
Abstract
Background
Union deformities are relatively common in proximal fifth metatarsal (5MT) fractures following both conservative and surgical treatment. Several risk factors have been identified to guide risk prediction and management. This review aimed to summarize factors contributing to delayed or nonunion in 5MT fractures.
Methods
A literature search for studies reporting risk factors for 5MT fractures was performed using PubMed/Medline, EMBASE, ScienceDirect, Web of Science, and CINAHL databases. Methodological quality was assessed using the Methodological Index for Non-Randomized Studies (MINORS). Data on bone healing rates, complications, fracture zones, treatment approach, and healing outcomes were collected and summarized.
Results
The initial search identified 668 articles, of which 13 met inclusion criteria, including over 1000 cases. Multiple risk factors were significantly associated with impaired union in 5MT fractures. Fracture zone (particularly zone 2), a plantar gap >1 mm, small screw diameter, and early return to activity before radiographic healing were the most consistent predictors of delayed or nonunion. Surgical treatment led to faster union but higher rates of delayed union and refracture. Bone grafting and larger screw diameters significantly improved union outcomes.
Conclusion
Healing outcomes in 5MT fractures are influenced by multiple risk factors, with fracture zone, fracture chronicity, and fixation strategy being the most significant contributors to union deformities. Identifying high-risk patients and tailoring treatment may reduce nonunion and improve recovery. Further high-quality studies are warranted to establish standardized definitions, treatment protocols and risk stratification models.
Level of Evidence:
Level IV: scoping review.
“Although numerous studies have examined these outcomes, variations in definitions, classifications, and outcome measures across the literature make direct comparison and standardization difficult.”
Introduction
Metatarsal fractures are among the most common bone fractures, with an incidence rate of 75.4 per 100 000 per year. 1 Among these, fifth metatarsal (5MT) fractures account for over 80% of isolated metatarsal fractures. 2 Treatment choice of a 5MT fracture is mostly based on the fracture’s location, degree of displacement, patient’s lifestyle, activity level, and expectations.1 -5 There are controversies within the literature regarding the surgical or nonsurgical approach for 5MT fracture treatment of various types. Surgical management carries risks such as wound infection, hardware prominence, nerve irritation (peroneal or sural), peroneus brevis rupture, metatarsalgia, and iatrogenic fractures. 6 To reduce the nonunion rate, research has focused on identifying risk factors to better recognize high-risk patients. In addition to fracture location and treatment methods, patient demographics, comorbidities such as diabetes mellitus (DM), smoking, use of bone grafts during surgery, and early return to activity have also been suggested to contribute to nonunion or delayed union in 5MT fractures.3,7 -12 Despite these studies, the available evidence remains heterogeneous, with variability in study design, definitions of union, and outcome measures. Definitions of bone union vary across the literature. Nonunion is most commonly defined as the absence of radiographic bridging after 6 months, while delayed union has been variably defined as a lack of radiographic progression at 3 months or prolonged healing beyond expected timeframes. Some studies rely solely on radiographic criteria, whereas others incorporate persistent pain or functional limitation.7,9,12 -16 This heterogeneity limits direct comparison and underscores the need for standardized outcome definitions.
The purpose of this scoping review is to systematically identify and evaluate the reported risk factors associated with impaired union in fifth metatarsal fractures. This review aims to provide clinicians with an evidence-based framework for recognizing high-risk patients and optimizing treatment strategies to improve bone healing and functional outcomes.
Methods
The databases that we used for this systematic review were PubMed/Medline, Science Direct, and CINAHL. We searched these databases for all available evidence up to January 2024, without applying any date restrictions at the beginning of the search. Our PubMed search strategy was as follows: (fifth metatarsal fracture OR 5th metatarsal fracture OR metatarsal fracture OR jones fracture) AND (nonunion OR non-union OR delayed union OR union deformity OR union) AND (risk OR risk factor OR associated factor OR correlation OR correlated factor).
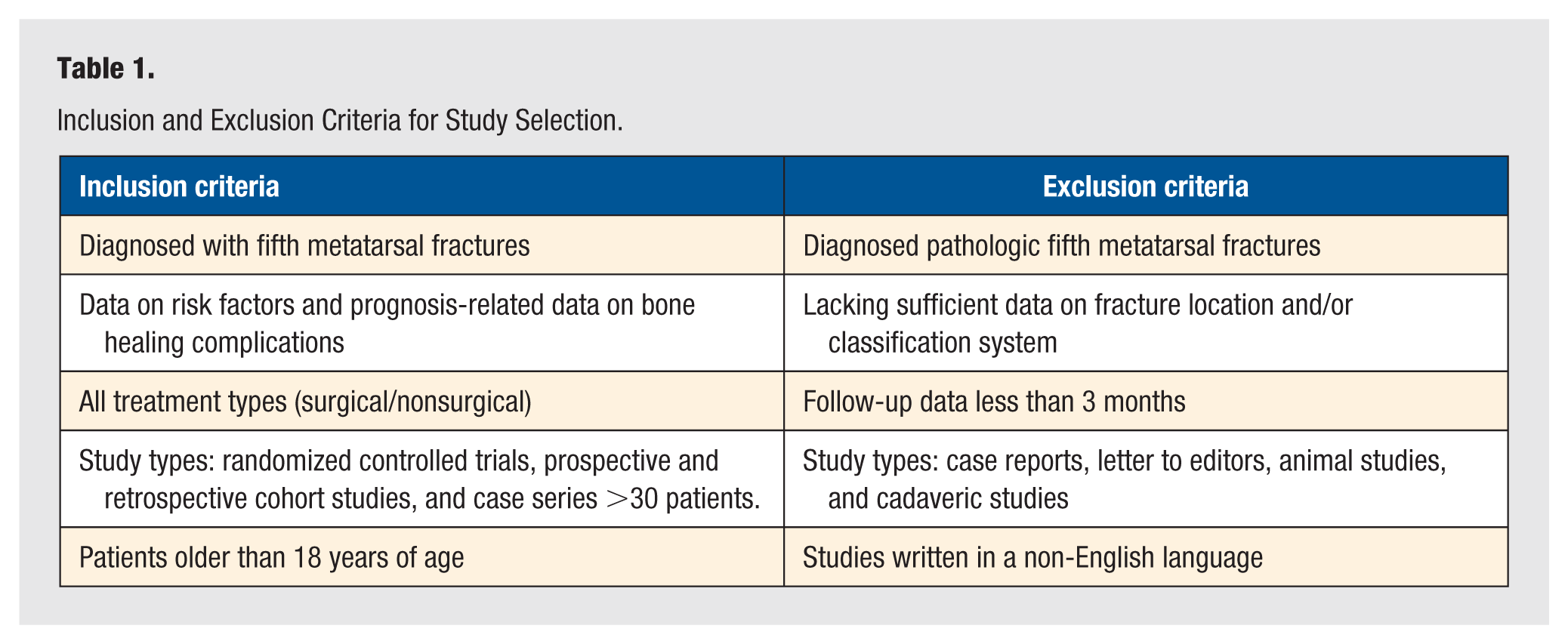
Studies included prospective and retrospective studies, case series (≥30 patients), and randomized controlled trials (RCTs) examining risk factors and predictive models for union issues in 5MT fractures. Both surgical and nonsurgical treatment types for all 3 anatomical zones (1, 2, and 3) were considered. A minimum follow-up of 3 months was set as an inclusion criterion (Table 1; Figure 1). Quality assessment was conducted using the Methodological Index for Non-Randomized Studies (MINORS). Study characteristics and outcome measures were collected using Covidence software (Covidence, Australia). Data on fracture characteristics, treatment methods, and outcomes were extracted for qualitative synthesis.
Inclusion and Exclusion Criteria for Study Selection.
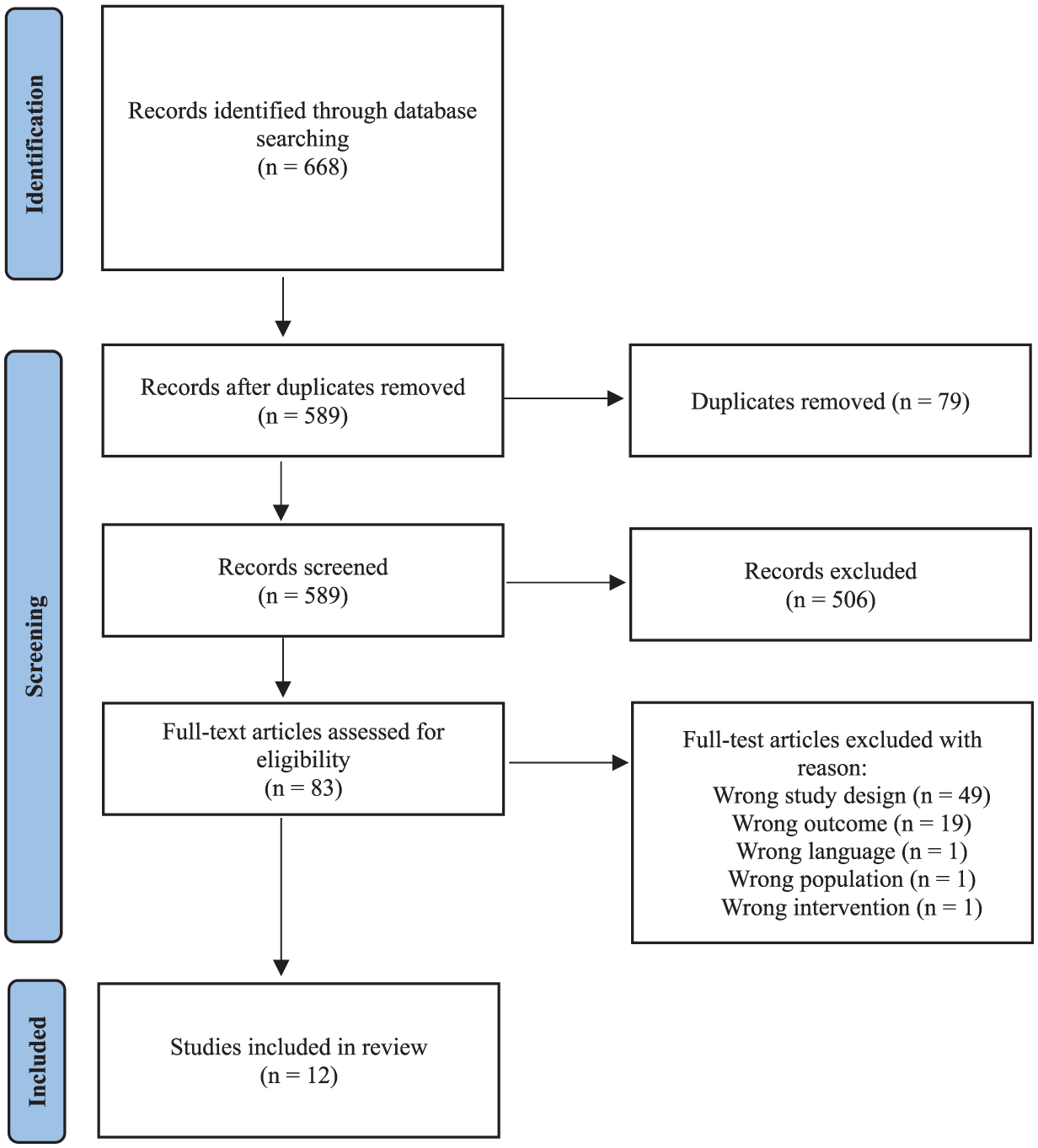
PRISMA flowchart of selected studies during the systematic review process.
Results
Literature Search and Study Characteristics
The search yielded 668 articles, with 589 eligible after duplicate removal. Following full-text screening, 13 studies were selected. These included 1 RCT, 1 prospective cohort study (PCS), 1 retrospective comparison study, 3 retrospective case series, and 7 retrospective cohort studies (RCSs; Tables 2 and 3).7 -9,12 -21 The total patient count was 995, with 1000 (some bilateral fractures) 5MT fractures. Age ranged from 13 to 95.6 years, with a mean of 33.99 years. The studies varied in terms of fracture classifications, treatment approaches, and follow-up durations (range 6-42 months) as summarized in Tables 2 and 3. Across the included studies, definitions of delayed union and nonunion varied considerably (Table 5). Given the scoping review design and heterogeneity in study methodology and outcome definitions, results are described in terms of patterns of association and consistency across studies rather than pooled measures of statistical significance.
Study Characteristics.
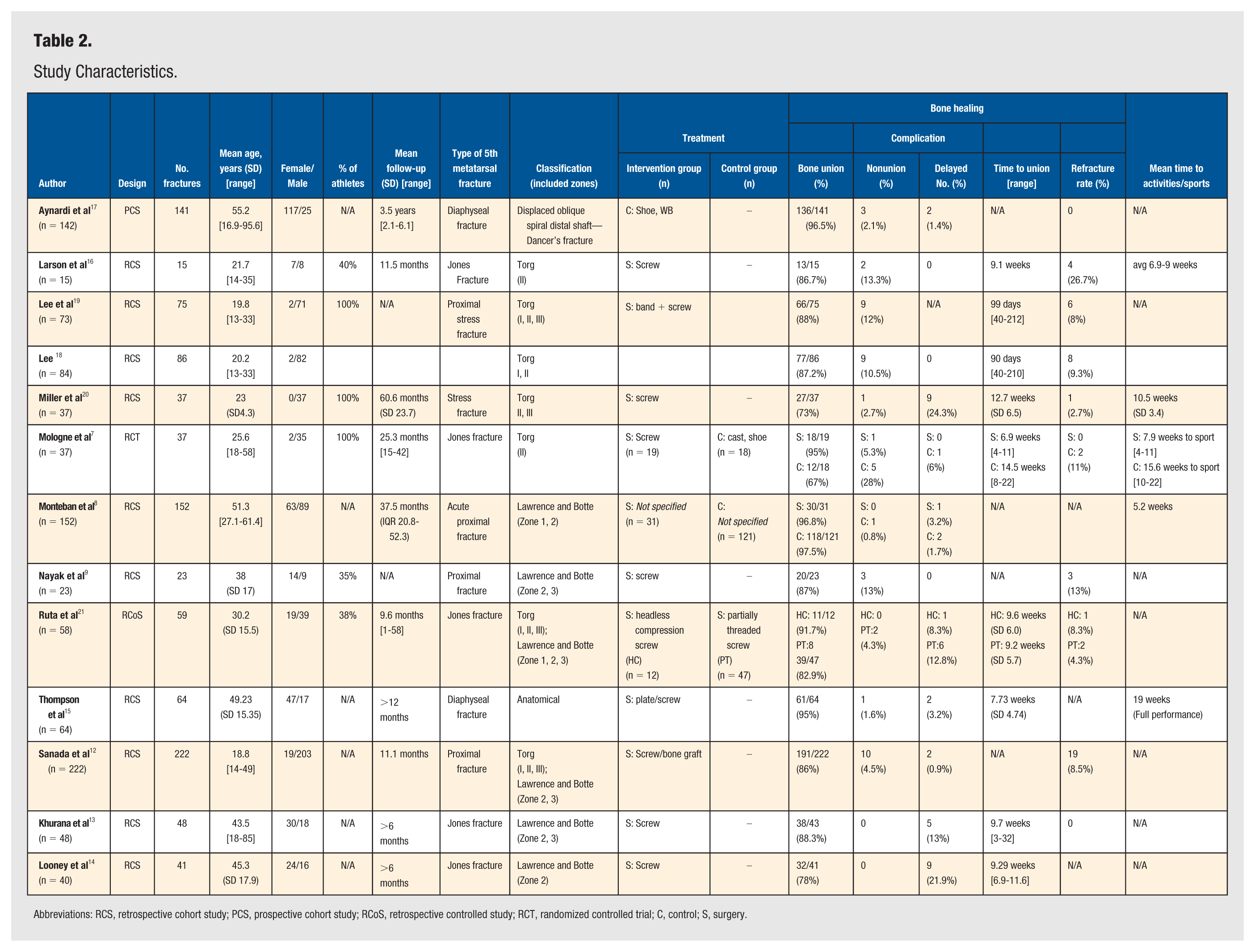
Abbreviations: RCS, retrospective cohort study; PCS, prospective cohort study; RCoS, retrospective controlled study; RCT, randomized controlled trial; C, control; S, surgery.
Study Characteristics, Bone Healing Outcomes, and Complications.
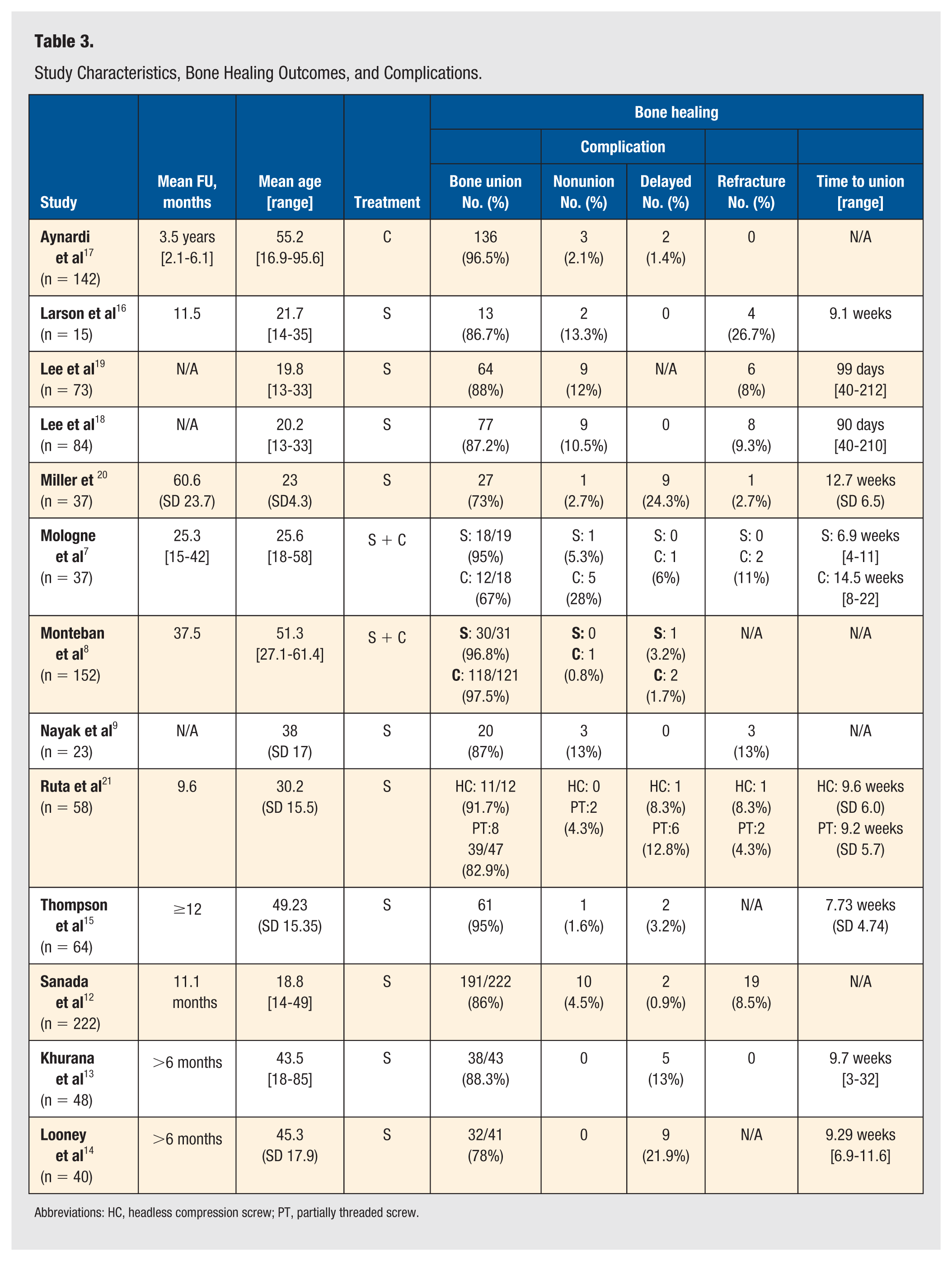
Abbreviations: HC, headless compression screw; PT, partially threaded screw.
Risk Factors for 5MT Fracture Union Deformity
The risk factors associated with union deformity in fifth metatarsal (5MT) fractures can be categorized into demographic factors, fracture characteristics, and treatment-related factors. We summarized each of these categories below. Throughout the review, the statistical and clinical significance of these risk factors is examined, highlighting which variables are most strongly associated with adverse union outcomes such as delayed union, nonunion, or refracture. Identified risk factors for fifth metatarsal fracture union deformity are summarized in Table 4.
Risk Factors for Union Complications in Fifth Metatarsal Fractures: Evidence Strength and Study Sources.
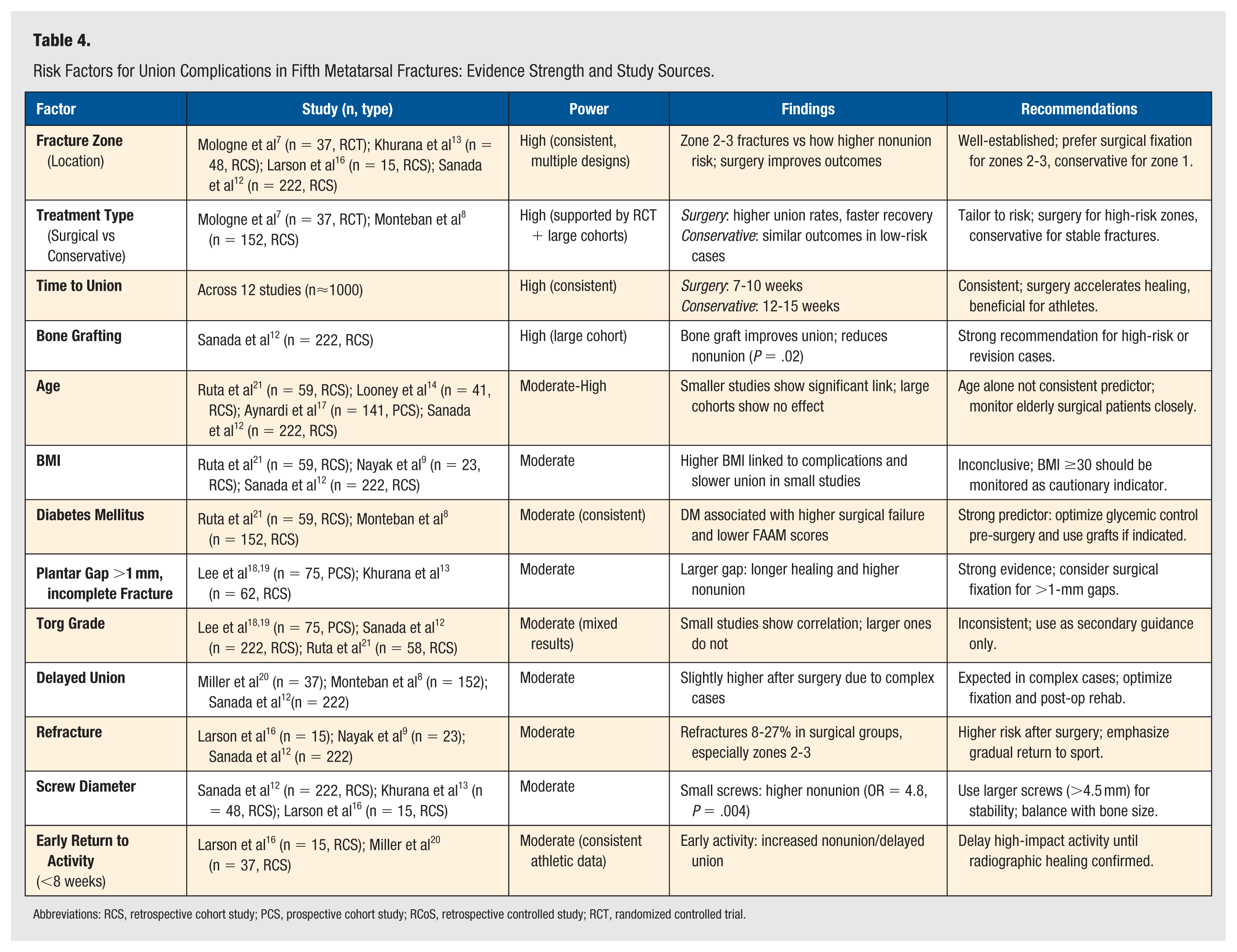
Abbreviations: RCS, retrospective cohort study; PCS, prospective cohort study; RCoS, retrospective controlled study; RCT, randomized controlled trial.
Demographic factors
Increasing age
Four studies assessed age as a risk factor for nonunion.14,18,19,21 Two smaller retrospective cohort studies (Ruta et al, P < .001; Looney et al, P = .031) found a significant positive association between increasing age and surgical failure. Retrospective cohort study (RCS) by Ruta et al 21 included 59 patients with zone 2 and 3 fractures and compared intramedullary partial threaded and headless screws with a follow-up of 9.6 months. Similarly, Looney et al, 14 identified through univariable logistic regression (P = .031) age as a significant risk factor in their RCS of 41 surgically treated patients with zone 2 and 3 fractures. In contrast, 2 higher-powered studies found no significant differences in bone healing outcomes based on age, such as the PCS by Aynardi et al 17 with conservatively treated 141 diaphyseal fractures and a follow-up of 3.5 years, and the large RCS by Sanada et al 12 on predicting bone union disorders following surgical treatment of fifth metatarsal fractures, including 222 zone 2 and 3 stress fractures with an 11-month follow-up. Overall, while smaller surgical series suggest an age-related risk, evidence from larger, methodologically stronger studies indicates that age alone is not an independent predictor of nonunion.
Higher BMI
Of the 3 studies that examined BMI, 2 reported significant findings. Ruta et al 21 identified a statistically significant association between increased BMI and surgical failure (r = .281, P = .03), while Nayak et al 9 found a higher rate of complications in patients with BMI ≥30. However, Sanada et al, 12 in their substantially larger study of 222 patients, did not find a significant relationship between weight, height, or BMI and bone healing abnormalities. In conclusion, the evidence for BMI as a risk factor remains weak due to inconsistent findings and limited statistical power in smaller studies.
Diabetes mellitus
Diabetes mellitus was assessed in 2 studies and significant associations were identified for healing complications.9,21 Ruta et al 21 (n = 59) reported that DM was significantly associated with an increased probability of surgical failure after compression screw fixation of Jones fractures (r = .390, P = .002). Similarly, Monteban et al 8 observed lower functional scores (FAAM) in the diabetic subgroup. These findings suggest that DM is a consistent and clinically meaningful predictor of suboptimal healing outcomes, warranting careful preoperative consideration.
Fracture characteristics
Fracture location
Fracture location appears to be a significant determinant of healing outcomes in 5MT fractures, with zone 2 and, to a lesser extent, zone 3 fractures associated with higher risks of nonunion, delayed union, and refracture compared with zone 1 fractures.7 -9,12 -21 In particular, zone 2 fractures have been repeatedly identified as high risk, with studies such as Larson et al 16 and Khurana et al 13 reporting significantly lower union rates and longer healing times in this zone. However, zone 2 fractures demonstrated improved outcomes with surgical fixation compared to conservative treatment in studies directly comparing these approaches. Mologne et al 7 found that surgically treated zone 2 fractures had a union rate of 95% compared with 67% in conservatively managed cases (P < .05), along with shorter time to union and quicker return to activity. Across studies, current evidence suggests that zone 2 fractures, and selected zone 3 fractures in high-risk or high-demand patients, may benefit more from surgical management, potentially lowering the risk of complications. In contrast, fractures involving well-vascularized regions such as zone 1 typically achieve higher union rates with conservative management than fractures in zones 2 and 3.7,9,13,16 In conclusion, the fracture zone is a significant predictor of healing outcome, with zone 2 and 3 fractures at higher risk for union failure and therefore more likely to benefit from surgical management, whereas zone 1 fractures respond well to conservative care due to favorable vascular conditions.
Incomplete fractures and plantar gap >1 mm
Fracture morphology, specifically plantar gap size and fracture completeness, has been shown to significantly affect healing outcomes in 5MT fractures. In a prospective study of 75 patients with an 18-month follow-up, Lee et al18,19 classified fractures based on completeness and plantar gap size, finding that incomplete fractures with a plantar gap >1 mm exhibited significantly longer union times and higher nonunion rates compared with complete fractures (P < .05). The study emphasized that a plantar gap >1 mm poses a mechanical challenge for achieving adequate compression, even with tension band fixation, likely impairing healing. These findings were further supported by Khurana et al, 13 who studied a cohort of 62 patients with a mean follow-up of 12 months. Their results demonstrated that fractures with a plantar gap required significantly longer healing time with an average of 12.2 weeks compared with 10.8 weeks for those without gaps (P < .05). Both studies highlight the critical role of plantar gap size in influencing union rates and healing outcomes. In conclusion, plantar gap >1 mm and incomplete fracture morphology are significant predictors of delayed union and nonunion, warranting careful consideration for early surgical fixation to optimize mechanical stability and healing outcomes.
Higher Torg classification
The Torg classification evaluates the chronicity and severity of 5MT stress fractures. In a smaller cohort study involving 75 patients with an 18-month follow-up, Lee et al18,19 found a statistically significant relationship between higher Torg grades and prolonged union times (P < .05). These results suggest that higher-grade stress fractures, marked by radiographic features of chronicity, may require longer periods to achieve union. However, these findings were not supported by larger-scale studies. Sanada et al, 12 in a cohort of 222 patients with a mean follow-up of 11.1 months, found no significant association between Torg classification and final bone union rates. Ruta et al, 21 examining 58 patients with Jones fractures, also reported no significant difference in healing outcomes when stratified by Torg grade. Thus, while 2 smaller studies by Lee et al demonstrated a significant association between Torg Type III fractures and delayed union, larger studies failed to replicate these results, suggesting limited generalizability.
Conservative Versus surgical treatment
Union rates
Union rates differ significantly between surgical and conservative treatments depending on fracture risk level, with surgical management showing superior outcomes in high-risk cases (zone 2-3 fractures, stress or chronic, high functional demand, or healing-impairing comorbidities). Nonunion, as defined by Sanada et al, 12 was the absence of a continuous bone bridge after 6 months. In high-risk fractures, such as those in zones 2 and 3, with plantar gaps >1 mm, or classified as Torg Type III, surgical management consistently produced higher union rates.7 -9,12 -21 Lee et al18,19 reported a 97% union rate with intramedullary screw fixation in 75 patients, and Mologne et al 7 found a significantly lower nonunion rate with surgery (5.3%) compared with conservative treatment (28%, P < .01). 8 However, Monteban et al 8 demonstrated similar union rates for surgical (96.8%) and conservative (97.5%) management in low-risk fractures, supporting conservative treatment in zone 1 or non-displaced cases. Definitions of delayed union and nonunion varied across studies and are summarized in Table 5.
Definitions of Delayed Union and Nonunion Across Included Studies.
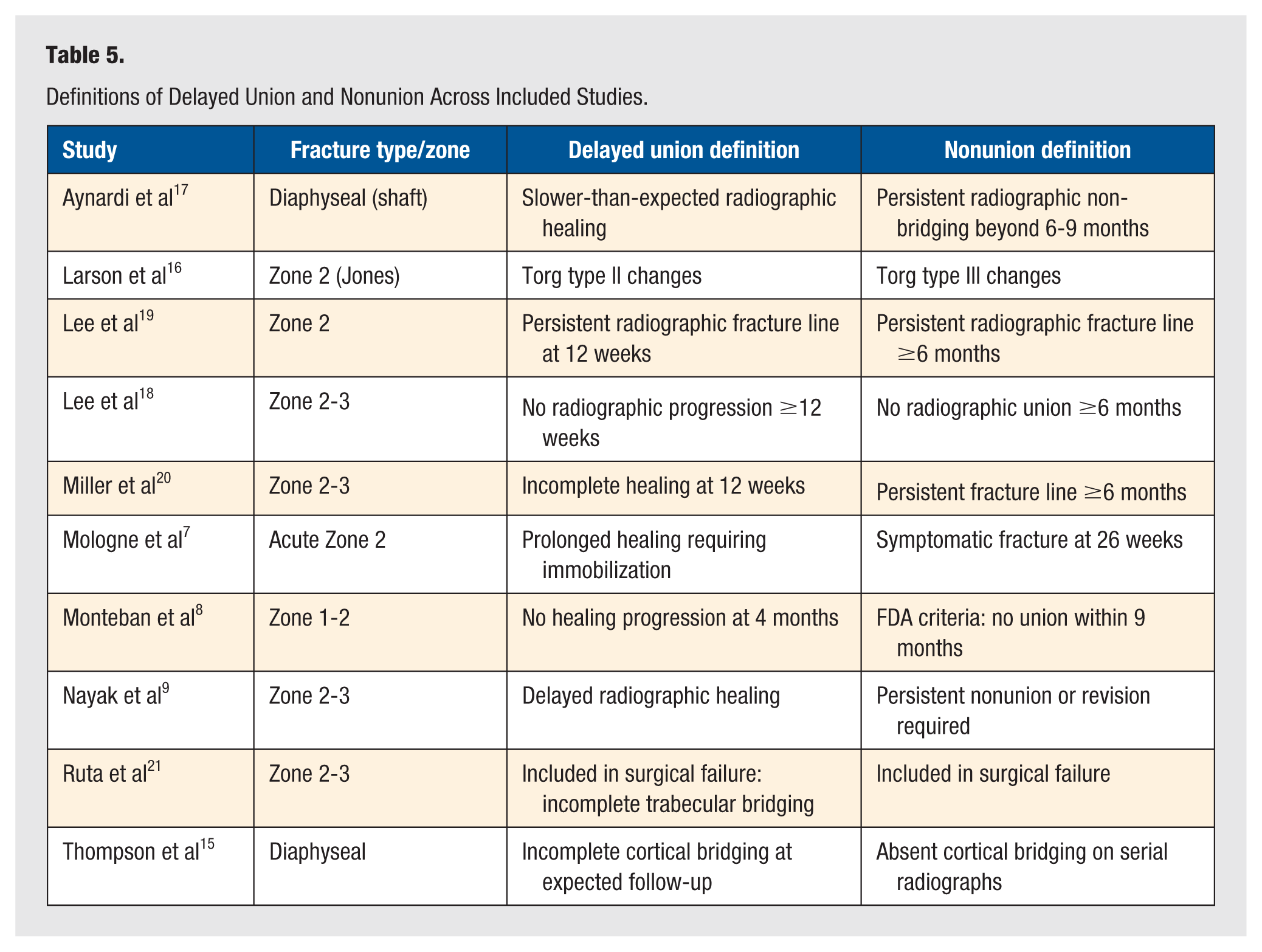
In conclusion, surgical intervention significantly improves union rates in high-risk fractures, whereas conservative treatment remains effective in stable, well-vascularized fractures. This difference likely reflects the mechanical advantage of internal fixation in providing compression and stability in areas of limited vascular supply.
Time to union
Surgical treatment appears to significantly reduce time to union compared with conservative management in 5MT fractures. Across the studies, the average union time was 9.4 weeks, with individual reports ranging from 6.9 to 14.5 weeks.7,8,13 -16,18 -21 The surgical group consistently demonstrated faster and more predictable healing, with mean union times between 7.73 and 14.1 weeks, as reported in multiple studies.12,19,21 In contrast, conservative management showed longer reported healing durations. Mologne et al 7 found a significantly longer union time of 14.5 weeks in nonsurgically treated patients. The available evidence indicates that surgical intervention significantly shortens time to union, especially in cases involving poor vascularity or mechanical instability, whereas conservative treatment may prolong healing, though it remains appropriate for low-risk fractures. The accelerated union after fixation is attributed to increased stability, reduced micromotion, and earlier revascularization of the fracture site provided by screw fixation. Because several studies evaluated restricted cohorts (low-risk or high-risk fractures), differences between surgical and conservative management should be interpreted within those risk profiles.
Delayed union
Delayed union, defined as the absence of a continuous bone bridge after 3 months of treatment 12 was slightly more common following surgical intervention (3.83%) than conservative treatment (2.28%). However, this difference appears to reflect the complexity of surgically treated fractures, rather than the effectiveness of the procedure itself.7,9,12 -16
In surgical treatment, delayed union rates varied widely (0%-24.3%) depending on fracture type and study population. For example, Miller et al 20 reported the highest rate (24.3%) in a high-risk surgical group. Conversely, Lee et al 19 observed no delayed unions in surgically treated zone 3 fractures, suggesting that fracture location and tailored surgical techniques significantly impact outcomes. In contrast, conservative treatment yielded more consistent and generally lower delayed union rates, typically between 1.4 and 6%. For instance, Monteban et al reported a rate of 1.7%, whereas Aynardi et al noted 1.4%.9,12,15,21
In conclusion, while delayed union is slightly more frequent in surgically treated fractures, this likely reflects the higher baseline risk in these patients rather than an inherent disadvantage of surgery. Most surgically treated cases involved complex, high-risk fractures (zones 2 and 3 or chronic stress injuries), which inherently demonstrate slower biological healing regardless of fixation method.
Rehabilitation and return to activity
Across the reviewed studies, surgical treatment consistently demonstrated a faster return to sports and daily activities compared with conservative management.7,12,18,20 This difference was most clearly illustrated in the RCT by Mologne et al, 7 where patients undergoing intramedullary screw fixation returned to sports at a median of 8 weeks, significantly earlier than the 15 weeks observed in the nonsurgical group. Similarly, Larson et al reported a trend toward earlier return to activity among surgical patients, suggesting that operative fixation may allow for more accelerated rehabilitation protocols and earlier functional loading. In contrast, conservative treatment was associated with prolonged immobilization and delayed weight-bearing, often leading to extended recovery timelines despite comparable union rates in low-risk patients. 16 While conservative management demonstrated high union rates in several studies, the extended rehabilitation period poses a limitation for athletes or individuals aiming for a quicker recovery. Miller et al 20 and Larson et al highlighted the risks of early return to activity (<8 weeks) following surgery, associating it with increased rates of complications such as delayed union and refracture. In summary, while both treatment strategies can achieve union, surgical intervention significantly shortens rehabilitation time and may be the preferred option for athletes and patients with time-sensitive recovery goals.7,8,13,14,16,20
Refractures
Of the 12 studies included in this review, 8 reported cases of refracture, with an average rate of 14.1%.7,8,15,16,18 -20 While most studies documented refracture rates below 10%, 2 stood out with higher rates. Larson et al 16 reported a refracture rate of 26.7% in a retrospective case series involving 15 surgical patients with Jones fractures in zone 2, and Nayak et al 9 observed a 13% refracture rate among 23 surgically treated patients with proximal fractures in zones 2 and 3. These findings suggest an association between surgical treatment and an increased risk of refracture in certain fracture locations.
When stratified by treatment strategy, the surgical group demonstrated a higher mean refracture rate of 8.61%, with individual rates ranging from 0% to 26.7%. In contrast, the nonsurgical group exhibited a lower average refracture rate of 2.75%, with a narrower range of 0% to 11%. This trend suggests that surgically treated fractures, often more severe or unstable, are at greater risk of refracture, likely due to underlying mechanical and biological challenges. Fracture location also played a significant role in refracture risk. Refractures were not reported in zone 1 or in distal shaft fractures, which benefit from better vascular supply and reduced mechanical stress. Conversely, refracture rates were higher in more proximal locations: zone 2 showed a rate of 6.67%, and zone 3 had the highest at 8.65%.9,15,16,18 -21 In conclusion, refractures were significantly more common in zones 2 and 3 and occurred more frequently following surgical intervention. While surgery is often necessary for complex or high-risk fractures, these findings suggest that it may carry a higher refracture risk, particularly in less vascularized or biomechanically stressed regions. This higher refracture rate likely reflects early mechanical loading, stress concentration at the screw entry site, and the inherently poor vascularity of proximal fracture zones, rather than a failure of fixation itself. Conversely, nonsurgical management showed lower refracture rates but is typically reserved for more stable fracture types with favorable healing profiles.
Other treatment-related factors
Bone grafts
Bone grafting demonstrates a significant benefit in enhancing union rates in fifth metatarsal (5MT) fractures, particularly in high-risk cases. Sanada et al 12 reported that bone grafting was more frequently performed in patients who achieved normal union compared with those who developed union disorders, with this difference reaching statistical significance (P = .020). 13 Moreover, the absence of bone grafting was associated with a significantly increased risk of nonunion, as reflected by an odds ratio of 3.13 (95% CI, 1.22-8.02; P = .02). Bone grafting was not routinely performed across all studies but was selectively applied in high-risk or revision cases, such as those with delayed union, nonunion, or poor intraoperative vascularity. These findings support the clinical utility of bone grafting in carefully selected patient populations.
Screw diameters for intramedullary fixation
The use of small-diameter screws has been significantly associated with union disorders in fifth metatarsal fractures. Sanada et al 12 found that smaller screws increased the risk of nonunion, reporting an odds ratio of 4.81 (95% CI, 1.62-14.2; P = .004). Smaller screws may fail to provide adequate stabilization, thereby compromising the healing process. However, Khurana et al 13 and Larson et al 16 did not find a clear association between screw diameter and union outcomes, indicating that more evidence is needed to determine its significance as a risk factor. Larger screw diameters are associated with improved stability and higher union rates in fifth metatarsal fractures, particularly in high-risk zones, though excessively large diameters could weaken the bone and increase refracture risk.
Early return to vigorous full activity
Early return to high-impact activity before radiographic union is significantly associated with higher complication rates. Larson et al 16 reported a significant increase in nonunion among patients who resumed activity prematurely (P < .01). Similarly, Miller et al 20 found that professional athletes who returned to play within 8 weeks after surgery had delayed union, although this delay did not prevent continued sports participation. Early loading of the fracture site might impair bone healing and should be carefully managed in postoperative care. In conclusion, early return to vigorous activity, particularly within 8 weeks or before radiographic healing is complete, significantly increases the risk of delayed union and refractures following 5MT fracture treatment.
Discussion
This scoping review identified 4 main categories of risk factors contributing to bone healing complications in fifth metatarsal (5MT) fractures: demographic factors, fracture characteristics, fracture location, and treatment-related factors. Among these, some factors such as DM, use of small-diameter screws without bone grafting, incomplete fractures with a plantar gap greater than 1 mm, and an early return to full activity (particularly within 8 weeks post-surgery) were more consistently associated with an increased risk of nonunion or delayed union. Conversely, other potential factors, such as treatment strategy, athlete status, fracture location, age, Torg classification, and BMI, showed conflicting associations, suggesting that healing outcomes depend on the interaction between patient characteristics, fracture type, and treatment protocols.
Building on these findings, this review provides a comprehensive summary of the existing literature on risk factors associated with bone healing complications in 5MT fractures and explores their implications for clinical practice and research. The principal complications investigated include nonunion, delayed union and refracture. Although numerous studies have examined these outcomes, variations in definitions, classifications, and outcome measures across the literature make direct comparison and standardization difficult. This inconsistency highlights the need for uniform diagnostic and reporting criteria in future work.
Fifth metatarsal fractures are challenging due to their unique anatomy and susceptibility to healing complications, particularly in the vascular watershed region of the 5MT. While studies, such as those by Chloros et al, 22 mention factors such as smoking, nutritional deficiencies, and compliance with weight-bearing restrictions as contributors to healing complications, the studies included in this review did not consistently evaluate these factors. Associations between age and healing outcomes were inconsistent: while Ruta et al 21 and Looney et al identified increasing age as associated with healing complications, other studies did not identify age as an independent predictor. This variability likely reflects differences in cohort composition and treatment selection, with age acting as a surrogate for fracture chronicity, bone quality, or metabolic comorbidities rather than a direct determinant of healing. Supporting this interpretation, Samsonov et al 23 reported prolonged healing in delayed (Torg grade II) fractures compared with acute (Torg grade I) injuries despite lower nonunion rates with internal fixation in athletes. These findings underscore the need to consider a variety of risk factors when assessing and treating 5MT fractures.
Fracture location, particularly zone 2 fractures, appears to be a significant factor influencing healing outcomes. Our review indicates that zone 2 fractures have a higher risk of nonunion, delayed union, and refracture compared to distal shaft and zone 3 fractures. For example, Larson et al 16 and Khurana et al 13 reported lower union rates and longer healing times for zone 2 fractures. However, the data also suggests that surgical intervention in zone 2 fractures may result in improved outcomes. Mologne et al 7 demonstrated a significantly higher union rate (95% vs 67%) and quicker healing times with surgical fixation compared with conservative treatment. Nonetheless, despite some studies suggesting improved outcomes with surgery in zone 2 fractures, the overall evidence remains inconsistent, and more controlled investigations are needed to definitively determine the impact of fracture location on healing parameters.
The debate over the optimal treatment strategy (surgical versus conservative) remains contentious. This review reveals that while surgical intervention generally results in faster healing times (a mean of 10.38 weeks compared with 14.5 weeks in nonsurgical management), the rates of nonunion, delayed union, and refracture vary.7,8,13,15,16,21 Specifically, surgery had slightly lower nonunion rates (6.17% vs 9.35% in nonsurgical groups) but presented a wide range of refracture rates, with some studies reporting rates as high as 26.7%. 16 Conversely, conservative management demonstrated lower delayed union and refracture rates but showed greater variability in bone union rates (ranging from 67% to 97.5%).7,8 Mologne et al reported a statistically significant faster union time and return to sports after surgery, while Monteban et al found no statistically significant difference in healing complications. These mixed results highlight that treatment decisions should be individualized, balancing the benefits of earlier recovery with the risks associated with surgical fixation. Factors such as early weight-bearing and the use of small-diameter screws without bone grafting have been associated with an increased risk of delayed or failed union, suggesting that both the surgical technique and postoperative management play critical roles in determining outcomes.7,8,12,13,16,20
The evidence base remains constrained by methodological heterogeneity, including differences in study design, fracture classification, and definitions of healing outcomes. For instance, Lee et al18,19 defined nonunion as a fracture showing no healing potential for 3 months, whereas Miller et al 20 considered this timeframe indicative of delayed union. These differences underscore the necessity for standardized definitions and uniform reporting practices in future research.
Furthermore, while our review supports the benefits of surgery in specific cases, such as zone 2 fractures, the variability in outcomes across studies highlights the need for RCTs that consider factors like fracture location, grade, and patient activity level. Recent findings by Wang et al 24 suggested that surgical treatment led to faster return to sports and lower pain scores. However, the overall variability in therapy outcomes indicates that further investigation into the optimal treatment strategy for different patient populations is required.
This scoping review has several limitations that are worth noting. Many of the studies in the current literature exhibit variability in both nonsurgical and surgical protocols, as well as small sample sizes and heterogeneity in study designs, treatment methods, and outcome reporting. Additionally, there is a lack of standardized definitions for reporting complications and healing outcomes, leading to inconsistent criteria for delayed union, nonunion, and even fracture types throughout the literature. This highlights the need for standardized and uniform definitions. Achieving consistent outcomes requires the implementation of standardized therapeutic protocols. Furthermore, few studies in this review reported follow-up beyond 12 months, with only a subset providing long-term data on reinjury or return to function. While these findings offer insight into sustained outcomes, the limited number of long-term studies restricts our understanding of how risk factors impact functional recovery over time. At last, a higher degree of power and generalizability may be achieved through larger, multicenter studies. The evidence base would be significantly strengthened by the inclusion of high-quality comparative research that employs standardized definitions, controlled study designs, and uniform reporting practices.
Conclusion
This review highlights the complex interplay of risk factors influencing the healing outcomes of 5MT fractures. While certain factors such as fracture location, patient demographics, and treatment approach have been identified, the evidence remains inconsistent. For
Supplemental Material
sj-docx-1-fas-10.1177_19386400261426853 – Supplemental material for Risk Factors for Union Deformities in Fifth Metatarsal Fractures: A Scoping Review
Supplemental material, sj-docx-1-fas-10.1177_19386400261426853 for Risk Factors for Union Deformities in Fifth Metatarsal Fractures: A Scoping Review by Date Van der Meij, Bradley Weaver, Alireza Ebrahimi, Lorena Bejarano-Pineda, Gregory Waryasz, Peter Kloen, John Y. Kwon and Soheil Ashkani-Esfahani in Foot & Ankle Specialist
Supplemental Material
sj-docx-2-fas-10.1177_19386400261426853 – Supplemental material for Risk Factors for Union Deformities in Fifth Metatarsal Fractures: A Scoping Review
Supplemental material, sj-docx-2-fas-10.1177_19386400261426853 for Risk Factors for Union Deformities in Fifth Metatarsal Fractures: A Scoping Review by Date Van der Meij, Bradley Weaver, Alireza Ebrahimi, Lorena Bejarano-Pineda, Gregory Waryasz, Peter Kloen, John Y. Kwon and Soheil Ashkani-Esfahani in Foot & Ankle Specialist
Footnotes
Authors’ Note
All authors of this article have been involved with the investigation and have approved the paper and agree to its submission and publishing in this journal. This paper is not under consideration in the same or substantially similar form in any other journal.
Author Contributions
Conceptualization, Visualization, and Methodology: SAE, PK, JYK, DM.
Supervision, and Project administration: SAE, PK, LBP, JYK.
Investigation: DM, BW, AE.
Writing and editing: DM, BW, AE, MG.
Reviewing, revising, and finalizing the manuscript: AE, SAE, LBP, JYK, MG.
All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.