
Abstract
Background
This study aimed to evaluate outcomes after a minimum 5-year follow-up of feet with tarsal tunnel syndrome (TTS) after electroneuromyographic (ENMG) diagnosis and treatment. Possible predictive factors of outcome were sought.
Methods
All patients underwent, at the least, initial clinical evaluation, ENMG diagnosis, ultrasound and medical treatment for TTS. If treatment was unsuccessful after 6 months, tibial nerve release was proposed. Outcomes were classified as satisfactory (excellent and good) or unsatisfactory (fair and poor) based on Pfeiffer’s classification.
Results
Seventy-six feet received conservative treatment, with 65% of satisfactory outcomes, rising to 78% in case of additional tibial nerve release (16 feet, 21%, excellent results in 10 of 76 feet). Improvement was insufficient in 14% of feet, but the patients did not consider that surgery was necessary. Five years after medical treatment, outcome was satisfactory in 5 of 8 feet with nerve contact on ultrasound within the tarsal tunnel, and in 9 of 10 feet with isolated talus-nerve contact. Finally, 18% of feet had nerve contact on ultrasonography and a satisfactory outcome after conservative treatment when evaluated after a minimum of 5 years. Results tended to be better in the absence of static disorders (P = .058), hindfoot varus in particular (P = .032), and in women (P = .047).
Conclusions
Conservative treatment of TTS yielded satisfactory outcomes at 5-year follow-up. Except in rare cases, it should be the first-line treatment even when nerve contact is seen on imaging. Surgical release appeared to be beneficial after failure of medical treatment at 6 months. Outcomes appeared poorer in feet with static disorders and better in women.
Levels of Evidence:
Therapeutic, Level IV, Retrospective
“. . . we conducted a study analyzing the outcomes of TTS after a minimum 5-year follow-up in patients with a confirmed electroneuromyographic (ENMG) diagnosis . . .”
Introduction
Tarsal tunnel syndrome (TTS) results from damage to the tibial nerve or its branches. Most reports on TTS treatment appear difficult to compare, 1 and the published patient series do not have a long follow-up. Moreover, the majority of studies relate to the results of surgical interventions, whereas in order to target the best therapeutic approach it would be useful to know the results yielded by both medical and surgical treatment. 2 There is currently insufficient knowledge to accurately identify the most effective therapeutic indications. Hence the value of a study of the long-term course of TTS in feet with a confirmed diagnosis and a study that also takes into account the outcome of combined medical and surgical treatments. To improve knowledge for optimizing therapeutic strategies and clarifying surgical indications, we conducted a study analyzing the outcomes of TTS after a minimum 5-year follow-up in patients with a confirmed electroneuromyographic (ENMG) diagnosis who underwent medical and/or surgical treatment. Predictive factors were also sought to assist clinical diagnosis and optimal treatment choice.
Materials and Methods
Inclusion Criteria
Feet with functional symptoms of TTS that had undergone physical examination were further assessed only if electromyography of the lower limbs (ENMG) confirmed damage of the tibial nerve or its branches.3,4 Feet with a confirmed diagnosis of TTS were included in the study.
Clinical Examination
Patient characteristics, subjective symptoms (plantar pain or numbness, paresthesias, tingling sensations) and the patient’s history, circumstances of occurrence, particularly prior triggering trauma or microtrauma, were recorded. Physical examination sought obvious valgus or varus deformity of the hindfoot (visualized during walking at the end of the stand phase, before lifting the heel off the ground). 5 This qualitative visual gait assessment was repeated at each follow-up visit. Also assessed were a medial retromalleolar trigger zone4,6 and asymmetric sensory disturbances in the tibial nerve territory using a monofilament that grazes the skin (light touch).7 -9 These sensory disturbances—either hypoesthesia or, in some cases, hyperesthesia—were assessed during the initial physical examination using a monofilament that lightly touches (or very gently grazes) the skin over the tibial nerve distribution, following the protocol below. The first assessment involves light contact on the medial edge of the calcaneus, the plantar heel, the medial arch, the flexion crease of the first metatarsophalangeal joint, the ball of the hallux, and the lateral plantar surface of the foot (the so-called “isthmus”). A second, identical assessment was then performed. After a few minutes’ delay, a third evaluation was carried out to compare and confirm the results.
Imaging Studies
Ultrasonography, supplemented by MRI if needed, sought for contacts within the tarsal tunnel with the tibial nerve or its branches. 10 A space-occupying lesion was identified if a mass was present in the tarsal tunnel, whatever its nature (cysts, varicosities, accessory muscles, etc) (Figure 1). In addition to these space-occupying lesions, contacts external to the tarsal tunnel were sought on imaging. These were talus-nerve contacts (TNC) (Figure 2). They were often only detectable in a standing position (Figure 3) and may potentially create nerve compression between the nerve and the bone during walking. Direct contact of a space-occupying lesion or contacts external to the tarsal tunnel observed on ultrasonography were termed “contacts.” Plantar aponeurosis ≥5 mm and muscular disorders were also sought.
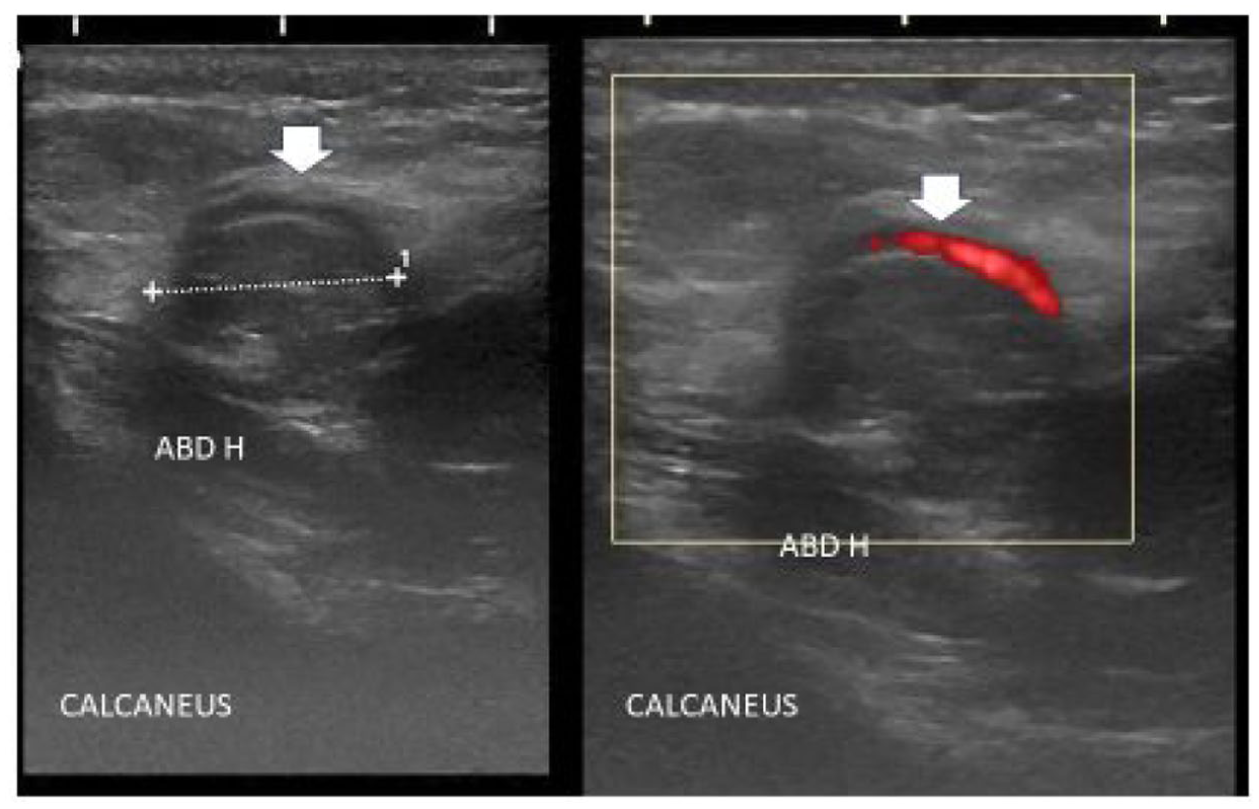
Ultrasound, axial sections with and without Doppler. Lipoma pressing on the medial calcaneal neurovascular pedicle (white arrows). ABD H: abductor hallucis longus.
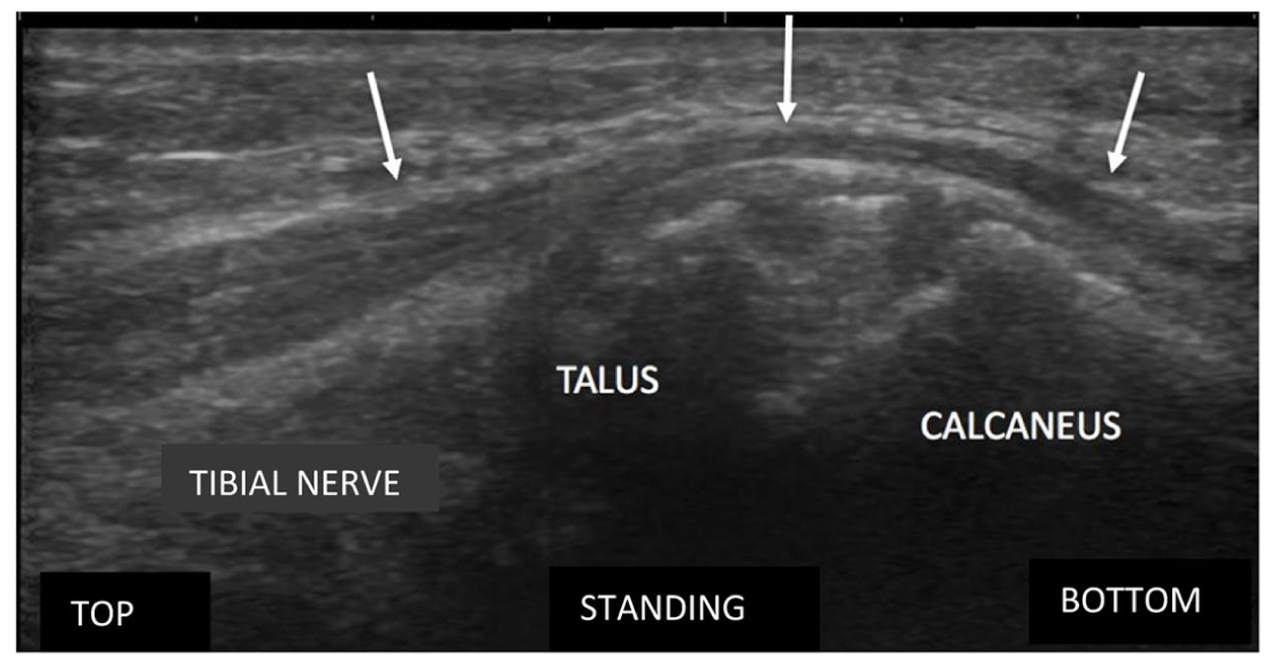
Ultrasound, talus/tibial nerve contact.
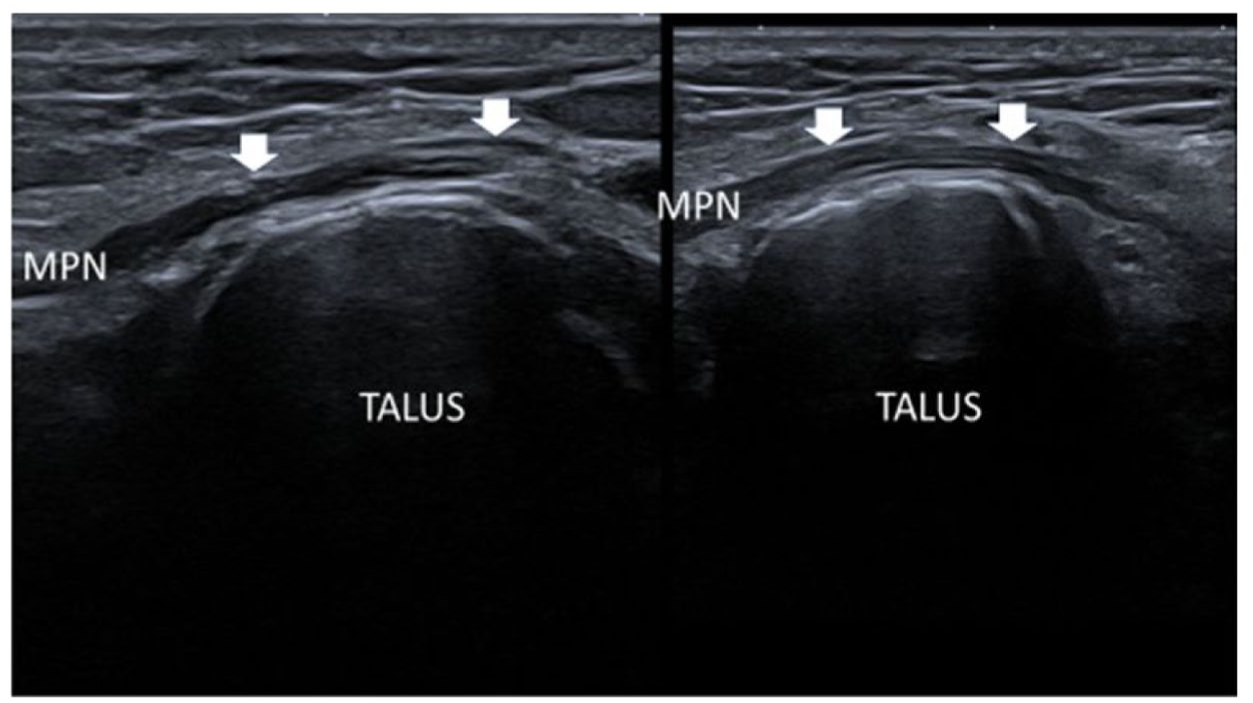
Ultrasound, frontal section, patient supine and standing. Talus-MPN contact increased on standing. MPN: medial plantar nerve.
Treatment
Conservative treatment consisted of activity modification, appropriate grade analgesics, plantar orthoses and adapted footwear (including rocker shoes or custom-made shoes), 11 and rehabilitation including stretching of the posterior muscular chains of the lower limbs, or intrinsic foot strengthening exercises. 12 In some cases, venotonic agents and support stockings were prescribed. An ultrasonography-guided corticosteroid injection in the tarsal tunnel was given if previous treatment was unsuccessful. The treatment goals were explained to patients since results depend on compliance with treatment, particularly in sports patients. 4 All patients were seen again at least once to check progress. Patients were informed that surgery would be considered if symptoms did not sufficiently improve after 6 months. Surgery could be debated earlier when there was obvious initial evidence of compression (cf infra) (Figure 4). After the patient had been informed of the benefits and risks of neurolysis (previously reported as yielding favorable results in about half of cases), 13 he or she decided whether to undergo surgery or not, depending on the functional discomfort they experienced. All procedures were carried out by practitioners specialized in osteoarticular pathology of the foot: radiologists, a neurologist, and surgeons, who used a similar surgical technique. 14
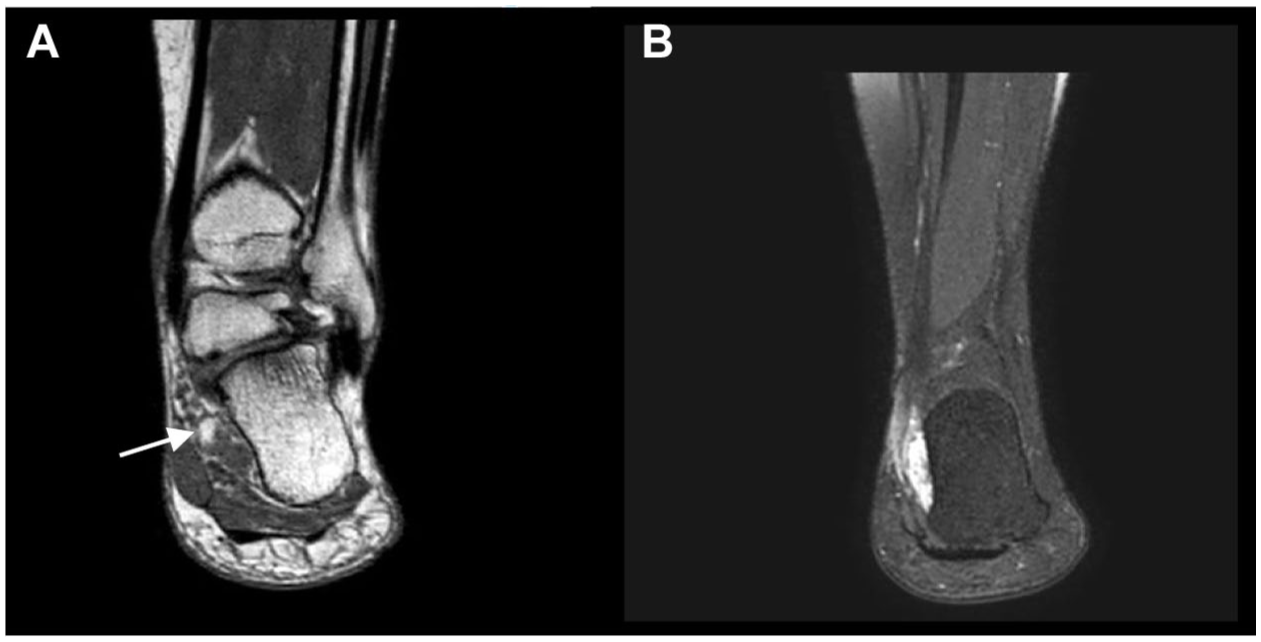
MRI, frontal section. (A) T1-weighted image, onset of fatty involution of the quadratus plantae muscle (white arrow). (B) T2-weighted fat-sat image, increased signal intensity of the quadratus plantae muscle in a female patient with marked valgus hindfoot and tarsal tunnel syndrome. Surgical treatment is justified by the muscle atrophy.
Following clinical diagnosis, the first step in the treatment protocol involved the immediate recommendation of foot orthotics and appropriate footwear when static disorders were present. The quality and correct use of these devices were evaluated a few weeks after initial use. Patients were advised to modify any weight-bearing activities—for example, replacing running with brisk walking, which is less traumatic. Stretching exercises targeting the posterior muscle chains of the lower limbs were also prescribed. Analgesics may be used, provided they did not obscure the progression or regression of symptoms. Subsequent management depended on the clinical response and imaging findings after this initial phase.
Assessment Criteria
Five years minimum after electrodiagnosis and start of specific treatment for TTS, patients were contacted by mail or telephone, or seen in consultation. Their initial and current symptoms of TTS were evaluated. Lesions of other peripheral nerves were observed on ENMG, and consequently only plantar symptoms were considered in the evaluation.
Evaluation, based on Pfeiffer’s classification, took into account medical treatment and surgical treatment, if applicable, as follows 13 :
Group 1: excellent results, recovery with complete disappearance of TTS symptoms,
Group 2: good results, improvement with pain that did not interfere with daily function, no regular use of medication,
Group 3: fair results, unsatisfactory improvement, reduction in pain intensity or frequency, but functional disability in daily life, regular use of medication,
Group 4: poor results.
Patients with categories 1 and 2 outcomes taken together were considered as the satisfactory outcome group. This group was compared with groups 3 and 4 taken together, considered as the unsatisfactory outcome group. 13 Similarly, patients in group 1 were compared with patients in groups 3 and 4 taken together. Finally, when the results were known, some patients were contacted again to clarify the treatment modalities.
Predictive Factors
Possible predictive factors of treatment outcome were sought and discussed: age, sex, laterality, symptom duration before conservative and/or surgical TTS treatment, previous trauma and microtrauma, trigger zones, sensory disturbances, aponeuropathy, contacts with the nerve within and external to the tarsal tunnel. The relation between the simultaneous presence of a trigger zone and sensory disorders with confirmed TTS on ENMG was sought, as this has been emphasized as a clinical predictor of a diagnosis of TTS.8,9
Too few patients had received surgical treatment for sufficient conclusions to be drawn based on this factor alone.
Statistical Analysis
Qualitative variables were described using frequency and percentage distributions. The number of missing data, if any, were not considered for the calculation of proportions. Quantitative data were described using the number of observations, mean, standard deviation, median, interquartile ranges, minimum and maximum values.
The study was not powered to detect significant statistical effects and P-values are given only as an indication. However, a 20% level of significance was used to detect potential predictive factors of successful treatment (medical or overall). Predictive factors of successful treatment (medical or overall) were investigated using univariate and multivariate logistic regression models: significant predictive factors (at a 20% level) from the univariate analyses were integrated in a multivariate logistic regression model.
Depending on type of data, Pearson’s chi-square test, Fisher exact test, or the Wilcoxon rank-sum test were used to compare treatment outcome according to feet characteristics. Statistical analyses were performed using R software version 4.3.1.
Results
In 2016 and 2017 in a medical consultation for foot and ankle pathology, 76 patients (103 feet) underwent lower limb ENMG which confirmed the diagnosis of TTS. Five feet without TTS symptoms were excluded (they were contralateral to symptomatic feet justifying the indication for ENMG of the lower limbs). A total of 98 feet were included in the study. Percentages below were rounded to the nearest whole number.
At 5 years minimum after electrodiagnosis and the start of specific conservative treatment for TTS, the patients were contacted to ascertain the status of their TTS symptoms compared with symptoms before treatment. Twenty-two of the 98 feet (22%, 14 patients) were lost to follow-up and 76 feet were finally included in the study.
One patient with failure after previous surgery for TTS was included in our study and was again dissatisfied after treatment that included a second surgical release. The results, expressed per feet were studied.
Initial Characteristics
Among previous triggering trauma or microtrauma in 23 of the 76 feet (30%) were 15 unusual walking or running conditions, 2 ankle sprains, 2 falls, 1 sequela of ankle fracture, 1 calcaneus fracture, 1 talar subluxation, and 1 hallux valgus surgery (Table 1). Aponeuropathy was observed in 29 feet (38%). The association of a trigger zone and the sensory disturbances of TTS was observed in 58 of the 76 feet (76%).
Characteristics of 76 Feet With TTS Diagnosed by Electroneuromyography (ENMG).
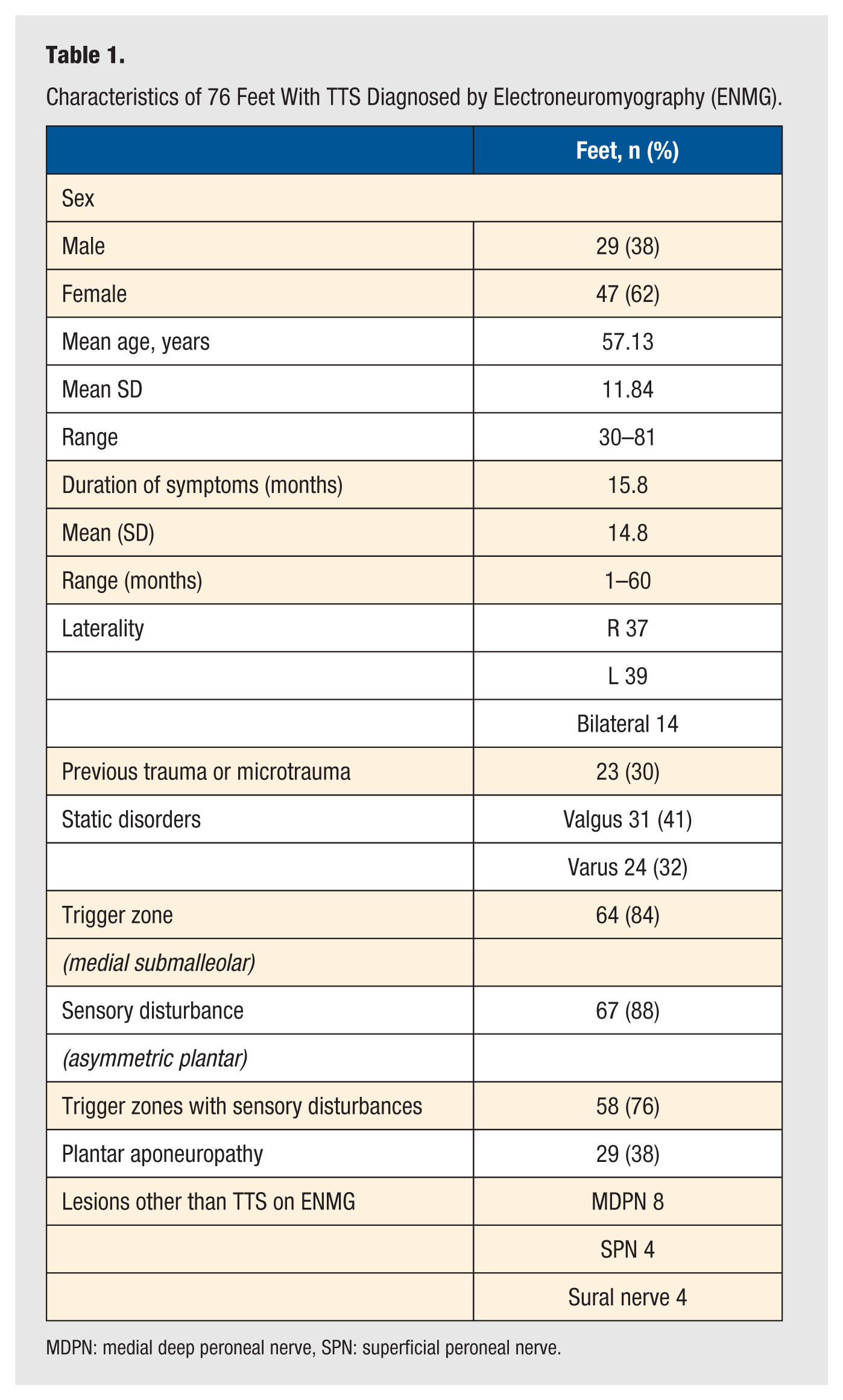
MDPN: medial deep peroneal nerve, SPN: superficial peroneal nerve.
Treatment Outcome After 5 Years Minimum
The 76 feet included had received conservative treatment, with 49 (65%) satisfactory outcomes and 27 (35%) unsatisfactory outcomes (Table 2). For 11/76 feet (14%), the patients were dissatisfied but their decision was that surgery did not appear necessary. Finally, after 6 months of ineffective medical treatment, 16 (21%) underwent surgical release, 10 (13%) had an excellent result, and 6 (8%) an unsatisfactory result. At the end of a minimum of 5 years specific treatment of TTS, the overall results were 59 (78%) satisfactory results (Figure 5).
Patient Satisfaction With Outcome 5 Years After Start of Treatment of Tarsal Tunnel Syndrome (76 Feet).
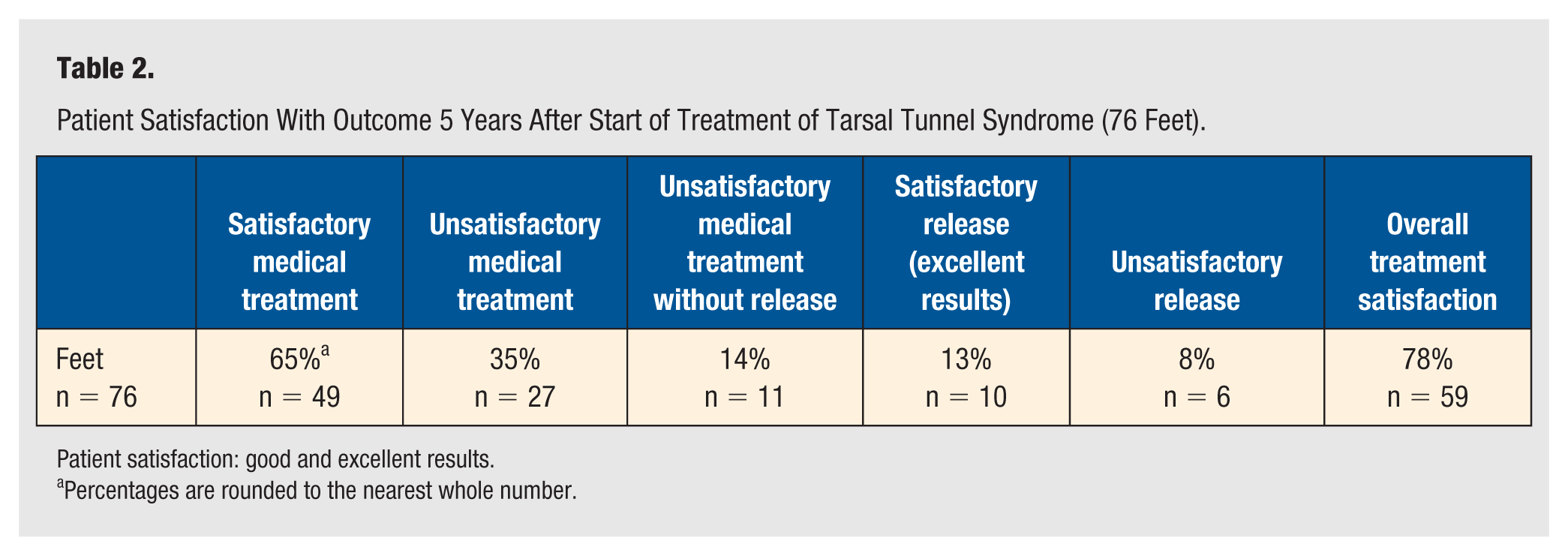
Patient satisfaction: good and excellent results.
Percentages are rounded to the nearest whole number.
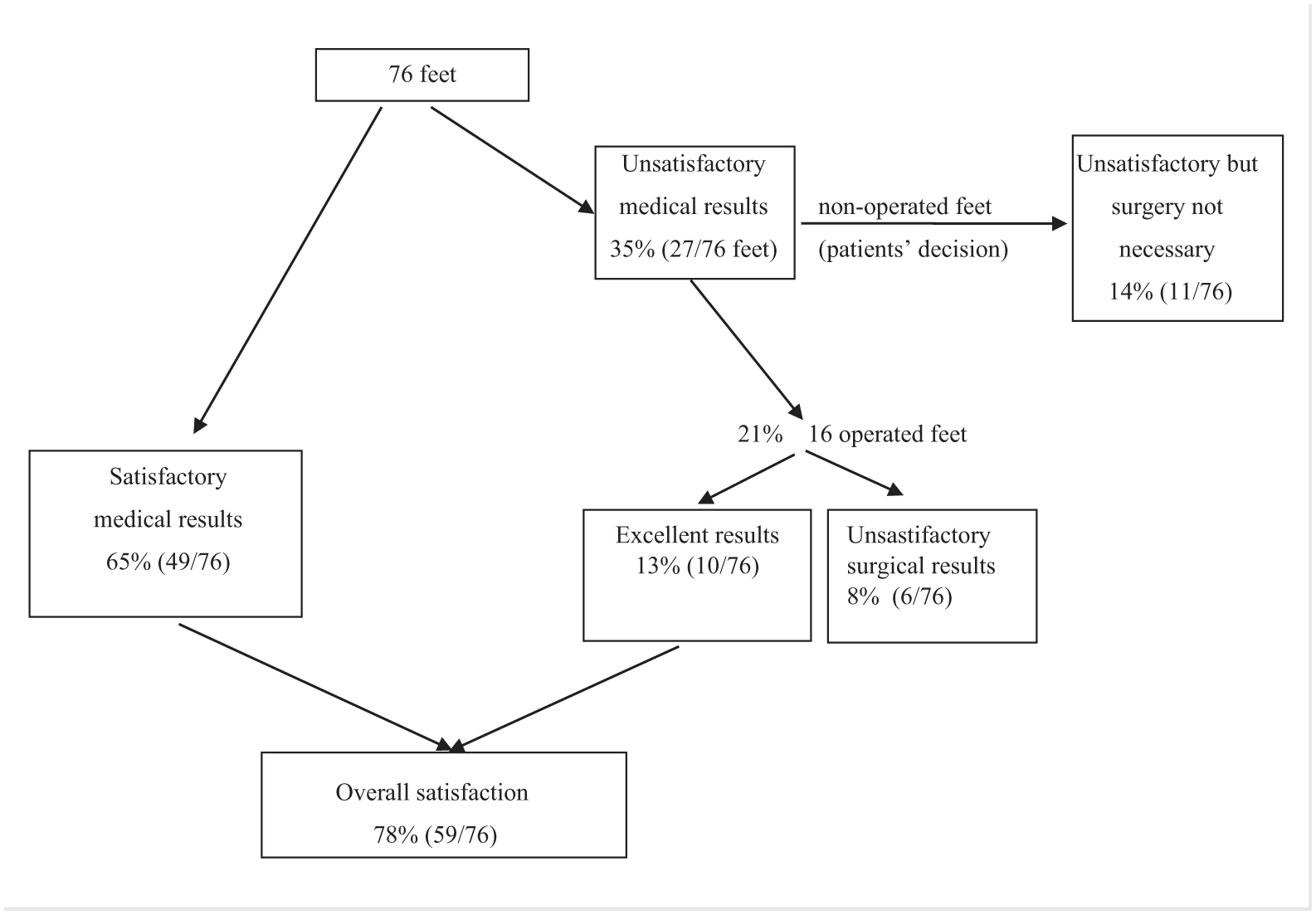
Decision tree and treatment results in 76 feet with TTS in a medical consultation for foot and ankle diseases. Percentages are rounded to the nearest whole number. TTS, tarsal tunnel syndrome; ENMG, electroneuromyography.
During this period of at least 5 years, for 3 feet (3 patients) with static disorders (1 valgus and 2 varus feet), surgical revision was performed after neurolysis but the results remained unsatisfactory.
Medical treatment yielded excellent results in 34 of 76 feet (45%) after 5 years and more. With combined medical and surgical treatment, excellent results were observed in 44 feet (58%).
Treatment Outcome for Feet With Contact Within the Tarsal Tunnel on Ultrasonography (Space-Occupying Lesions)
In 8 feet with static disorders, lesions within the tarsal tunnel were in contact with the nerve on ultrasonography: 2 lipomas, 1 cyst arising from the subtalar joint, 3 feet with varicosities and 2 feet with an accessory flexor digitorum longus muscle (FDL) (Table 3). After medical treatment, 5 of these feet (5 patients) with nerve contact had satisfactory results. Four of these 5 feet had isolated contact: a varus foot with a lipoma (Figure 3) had an excellent result, and 3 cases had a good outcome: another varus foot with lipoma, a valgus foot with a cyst arising from the subtalar joint and a valgus foot with FDL. Finally, one foot with good results had contacts both within and external to the tarsal tunnel; this was a valgus foot with varicose veins and TNC. When these 5 patients were recontacted, they all cited foot orthoses as the principal factor of improvement.
Outcome 5 Years After Start of Treatment of Tarsal Tunnel Syndrome (76 Feet).
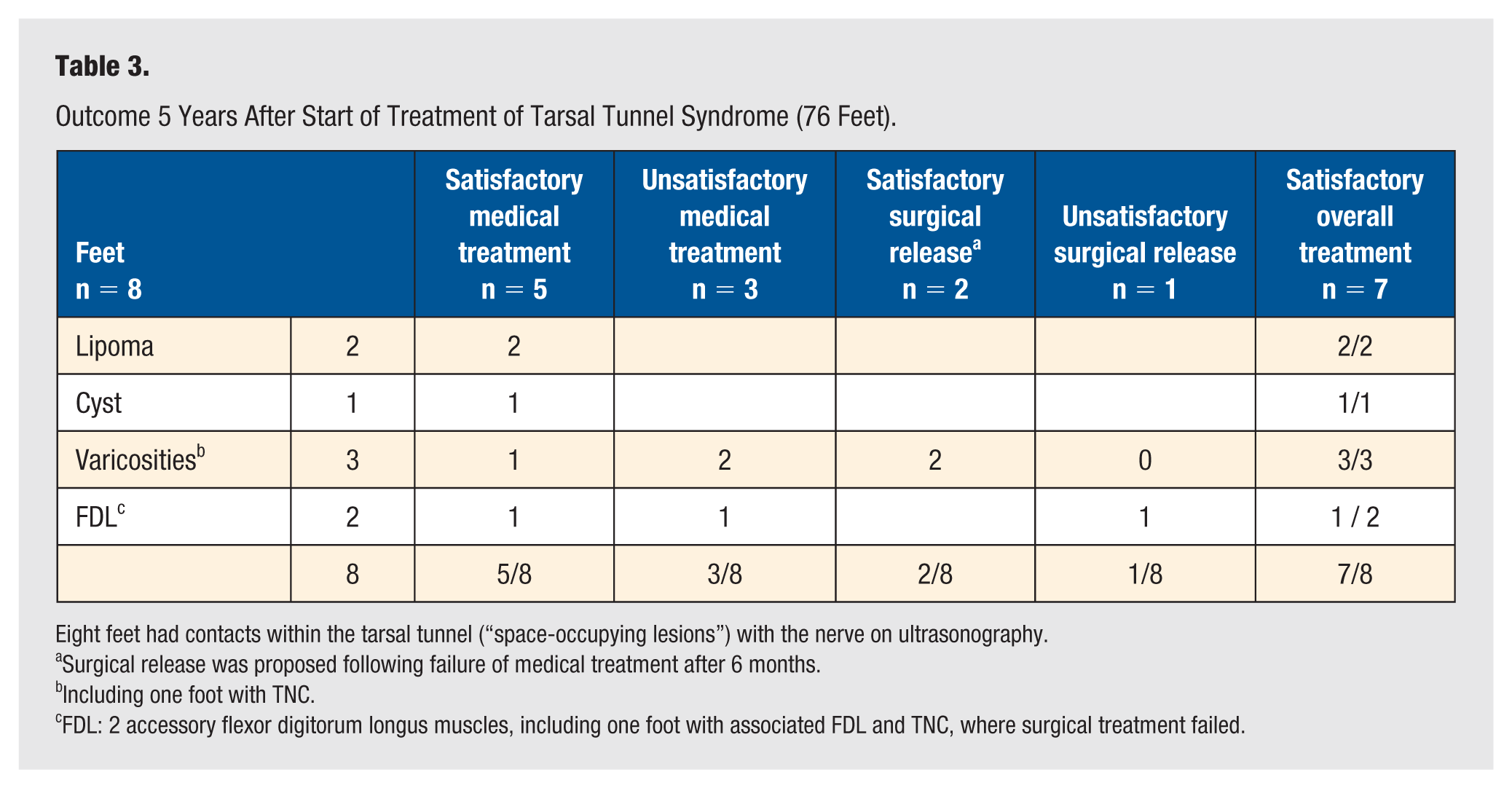
Eight feet had contacts within the tarsal tunnel (“space-occupying lesions”) with the nerve on ultrasonography.
Surgical release was proposed following failure of medical treatment after 6 months.
Including one foot with TNC.
FDL: 2 accessory flexor digitorum longus muscles, including one foot with associated FDL and TNC, where surgical treatment failed.
In 3 of the 8 feet with lesions within the tarsal tunnel, medical treatment was not satisfactory and these feet underwent neurolysis. Two feet with varicosities improved after surgical release, while one foot with FDL and TNC was not improved (Tables 3 and 4).
Satisfactory Conservative Treatment When Contact on ultrasonography (14/76 Feet, 18%).
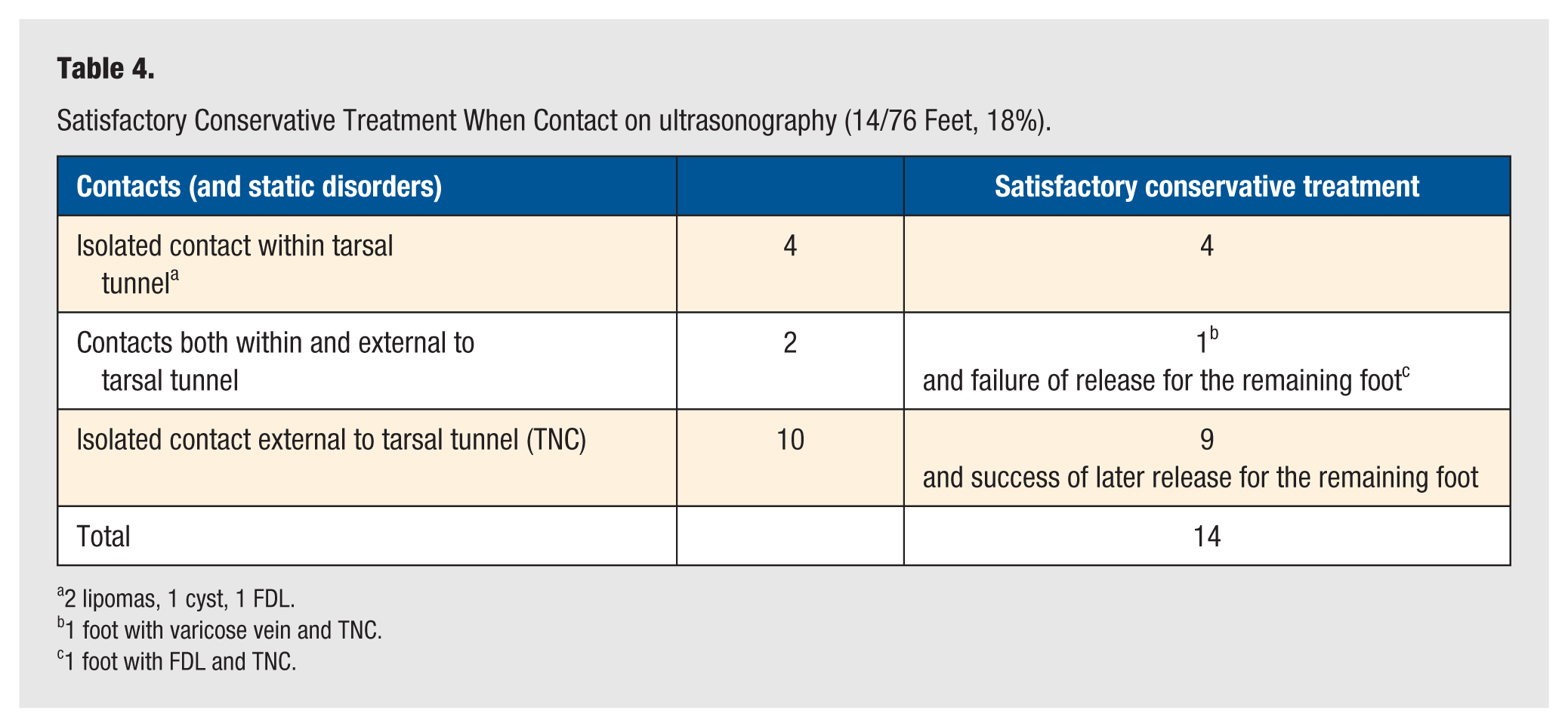
2 lipomas, 1 cyst, 1 FDL.
1 foot with varicose vein and TNC.
1 foot with FDL and TNC.
We observed contact external to the tarsal tunnel (talus-nerve contact, TNC) on ultrasonography in 12 feet (Table 4). All 12 feet had a static disorder (7 valgus, 5 varus). Ten feet had isolated TNC and 2 feet had lesions within and external to the tarsal tunnel (cf. supra).
Of the 10 feet with isolated TNC, 9 had a satisfactory outcome after medical treatment and 1 foot only after release. The 2 feet that had both external TNC and lesions within the tarsal tunnel on the same foot included one foot with varicosities, which improved with medical treatment (cf. supra). The second foot with TNC and FDL was not improved by medical treatment and surgical release did not give a satisfactory result (Table 4).
Finally, in the current series of feet with TTS, the outcome of conservative treatment was satisfactory in 5 feet with contacts within the tarsal tunnel (Table 3, second column) and in 9 feet with isolated contacts external to the tarsal tunnel (Table 4) observed on ultrasound. Thus, a total of 14 of 76 feet (18%) had a satisfactory outcome when evaluated after a minimum of 5 years (Table 4).
Predictive Factors of Successful Conservative or Overall Treatment
Trends were observed (Table 5). Varus was associated with a greater risk of unsatisfactory outcome than the absence of static disorders (P = .032).
Predictive Factors of Medical and Overall Treatment, Observed Trends (76 Feet).
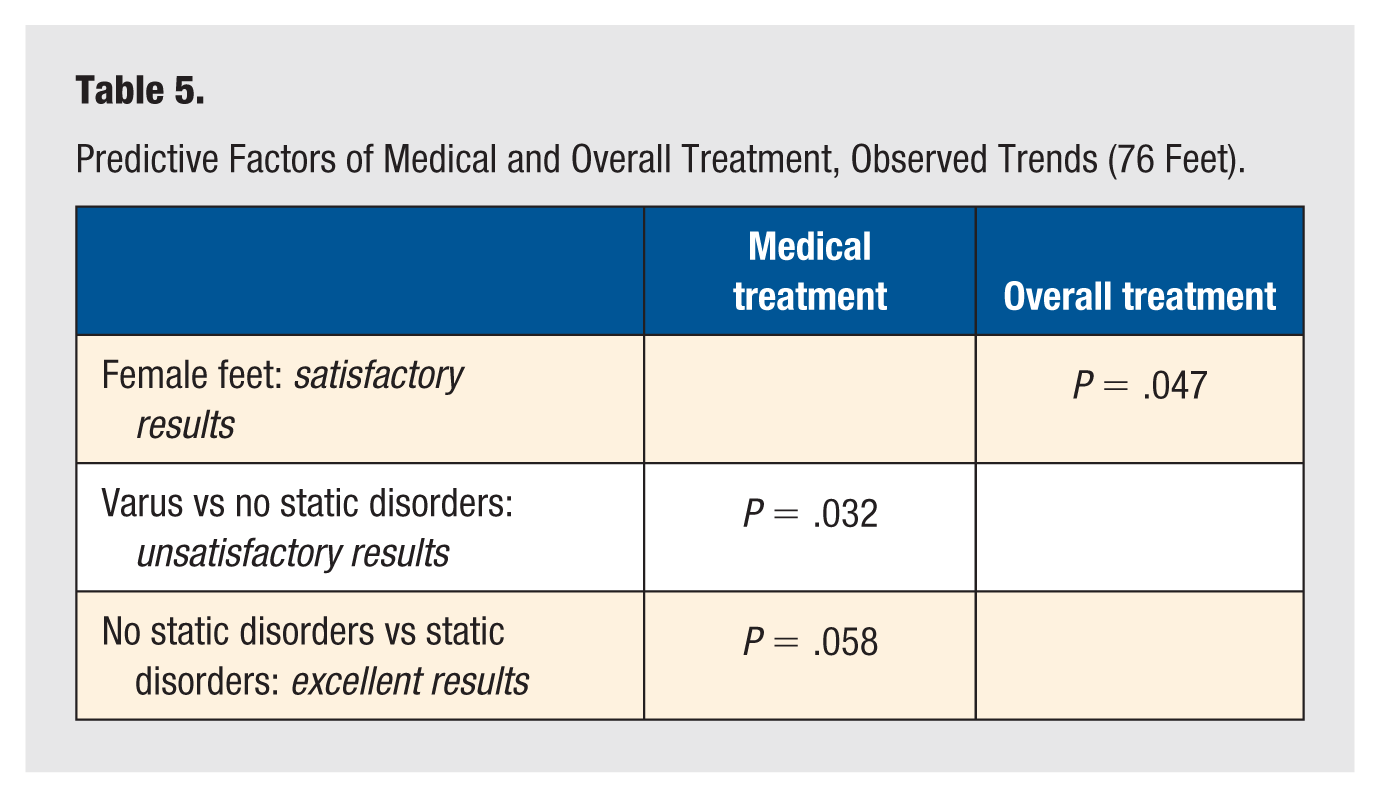
Excellent results tended to be more frequent in feet without static disorders (P = .058). For the overall treatment, considering feet with an excellent or a satisfactory outcome, no relation was observed between outcomes and several factors: age, duration of symptoms, laterality, previous triggering trauma and microtrauma, trigger zones, sensory disturbances, and aponeuropathy. The rate of satisfaction after overall treatment was higher in female patients (P = .047).
Discussion
Seventy-six feet with functional symptoms and a diagnosis of TTS confirmed by ENMG were evaluated. At 5 years minimum after diagnosis and start of conservative treatment, patients were questioned about their symptoms of TTS compared with their initial symptoms. Following combined medical and surgical treatment, excellent outcomes were observed in 58% of cases, while satisfactory outcomes were achieved in 78% of cases. We chose this 5-year follow-up period since in another study of TTS patients with an average follow-up of 3 years, it was observed that some patients who initially improved after surgical treatment later reported a return of pain. 13 On the other hand, although it has been reported that non-operative measures yielded a successful outcome only in some case reports, 13 we however observed better results, with 65% of satisfaction with conservative treatment after a minimum of 5 years. This result, which is significantly higher than previously reported data, can be explained as follows.
On the one hand, 14 out of 76 feet (18%) with a mass identified on imaging showed improvement with conservative treatment. Five feet in 5 patients with TTS and static disorders, and with lesions within the tarsal tunnel in contact with the nerve observed on ultrasonography had satisfactory results after conservative treatment (Table 3). The initial imaging findings could have suggested that surgery was indicated because TTS was attributed to compression demonstrated by mass-nerve contact on imaging. When contacted again at the end of the study, these 5 patients cited foot orthoses as the principal factor of improvement. This improvement may be explained by treatment of the static disorders. Firstly, combined eversion-dorsiflexion and cyclical loading with internal rotation of the leg cause tibial nerve lesions as the nerve is under tension. 15 In valgus hindfoot, probably correction of the valgus should lead to improvement. Moreover, in static disorders of the foot the tarsal tunnel is decreased in volume, and pressure in the tunnel is increased, which may explain damage to the tibial nerve.16,17 After correction of the static disorders, it may be hypothesized that the symptoms of TTS may decrease when the hindfoot is in a neutral position, 16 explaining the improvement. In cases of hindfoot varus (a high-arched or supinated, often stiffer foot), there may be increased strain on the tibial nerve and reduced shock absorption. This could explain why varus alignment was identified as a risk factor for poor outcomes, and why correcting such alignment—when possible—may be beneficial. In the case of contact within the tarsal tunnel, we should nevertheless remember that surgical release was effective in presence of identical lesions within the tarsal tunnel,1,13,18,19 in particular lipomas,20,21 and in certain cases of accessory muscles with tarsal tunnel syndrome (cf infra). 18 ,22 -26
Additionally, contacts external to the tunnel (TNC) and static disorders were observed in isolation in 10 feet and 9 of these feet were improved by medical treatment (Table 4). TNC causing nerve compression could explain the symptoms of TTS, and consequently treatment of static disorders could improve the symptoms. 16
Pfeiffer and San Marco (in TTS confirmed by ENMG) observed that surgery should be considered only after conservative management had afforded no improvement of major symptoms.13,19 A recent update also recommends initial conservative treatment in TTS. 1 In the current series, since initial conservative treatment of TTS appeared satisfactory in 18% of cases, this is a strong argument in favor of such treatment, even if there are contacts with the nerve on ultrasonography (Table 4).
These findings should not lead us to forget that surgical release is immediately indicated if motor deficit is present, if there are muscle symptoms due to a localized lesion of the tibial nerve on imaging (Figure 4), or if there is obvious symptomatic evidence of compression by a large mass or malignancy. 4 It should be remembered that in presence of inflammatory rheumatism, if possible the inflammatory lesions should first be rapidly treated.
In our current patient series, we sought predictive factors for the outcomes of conservative and overall treatment. Predictive factors of the outcome of surgical treatment may sometimes be observed in the onset of TTS. 20 ,25 -27 For Seidel, the best predictors of improvement in patients with TT release were preoperative ENMG evidence of tibial neuropathy and tibial nerve plantar symptoms. 27 All the patients operated in this current study fulfilled these conditions and surgical treatment was successful in 10 of 16 feet. Regarding duration of symptoms, a short period of time (around 1 year) between symptom onset and release yielded the best results.19,25 However, this finding was not obvious in other series, 1 nor was a relationship found with presence or absence of a causal trauma. 28 In the current series, the results of overall treatment were significantly better in women, but this point is not mentioned in other studies. In our series, the presence of static disorders may be suggested as a reason for patient dissatisfaction.
It was explained to the patients with TTS that “there appears to be no method that can confirm the diagnosis clinically.” 13 But in our study, the association of a trigger zone and of sensory disturbance in patients with a confirmed diagnosis of TTS was observed in 76% of feet. This observation confirms that this association may be useful to assist clinical diagnosis.9,10
For 14% of feet, although patients were dissatisfied with medical treatment, they considered their pain bearable and sufficiently improved for surgery not to be required. This observation highlights the difficulty of categorizing subjective outcomes. Furthermore, it is possible that some patients could have been considered as having good results according to other classifications.2,13
Conclusions
Evaluation of outcomes over a period of 5 years or more in our study showed that conservative treatment of TTS yields significantly better results than previously expected. These findings suggest that addressing underlying foot biomechanics (such as static disorders) is a key component of effective TTS management. However, the study involved a small sample size and was subject to the inherent limitations of an observational design, highlighting the need for a prospective study with a larger cohort.
Footnotes
Acknowledgements
The authors thank Nina Crowte for language assistance.
Author Contributions
M.B. conceived and designed the analysis and wrote the paper.
M.L. contributed to study conception and wrote the paper.
D.D. critically reviewed the paper.
G.B. contributed data.
O.F. contributed data.
X.M. critically reviewed the paper.
T.T. contributed data.
N.C. contributed data.
J.-Y.C. contributed data.
D.B. contributed data.
F.C. contributed analysis and wrote the paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethics committee of Rouen University Hospital (protocol no. E2025-04) on January 1, 2025. This is an IRB-approved retrospective study, all patient information was de-identified. Patient data will not be shared with third parties.
Informed Consent
Patients were orally informed about the study. In accordance with local regulations and the retrospective nature of the study, written informed consent was not required.
Trial Registration
Not applicable, because this article does not contain any clinical trials.