
Abstract
Objective
To compare patient-reported outcomes and reintervention rates after open vs arthroscopic fusion of the ankle (TT—tibiotalar) or subtalar (ST) joint over a 10-year period in a cohort of patients from a single center.
Methods
In total, 129 patients (142 joints) underwent surgery for isolated TT or ST osteoarthritis between 2010 and 2020: 40 TT fusions (11 arthroscopic, 29 open) and 102 ST fusions (25 arthroscopic, 77 open). The course of treatment was followed clinically using patient-reported outcome measures (PROMs) for ankle function: Foot and Ankle Outcome Score—FAOS, general quality of life (European Quality of Life in Five Dimensions 3-level time-trade-off—EQ-5D 3L-TTO) and activity level (Tegner Activity Scale—TAS), and by tracking revision procedures.
Results
The median follow-up time was 8 (3–13) years. The mean age at the time of surgery was 52 (14) years. Most subjective scores showed significant improvement; cumulative FAOS improved from 41 to 57 in the TT group and from 41 to 67 in the ST group and EQ-5D from 0.40 to 0.55 (TT group) and from 0.38 to 0.60 (ST group), while TAS remained at 2. The ST fusion patients had better subjective outcomes than TT fusion patients. There were no significant differences in PROMs between arthroscopic and open procedures. Older age and preoperative FAOS pain were found to be negative predictors for the postoperative FAOS subscales. Overall, there was an 18% revision rate: 17 non-unions and 8 infections. In addition, 20 hardware removals were performed.
Conclusion
Isolated TT or ST fusions performed open or arthroscopically were safe and significantly improved function and quality of life and reduced joint-related pain but did not increase patients’ activity levels. Patients with ST fusion had a better subjective outcome. Older age and lower preoperative FAOS pain were associated with a worse postoperative subjective outcome.
Level of Evidence:
Level III
“Patients with st fusion had a better subjective outcome.”
Introduction
Osteoarthritis (OA) of the ankle joint (tibiotalar [TT]) and subtalar joint (ST) is less common than that of other large joints but can lead to severe functional limitations and a reduction in quality of life. 1 The main cause of TT or ST OA is trauma, which accounts for almost 80% of all cases. Other causes include joint arthropathies (rheumatoid arthritis, hemochromatosis, hemophilia, osteonecrosis), infections, tumors, and neuropathic diseases.2 -4 Only about 10% of OA of the TT or ST joint is of primary origin.
As with all OA, initial treatment is based on conservative treatment. Motion adjustment, physiotherapy, weight reduction, braces, and orthoses are used in combination with non-steroidal anti-inflammatory drugs and intra-articular injections (corticosteroid, hyaluronic acid, etc). 5 If conservative options fail, surgery is indicated. Many treatment options are possible: debridement and osteophyte reduction, osteotomies, arthroplasty, and fusion. Although ankle arthroplasty has become increasingly common in recent years thanks to new implant designs and techniques, fusion remains the mainstay for the definitive treatment of end-stage TT and ST joint degeneration. 6
Indications for TT and/or ST fusion include end-stage arthritis with joint degeneration, avascular necrosis, Charcot neuroarthropathy, flat foot deformity, tarsal coalition, and failure of total ankle replacement. 7 Since the introduction of open TT fusion in 1897 by Albert, 8 many techniques have been described that have provided good results, so that the open technique is still the standard treatment option.9,10 However, arthroscopic procedures for both joints are becoming increasingly popular as they lead to similar outcomes. These include comparable fusion rates, operative time and PROMs with faster union, shorter hospital stay, fewer complications, and less short-term postoperative pain.6,11 The choice between different surgical approaches depends on several factors, including patient characteristics (bone and soft tissue quality, comorbidities), extent of surgery required (alignment deformities, concomitant procedures), and surgeon experience.12 -14
The aim of the study was to compare patient-reported outcomes and reintervention rates in a cohort of patients who underwent isolated TT or ST fusion surgery, employing either an open or arthroscopic approach, for the treatment of end-stage OA at a university-based orthopedic referral center over a 10-year period. Demographic, surgical, and radiologic covariates were analyzed for their potential impact on treatment outcomes. We hypothesized the following: Both groups would improve significantly from preoperative levels, postoperative function would be better after ST fusion than after TT fusion, and reintervention rates would be in the 20% range.
Materials and Methods
Study Design
This is a retrospective analysis of prospectively collected data from adult patients treated with isolated, open, or arthroscopic TT or ST joint fusion at a university-based orthopedic referral center. The study was approved by the National Medical Ethics Committee (approval no. #0120-99/2019/4). Patients over 18 years of age who had undergone open or arthroscopic TT and/or hindfoot fusion surgery between 2010 and 2020 were included. Informed consent was obtained from all participants prior to inclusion. Non-reconstructive procedures such as Achilles tendon lengthening (TAL), valgus/varus corrective osteotomies of the calcaneus, forefoot surgery, or osteophyte removal were allowed and recorded. Patients were excluded from the study if they underwent other concurrent reconstructive procedures, such as metatarsal or forefoot fusion, TT and hindfoot ligament reconstruction, if they had systemic or neurologic conditions that could affect the musculoskeletal system, or if they were unwilling to participate in the study. All procedures were performed by a single surgeon, one of the co-authors, who has more than 10 years of experience in foot and ankle surgery.
Surgical Intervention
During the observed timeframe, 129 of 275 patients (involving 142 joints) who underwent isolated TT or ST fusion met the inclusion criteria. Each fusion was considered a separate entity. The cohort included 40 cases of isolated TT fusion (11 arthroscopic, 29 open) and 102 cases of isolated ST fusion (25 arthroscopic, 77 open).
The procedures were performed under general anesthesia or spinal anesthesia. All open fusions were performed via an anterior approach for the TT joint and a lateral approach for the ST joint. For arthroscopic TT fusion, the standard arthroscopic portals for anterior ankle arthroscopy were used, while a posterior arthroscopic approach was chosen for ST fusion. Cartilage removal, subchondral bone perforation, soft tissue release, and osteophyte resection were performed. In addition, corrective calcaneal osteotomy and TAL were performed when deemed necessary to achieve the desired joint position (neutral flexion, 0-5° hindfoot valgus, 5-10° external rotation for TT fusion; 5-10° calcaneal valgus for ST fusion). The position of the ankle joint was maintained either with 2 to 3 cannulated screws inserted percutaneously during arthroscopic surgery or with 2 screws and a precontoured anterior locking plate during open surgery. In both surgical techniques, the ST joint was fixed with 2 percutaneously inserted, cannulated screws from the tip of the heel to the talar neck, which also stabilized a possible concomitant calcaneus osteotomy. All fixation methods were fluoroscopically controlled and monitored. The accompanying interventions were documented.
Postoperatively, all patients followed a similar, standardized rehabilitation protocol. They were placed in a non-weight-bearing cast with crutches until the first follow-up examination after 4 weeks. After that, the immobilization was exchanged for a rigid walking boot, and weight bearing as tolerated was allowed. If the X-rays and clinical examination indicated successful fusion after 8 weeks, the boot and crutches were removed and the patients began to bear full weight in standard shoes. In case of doubt, a follow-up computed tomography (CT) scan was performed, and if fusion was not confirmed, immobilization was extended for another 4 to 6 weeks, or a decision on revision surgery was discussed. Immediately after surgery, continuous passive motion excluding the fused joint, isometric exercises, electrostimulation, and cryotherapy were started. This was followed by physiotherapy, and a return to moderate-intensity activities after immobilization was lifted. After 6 months, rehabilitation was considered complete, and patients were able to resume full activities within the functional status of the treated joint.
Clinical and Radiological Evaluation
Patient demographics (age, gender, body mass index—BMI), medical history (general health, duration of symptoms, smoking, primary/revision surgery), preoperative clinical status and native radiographs of the foot and ankle and PROMs for ankle function: Foot and Ankle Outcome Score (FAOS), general quality of life (European Quality of Life in Five Dimensions 3-level time-trade-off [EQ-5D 3L-TTO]), and Visual Analogue Scale (EQ-VAS), as well as activity level (Tegner Activity Scale [TAS]) were recorded preoperatively and stored in a hospital database. The FAOS and the TAS were translated (and back-translated) into Slovenian and had already been used in several studies,15,16 while the European Quality of Life in Five Dimensions (EQ-5D) had been validated for the Slovenian population.17,18 A country-specific EQ-5D 3-level score (EQ-5D 3L-TTO) based on the time-trade-off (TTO) was established to determine the index numbers corresponding to the 5-digit score of the patients’ health conditions. The native radiographs were analyzed for TT and ST joint alignment (kite angle, Meary’s angle, calcaneal pitch) and OA (modified Kellgren-Lawrence criteria for ankle joints, grade 0–4; osteophyte formation and joint space narrowing for ST joints, grade 0–3). Fusion rates were assessed clinically and from postoperative radiographs or, if necessary, by CT scan. Postoperative revision procedures were recorded and categorized into one of 5 categories: none, non-union, infection, hardware removal, and other. The final subjective re-evaluation was performed using the same PROMs, as was the use of analgesics by post or mail. The details are shown in Table 1.
Patient Demographics, Medical History, and Operative Details for All 142 Cases Enrolled in the Study.
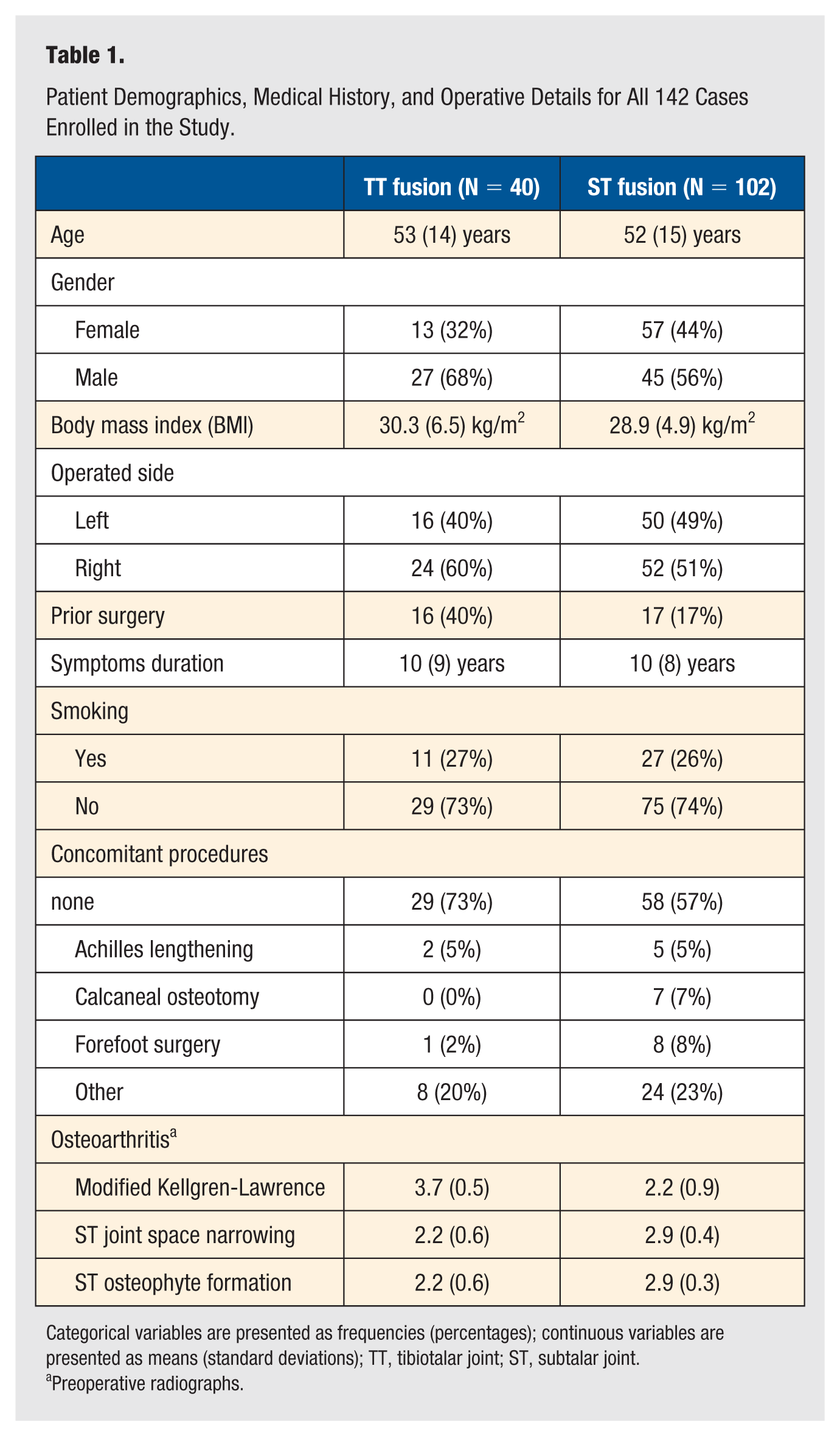
Categorical variables are presented as frequencies (percentages); continuous variables are presented as means (standard deviations); TT, tibiotalar joint; ST, subtalar joint.
Preoperative radiographs.
Statistical Analysis
Descriptive statistics are used for patient demographics, medical history, and operative details of all 142 cases. Categorical variables are presented as frequencies with associated percentages, and continuous variables as means with standard deviation (SD). Follow-up times and TAS are presented as medians (min–max). Paired t-tests or Wilcoxon signed-rank tests were used to compare preoperative and postoperative differences (Δ) for all PROMs. These differences were additionally compared between the open and arthroscopic groups using 1-way analysis of variance (ANOVA). The postoperative PROMs were further analyzed using linear regression models to examine the associations between the predictors, including the corresponding preoperative PROM value. Statistical analyses were performed using SPSS software (version 23.0; IBM, Chicago, Illinois). The level for statistical significance was set at P < .05. The FAOS cumulative was defined as the primary study outcome; a post-hoc analysis yielded a power of 0.99 (effect size 0.45) (G*Power Ver 3.1.9.4, University of Kiel, Germany).
Results
Both genders were equally represented—65 male and 64 female patients. The average age at surgical intervention was 52 (14) years. The median follow-up time of the patients was 8 (3-13) years (7 in the TT group and 8 in the ST group). Most procedures were done as an open surgery—106 (29 in the TT group and 77 in the ST group), while 36 were performed arthroscopically (11 in the TT group and 25 in the ST group).
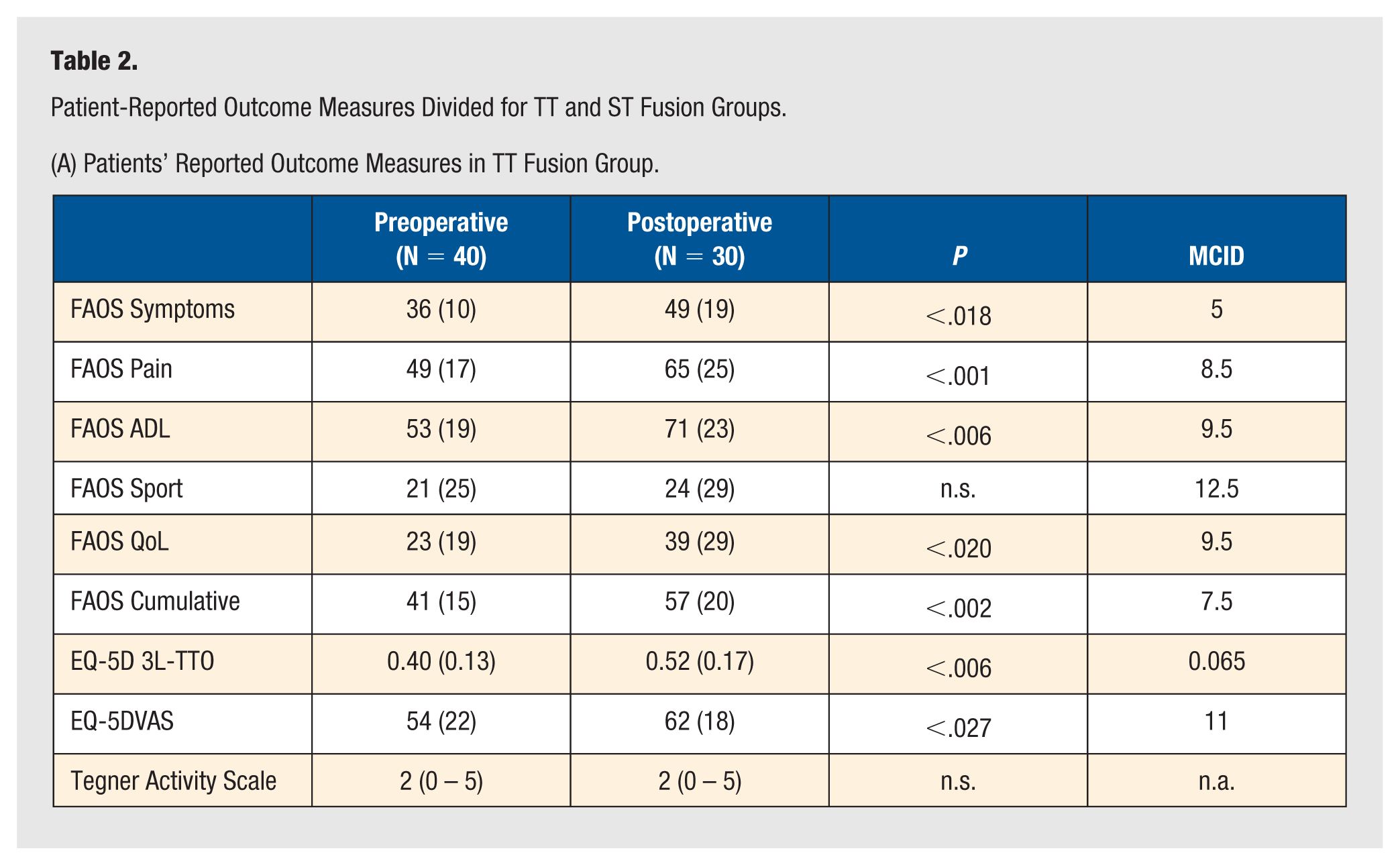
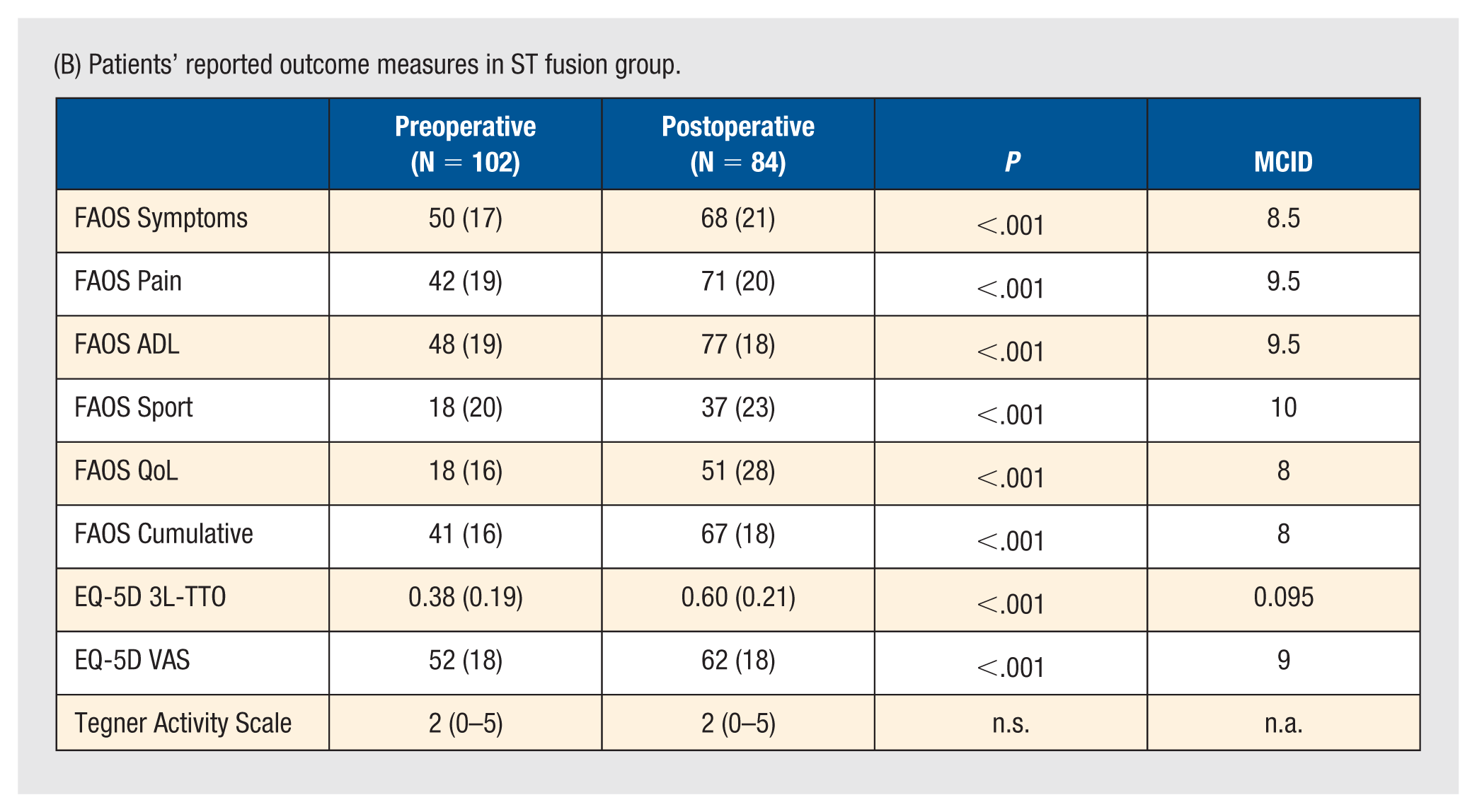
Postoperative PROMs were obtained from 114/142 cases (30 TT and 84 ST group), corresponding to a response rate of 80%. All postoperative patient-related outcome measures showed a significant improvement compared to preoperative values, with the exception of FAOS sport in the TT fusion group and TAS in both groups. The mean preoperative FAOS cumulative score was 41 in both the TT and ST groups; at follow-up, scores showed significant improvement: 57 in the TT group (55 in the arthroscopic and 59 in the open group) and 67 in the ST group (72 in the arthroscopic and 65 in the open group). The analysis of the EQ-5D 3L-TTO scores showed an improvement in both groups, in the TT group from 0.40 to 0.55 (0.57 in the arthroscopic group and 0.51 in the open group) and in the ST group from 0.38 to 0.60 (0.65 in the arthroscopic group and 0.60 in the open group). The preoperative VAS score was 54 in the TT group and 52 in the ST group. Pain relief was achieved in both groups, with a postoperative VAS score of 62 in both the TT and ST groups. There were no significant differences in PROMs depending on the type of surgical procedure (arthroscopic vs open). However, when comparing the fused joints (TT vs ST fusion), a statistically significant higher improvement in FAOS cumulative, FAOS symptoms, and FAOS quality of life was found in the ST fusion group. No improvement was found when analyzing TAS, which remained at 2. Multivariate linear regression models revealed a negative correlation between older age and postoperative FAOS cumulative, FAOS symptoms, and FAOS quality of life. Lower preoperative FAOS pain scores were also a strong negative predictor of FAOS cumulative, FAOS ADL, and FAOS sports. Shorter symptom duration had a negative effect on postoperative FAOS quality of life. Full details of these data can be found in Tables 2 and 3 and in Figures 1 and 2.
Patient-Reported Outcome Measures Divided for TT and ST Fusion Groups.
(A) Patients’ Reported Outcome Measures in TT Fusion Group.
(B) Patients’ reported outcome measures in ST fusion group.
(C) Patients’ Reported Outcome Measures Compared Depending on the Type of Surgical Technique.
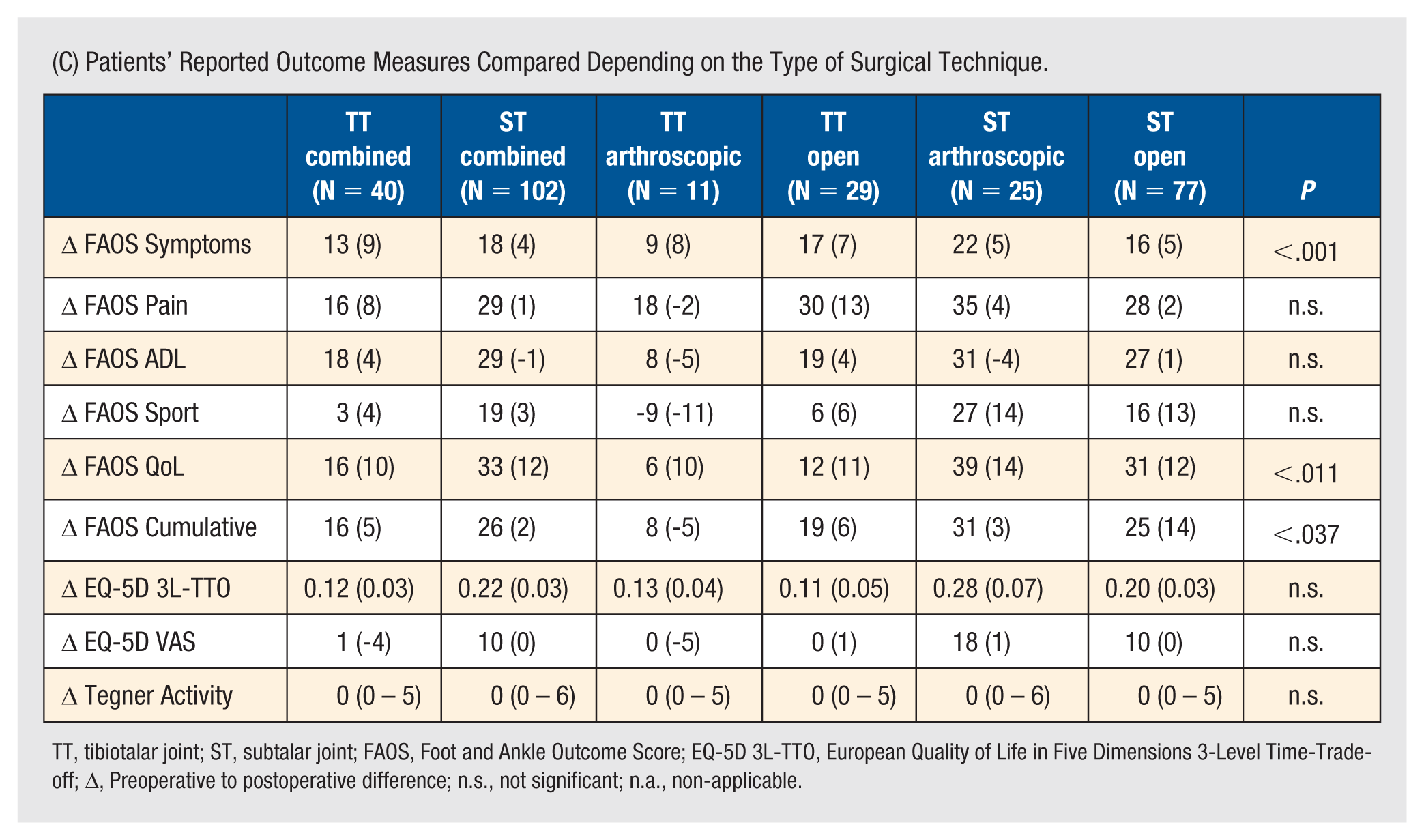
TT, tibiotalar joint; ST, subtalar joint; FAOS, Foot and Ankle Outcome Score; EQ-5D 3L-TTO, European Quality of Life in Five Dimensions 3-Level Time-Trade-off; Δ, Preoperative to postoperative difference; n.s., not significant; n.a., non-applicable.
Regression Models for Correlation Between Predictors and Postoperative Values of Patient-Reported Outcome Measures.
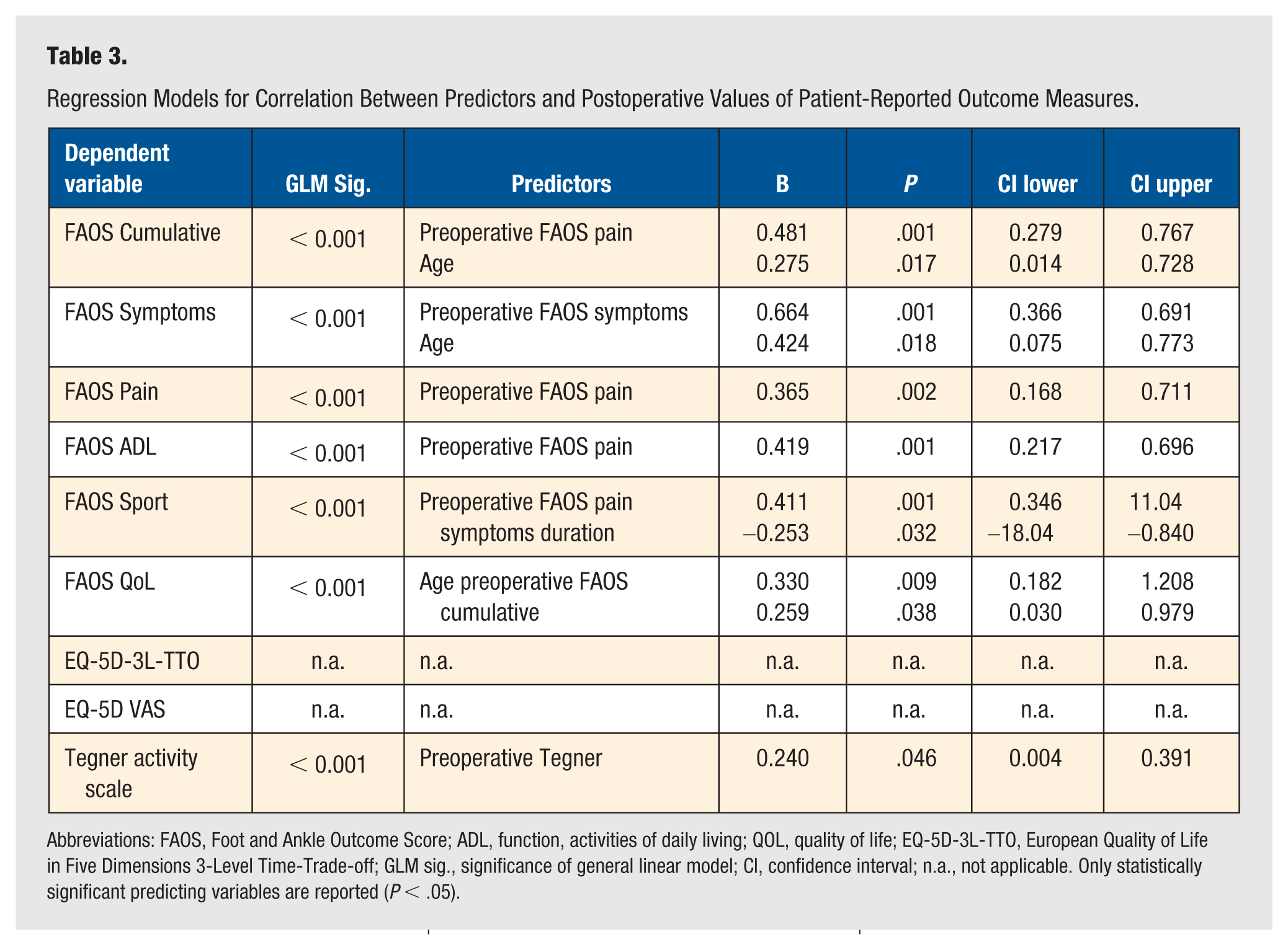
Abbreviations: FAOS, Foot and Ankle Outcome Score; ADL, function, activities of daily living; QOL, quality of life; EQ-5D-3L-TTO, European Quality of Life in Five Dimensions 3-Level Time-Trade-off; GLM sig., significance of general linear model; CI, confidence interval; n.a., not applicable. Only statistically significant predicting variables are reported (P < .05).
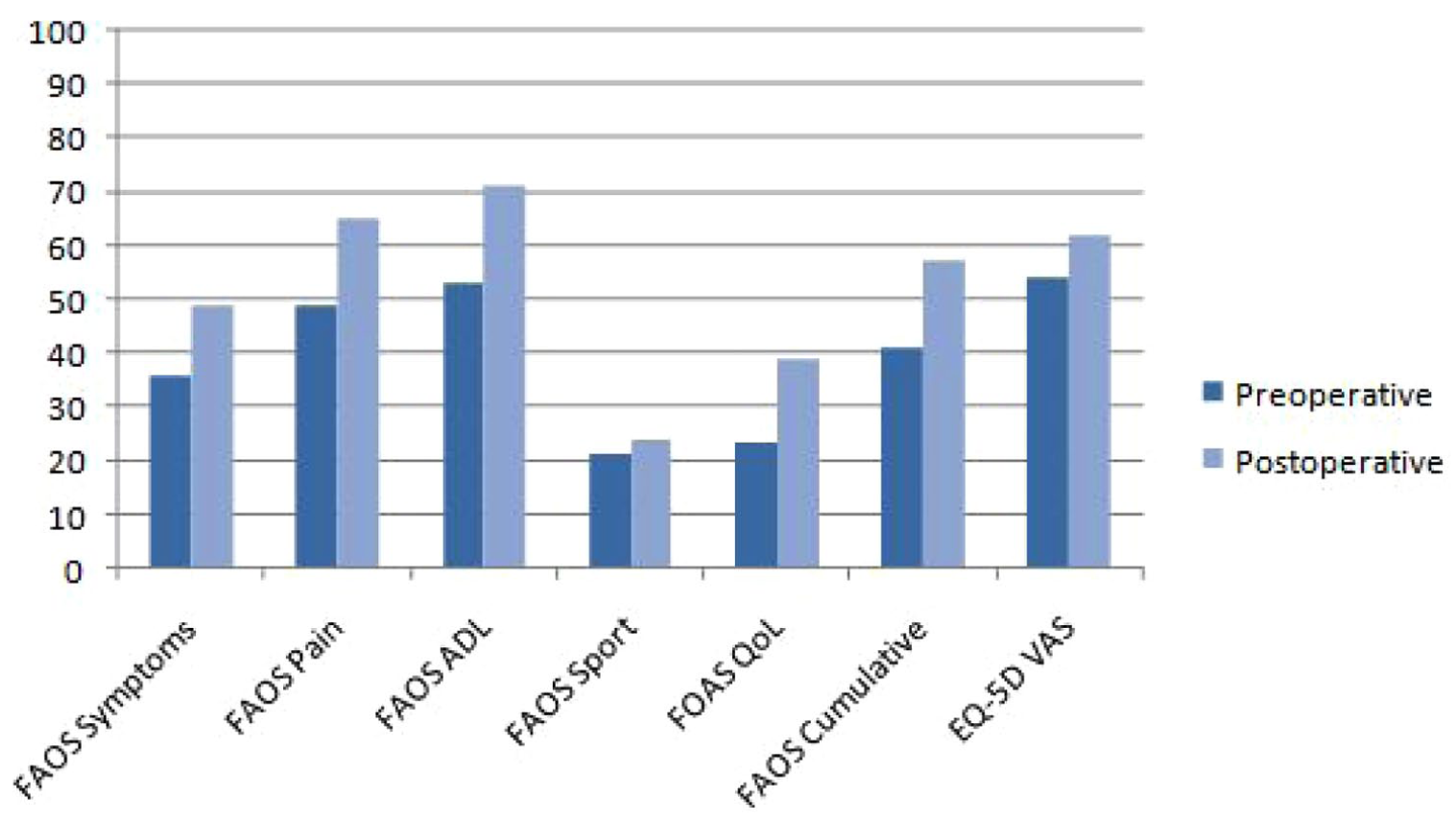
Patients’ reported outcome measures in TT fusion group.
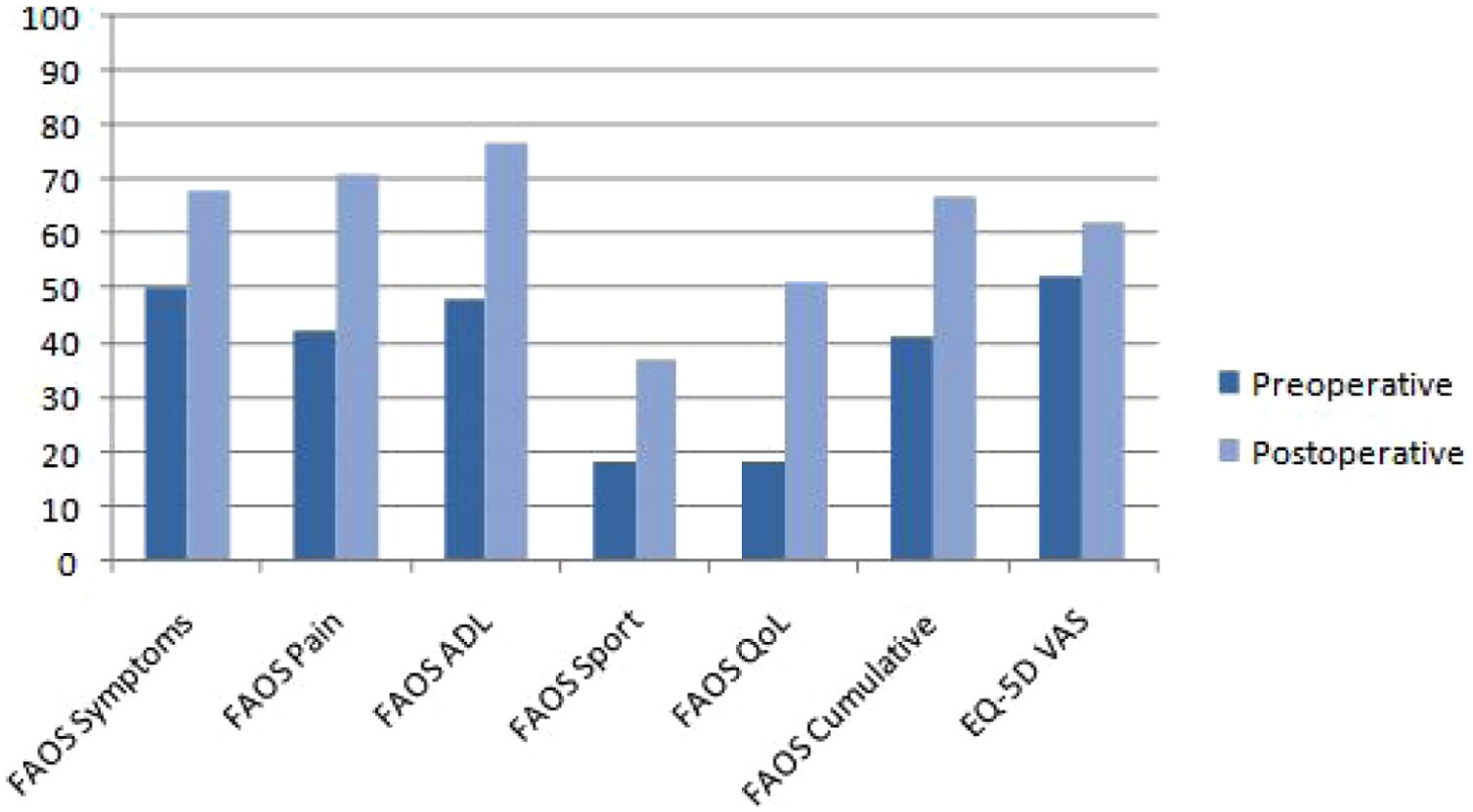
Patients’ reported outcome measures in ST fusion group.
In our series, there were 6 non-union cases in the TT group (3 in the arthroscopic and 3 in the open group) and 11 non-union cases in the ST group (2 in the arthroscopic and 9 in the open group) that required a second surgical procedure (Table 4). There were 8 infections that required surgical treatment (1 in the TT and 7 in the ST fusion group), corresponding to an overall revision rate of 18% (25/142 cases). In addition, there were 20 hardware removals (3 in the TT and 17 in the ST fusion group).
Complications Rate Divided for TT and ST Fusion Groups.
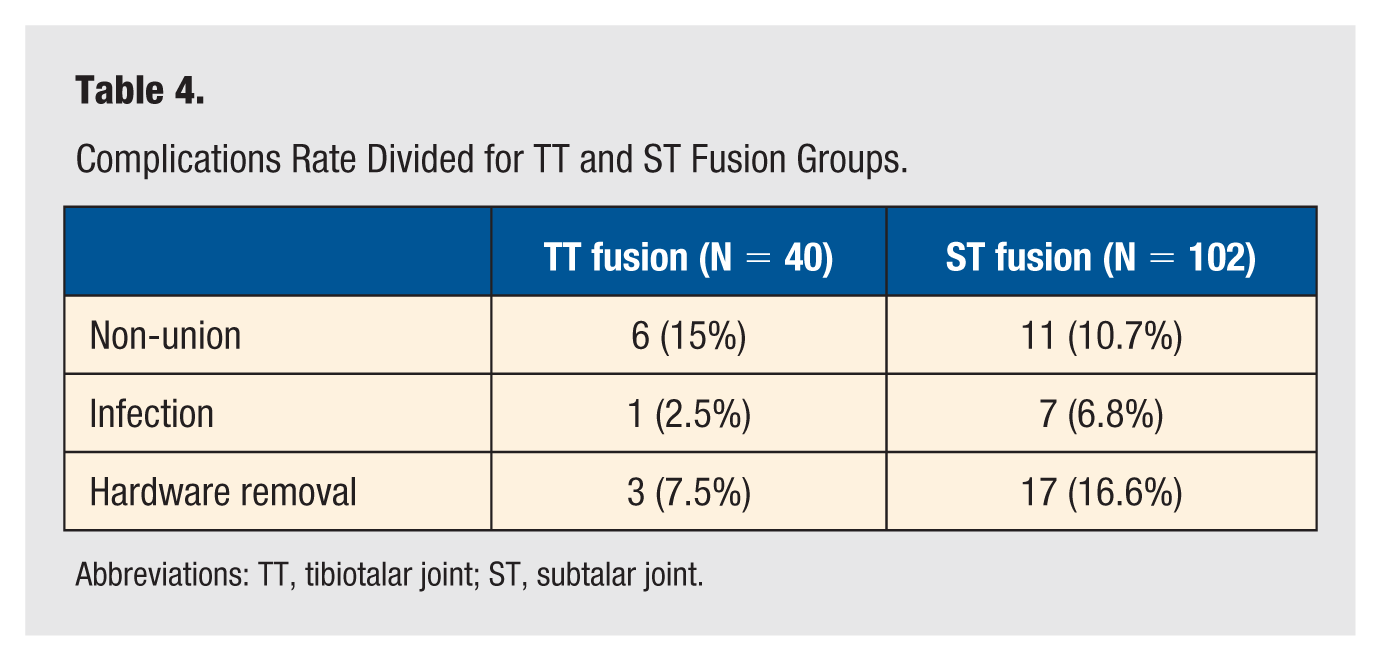
Abbreviations: TT, tibiotalar joint; ST, subtalar joint.
Discussion
The most important findings of this study were: (1) open or arthroscopic, TT or ST fusion significantly improved ankle joint function, quality of life and reduced joint-related pain but did not increase patients’ activity level; (2) ST fusion patients reported statistically higher improvement in subjective outcomes in some FAOS subscales than patients in the TT group; (3) older age, shorter symptom duration, and lower preoperative FAOS pain scores were strong negative predictors of postoperative PROMs.
The FAOS is commonly used to assess patient-reported outcomes in foot and ankle disorders.19 -21 Jones et al 19 reported a postoperative FAOS of 87 (10) after arthroscopic subtalar (ST) fusion, while Chraim et al 20 documented slightly lower scores of 60 (21) after open ST fusion. For ankle fusion, Berk et al 21 reported postoperative FAOS values of 54 (11) for open and 41 (13) for arthroscopic procedures. Although our results showed slightly lower postoperative FAOS scores (ST fusion group: 68 [21]; TT fusion group: 49 [19]), they are within the reported range. Importantly, the improvements in all FAOS subscales exceeded the established Minimum Important Clinical Difference (MICD) values for foot and ankle procedures. 22
The EQ-5D is the most commonly used instrument to assess health-related quality of life (HrQoL) and consists of a descriptive system EQ-5D and a vertical visual analogue scale EQ-VAS for self-assessment of patients’ health status. 23 In our study, while the EQ-5D scores (TT group: 0.55; ST group: 0.60) were lower than values reported by Morelli et al, 11 Hollman et al, 24 Van der Vliet et al, 25 and Loveday et al, 26 they still demonstrated statistically significant improvement. Conversely, our EQ-VAS scores (62 in both groups) were comparable to these reference studies and showed similarly significant improvement. This discrepancy could be due to methodological differences in score calculation available in each language—our study utilized the TTO valuation method (final scores from −1 to +1), which typically yields lower values than the visual analogue scale (VAS) approach (final scores from 0 to 1) used by other authors. 18 The TTO method was selected for our analysis due to its superior correlation with HRQoL outcomes, as supported by contemporary research.
The Tegner Activity Scale (TAS) is a standardized questionnaire for grading work and exercise activities that was originally developed for anterior cruciate ligament injuries but is now commonly used for other lower extremity activities. No improvement in TAS scores was observed following TT or ST arthrodesis as it remained at 2, although individual scores varied widely, ranging from 0 to 5. These results align with current literature and suggest the TAS, designed for sports-related injuries, may lack sensitivity to detect functional changes in end-stage OA patients with chronic activity limitations.15,16,27,28
The literature on predictive factors for TT and ST fusion outcomes remains limited and inconsistent. While some studies report conflicting associations between smoking and BMI on non-union rates, our findings align more closely with Saraiva et al’s demonstration of age and BMI as significant prognostic factors.29 -31 We confirmed a strong negative correlation between higher age and clinical outcomes, particularly for FAOS pain and symptom duration. The reasons for this could lay in older people having less healing potential and comorbid conditions leading to worse outcomes. 32 Contrary to Saraiva et al’s report of a positive BMI-FAOS correlation, our study did not confirm this paradoxical relationship. Our results confirmed that increased load impairs function and increases pain, while it causes delayed healing at the same time.
In our study, there were no statistically significant differences in PROMs between patients treated with open versus arthroscopic TT or ST fusion. This finding suggests that both surgical techniques provide comparable functional outcomes and a comparable level of patient satisfaction in the mid and long postoperative period. This leads us to several conclusions. First, the surgical approach may not have a significant impact on long-term PROMs if solid fusion is achieved, and second, the choice of surgical technique may be based on surgeon experience and patient anatomy rather than expected differences in PROMs.
While systematic reviews demonstrate lower complication rates for arthroscopic versus open hindfoot arthrodesis (12% vs 27%, 8% vs 27%), our findings challenge this paradigm.6,11 We demonstrated comparable outcomes between approaches for TT (3 arthroscopic, 3 open cases) while revealing a potential arthroscopic advantage only in ST procedures (2 arthroscopic, 9 open cases). Overall, the reintervention rate remained well below 20% and is comparable to or better than in other studies.6,11,33 This would suggest approach selection should consider both joint pathology and surgeon expertise rather than the presumed universal superiority of either technique.
This retrospective analysis of prospectively collected data carries several limitations. The choice between open and arthroscopic approaches was surgeon dependent, potentially introducing selection bias if more complex cases preferably received open procedures, although no such pattern was evident in our radiographic or clinical data. The sample being decent, the cohort’s heterogeneity, particularly the substantial discrepancy in group sizes (40 TT vs 102 ST fusion), along with the absence of objective functional measures like gait analysis, may limit generalization. Despite these constraints, the study benefits from considerable methodological strengths, including standardized surgical techniques (all procedures performed by a single surgeon at 1 institution), comprehensive patient capture over a 10-year period, and an exceptionally high 80% follow-up rate facilitated by our centralized health care system. While a randomized controlled trial with stricter inclusion criteria might better isolate technique-specific outcomes, our findings provide valuable real-world evidence reflecting actual clinical practice.
Conclusion
Isolated TT or ST fusions performed open or arthroscopically were safe and significantly improved function and quality of life and reduced joint-related pain, but did not increase patients’ activity levels. No differences emerged between surgical approaches in patient-reported outcomes. Patients with ST fusion had a better subjective outcome, while older age and lower preoperative FAOS pain were associated with a worse postoperative subjective outcome.
Footnotes
Acknowledgements
None.
Data Availability Statement
All the data related to the study are available upon request from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was in part funded by the University Medical Centre Ljubljana—institutional research funding grant #20230170 to MD.
Ethics Approval Statement
The study was approved by the National Medical Ethics Committee (approval no. #0120-99/2019/4). Respondents gave written consent for review and signature before starting interviews.