
Abstract
Lateral intersection syndrome, or fibularis intersection syndrome, is an uncommon overuse condition affecting the lateral aspect of the foot involving the intersection of the peroneus longus and brevis tendons. While intersection syndromes have been described in other anatomic locations, such as the wrist and medial foot/ankle, this pathology remains underreported. This cadaveric study aimed to establish baseline anatomical measurements relevant to lateral intersection syndrome. Eight thawed fresh-frozen cadaveric lower limbs, 4 matched pairs, were dissected, and measurements of key lateral foot structures were recorded, including plantar fascia width, peroneus brevis width, the distance between the peroneus brevis and the plantar fascia, and the distance between the cuboid groove and the fifth metatarsal. The average (mean) plantar fascial width was 4.99 mm, whereas the peroneus brevis width averaged 6.64 mm. A notable laterality difference was identified, with right-sided specimens consistently showing larger measurements compared with the left. Limitations include a small sample size and the use of cadaveric models, which may not replicate in vivo tissues. This study serves as a foundational reference for further research into lateral intersection syndrome and highlights the need for increased clinical recognition of the pathology.
Keywords
“A great degree of clinical suspicion, a thorough physical examination, and utilization of MRI and point of care ultrasound are important in the differentiation of lateral intersection syndrome.”
Introduction
Intersection syndrome is a term traditionally used to describe a pathology of the wrist, characterized by pain at the intersection of the abductor pollicis longus and extensor pollicis brevis, where they cross the extensor carpi radialis longus and the extensor carpi radialis brevis tendons.1,2 As an overuse injury, intersection syndrome is common in athletic endeavors that require wrist flexion and extension for extended periods, such as rowers, racket athletes, and weightlifters. Pain, swelling, and crepitus are all common symptoms due to the peritenosynovitis present in intersection syndrome.
An “intersection syndrome” of the foot has also been described for both the medial and lateral aspects of the foot. Medial intersection syndrome of the foot is characterized by fibrosis at the interconnection of the flexor hallucis longus and flexor digitorum longus tendons. 3 This condition has been sparsely described in the literature, with clinical symptoms of pain and tenderness at the master knot of Henry, and in some cases a trigger hallux. 4
Even fewer descriptions of “fibularis intersection syndrome” or lateral intersection syndrome exist in the present literature. In similar fashion to the previous described intersection syndromes, this overuse condition occurs at the intersection of the peroneus longus and brevis. 5 The location of lateral intersection syndrome involves the confluence of not only the peroneal tendons, but also the lateral band of the plantar fascia, the long plantar ligament, and in 4% to 30% of cases an os peroneum.6,7 The purpose of this study is to use cadaveric models to provide anatomic baselines for the structures local to the area of concern in lateral intersection syndrome and to add to the limited available literature on the topic.
Methods
Eight thawed fresh-frozen cadaveric above-knee specimens, 4 matched pairs, were used at the Chicago Cadaveric Anatomy Research Symposium for this study. The authors state that every effort was made to follow all local and international ethical guidelines and laws that pertain to the use of human cadaveric donors in anatomic research. As a cadaveric study, no institutional review board review was required. Identification numbers were assigned to each cadaver, and demographic data were recorded, including gender, weight, height, and laterality.
Specimens were carefully dissected in a layered fashion to evaluate the lateral structures of the rear-/midfoot with dissection based off the longitudinal axis of the fifth metatarsal, as shown in Figure 1. This incision began at the proximally at the level of the fibula and extended distally past the base of the fifth metatarsal to allow full exposure of the anatomic landmarks of interest. Structures of interest were identified, including the peroneus longus, peroneus brevis, cuboid groove, and lateral band of the plantar fascia, as shown in Figure 2. Digital calipers were then used to measure the width of the lateral band of the plantar fascia in a dorsal to plantar fashion, the width of the peroneus brevis in a dorsal to plantar fashion, the distance between the peroneus brevis and the plantar fascia, and the distance between the cuboid groove and the fifth metatarsal. All measurements were recorded in millimeters. Widths were measured just distal to the junction of the peroneus longus and brevis, as demonstrated in Figure 3. All measurements were conducted by a single senior author (CFH).

An example of the cadaveric specimen marked out for dissection based on the longitudinal axis of the fifth metatarsal.
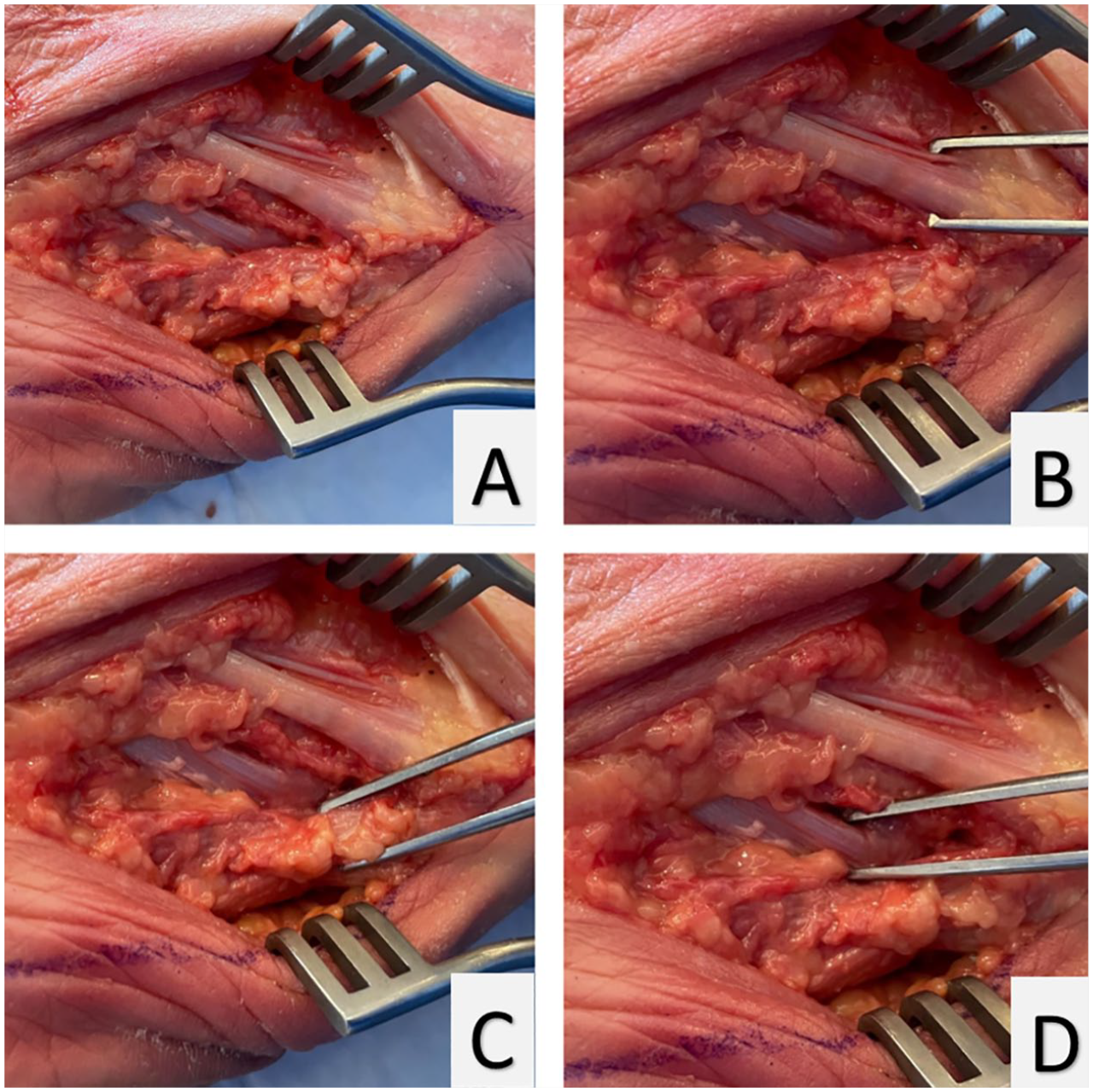
Examples of the dissection (A), with the structures of interest highlighted: peroneus brevis (B), lateral band of the plantar fascia (C), and peroneus longus (D).
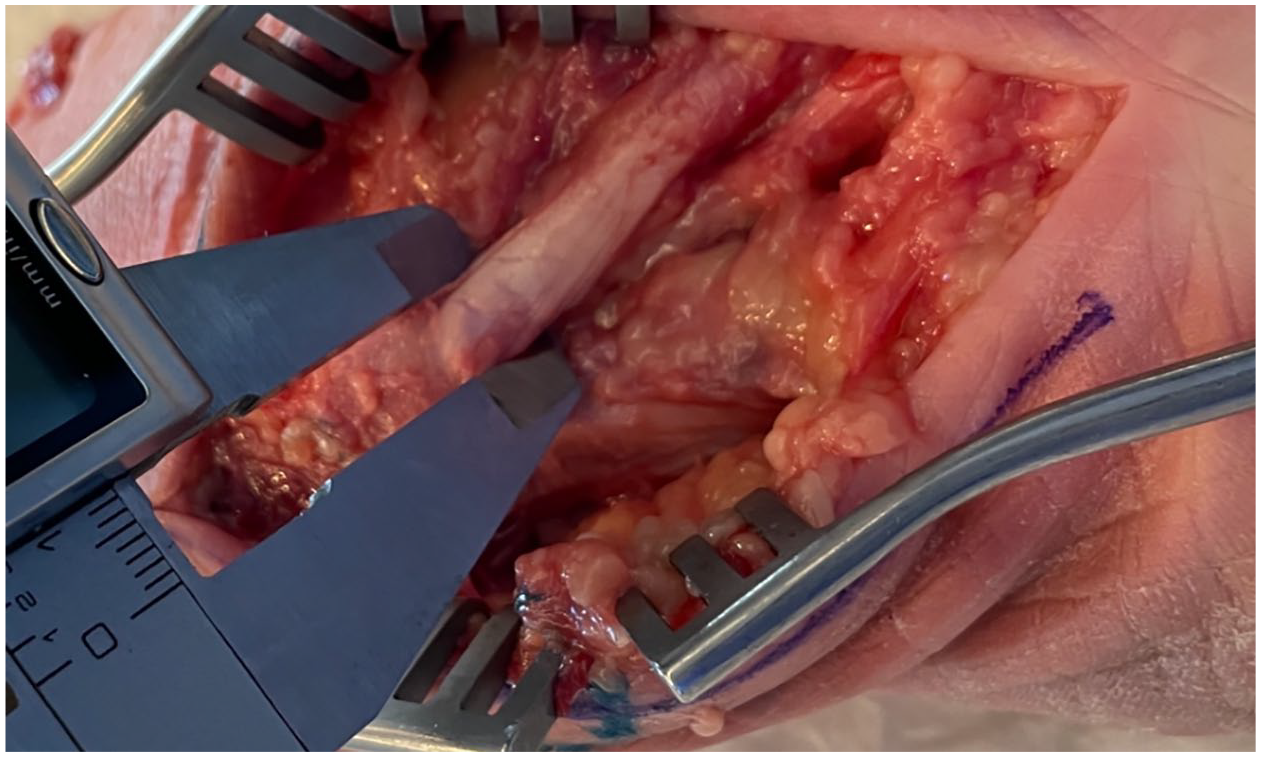
An example of the cadaveric specimens being measured with the digital calipers.
Results
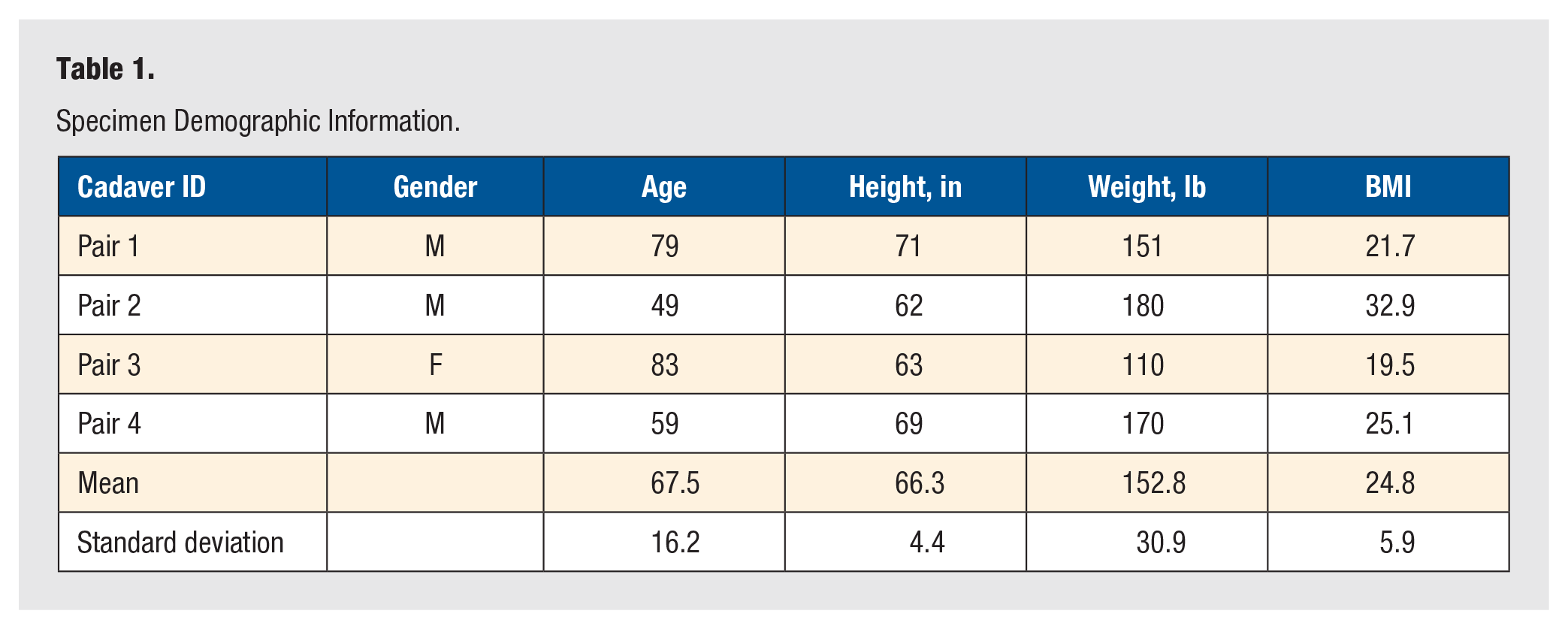
Specimen demographic data were obtained and recorded for all specimens and is shown in Table 1. Of the 4 matched pairs, 3 were male. The average (mean) age of the cadavers at time of expiration was 67.5, with height (in), weight (lb), and body mass index measuring 66.3, 152.8, and 24.8, respectively.
Specimen Demographic Information.
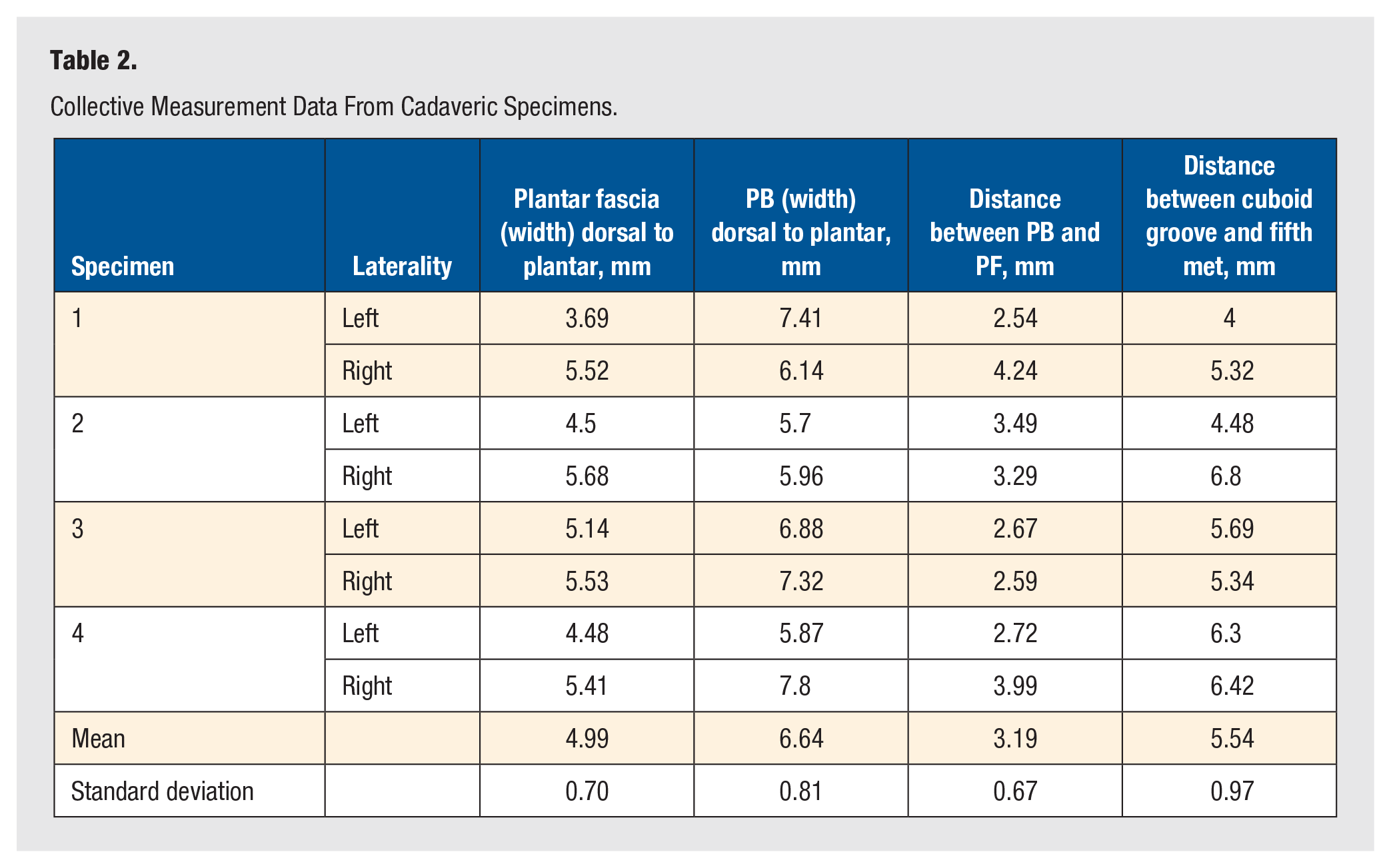
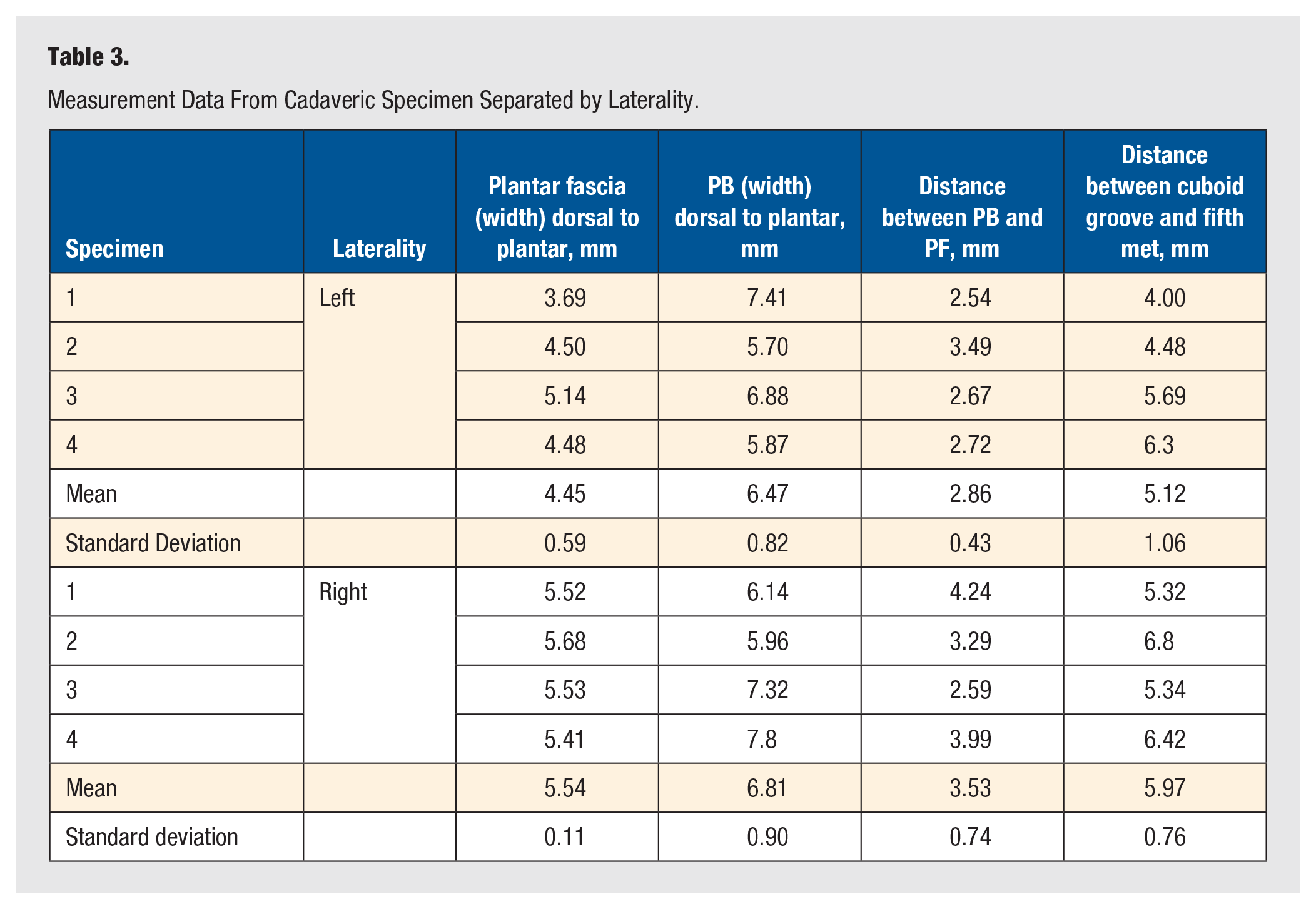
Following dissection, measurements of the lateral aspect of the rear-/midfoot were taken as shown in Table 2. The plantar fascial width from dorsal-to-plantar averaged 4.99 mm across all specimens. Additional measurements included peroneus brevis dorsal-to-plantar width, the distance between the peroneus brevis and plantar fascia, and the distance between the cuboid groove and fifth metatarsal. These measurements averaged (mean) 6.64, 3.19, and 5.54 mm, respectively. When separating the measurements based on laterality, right-sided specimens recorded greater values when compared with left sided specimens, as shown in Table 3.
Collective Measurement Data From Cadaveric Specimens.
Measurement Data From Cadaveric Specimen Separated by Laterality.
Discussion
Fibularis intersection syndrome, or lateral intersection syndrome, is an uncommon overuse condition characterized by pain at the confluence of the peroneus longus and brevis in the lateral aspect of the rearfoot. The present anatomic study provides additional characterization to the anatomic structures involved with this rare pathology.
Our study identified an average (mean) dorsal-to-plantar plantar fascia width, peroneus brevis dorsal-to-plantar width, distance between the peroneus brevis and plantar fascia, and distance between the cuboid groove and fifth metatarsal to be 4.99, 6.64, 3.19, and 5.54 mm, respectively. A difference in laterality was also noted, with right-sided measurements being greater across-the-board compared with their left sided counterparts, as shown in Table 3.
Our findings of an average plantar fascial width of 4.99 mm are within a range that is typically regarded as pathologic. Many studies of plantar fasciitis in symptomatic patients suggest that a thickness of 4 mm or greater is diagnostic for the condition.8,9 However, studies have also suggested that plantar fascial thickness can fluctuate due to activity level, such as in runners, or as a result of thicker and stiffer heel fat pads, such as in the elderly population.10,11 As such, it is possible the average age of our cadaveric specimens at time of expiration (67.5 years) may have contributed to the higher plantar fascia width values obtained in this study.
Conversely, while our study demonstrates measurements that could be interpreted as pathologic when compared with prior magnetic resonance imaging (MRI) studies, the authors believe this may have occurred due to methodological differences. Specifically, that previous studies utilized imaging measurements based primarily off the medial and central bands of the plantar fascia. In addition, MRI and ultrasound measurements are the primary source of measurement in these studies, whereas the measurements in the present study were obtained through direct anatomical dissection. 11 When making a more direct comparison, a cadaveric study by DeVries et al found the average width of the lateral band of the plantar fascia to be 7.2 mm when measured just proximal to insertion on the fifth metatarsal, even greater than in the present study. Their study also found an average dorsal to plantar distance of 5.4 mm between the insertion of the lateral band of the plantar fascia and the peroneus brevis on the fifth metatarsal. 12
Similar to our plantar fascia measurements, the peroneus brevis measurements averaging 6.64 mm would be considered pathologic based on MRI studies.13,14 Again, these clinical and MRI measurements can differ depending on the location of the measurements performed, due to the discontinuity within the peroneus brevis. A prior cadaveric study by Imre et al 15 found an average peroneus brevis tendon width of 14.85 and 4.46 mm at its insertion and prior to insertion, respectively. DeVries et al found an average width of 6.9 mm, correlating well with our findings. In that study, measurements were performed in a similar position to the present study, taken just proximal to the insertion on the fifth metatarsal, as shown in Figure 3. 12
An accurate diagnosis of lateral intersection syndrome can be difficult due to the many pathological conditions that affect the peroneal tendons, such as tenosynovitis, tendon tear, tendinopathy, tendon dislocation or subluxation, hypertrophic peroneal tubercles, and the presence of painful ossicles.13,14 A great degree of clinical suspicion, a thorough physical examination, and utilization of MRI and point of care ultrasound are important in the differentiation of lateral intersection syndrome. Currently, there are no well-established criteria for diagnosing this condition due in large part to the lack of literature. In the author’s practice, it often serves as a diagnosis of exclusion, applied when imaging studies fail to identify a clear pathology, yet the patient’s symptoms persist despite conservative treatments.
As a cadaveric, anatomic study, there are inherent limitations. The first is the relatively small cohort of specimens. While the use of matched pairs is a strength, using a total of 8 specimens limits the ability to generalize the results. Additionally, cadaveric tissues inherently differ from native tissue, potentially impacting the results. Finally, this study is an anatomic, cadaveric study with the purpose of establishing baseline measurements. As such, there is a lack of direct clinical correlation until future studies can expand on these findings.
This study provides additional anatomical insights into the lateral intersection syndrome of the foot, a condition with limited existing literature. Our findings add to the literature by continuing to establish a baseline for the anatomic structures associated with this pathology. Due to the uncommon nature of this pathology, this study should serve as a building block for further research and clinical understanding, with the hope that this brings increased awareness to this rare condition. The authors recommend future studies on this topic, including larger cadaveric studies and clinical imaging studies, to add to the sparse literature.
Footnotes
Acknowledgements
The authors recognize the support Medline Unite Foot and Ankle for sponsoring the Chicago Anatomic Research Symposium by providing the cadaveric specimens and the lab. No financial compensation was provided to the investigators for this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors did not use generative AI or AI-assisted technologies.
Ethics/IRB and Consent
The authors state that every effort was made to follow all local and international ethical guidelines and laws that pertain to the use of human cadaveric donors in anatomical research. As a cadaveric study, no IRB review was required.
Trial Registration
This is not a randomized trial—Cadaveric research.