
Abstract
We report the case of an 11-year-old boy with a late-presenting distal tibial Salter-Harris type 2 injury. Before approaching us, he had undergone 2 failed attempts of treatment (closed reduction with plaster cast application and closed reduction and K-wire fixation with plaster cast application). On the 13th day after the injury, the fracture was treated with a closed reduction and metaphyseal canulated cancellous screw fixation and plate fixation of the fibular fracture. At skeletal maturity (4.5 years after the surgery), there was no physeal growth arrest or deformity. We report a favorable outcome in a late-presenting distal tibial Salter-Harris type 2 physeal injury after surgical intervention, which was effective despite the delayed presentation and prior treatment failures.
Keywords
“We report a favorable outcome in a late-presenting distal tibial Salter-Harris type 2 physeal injury after surgical intervention, which was effective despite the delayed presentation and prior treatment failures.”
Introduction
Physeal fractures need urgent treatment. Any treatment interventions in late-presenting physeal injuries are fraught with a high risk of premature physeal closure. If treated 5 to 7 days after the injury, physeal injuries carry a high risk of premature physeal closure. This leads to deformity and limb length inequality, especially in a young child.1,2
Salter-Harris type 2 is the most common physeal fracture of the distal tibia. 3 The physis of the distal tibia is an important contributor to the growth of the tibia. It adds 3 to 5 mm of length annually and provides 30% to 40% of the growth of the tibia. 4 This growth plate ceases to grow at around 15 years of age in boys and around 14 years of age in girls. Due to this growth potential, the premature physeal closure of the distal tibia in a growing child may lead to significant shortening and/or angular deformity of the leg. This deformity may need surgical treatment.
To the best of our knowledge, there is no report of a successful outcome in a late-presenting distal tibial Salter-Harris type 2 fracture with a history of 2 previous treatment attempts.
The patient and his parents were informed that data concerning the case would be submitted for publication, and they have provided consent.
Case Presentation
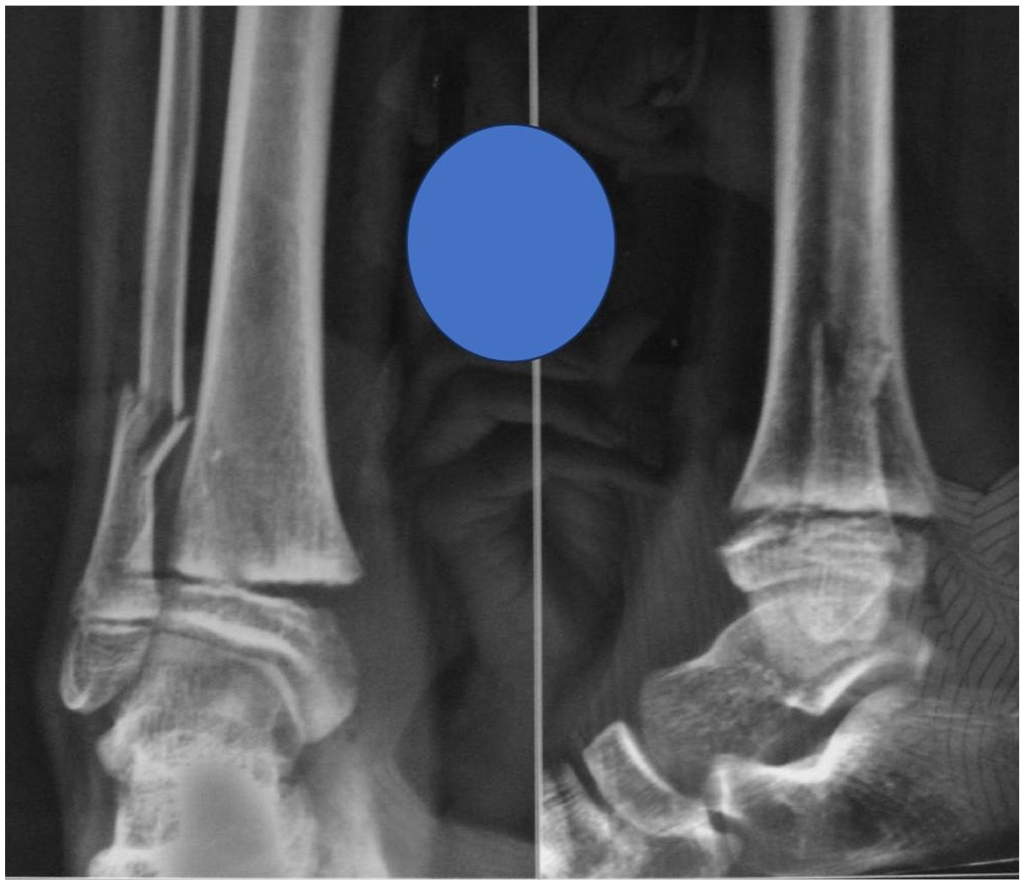
An 11-year-old boy presented with a right ankle fracture of 11 days duration after having undergone 2 treatment interventions elsewhere. He injured his ankle while running. He had undergone closed reduction and cast application under general anesthesia in the operating room on day 2, followed by redo closed reduction, K-wire fixation, and cast application on day 5 postinjury. The patient was referred to us for further treatment due to the unacceptable position of the distal tibial physeal fracture. The patient’s height at the time of presentation was 142 cm and weight was 36 kg. Clinical examination after plaster cast removal showed an isolated closed injury to the ankle with diffuse swelling. A K-wire was noted outside the skin without any signs of local infection. Tenderness was present over the distal tibia and fibula. The neurovascular examination was unremarkable. The radiographs demonstrated a Salter-Harris type 2 physeal fracture of the distal tibia with posterolateral displacement with a comminuted distal fibular fracture with K-wire (Figure 1).

Radiographs showing displaced Salter-Harris type 2 physeal fracture of the distal tibia with K-wire in situ and a distal fibular fracture.
The radiographs on the day of injury showed a displaced Salter-Harris type 2 fracture involving the distal tibia and a comminuted extra-articular distal fibular fracture (Figure 2). Radiographs after the closed reduction showed a persistent gap at the distal tibial physis (Figure 3). Radiographs after re-reduction and K-wire fixation showed a posterolaterally displaced distal tibial epiphysis with a physeal gap of 4 mm with a K-wire present medially in the distal tibia. It also showed an anterior opening at the physis. In order to determine the exact fracture geometry, a computed tomography (CT) scan was done. It showed a distal tibial Salter-Harris type 2 physeal fracture with a posterolaterally displaced metaphyseal fragment with a physeal widening of 4 mm (Figure 4).
Radiographs showing displaced Salter-Harris type 2 physeal fracture of the distal tibia with K-wire in situ and a distal fibular fracture.
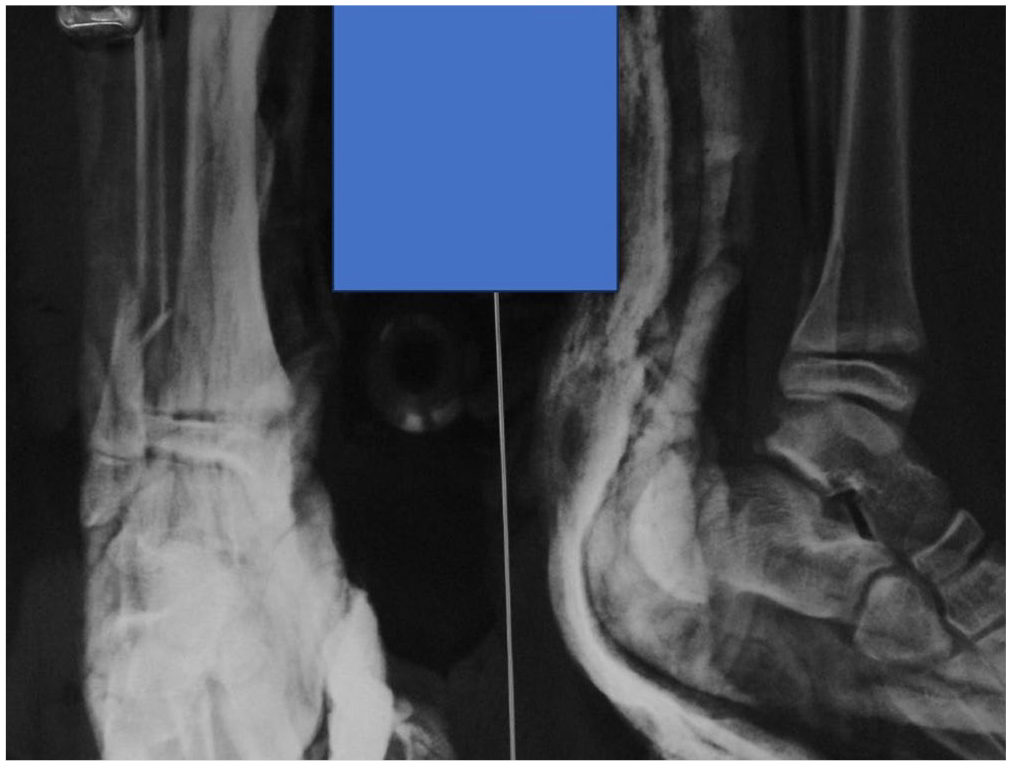
Radiographs after a closed reduction and cast application showing persistent displacement of the distal tibial physeal fracture.
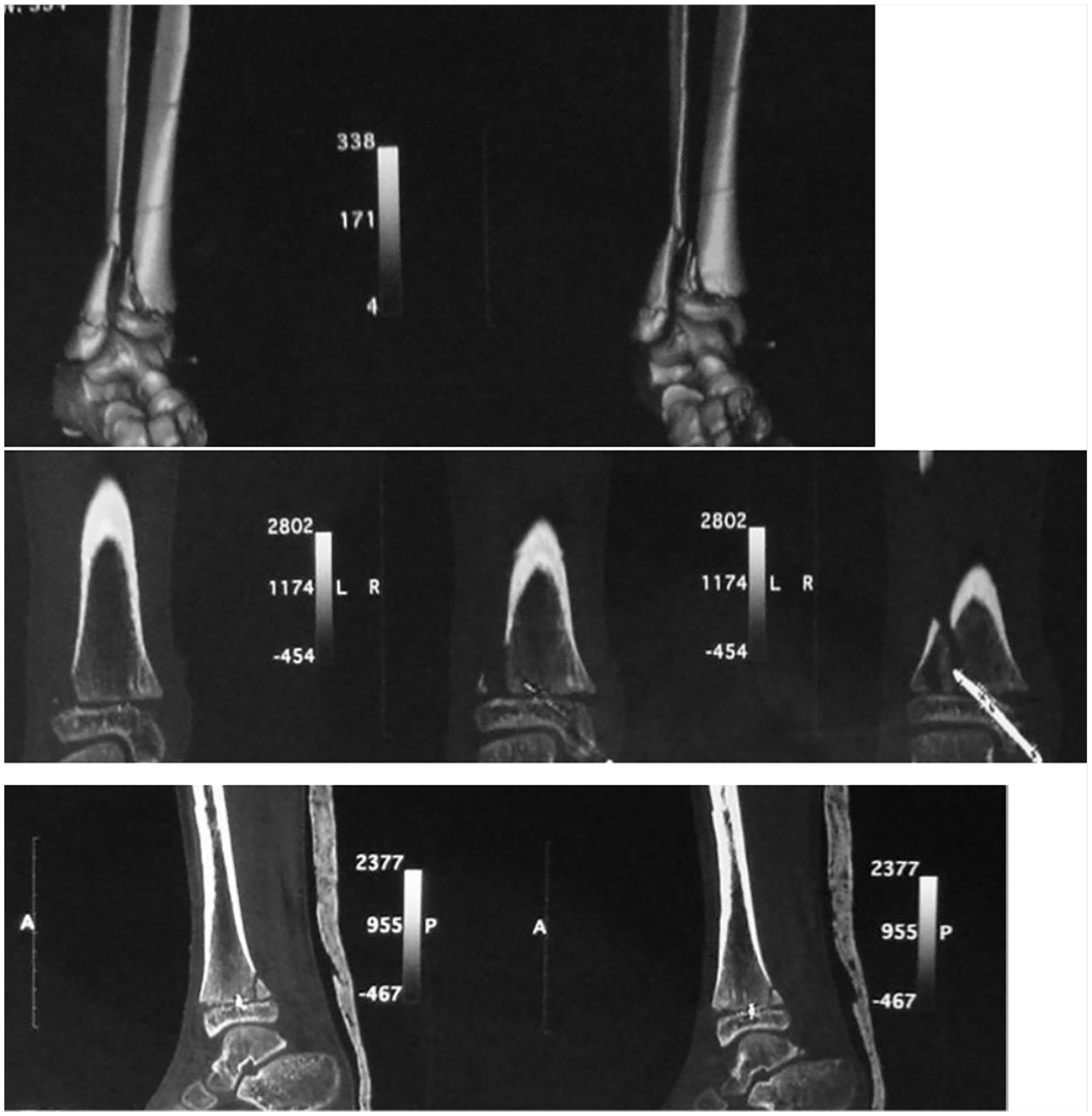
CT scan images showing displaced physeal fracture with a posterolateral metaphyseal fragment.
Operative Treatment
The treatment options discussed with the parents were accepting the position and dealing with the deformity later or performing re-reduction and fixation. The high risk of premature physeal closure was discussed. The parents chose re-reduction and fixation. The surgery was performed under general anesthesia on the 13th day after the injury. A single dose of intravenous cefuroxime was given 30 minutes before the procedure. The K-wire was removed. Under C-arm guidance, a gentle closed reduction was done. Considering the satisfactory alignment of the physeal fragment in anteroposterior (AP) and lateral views, it was decided that an open reduction was unnecessary. Two guidewires were passed percutaneously from the anteromedial to the posterolateral direction in the metaphyseal fragment of the distal tibia. As fibular fracture reduction was unstable, it was decided to fix the fibular fracture. The fibular fracture was treated with open reduction (via the lateral approach) and plate fixation using a nonlocking 1/3rd tubular plate with 3.5 mm screws. Two 4.0 mm partially threaded cannulated cancellous screws were inserted over the tibial guide wires. The screws were tightened to achieve uniform compression across the fracture site. Several C-arm images were taken to confirm the reduction and satisfactory position of the screws. After releasing the tourniquet, hemostasis was achieved. The incisions were closed in layers. A below-knee splint was applied. The patient was kept non–weight bearing and was ambulating with the help of crutches for 6 weeks.
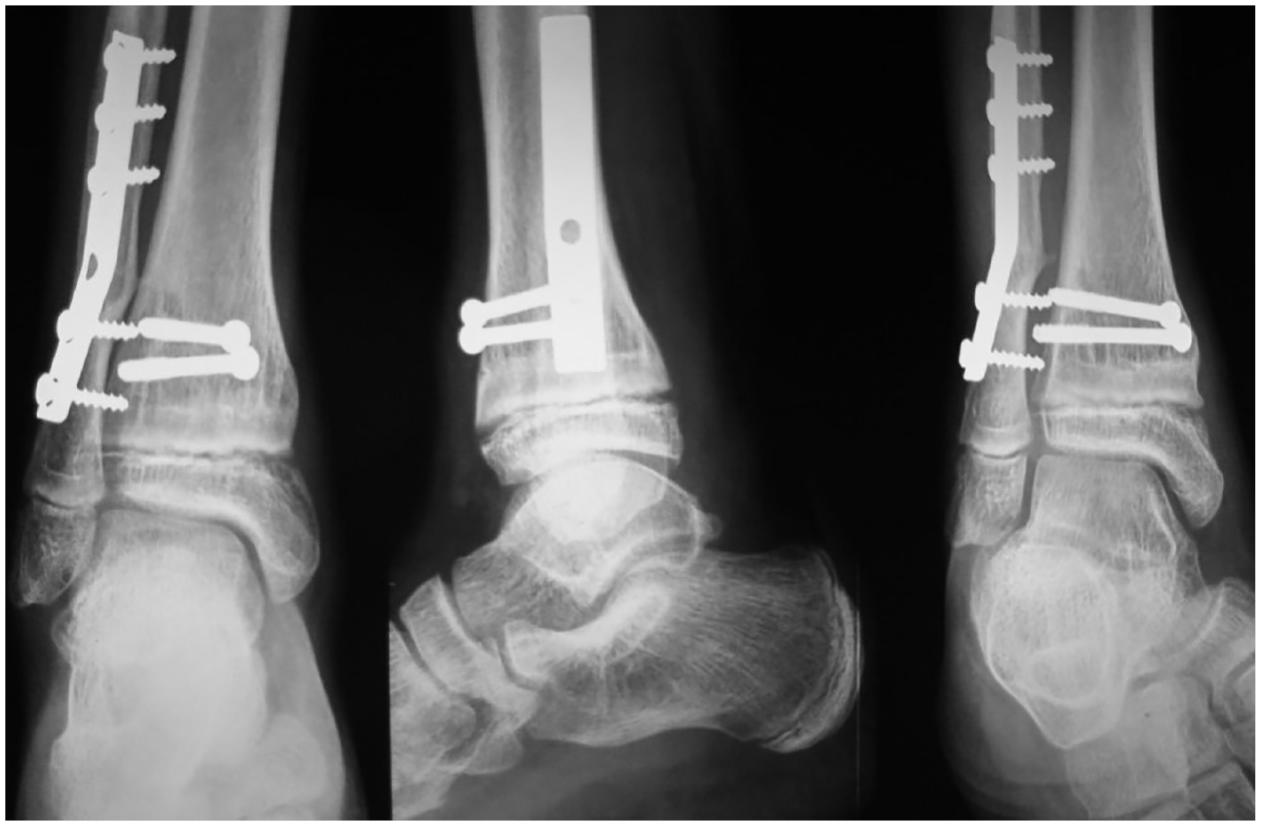
At 2 weeks, the healing of the incisions was confirmed. Radiographs at 6 weeks showed healing at the fracture site (Figure 5). Physiotherapy was started for ankle range of motion, proprioception, and strengthening. Progressive weight bearing was allowed after 6 weeks. At 6 months, the patient had resumed all his previous activities, including sports. Implant removal was offered after 1 year, but the family declined. The patient was followed up at 6-monthly intervals (Figure 6).
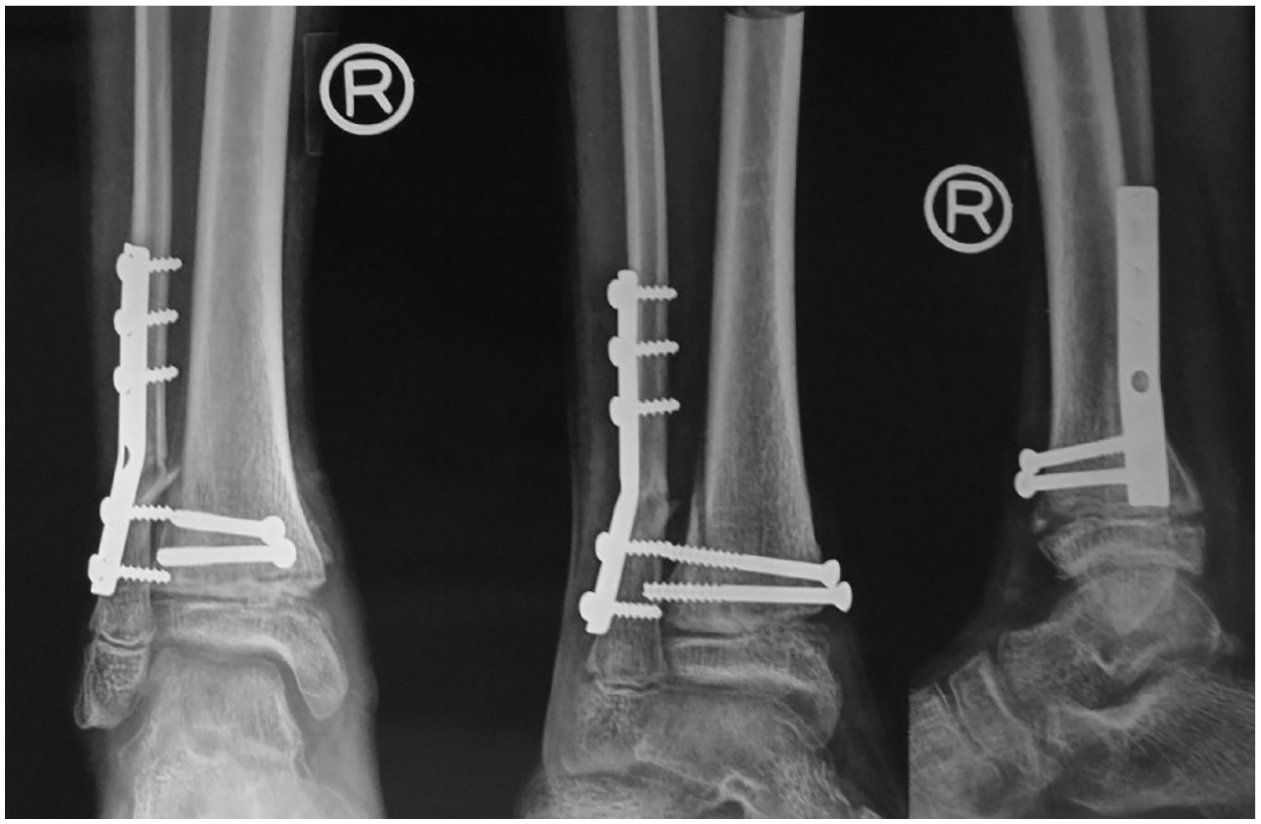
Radiographs after re-reduction of canulated cancellous screw fixation of the distal tibial physeal fracture and plate fixation of the fibular fracture.
Radiographs at 2-year follow-up showing healed fractures and open distal tibial physis without any signs of premature physeal closure.
At the last follow-up, 4.5 years after the surgery, his ankle was painless with no deformity. His height and weight were 157 cm and 50 kg, respectively. He was participating in sports such as soccer and cricket without any difficulty or pain. On examination, the ankle dorsiflexion was 10 degrees and plantarflexion was 30 degrees. His leg lengths were equal. The final radiographs showed congruent articular margins with symmetrical joint space. The distal tibial and fibular growth plates were fused, demonstrating skeletal maturity. At the final follow-up (4.5 years postsurgery), the patient demonstrated full skeletal maturity without deformity, proving that late surgical intervention can be successful in select cases (Figure 7).

Radiographs at 4.5 years of follow-up showing physeal closures due to skeletal maturity.
Discussion
We report the successful outcome of a late-presenting distal tibial Salter-Harris type 2 physeal fracture with a history of 2 previous interventions.
Considerable variability exists regarding the indications for operative and nonoperative management and the methods of treatment of distal tibial Salter-Harris type 2 physeal fractures. Consensus exists for the management of patients with <3 mm of displacement after closed reduction, but no consensus exists for cases where the displacement is >3 mm. 5
The rate of premature physeal closure following operative or nonoperative treatment is 0.20% to 40%. 3 Factors contributing to premature physeal closure are the mechanism of injury, fracture type, method of treatment, repeated reduction maneuvers, and residual deformity after the reduction.3,6 -9 With every additional attempt of fracture manipulation, the risk of premature physeal closure increases.8,10 The effect of time elapsed between the injury and the treatment on premature physeal closure is unclear. There is no information on fractures treated at different time frames. Delayed presentation with a history of previous reduction maneuvers and K-wire fixation point toward an unfavorable outcome. The size of the physeal gap might be a guide to decide the treatment. However, opinions are divided regarding doing an open reduction or a closed reduction.7,11
There are no guidelines on the treatment of late-presenting physeal injuries. The treatment decision depends on the age of the child and the plane and severity of the deformity, anatomical location, and the type of physeal fracture. A recent report has shown favorable outcomes in late-presenting distal radial physeal injuries. 12 Another report describes the successful outcome of a late-presenting Salter-Harris type 3 fracture of the distal tibia in a 12-year-old boy treated via a transphyseal open approach. 13 However, there are no case reports or studies on late-presenting Salter-Harris type 2 fractures of the distal tibia with failed prior interventions.
In our case, we considered 2 options—accepting the deformity and dealing with it later if remodeling does not occur or redoing the surgery. Evidence in adults shows that a minimal angular deformity of the distal tibia can have a marked increase in the tibiotalar pressure, leading to the development of early arthritis. 14 Hence, it is desirable to prevent a deformity. After a distal tibial premature physeal closure, the extent of remodeling and the degree of deformity of the distal tibia remain unknown. We discussed the risks of operative and nonoperative treatment with the parents. The parents chose the operative option for restoration of anatomy.
Why did premature physeal closure not happen? The biology of the growth plate is not fully understood. The distal tibial physes may have variable growth potentials. We believe this distal tibial physis responded favorably because of its growth potential and other possible factors such as preserved blood supply, limited physeal damage, or successful anatomic reduction. We do not have a clear answer yet.
While treating a late-presenting physeal fracture, shared decision-making with caregivers is prudent. It is possible to achieve a good outcome following surgical treatment of late-presenting distal tibial Salter-Harris type 2 physeal fracture.
We report the successful outcome in a late-presenting physeal injury with previous failed attempts of treatment. Since this is a single case, the findings may not be generalizable. Although our patient had a good radiological outcome at skeletal maturity (4.5 years postsurgery), the long-term functional outcomes, gait mechanics, and pain scores were not evaluated. We would cautiously recommend considering this approach in a similar scenario. Studies with long-term outcomes are needed to establish standardized treatment guidelines for late-presenting distal tibial Salter-Harris type 2 fractures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
No applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
No applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.