
Abstract
Background
Resiliency is the ability to recover from stressful events and has been shown to correlate with patient outcomes following certain orthopaedic procedures. The purpose of this study was to determine the relationship between resiliency and outcomes following TAA.
Methods
A retrospective analysis of patients undergoing primary TAA between April 2015 and September 2022 was performed (N = 83). Data included demographics, comorbidities, complications, preoperative and postoperative visual analog scale (VAS) pain and Foot and Ankle Ability Measure (FAAM) functional scores, Brief Resilience Scale (BRS) scores, and surgical satisfaction. Patients were defined as having low resilience (LR), normal resilience (NR), or high resilience (HR) based on a BRS score of <3, 3–4.30, and >4.3, respectively.
Results
High resilience patients had significantly higher postoperative FAAM ADL, Sports, and Overall scores as well as a significantly greater increase from preoperative scores compared with LR and NR patients. Low resilience patients had significantly lower FAAM Sports and Overall scores compared with normal and high resilience patients. BRS scores positively correlated with postoperative FAAM scores. We found no difference in satisfaction or VAS between the 3 cohorts. Multivariate regression analysis identified BRS scores to be an independent predictor for greater changes in FAAM scores following TAA.
Conclusion
Although functional improvements following TAA are expected, patients with higher resilience at baseline are more likely to experience greater improvements in functional outcomes following surgery.
Level of Evidence:
Level III
“Although functional improvements following TAA are expected, patients with higher resilience at baseline are more likely to experience greater improvements in functional outcomes following surgery.”
Introduction
Total ankle arthroplasty (TAA) has become increasingly more popular over the past decade as a treatment for end-stage ankle arthritis. Previous literature has demonstrated significant improvement in functional outcome scores and ankle range of motion (ROM) compared with ankle arthrodesis while maintaining a similar complication profile and reducing rates of adjacent joint arthritis.1 -3 While there have been much advancements in surgical techniques and implant designs to optimize patient outcomes following TAA, recent interest has turned to the impact of psychological factors on patient outcomes.
Amongst all orthopaedic procedures, depression and anxiety have been shown to correlate with both subjective and objective outcomes.4 -7 Particularly following TAA, Cunningham et al 8 found that depression led to worse outcomes at mid-term follow-up. In a follow-up study, these authors found that patients with depression and lower preoperative mental component summary (MCS) scores had worse outcomes, with less improvement in pain and function compared with those without depression. 9
Despite the known association between psychological co-morbidities and surgical outcomes, what is often underappreciated are the subclinical psychological variables, particularly resilience. Resilience is defined as the ability to bounce back or recover from stress. 10 An individual with a high level of resilience is better able to manage difficult circumstances and accept situations that cannot be changed. Patients undergoing orthopaedic surgery may experience a significant amount of stress. Patients with greater resilience may be more successful at managing their perioperative circumstances, ultimately leading to a better functional outcome postoperatively.11 -13
There are many scales that measure resilience. 14 The Brief Resilience Scale (BRS), which is a 6-item Likert Scoring scale, has been validated in the adult population and is the most used resilience scale in musculoskeletal literature. 10 Following total joint arthroplasty, resilience has been found to be a predictor of improved postoperative outcomes and shorter length of stay.11 -13 The foot and ankle literature, however, has demonstrated more mixed results on the influence of resiliency and postoperative outcomes.15,16 No study to date has investigated the influence of resilience on outcomes following TAA.
Since resilience can be a promising predictor of postoperative outcomes, further knowledge of this subject specific to TAA would help guide the treatment of patients undergoing this procedure and help predict postoperative success. The purpose of this study is to investigate the relationship between patient resilience and outcomes after TAA. We hypothesize that patients with higher resilience will report higher postoperative outcome scores, and a greater improvement in pain and functional compared with preoperatively.
Materials and Methods
After obtaining approval from the Institutional Review Board (IRB), a retrospective review was conducted on patients who completed preoperative Foot and Ankle Ability Measure (FAAM) and Visual Analog Scale (VAS) and underwent a primary total ankle arthroplasty between April 2015 and September 2022 by 1 of the 4 fellowship trained orthopaedic foot and ankle surgeons. Details regarding the recruitment process are depicted in Figure 1.
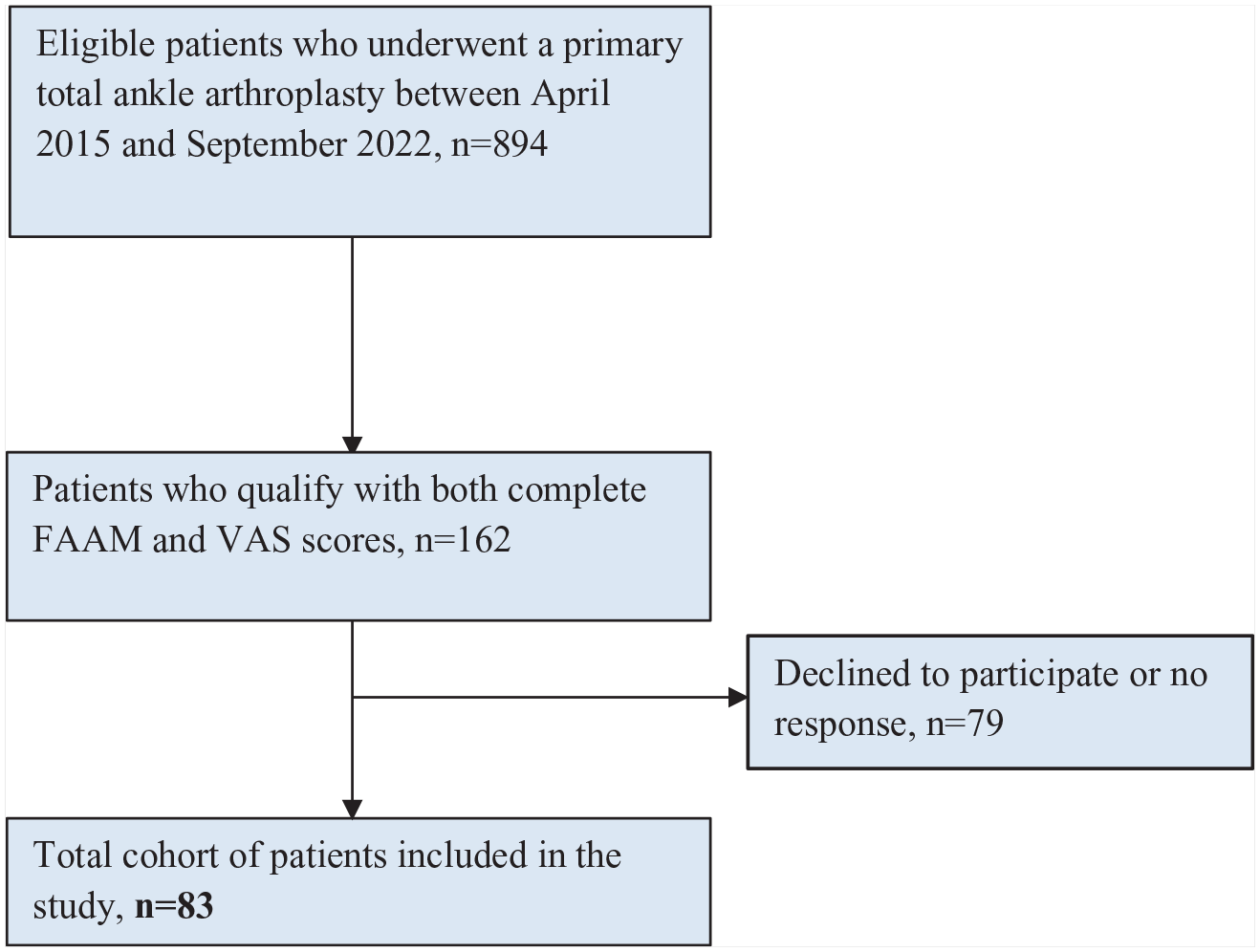
Flow diagram of patient recruitment and inclusion.
Data Collection
Demographic data comprising of date of birth (DOB), diabetes mellitus (DM), body mass index (BMI), smoking history, surgical complications, and subsequent surgeries was collected via chart review. Both preoperative and postoperative patient-reported outcome measures (PROMs) including FAAM functional scores and VAS scores were collected. Both PROMs had already been collected in the clinic during patients’ appointments. If multiple dated preoperative and postoperative scores were presented, then the closest preoperative date to surgery and most recent postoperative date were used. The VAS is a validated, subjective measure for acute and chronic pain which reports pain scores on a continuum. 17 The FAAM is an instrument used to measure the function of the ankle/foot joint complex. It’s a validated tool that is divided into 2 subscales: activities of daily living (ADL) and sports. 18 An overall FAAM score is also reported.
Patients were contacted via telephone to complete their Brief Resilience Scale (BRS) scores and satisfaction with the outcome of their primary TAA surgery. The BRS is one of the most commonly used tools to measure resilience. 19 It has been shown to be a reliable tool with good criterion validity to evaluate resilience.10,19 Patients in the current study were defined as having low, normal, or high resilience based on a BRS score of < 3, 3-4.30, and > 4.3, respectively. By completing the BRS and satisfaction survey, participants thereby consented to participate in the study and their scores were then included in the data analysis. Patients were excluded if they did not have preoperative and postoperative FAAM and VAS scores. The remaining 162 patients were then contacted to complete the BRS and surgical satisfaction surveys, resulting in a total of 83 patients making up the final cohort for data analysis (Figure 1).
Statistical Analysis
Continuous data are presented as either mean (standard deviation) or median [first quartile; third quartile] depending on its normality. Normality was assessed using Shapiro-Wilks tests and Kolmogorov-Smirnov. Categorical data are presented as cell count (%). Analysis of variance (ANOVA) or Kruskal-Wallis tests were used to compare continuous data and Chi-Square tests were used to compare categorical data. Further correlation analysis of BRS Overall Score to PROM Outcome Scores was performed and presented as Pearson product-moment correlation coefficient r. If data were proven to be significant, pairwise testing was performed to see whether a true difference existed. A multivariate logistic regression model was developed to assess for relationship between BRS and change in FAAM scores when controlling for demographic variables, including age, sex, BMI, diabetes, smoking status. A P-value of less than .05 is indicative of statistical significance. All statistical analyses were done using R Studio (Version 3.6.3, Vienna, Austria).
Results
Demographic Characteristics
A total of 83 patients (55 male, 28 female) who underwent primary TAA were included in this study. The average age was 64.4 (±8.5) years, with a median BMI of 28.9. Six (7.2%) patients had a diagnosis of diabetes at time of surgery, and 5 (6.0%) patients reported being current smokers. The average follow-up was 13.4 (11.0-24.8) months. The average BRS score was 4.0 (3.17-4.5), with 9 (10.8%) patients being classified as low, 44 (53.0%) classified as normal, and 30 (36.1%) classified as high resilience (Table 1).
Characteristics by Resiliency Cohort.
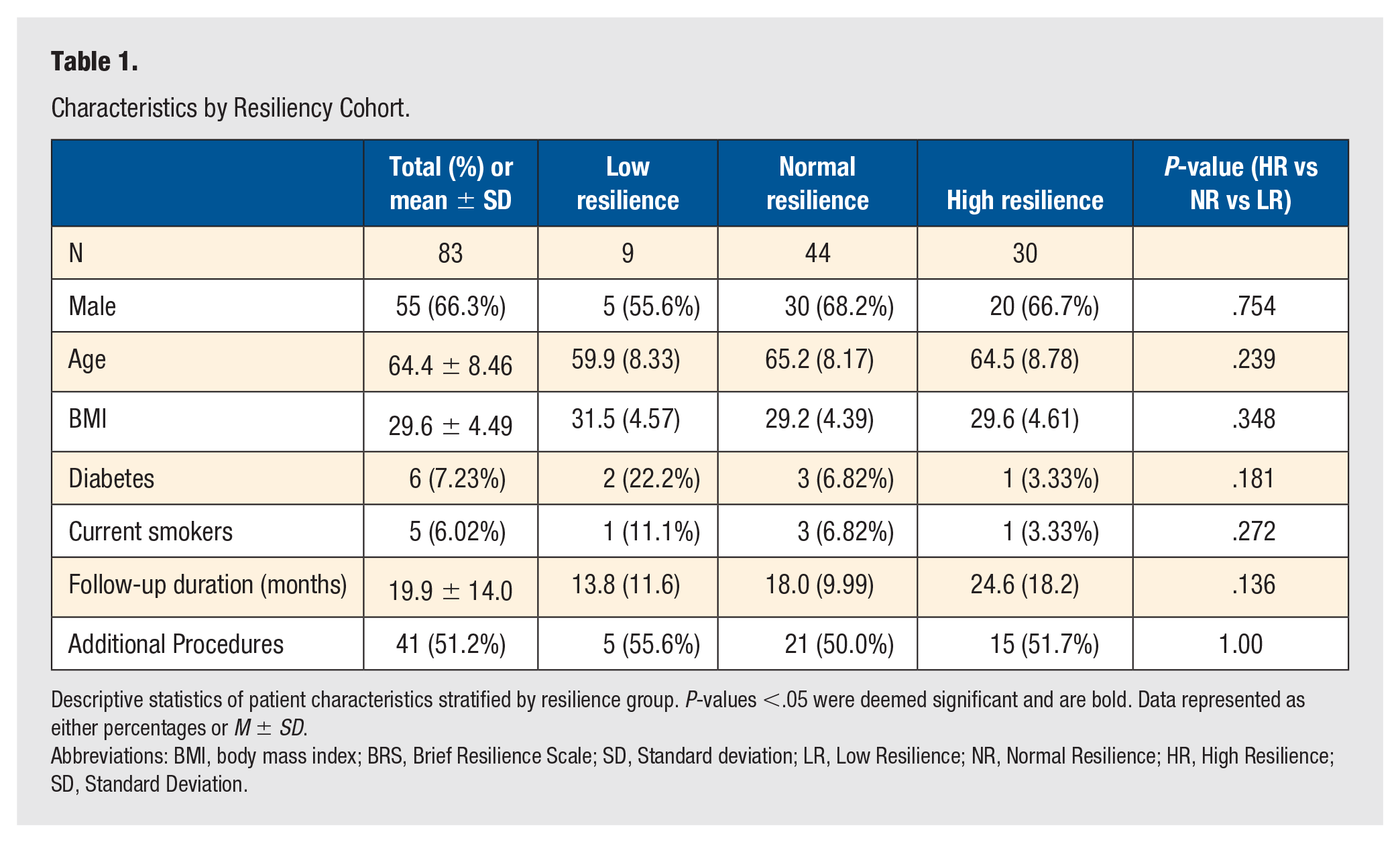
Descriptive statistics of patient characteristics stratified by resilience group. P-values <.05 were deemed significant and are bold. Data represented as either percentages or M ± SD.
Abbreviations: BMI, body mass index; BRS, Brief Resilience Scale; SD, Standard deviation; LR, Low Resilience; NR, Normal Resilience; HR, High Resilience; SD, Standard Deviation.
Clinical Outcomes
Eighty-four percent of patients reported being either very satisfied or satisfied with their procedure at final follow-up. The average preoperative and postoperative VAS and FAAM ADL, Sports, and Overall scores broken down by resiliency cohort are reported in Table 2. There were a total of 3 complications: 1 patient required irrigation and debridement for proximal tibial pin-tract infection, 1 patient had delayed wound healing of anterior incision requiring a wound vac, and 1 patient experienced a periprosthetic medial malleolar fracture that was successfully treated conservatively.
Clinical Outcomes by Resiliency Cohort.
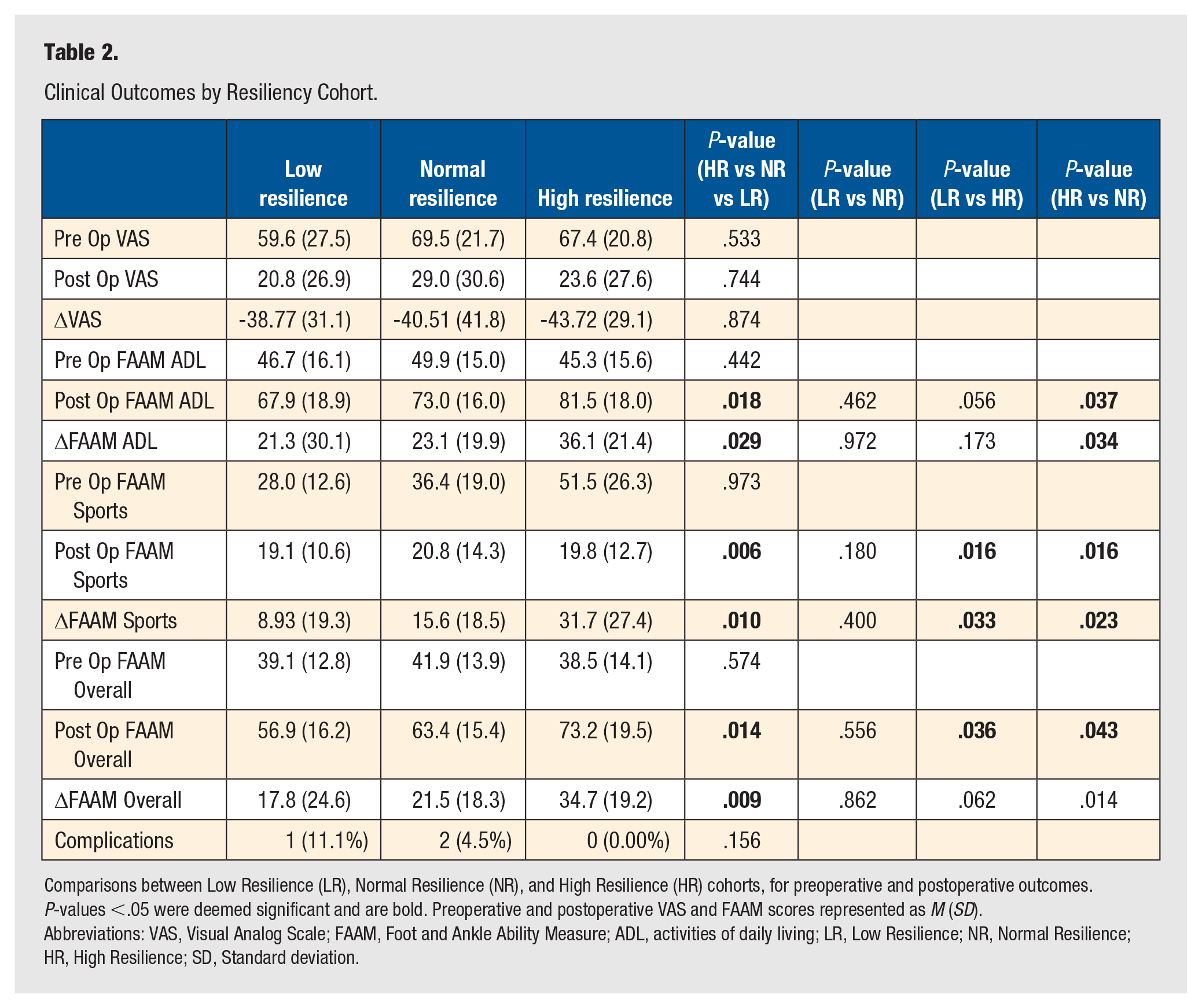
Comparisons between Low Resilience (LR), Normal Resilience (NR), and High Resilience (HR) cohorts, for preoperative and postoperative outcomes. P-values <.05 were deemed significant and are bold. Preoperative and postoperative VAS and FAAM scores represented as M (SD).
Abbreviations: VAS, Visual Analog Scale; FAAM, Foot and Ankle Ability Measure; ADL, activities of daily living; LR, Low Resilience; NR, Normal Resilience; HR, High Resilience; SD, Standard deviation.
Comparative Analysis
No statistical difference was found between low, normal, and high resilience groups in terms of demographics, BMI, diabetes, smoking, follow-up duration, or additional procedures performed (Table 1). There was no statistically significant difference in preoperative VAS or FAAM scores amongst resilience groups. High resilience patients had significantly higher postoperative FAAM ADL (P = .037), Sports (P = .016), and Overall (P = .043) scores as well as significantly greater increase from preoperative scores compared with normal resilience patients. Low resilience patients had significantly lower FAAM Sports (P = .016) and Overall (P = .036) scores compared with normal and high resilience patients. There were no statistically significant differences found between VAS pain scores or complication rates amongst groups (Table 2).
The BRS significantly, although weakly, correlated with increased postoperative FAAM ADL (r = .324), Sport (r = .402), and Overall Scores (r = .368), but did not correlate with VAS scores (r = .002) (Table 3). Multivariable regression analysis identified BRS score as an independent predictor of greater changes in FAAM ADL (P = .002), Sport (P ≤ .001), and Overall (P = .001) (Table 4).
Correlation of BRS and Clinical Outcomes. Correlation Values Between BRS Scores and Preoperative and Postoperative Clinical Outcomes.
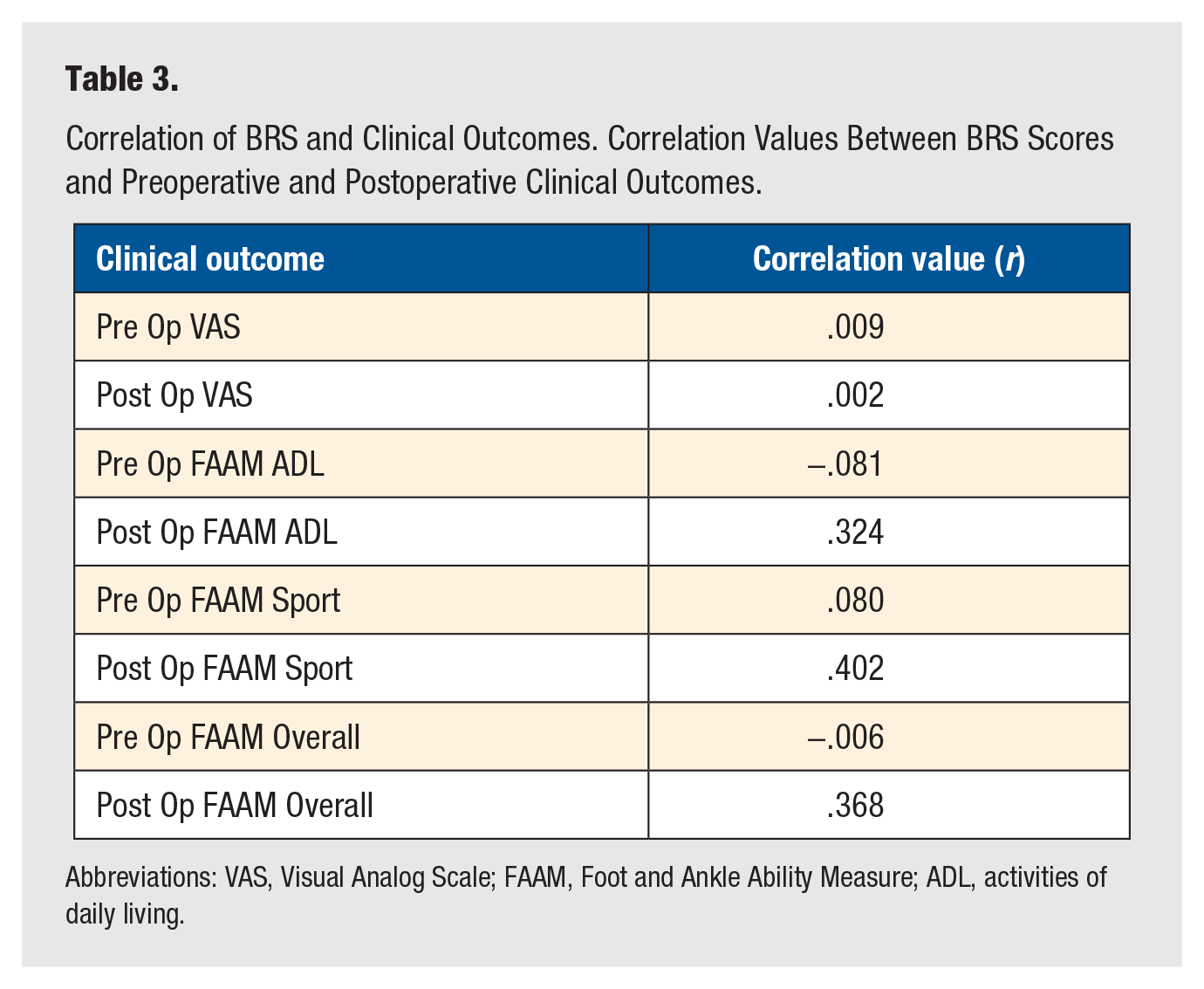
Abbreviations: VAS, Visual Analog Scale; FAAM, Foot and Ankle Ability Measure; ADL, activities of daily living.
Multivariate Regression Analysis of the Effect of BRS Scores on Change in FAAM.

P-values <.05 were deemed significant and are bold.
Abbreviations: FAAM, Foot and Ankle Ability Measure; ADL, activities of daily living.
Discussion
The impact of psychological comorbidities on outcomes following orthopaedic surgery is well documented.4 -7 Sub-clinical psychological factors, such as resilience, and their role in orthopedics is less understood. The purpose of this study was to investigate the relationship between patient resilience and PROMs after total ankle arthroplasty. Using the BRS, a validated 6-question survey that quantifies resilience, this study found that BRS scores positively correlated with postoperative FAAM scores following TAA. In addition, BRS score was found to be an independent predictor for greater changes in FAAM scores following TAA.
Recent studies in the orthopaedic literature have demonstrated mixed results on the impact of resiliency and postoperative outcomes.11 -13,15,16,20 There have been positive correlation between resiliency and outcomes following total joint arthroplasty. Magaldi et al 11 found resilience to be a significant predictor of overall physical and mental health outcomes at both 3 and 12 months following total knee arthroplasty. Similarly, following total shoulder arthroplasty, BRS scores were found to be significantly correlated with a number of postoperative PROMs. 12 Following total hip arthroplasty, increased resilience was found to be positively associated with decreased length of stay and a higher likelihood of same-day-discharge. 13
The foot and ankle literature, however, has demonstrated more mixed results regarding the influence of resiliency on postoperative outcomes.15,16 In a retrospective review of a large number of foot and ankle procedures, Hoch et al 16 found the BRS to be an unreliable tool for predicting outcomes in foot and ankle surgery. Their study, however, covered a variety of small foot and ankle procedures where large changes in postoperative outcomes would not be expected. For example, the most common procedure in this cohort was removal of hardware. This study investigated only primary TAA, which was not included in Hoch et al’s analysis.
As advances are made in the surgical techniques and implant designs for TAA, surgeons seek to maximally optimize postoperative patient outcomes. There remains, however, several factors outside of the surgeon’s control that play a vital role. Current data does demonstrate significant improvement in pain and functional outcomes following TAA 1 ; however, a number of factors have been found to have a negative impact on improvement, including depression, smoking, increased American Society of Anesthesiologists (ASA) score, obesity, and age.8,9 Identifying and eliminating some of these modifiable risk factors is vital for the continued improvement in outcomes of patients.
The primary patient outcome measure used in this study was the FAAM, which is a self-reported instrument to assess physical function in patients with foot and ankle conditions. The FAAM includes 21-item ADL and 8-item Sports subscales, which together produced information across the spectrum patient ability. Matheny and Clanton 21 investigated the reliability and validity of the FAAM utilizing the Rasch measurement rating scale model (RSM) and found strong evidence for the reliability and validity for the FAAM ADL and Sports scores.
The results of this study, which demonstrated resilience to positively correlate with functional outcomes following TAA, shed light on another important variable that plays a role in how patients will perform after surgery. These findings point to the importance of identifying sources of stress and anxiety during the perioperative period for patients. Furthermore, integrating questions into the surgical decision-making process may help reveal patients who are able to undergo such a stressful or potentially traumatic event such as TAA. Not only did resilience correlate with higher postoperative PROM, patients with high resilience were also more likely to report greater changes in FAAM scores from preoperatively to postoperatively. These findings validate the concept of resilience and highlight its relevance in patients undergoing total ankle arthroplasty.
Our study found no correlation between resilience and postoperative VAS scores. Although the VAS is a subjective measure for acute and chronic pain, there is mixed evidence on its true utility and reliability. A retrospective review of all foot and ankle procedures found no correlation between opioid or benzodiazepine use and VAS scores. 16 Although there is value in demonstrating improvement following intervention amongst individual patients, its true clinical correlation and reliability with subjective outcomes comes into question. 22
Within the patient cohort in this study, there were a total of 3 complications. One patient in the low resilience group required irrigation and debridement for proximal tibial pin-tract infection. In the normal resilience group, 1 patient had delayed wound healing of the anterior incision requiring a wound vac. The last patient experienced a periprosthetic medial malleolar fracture that was successfully treated conservatively. There were no complications in the high resilience group. There was no statistically significant difference in complication rates amongst resilience groups in our patient cohort.
We acknowledge the limitations of our study. First, the retrospective design of this study has the potential to introduce multiple biases known to afflict this design. Second, there is inherent response bias in the survey aspect of this study, as patients were contacted postoperatively to obtain postoperative PROMs. Recall bias could have been introduced into the study population as patients completed the BRS questionnaire postoperatively. Patients who experienced outcomes or satisfaction on the extremes may have been more willing to participate in the study. In addition, given the small sample size in this study, particularly with the low resilience group, there is potential for Type II error in our results. Despite this, our study did find significant differences between groups for FAAM ADL, Sports, and Overall scores when compared with the high resilience group; however, the potential differences, especially when compared with the low resilience group may have been greater with a larger sample size. This difference in number of patients in the low compared with normal and high resilience group is, however, in accordance with previous resilience studies when reported.20,13 Finally, administration of the BRS postoperatively is suboptimal when compared with preoperative administration, as postoperative state may affect one’s response to the questionnaire. Therefore, based on our study, it is not possible to say whether BRS scores, if collected preoperatively, would have been predictive of better or worse outcomes.
Conclusion
This was the first study to investigate the relationship between resiliency and clinical outcomes following TAA. Although functional improvements following TAA are expected, those patients with higher resilience at baseline are more likely to experience greater improvements in functional outcomes following surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was reviewed and approved by the IRB at Thomas Jefferson University, study number #21E.844
Informed Consent
Verbal informed consent was obtained from all subjects before the study, as outlined in section “Materials and Methods.”
Trial registration
Trial registration is not applicable.