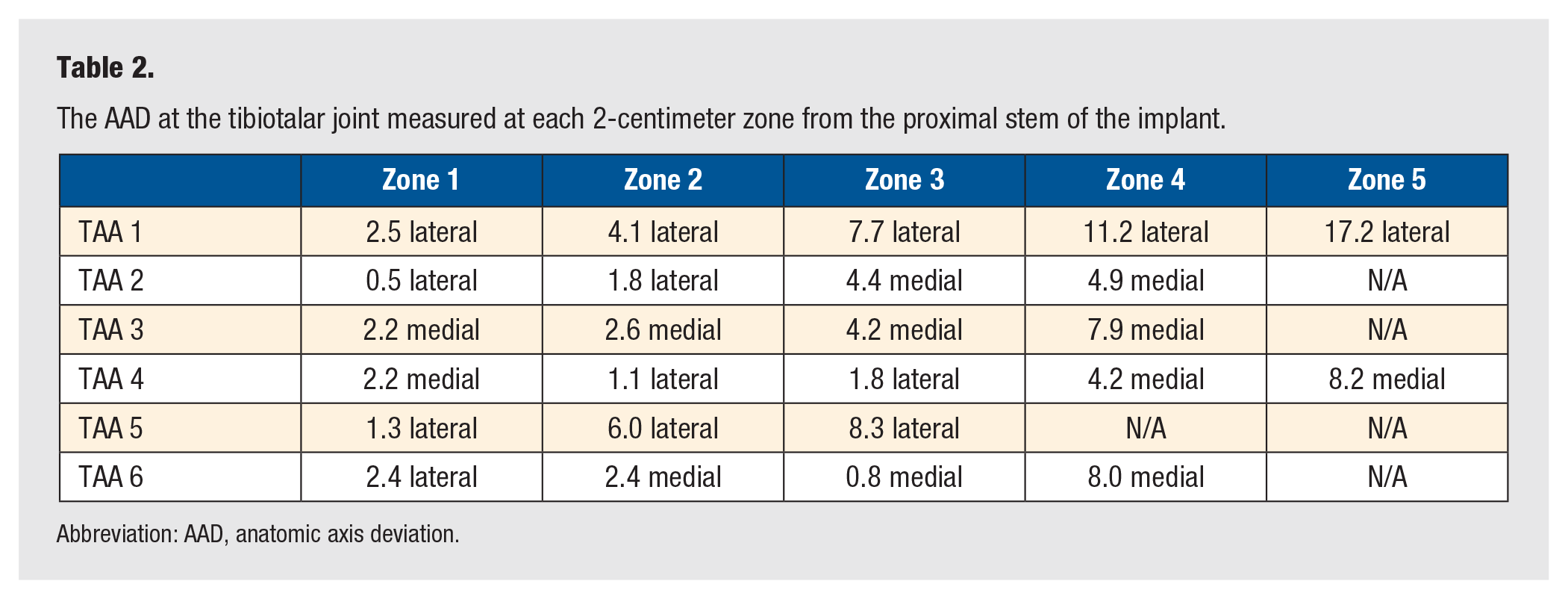
Abbreviation: AAD, anatomic axis deviation.
Results
A total of 22 TAAs were performed during the study period. There were 4 cases that were excluded due to inadequate intraoperative fluoroscopic images, leaving a total of 18 TAAs for review. While all TAA cases displayed parallax/distortion, we found that 6 of 18 (33.3%) cases had obvious parallax/distortion when compared to first postoperative plain film radiographs. Obvious parallax/distortion was defined as gross curvature or warping of anatomical structures on intraoperative fluoroscopic images as compared to postoperative plain film radiographs.
The normal aLDTA is 89° ± 3°. 13 Angular measurements obtained from intraoperative fluoroscopic images revealed an average aLDTA of 90.9° (ranging from 84° to 101°). Notably, the average aLDTA increased to 94° at the most proximally visualized tibial zone. The AAT should be centered within the tibiotalar joint. 14 We found a wide range of deviation from the center of the tibiotalar joint at the measured segments on intraoperative fluoroscopic images, with an average AAD of 4.7 (0.5-17.2) mm. The AAD ranged from 0.5 to 17.2 mm lateral to 0.8 to 8.2 mm medial (Table 3).
A summary of radiographic data obtained in a total of 6 cases that had obvious parallax/distortion.
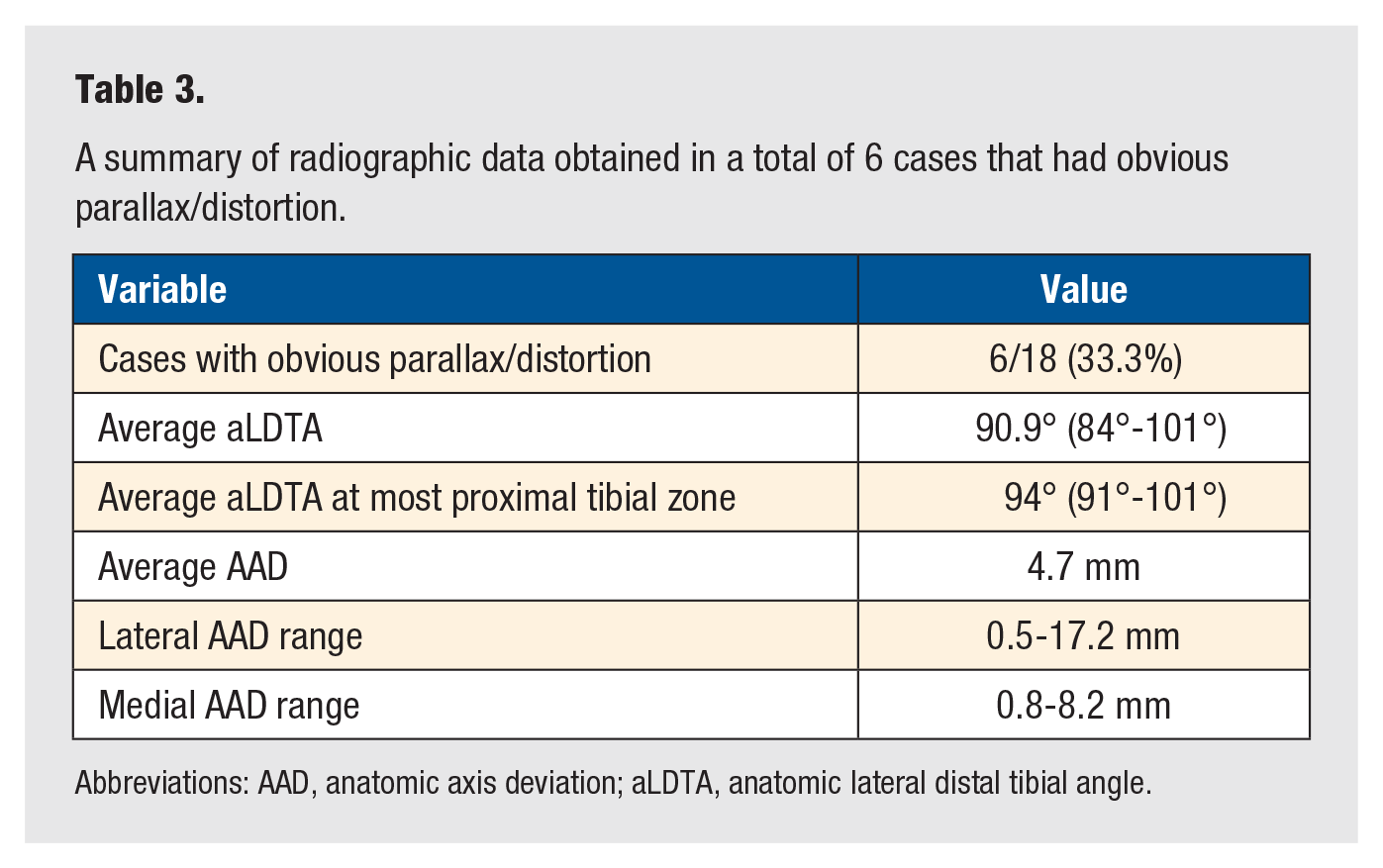
Abbreviations: AAD, anatomic axis deviation; aLDTA, anatomic lateral distal tibial angle.
In comparison to intraoperative fluoroscopic images, postoperative plain film radiographs displayed no obvious parallax/distortion, as noted by a lack of gross curvature of anatomical structures. The average aLDTA for postoperative plain film radiographs was 89.25° (ranging from 88.1° to 90.5°), which lies within the normal range for the aLDTA. In addition, the AAT was centered within the ankle joint in all postoperative plain film radiographs.
Discussion
The present retrospective review aimed to evaluate the impact of parallax/distortion on TAAs by analyzing intraoperative fluoroscopic images and measuring any angular deviations. We found that cases with obvious parallax/distortion had an average aLDTA of 90.9°, which increased to 94° at the most proximal tibial zone. In addition, we noted an average AAD of 4.7 mm, which ranged from 0.5 to 17.2 mm lateral to 0.8 to 8.2 mm medial. The findings of this study provide valuable insights into the challenges posed by parallax/distortion, its potential implications for TAAs, and potential ways to help mitigate these deleterious effects.
Fluoroscopy utilization is an indispensable tool for surgeons, providing imaging guidance to enhance precision of procedures, such as TAA. Parallax in fluoroscopy refers to the apparent shift in position of an object as observed from different angles. 8 This occurs due to the inherent variation of angled beams within fluoroscopy units, as well as the potential inaccurate projection of the C-arm on the intended object. The apparent shift of anatomical landmarks caused by parallax/distortion can result in angular deviation and linear displacements of implant components. Literature on total knee and total hip arthroplasties has emphasized these effects.9 -12 Talbot et al reported on femoral component malrotation due to parallax errors in total knee arthroplasty. They emphasized the importance of identifying reproducible anatomical landmarks and removing parallax errors to limit the malrotation of components. 9 Thorne et al 12 described changes in acetabular cup positioning due to parallax distortion and positioning of the fluoroscopy unit. To the authors’ knowledge, no literature has focused on the effect of parallax on TAAs.
Implant positioning is critical to a successful outcome in TAAs. Parallax/distortion can potentially lead to errors in surgical technique and malalignment of the prosthesis. In a normal ankle joint, there is a valgus moment as the weight-bearing axis passes slightly lateral from the midline of the tibia to the calcaneus. 15 When performing a TAA, the weight-bearing axis should be maintained with a valgus moment. In their study of 50 TAAs, Schuberth et al 7 found that malalignment of the prosthesis could occur secondary to inadequate fluoroscopic imaging of the tibial axis. Malalignment of components is likely to lead to increased wear and often requires revision.
Implant malposition can lead to significant complications, including impingement, increased risk of subsidence, and component loosening. Cody et al 6 reviewed risk factors for failure in TAAs of over 500 ankles and found that talar subsidence (41%) and component loosening (21%) were the most common reasons for revision. In addition, talar component tilting can lead to edge loading or shear forces secondary to abnormal forces at the component-bone and/or polyethylene-component interfaces. 7 These factors combine to show that malpositioned components lead to earlier failure in TAAs. The findings of this study emphasize the need for strategies to minimize parallax-related errors during TAA surgery and optimize implant positioning to mitigate these potential complications.
Similar to TAA, fluoroscopic imaging can affect surgical precision during intramedullary nailing. Kagan et al performed a cadaveric study evaluating the degree of error caused by parallax at the distal femur for intramedullary nailing of diaphyseal femur fractures. These authors found parallax can result in potentially clinically significant malrotation deformities. They emphasized the importance of perfect centering within the field of view (FOV) when obtaining intraoperative fluoroscopic images. 16 McArthur et al described a parallax phenomenon causing valgus malalignment at the ankle joint and the potential implications during intramedullary nailing. They found a mean LDTA of 89° when the image intensifier was orthogonal, whereas the mean LDTA was 79° with the image intensifier at 15° craniocaudal. They emphasized the importance of orthogonal alignment of the image intensifier to reduce this malalignment. 17 We found an average aLDTA of 90.9°, which increased to 94° at the most proximal tibial zone. We recommend centering of the tibiotalar joint within the FOV when obtaining intraoperative fluoroscopic images.
Several approaches can be considered to limit the impact of parallax/distortion in TAA. Multiple authors have emphasized the importance of ensuring the object being imaged is within the center of the FOV.16,18 -20 Weldon et al reported that measurement errors increase by 14% per 10 mm of horizontal C-arm offset. This is negated, with a minimal effect, when the image is obtained within 5 mm of the true center of the object. 18 In addition, narrowing the FOV or increasing the image magnification can decrease the amount of distortion. 19 Surgeons can work together with radiologist technicians to adjust the position of the X-ray beam relative to the object of interest in order to alter the apparent bony alignment. Although difficult to control, it is important to note that sigmoidal distortion can occur when electrons veer off course secondary to external electromagnetic fields. The most common sources of powerful electromagnetic fields include magnetic resonance imaging machines and the central power-supply grid. These factors should be considered when designing new surgical suites.
Limitations
There are several limitations of this study that should be mentioned. First, the retrospective design introduces inherent biases and limitations in data collection. Fluoroscopic images were likely derived from multiple fluoroscopic units. As this is a retrospective study, we are unable to identify which units were utilized to obtain the images. The reliance on radiographic measurements may introduce measurement errors and interobserver variability. No form of measuring parallax/distortion has been established, and thus measurements and any deviation were based on standard angles evaluated at the ankle joint. This study evaluated TAAs performed at a single institution, and thus, generalizability may be limited. In addition, patient outcomes and long-term radiographs were not evaluated. However, we believe the findings of this study are important to consider for surgeons who are performing TAAs.
Conclusion
In conclusion, parallax may distort the appearance of anatomical structures on intraoperative fluoroscopic images, particularly the normal tibial anatomical axis. Surgeons should be aware of the challenges posed by parallax/distortion in implant positioning. Further research is warranted to evaluate how parallax/distortion may impact patient outcomes in TAAs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was waived. Full waiver of HIPAA authorization for research for secondary analysis of medical records/biospecimens due to retrospective review of radiologic studies. OhioHealth Office of Human Subjects Protections. IRBNet # 2077283-1
Informed Consent
Informed consent was not sought for the present study.
Trial Registration
Not applicable because this was a retrospective radiological review and not a randomized clinical trial.