
Abstract
Background
The effectiveness of arthroscopic ankle surgery for chronic ankle conditions, including pain intensity, functionality, and success rates, remains uncertain.
Methods
PubMed, Scopus, and Web of Science databases were searched until October 2023. Mean differences (MDs) were calculated for pain reduction and functional improvements, and arthroscopy success rates were determined using a random-effects model.
Results
In total, 47 studies were included, encompassing 2,653 patients. Arthroscopic surgery resulted in a significant decrease in pain intensity for osteochondral lesions (MD = −4.49, P = .002) and ankle osteoarthritis (MD = −2.88, P = .034). Functional improvements were observed with notable success rates: 92.5% (soft tissue impingement), 87.5% (ankle synovitis), 73.2% (osteochondral lesions), 71.53% (bony impingement), and 54.7% (ankle osteoarthritis).
Conclusion
Arthroscopic ankle surgery proves effective, particularly for osteochondral lesions and impingement conditions, offering good outcomes in terms of pain reduction and functionality. However, the limited quality of available evidence calls for cautious interpretation of these results.
Level of Evidence:
Meta-analysis of studies with level of evidence III and IV
“Arthroscopic ankle surgery proves effective, particularly for osteochondral lesions and impingement conditions, offering good outcomes in terms of pain reduction and functionality.”
Introduction
Ankle disorders are frequent sources of pain and disability, with a prevalence of nearly 15% in middle-aged and older adults. 1 Chronic ankle pain often involves the injury of intra-articular structures, including osteochondral lesions, osteoarthritis (OA), or bony and/or soft tissue impingement. While these conditions can be managed conservatively, they may require surgical intervention if conservative treatment fails. However, there is currently no consensus on the optimal surgical approach for these disorders. Among the different surgical options that exist for the management of chronic ankle conditions, arthroscopy is probably the most widely used method of treatment compared to traditional open approaches 2 since it is a minimally invasive procedure, with low complication rates.3,4 and because recovery and return to activities are generally faster.5-7
Ankle arthroscopic surgery has been shown to be successful for the treatment of intra-articular osteophytes, chondral defects, and loose bodies.8,9 However, despite being commonly used, multiple questions still remain unanswered, such as how long do effects last, or what are the rates of success for the broad array of intra-articular chronic conditions of the ankle? Understanding the long-term effects on pain and functionality, and the success rate of arthroscopic surgery for different chronic ankle conditions is undoubtedly important for patients, surgeons, and policymakers, since these procedures have harms and costs that could outweigh beneficial effects.
To date, evidence to accurately assess the effectiveness of arthroscopic surgery for the management of chronic ankle conditions has been poorly conducted and reported. Previous reviews have investigated the usefulness of arthroscopic debridement, drilling, microfracture, or curettage in some conditions such as ankle impingement, ankle OA, or osteochondral lesions finding promising results. 5 ,10-13 However, all these reviews are qualitative in nature and have not quantified the success rates of these techniques or the mid-to-long-term clinical effects in other chronic conditions. Thus, to tackle these critical evidence gaps, the present study sought to quantify the mid-to-long-term effects on pain intensity and functionality in patients who underwent arthroscopic surgery and to estimate success rates of these procedures for ankle conditions by performing a systematic review and meta-analysis of ankle arthroscopic surgery studies.
Methods
The present systematic review and meta-analysis was developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 14 The study was submitted to the International Prospective Register of Systematic Reviews (PROSPERO) (registration number: CRD42023397621). The entire process from literature selection to data extraction was performed independently by 2 authors with the assistance of a professional librarian. Any disagreements were resolved through consensus.
Selection Criteria
To be eligible for inclusion in the meta-analysis, studies needed to meet the following criteria: (1) participants: individuals with a chronic ankle condition (ie, osteochondral lesions of the talus, soft tissue impingement, bony impingement, ankle OA, osteochondritis dissecans, chondral defects of the talar dome, cystic lesions, synovitis, osteophytes, loose bodies); (2) exposure: ankle arthroscopy technique (including debridement, curettage, drilling, removal of loose bodies, microfracture, synovectomy, or bone marrow stimulation); (3) outcomes: pain intensity, disability, satisfaction, and surgical complications; and (4) study design: cohort studies, case series, and randomized controlled trials. Studies were excluded if (1) did not report data regarding the variables of interest or (2) reported insufficient information for calculating prevalence and/or effect size and 95% confidence intervals (CIs).
Search Strategy
Two authors systematically searched MEDLINE, Web of Science, and Scopus electronic databases for articles from inception to October 2023. A librarian was consulted to audit the quality of the search. In addition, reference lists of eligible studies were hand-searched. The following search terms were used: ankle; impingement; talus; talar; tibiotalar; osteophy*; arthrosc*; surgery; osteoarthritis; debridement; curettage; drill*; and bone marrow stimulation (full search strategies for each database can be found in Supplementary Material 1). Searching was restricted to published articles in the English and Spanish languages.
Data Collection Process and Data Items
The extracted data from the articles meeting the selection criteria included the following information: (1) study characteristics (the first author’s name, publication year, enrollment year, study location, sample size, and study design); (2) participants’ information (sex, age, condition, duration of symptoms, sports participation, previous traumas, and size of the lesion); (3) measurements details (pain intensity assessment, functional assessment, satisfaction, and complications); and (4) analysis and study results (outcome of interest and main results). We requested from the study authors any effect sizes that were missing from the original published papers.
Risk of Bias in Individual Studies
The Quality Assessment Tool for Case Series Studies was used to evaluate the risk of bias. The checklist is composed of 9 items. Each item of methodological quality was classified as “yes,” “no,” or “not reported.” Depending on the final score, each study was deemed to be good (>8 points), fair (4-7 points), or poor (<4 points).
Summary Measures
We chose mean differences (MDs) and standardized MDs (Hedges’ g) as the main effect sizes for the present meta-analysis. We used baseline and last follow-up endpoints for pain intensity and American Orthopaedic Foot and Ankle Society (AOFAS) scores of each study to calculate the MD and standardized MD effect size estimates. These were entered along with the corresponding standard errors, and the software was set to produce pooled g values with 95% CIs using random-effects with the Hartung-Sidnapp adjustment. As a rule of thumb, the pooled effect size for g was classified as small (0.2), moderate (0.5), or large (0.8). 15 All analyses were performed using the admetan routine 16 within version 17 of STATA (STATA Corp., College Station, Texas). A P-value of <.05 was considered a threshold for statistical significance. In addition, the prevalence of success after ankle arthroscopic surgery across studies was pooled by applying a random-effects model that displayed the results as forest plots using the DerSimonian and Laird method (metaprop procedure 16 ). The Clopper-Pearson method was used to establish CIs for prevalence from the selected individual studies, 17 and a Freeman-Tukey transformation was used to normalize the results before calculating the pooled prevalence. 18
Synthesis of Results
For each meta-analysis, heterogeneity across studies was calculated using the total variance (Q), the degrees of freedom (df), and the inconsistency index (I2), 19 considering I2 values of <25%, 25% to 75%, and ≥75% as small, moderate, and high heterogeneity, respectively. 20 Sensitivity analyses were conducted to ascertain whether any single study with extreme results had an undue influence on the overall findings.
Risk of Bias Across Studies
The presence of potential small-study effects due to publication bias was analyzed using the Luis Furuya-Kanamori (LFK) index and the Doi plot. Values of –1, between –1 and –2, and >–2, are considered to represent no, minor, and major asymmetry, respectively. 21
Results
Study Selection
In total, 50 studies met the inclusion criteria and were included in the systematic review, although only 41 were included in the meta-analysis (the full list of excluded studies can be found in Supplementary Material 2). The PRISMA flow diagram displaying the number of studies excluded at each stage of the systematic review and meta-analysis is shown in Figure 1.
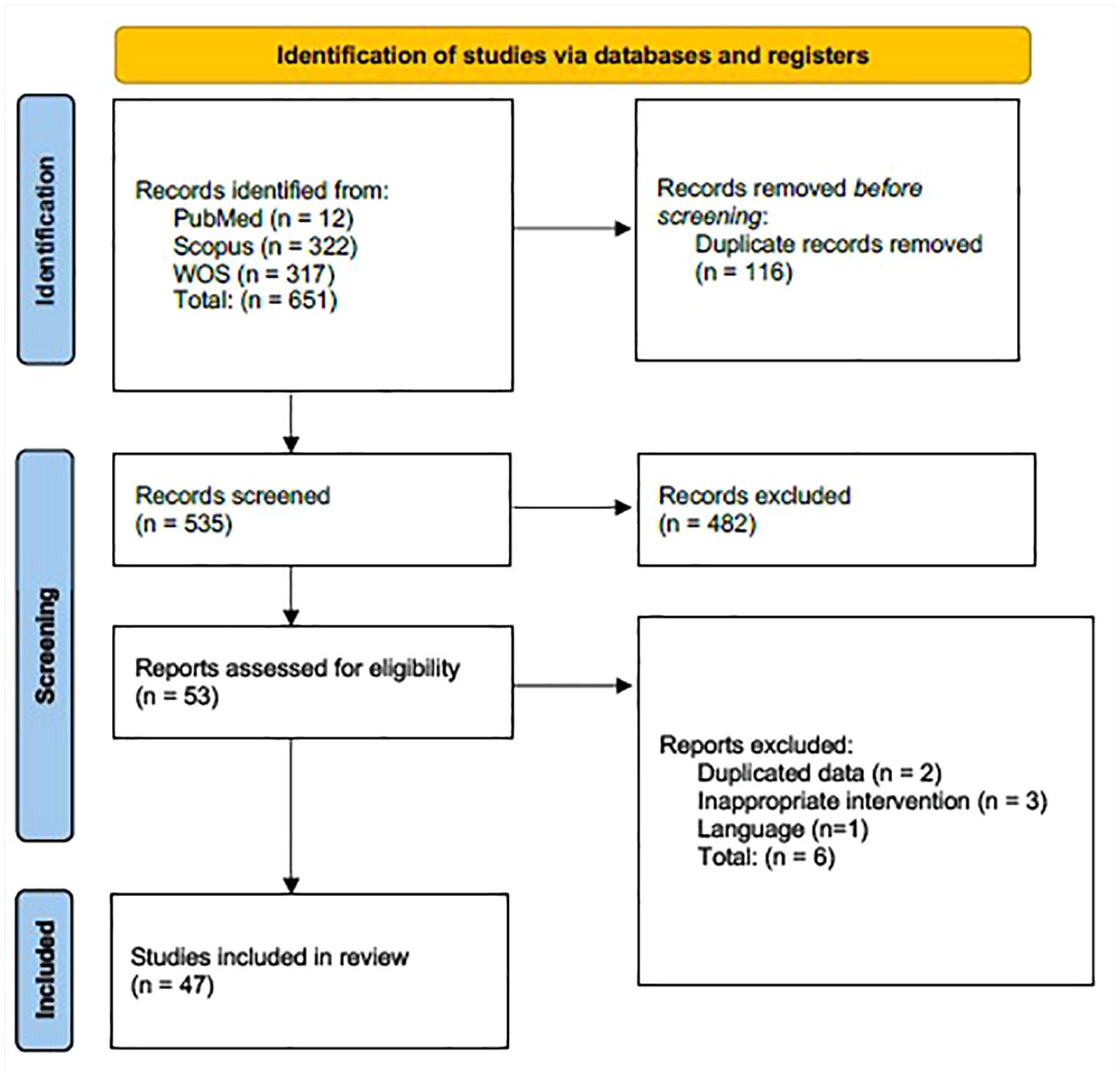
PRISMA flow diagram of literature search and study selection.
Study Characteristics
The main characteristics of the 47 included studies are summarized in Table 1. The included studies involved a total sample of 2653 patients with mean ages ranging from 25 22 to 53.7 years 23 (mean age = 33.3 years). Sample sizes across studies ranged from 9 24 to 300 participants, 25 and follow-up duration ranged from 12 26 to 104 months 27 (mean follow-up length: 42.5 months). Mean duration of symptoms before surgery ranged from 8 months 22 to more than 10 years, 28 although most studies did not report this information.
Characteristics of the Included Studies.
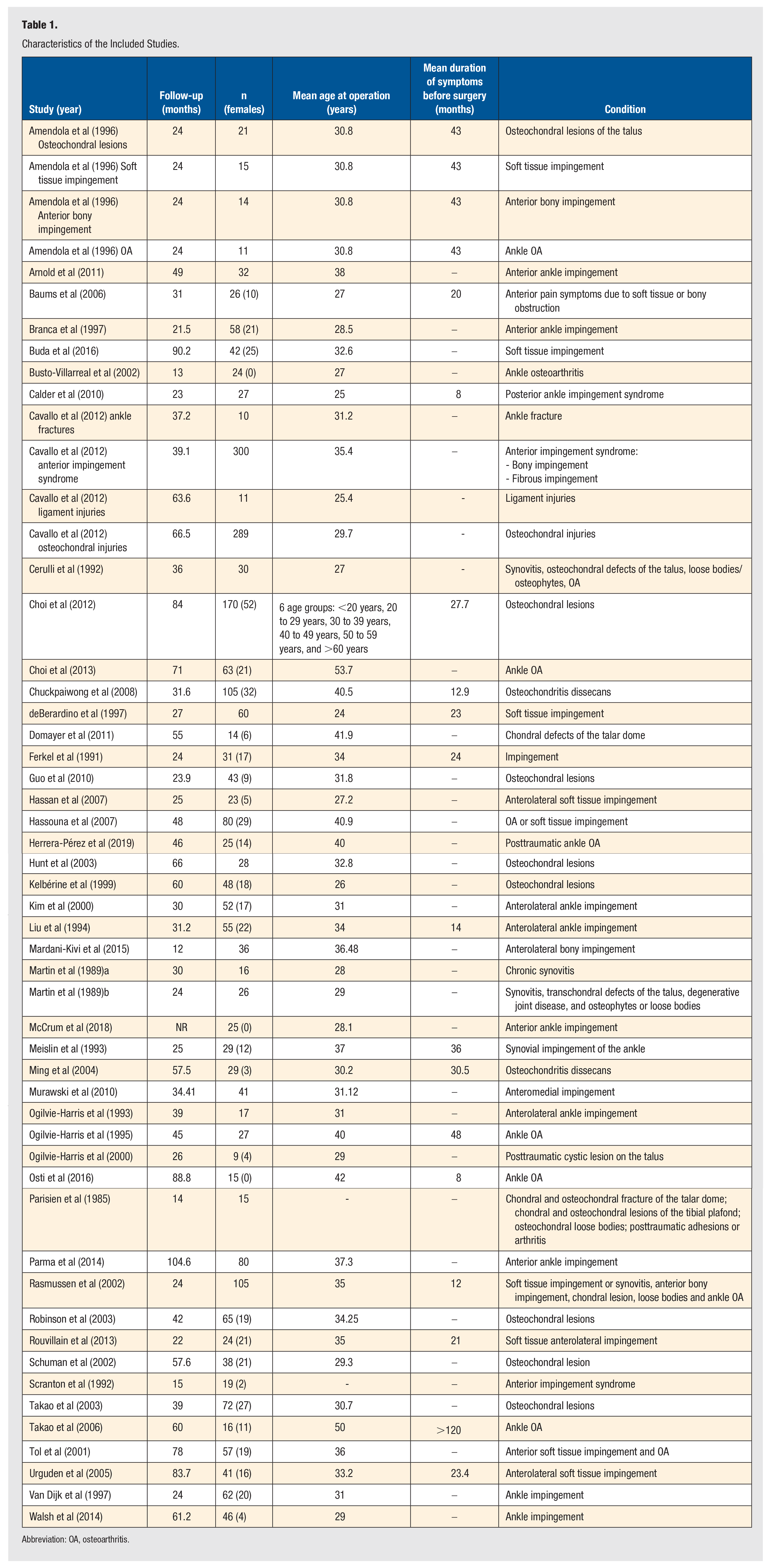
Abbreviation: OA, osteoarthritis.
Measurements
Regarding the outcomes assessment, pain intensity and functionality were evaluated homogeneously with the visual analogue scale (VAS) and the AOFAS Ankle-Hindfoot score. Methods to determine surgical success were more heterogeneous, including the use of the West Point Ankle score, modified versions of the McGuire score, McCullough score, Martin score, Kitaoka score, Ogilvie-Harris score, Meislin’s criteria, need for surgery due to recurrence of symptoms, patient satisfaction, and, in some cases, treatment was considered successful when 3 of 4 criteria were fulfilled: (1) more than 50% improvement in VAS score for pain during daily activities, (2) more than 50% improvement in VAS score for pain during exercise, (3) an AOFAS score that was increased by at least 30 points, and (4) a Roles and Maudsley score of 1 or 2.
Risk of Bias Within Studies
All 47 studies met at least 4 criteria and were considered to have fair methodological quality. The average score was 6.125/9 (Supplementary Material 3).
Synthesis of Results
Figures 2 to 4 show the synthesis of results. Figure 2 illustrates the pooled change from baseline to 24 to 88 months postoperatively in mean pain score. Arthroscopic surgery for osteochondral lesions showed a statistically significant decrease of 4.49 cm on a 0 to 10 cm VAS (MD = −4.49, 95% CI = −4.57 to −4.42; I2 = 0.0%; P = .002) and 2.88 cm in ankle OA (MD = −2.88, 95% CI = −4.93 to −0.83; I2 = 69.81%; P = .034).
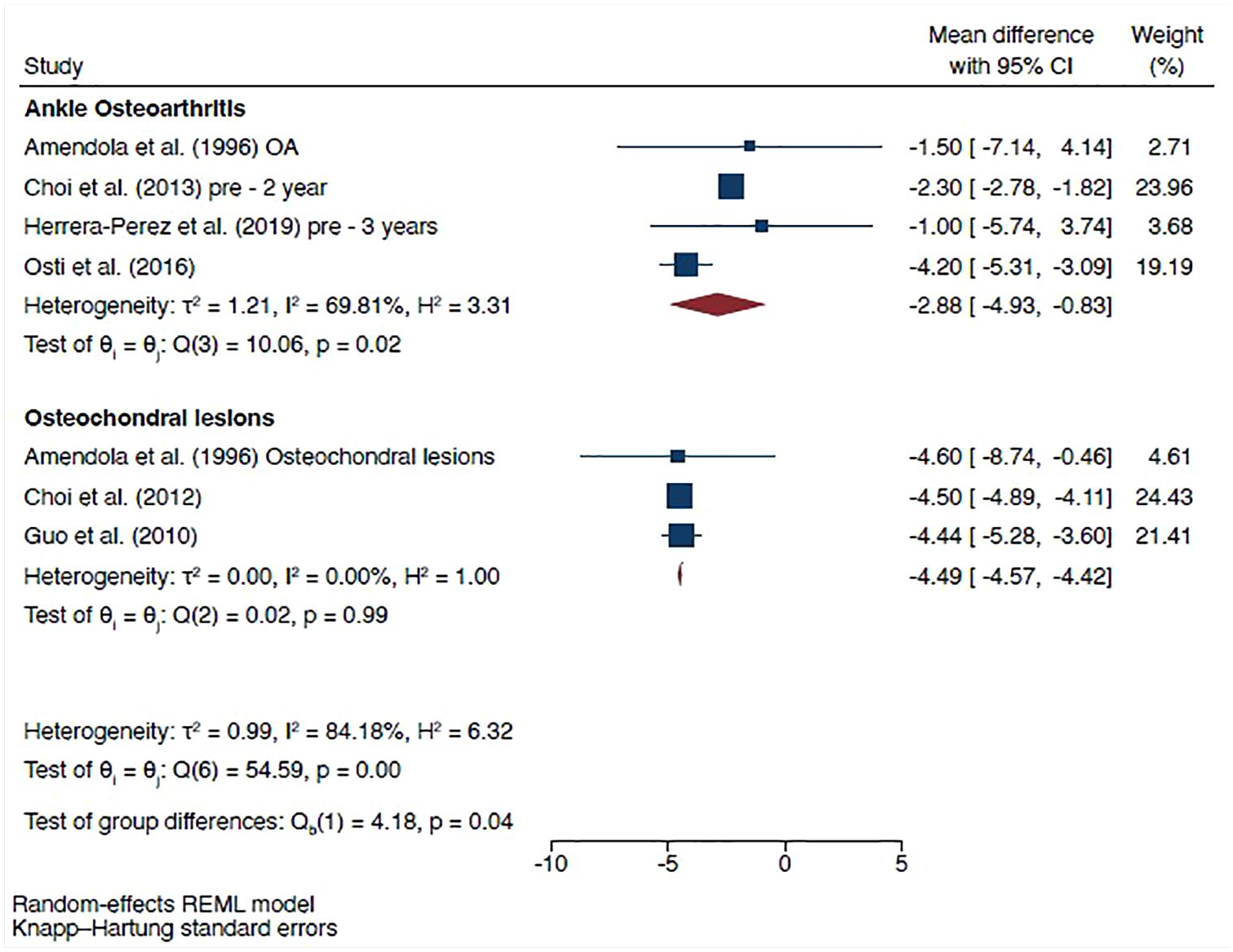
Forest plot showing the pooled mean difference change with a 95% confidence interval from baseline to 24 to 88 months postoperatively in the visual analogue scale (0 to 10 cm), for ankle osteoarthritis and osteochondral lesions.
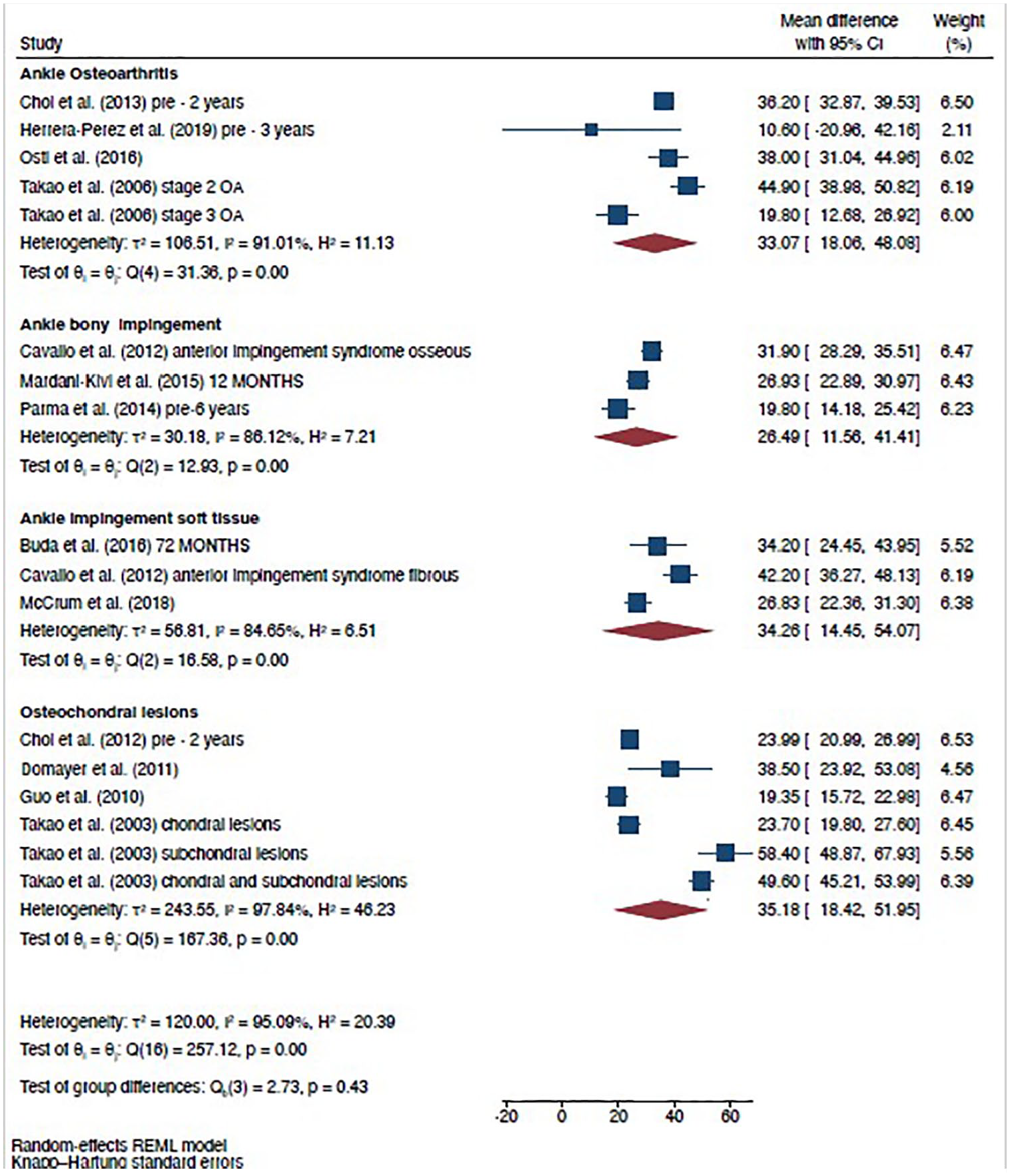
Forest plot showing the pooled mean difference change with 95% confidence interval from baseline to 12 to 88 months postoperatively in the AOFAS Ankle-Hindfoot Scale for ankle osteoarthritis, ankle bony impingement, ankle impingement soft tissue, and osteochondral lesions.
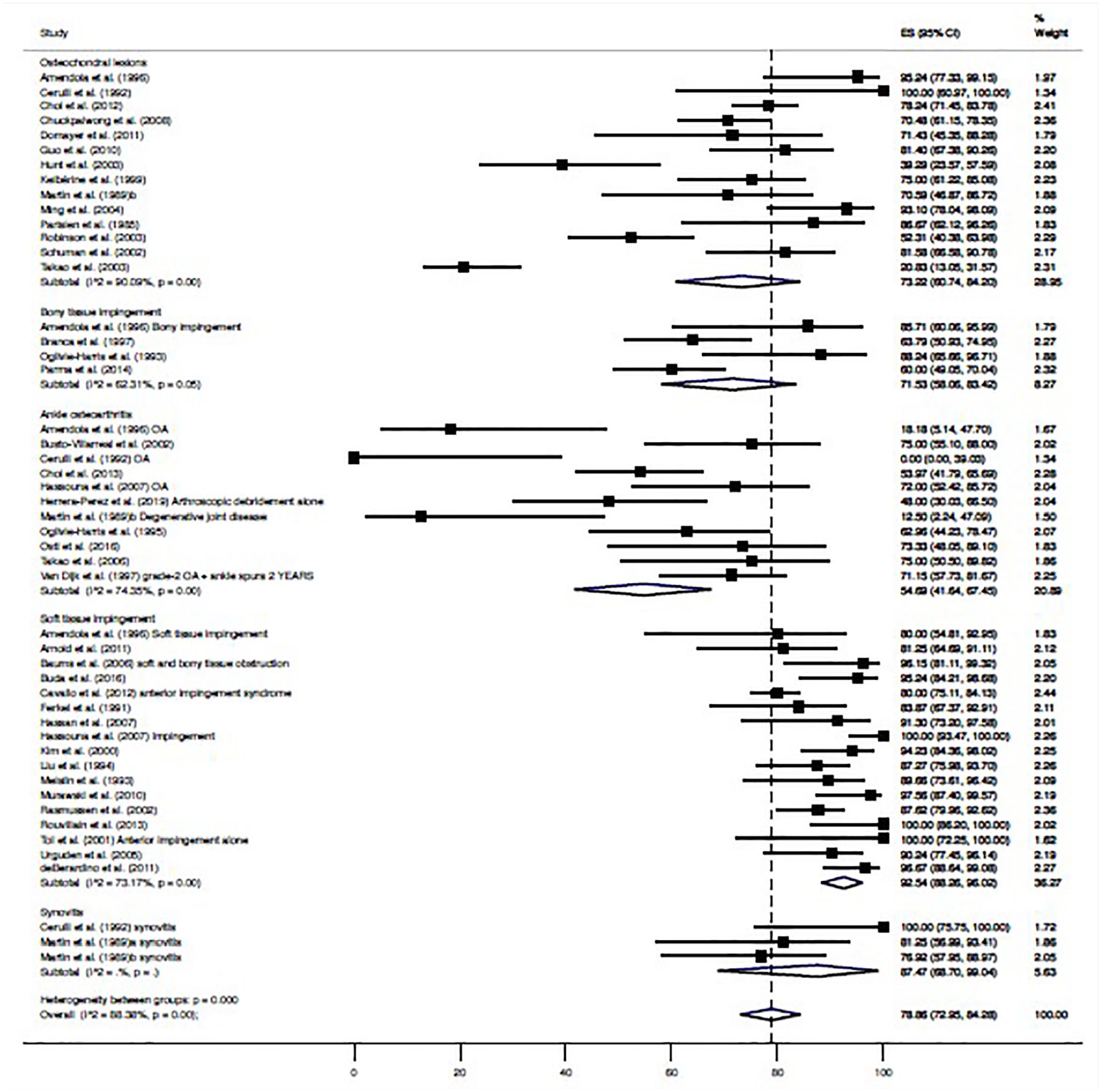
Forest plot showing the pooled prevalence and its 95% confidence interval of having good-to-excellent outcomes following ankle arthroscopy for osteochondral lesions, bony tissue impingement, soft tissue impingement, and synovitis.
Figure 3 shows the pooled MDs from baseline to 12 to 104.6 months in the AOFAS Ankle-Hindfoot Scale, showing a statistically significant increase in patients with osteochondral lesions (MD = 35.18, 95% CI = −18.42 to 51.95; I2 = 97.84%; P = .003), soft tissue impingement (MD = 34.26, 95% CI = 14.45 to 54.07; I2 = 84.65%; P = .024), ankle OA (MD = 33.07, 95% CI = 18.08 to 48.08; I2 = 91.01%; P = .003), and ankle bony impingement (MD = 26.49, 95% CI = 11.56 to 41.41; I2 = 86.12%; P = .017).
As shown in Figure 4, 92.5% of arthroscopic surgeries for soft tissue impingement were deemed good-to-excellent, 87.5% for synovitis, 73.2% for osteochondral lesions, 71.53% for bony tissue impingement, and 54.7% for ankle OA.
No asymmetry suggestive of small-study effects (LFK index = −0.99) was detected. Sensitivity analyses indicated no modifications in the results after removing 1 study at a time. Based on meta-regression analyses, no significant effects of length of follow-up (β = 0.02; 95% CI = −0.000 to 0.005; P = .076) were found (Supplementary Material 4), but significant effects were detected with age (β = −0.02; 95% CI = −0.036 to 0.000; P = .046) (Supplementary Material 5).
Discussion
The present study aimed to examine the clinical effectiveness of ankle arthroscopy derived from the available scientific literature, and to determine surgery success rates for the different chronic ankle conditions. Overall, arthroscopic surgery was found effective in improving clinical outcomes postoperatively with minimum follow-up ranging from 24 to 88.8 months for pain assessments and from 12 to 104.6 months for AOFAS assessments, although outcomes were not uniformly improved across the different chronic conditions. Despite the heterogeneity of definitions of success, rates of good-to-excellent results after surgery ranged from 54.7% for ankle OA to 92.5% for soft tissue impingement.
Current evidence indicates good-to-excellent results in more than 80% of patients following arthroscopic surgery for ankle impingement. 11 The rates observed in our study are slightly different from those observed by Gianakos et al, probably because they estimated the overall success rate for all anterior impingement studies, without distinguishing whether the impingement is due to bone or soft tissue. We found that ankle arthroscopic surgery was considered successful in 92% of patients with soft tissue impingement and in 71.5% of patients with bony tissue impingement. This could be because bony tissue impingement is caused by the presence of osteophytes that are formed frequently as a result of microtrauma or chronic instability and are generally accompanied by concomitant degeneration of the joint, which can limit arthroscopy effectiveness despite the impingement removal. 25 These differences were also observed in functionality, where patients with soft tissue impingement showed improvements of 34.3 points in AOFAS scores compared to 26.5 points in patients with bony ankle impingement.
Consistent with the literature, this study found that 73.2% of patients with osteochondral lesions had good-to-excellent results after arthroscopic surgery. In terms of function, osteochondral lesions showed the largest increases in AOFAS scores (35.2 points at a minimum of 2 years of follow-up), compared with the rest of chronic ankle conditions. Clinical outcomes for osteochondral lesions have been found to be influenced by the size of the lesion, previous surgeries, body mass index (BMI), age, 25 or duration of symptoms. 29 Some studies found the highest AOFAS scores at 12 months after the surgical procedure, 25 and some studies found excellent clinical results at last follow-up despite not improving magnetic resonance imaging (MRI) and arthroscopic findings. 30
Ankle OA was the condition showing the worst results, with only 54.7% of patients presenting good-to-excellent results at the last follow-up. While this rate might appear to be too low to recommend arthroscopic surgery to patients with ankle OA, long-term clinical outcomes revealed improvements in pain and function that should be considered when giving advice to these patients. While some studies support its use in mild to moderate cases and consider it safe, effective, and with satisfactory clinical results in selected patients,8,23,28 a previous review concluded that it is not effective and it should not be indicated, 5 based only on success rates from previous reports. From the available evidence, we observed that even in cases with severe cartilage degeneration, it might postpone major surgical procedures such as ankle arthrodesis or even joint replacement, providing a relief in symptoms during a reasonable amount of time. Other techniques, however, should be considered when discussing options for joint-preserving surgical treatment for ankle OA. For instance, the study by Herrera-Perez et al 31 compared arthroscopic debridement alone with hinged motion distraction and debridement. This study found that patients in the debridement-alone group had a higher pain level at the 3-year follow-up and a substantially higher rate of postoperative revision surgery, concluding that hinged motion distraction combined with debridement was a better option for delaying the progression of ankle degeneration, although the rate of major secondary procedures was high in both groups.
Although this study aimed to examine the available evidence on the effectiveness of arthroscopic surgery for chronic ankle conditions, effectiveness is highly influenced by other factors such as the experience and ability of the surgeon, specific patient populations, surgical techniques, lifestyle, and biological and individual factors, thus being difficult to analyze accurate estimates. Moreover, success rates can be a useful metric for evaluating the effectiveness of a particular procedure; however, there is no specific minimum success rate for recommending surgery, as this can vary depending on several factors. Surgery should only be considered when there is a reasonable chance of success, and when the potential benefits outweigh the risks and potential complications of the procedure. The optimum technique for the management of chronic ankle lesions is yet to be known; however, arthroscopic surgery is a promising procedure growing in popularity and in constant evolution that, together with the development of more specific devices for the ankle, will become more accessible and more effective over time.
Limitations and Strengths
The generalizability of these findings is subject to certain limitations. First, our results were limited by the lack of a uniformly accepted definition of success and failure after surgery, reflecting an inconsistency in the use of a standardized definition of surgery success, and thereby the use of diverse thresholds to detect patients with excellent or poor results after surgery. Thus, we cannot confirm that our pooled success rate reflects the true ankle arthroscopy effectiveness. Second, our results were limited by the scarcity of high-quality studies. In this regard, most studies were case series, which are studies descriptive in nature, have no comparator arm, and typically involve a small sample of patients who have a similar diagnosis or treatment. While this design can provide some useful information, it is subject to a range of biases and limitations, such as selection bias, confounding, and lack of control groups. These limitations can make it difficult to draw strong conclusions about the effectiveness or safety of ankle arthroscopy, and therefore may limit the generalization of our findings.
On the contrary, this study also has strengths that must be acknowledged. We believe the present study substantially adds to the information currently available in the literature regarding ankle arthroscopy, as it is the first study that quantifies the mid-to-long-term effects of arthroscopic interventions regarding pain and function and provides an estimate of its success rate across different ankle conditions. These measures can be complementary, as a surgery with a high success rate may not necessarily lead to a large improvement in pain or functionality, and vice versa. By including both measures in the meta-analysis, we provided a more comprehensive evaluation of the effectiveness of the surgery across different outcome domains, laying the groundwork for future research in the field.
Conclusion
Arthroscopic ankle surgery has been found to be effective in improving the clinical outcome of various chronic ankle pathologies. However, the success rates of this surgery can vary considerably depending on the specific diagnosis of the patient. Good results have been observed in cases of osteochondral lesions of the ankle and bony and/or soft tissue ankle impingement, while the results have been moderate in cases of ankle OA. Therefore, it is not justifiable to universally recommend this surgical technique, and it should be approached with caution.
Supplemental Material
sj-docx-1-fas-10.1177_19386400251345536 – Supplemental material for Mid-to-Long-term Clinical Outcomes of Ankle Arthroscopy on the Treatment of Chronic Ankle Conditions: Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-fas-10.1177_19386400251345536 for Mid-to-Long-term Clinical Outcomes of Ankle Arthroscopy on the Treatment of Chronic Ankle Conditions: Systematic Review and Meta-analysis by Mario Herrera-Pérez, Victor Valderrabano, Cesar de Cesar Netto, Eric I. Ferkel, Alexandre Leme-Godoy, Ali Dway, José Luis Pais-Brito and Sergio Tejero in Foot & Ankle Specialist
Footnotes
Acknowledgements
The authors of the study thank the authors of the included studies for their contribution to our study.
Author Contributions
MH-P contributed to the design, methodology, data acquisition, and writing – original draft preparation. VV, AD, CdCN, and EIF contributed to the methodology, formal analysis and interpretation of data, and supervision. AL-G and JLP-B contributed to the formal analysis and interpretation of data, and writing – review and editing. ST contributed to the methodology and supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This is a systematic review and meta-analysis, so it does not need ethical approval.
Informed Consent
This is a systematic review and meta-analysis, so it does not have direct patient information.
Institutional Review Board Statement
No ethical approval was required for this systematic review and meta-analysis since data were collected and synthesized from previous studies.
Trial Registration
The study was submitted to the International Prospective Register of Systematic Reviews (PROSPERO) (registration number: CRD42023397621).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.