
Abstract
We report an open pure ankle dislocation without fracture in a 61-year-old man after a heavy load struck his thigh. Preoperative computed tomographic angiography (CTA) demonstrated entrapment of the posterior tibial, flexor digitorum longus, and flexor hallucis longus tendons together with the tibial neurovascular bundle within a widened tibiofibular syndesmosis. Given irreducibility and risk to the bundle, open reduction was performed with careful disengagement of the entrapped structures, followed by staged dynamic fixation of the syndesmosis. The patient returned to normal activity without pain or limitation of range of motion. Pure ankle dislocation with syndesmotic diastasis accompanied by diminished or uncertain distal neurovascular findings and/or irreducibility should raise suspicion for deep entrapment, for which early CTA may facilitate safer operative planning and help avoid iatrogenic injury from repeated manipulation.
Keywords
“Pure ankle dislocation with syndesmotic diastasis . . . should raise suspicion for deep entrapment . . . CTA may facilitate safer operative planning and help avoid iatrogenic injury from repeated manipulation.”
Introduction
Ankle fractures are common injuries, and dislocation accompanies 21% to 36% of cases.1 -3 In contrast, pure ankle dislocation without accompanying fracture is an exceptionally rare injury, representing less than 0.065% of all ankle injuries. 4 While most dislocations are reducible, some cases present as irreducible due to interference from bone fragments or entrapment of soft tissues such as the joint capsule, ligament stump, posterior tibial (PT) tendon, flexor digitorum longus (FDL) tendon, and flexor hallucis longus (FHL) tendon at the tibiotalar joint or within the tibiofibular syndesmosis. 5 Forceful or blind attempts at closed reduction risk iatrogenic injury, particularly when the tibial neurovascular bundle is entrapped. Although neurovascular bundle entrapment in ankle dislocation has been described, awareness remains limited. Here, we present an open ankle dislocation without fracture in which preoperative computed tomographic angiography (CTA) identified syndesmotic entrapment of the neurovascular bundle and flexor tendons, thereby guiding controlled open reduction and staged stabilization. Because standardized imaging guidance is limited for this rare injury, we propose clinical clues and an imaging algorithm to guide selective CTA when deep entrapment is suspected.
Case Report
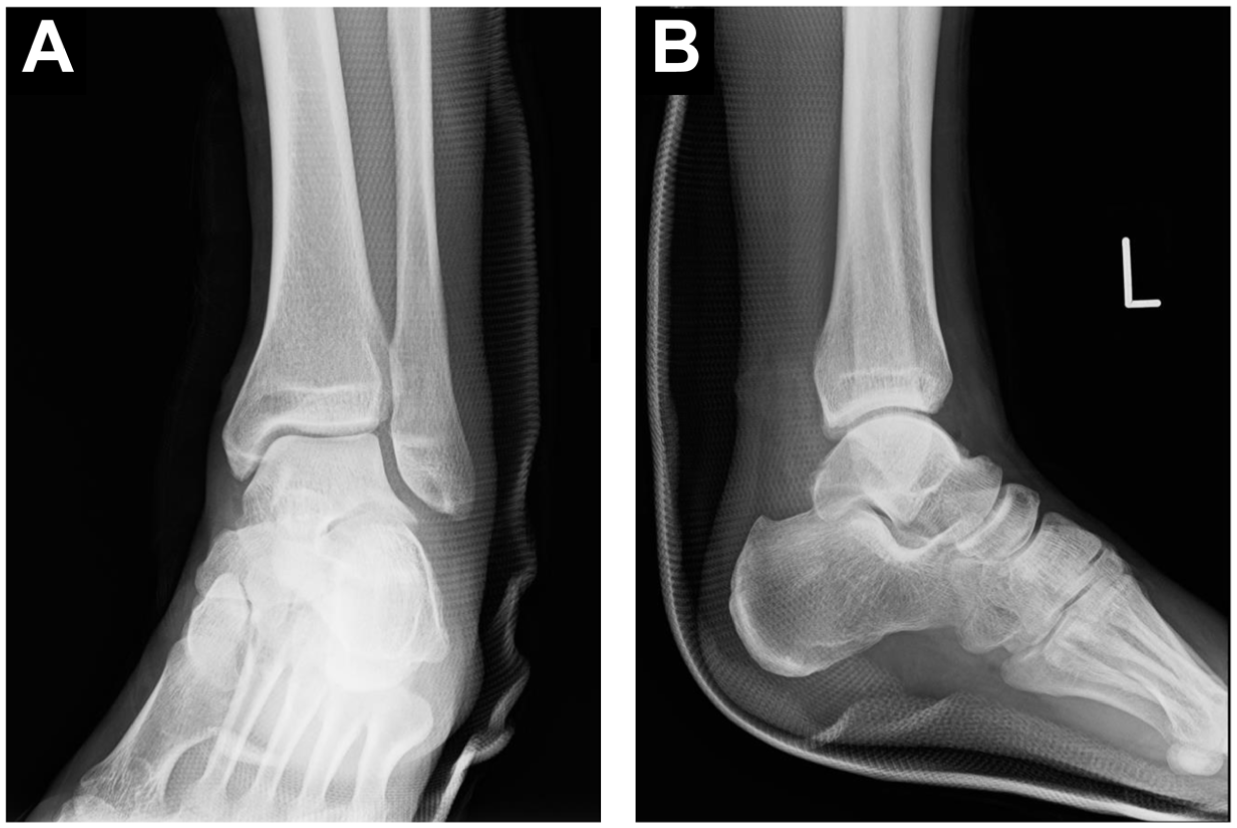
A 61-year-old man was transported to our emergency department after a 250-kg cart fell onto his left thigh at work, with resultant forced abduction and eversion of the left ankle. This resulted in a deformed left ankle and an approximately 15-cm open wound extending from the medial to the posteromedial aspect. There was no active bleeding. The distal tibial plafond and the talar dome were completely exposed, and the ankle was dislocated in an abduction and eversion position (Figure 1). The dorsalis pedis pulse was barely palpable, whereas palpation of the PT pulse was difficult because of the wound. There was no sensory disturbance except around the wound. He denied pain in the left thigh and knee, and inspection of these regions revealed no visible abnormality. Broad-spectrum intravenous antibiotics and tetanus prophylaxis were administered on arrival. Plain radiographs showed no fracture but complete anterolateral tibiotalar dislocation with distal tibiofibular diastasis (Figure 2). A gentle traction and countertraction attempt (knee flexed) at the bedside without anesthesia was unsuccessful
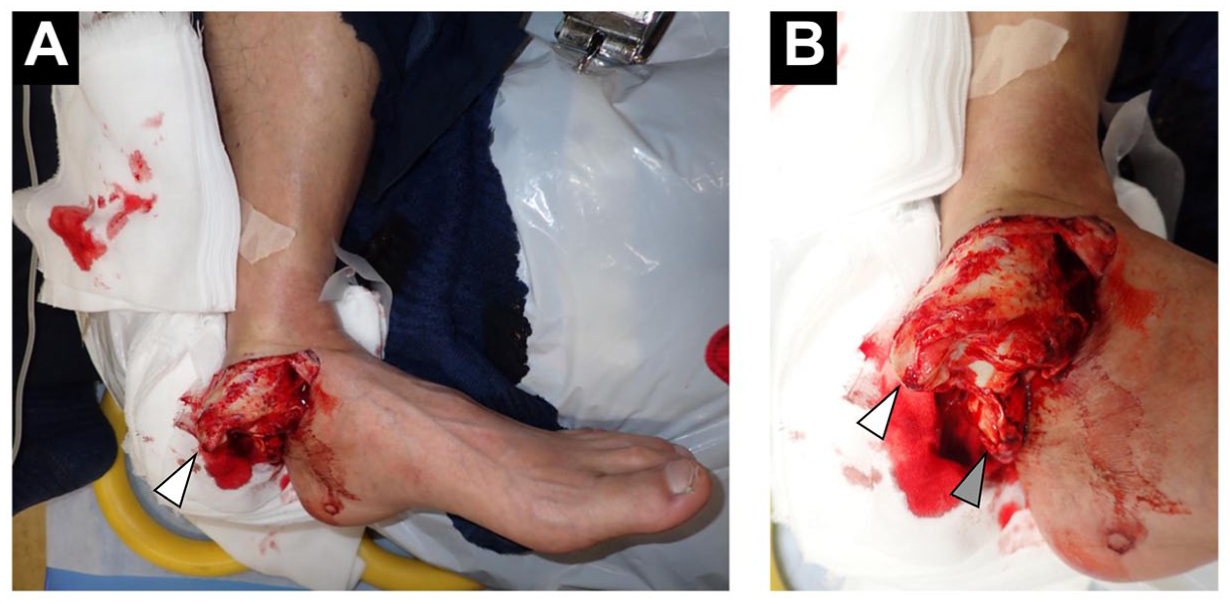
Initial presentation of the left ankle. Clinical photographs show an open dislocation of the left ankle with abduction and eversion deformities, revealing complete exposure of the distal tibial plafond. (A) Entire left lower limb and (B) close-up of the left ankle.

Initial plain radiographs of the left ankle showing complete tibiotalar dislocation without fracture.
On noncontrast CT, no fracture was identified, while the PT, FDL, and FHL tendons were displaced and entrapped within the widened distal tibiofibular syndesmosis. The Achilles tendon remained attached to the calcaneus but was displaced medially. CTA demonstrated the PT artery coursing from posterior to anterior across the widened syndesmosis (Figure 3A and B), and 3D reconstructions delineated its course to the foot (Figure 3C and D). There was no contrast extravasation or abrupt arterial cutoff, and distal opacification to the foot was preserved, suggesting maintained arterial patency. Based on these findings, syndesmotic entrapment of the tibial neurovascular bundle, including the tibial nerve, was strongly suspected. Soft-tissue 3D-CT reconstructions further showed displacement and entrapment of the PT, FDL, and FHL tendons and the PT artery, medial displacement of the Achilles tendon, and dislocation of the peroneal tendons (Figure 4). Before proceeding to surgery, full-length tibia-fibula CT confirmed the absence of a proximal fibular fracture and an intact proximal tibiofibular joint, excluding a Maisonneuve injury. In view of the risk of nerve and vascular injury with forceful manipulation, we avoided further bedside reduction and proceeded directly to emergency surgery under general anesthesia.
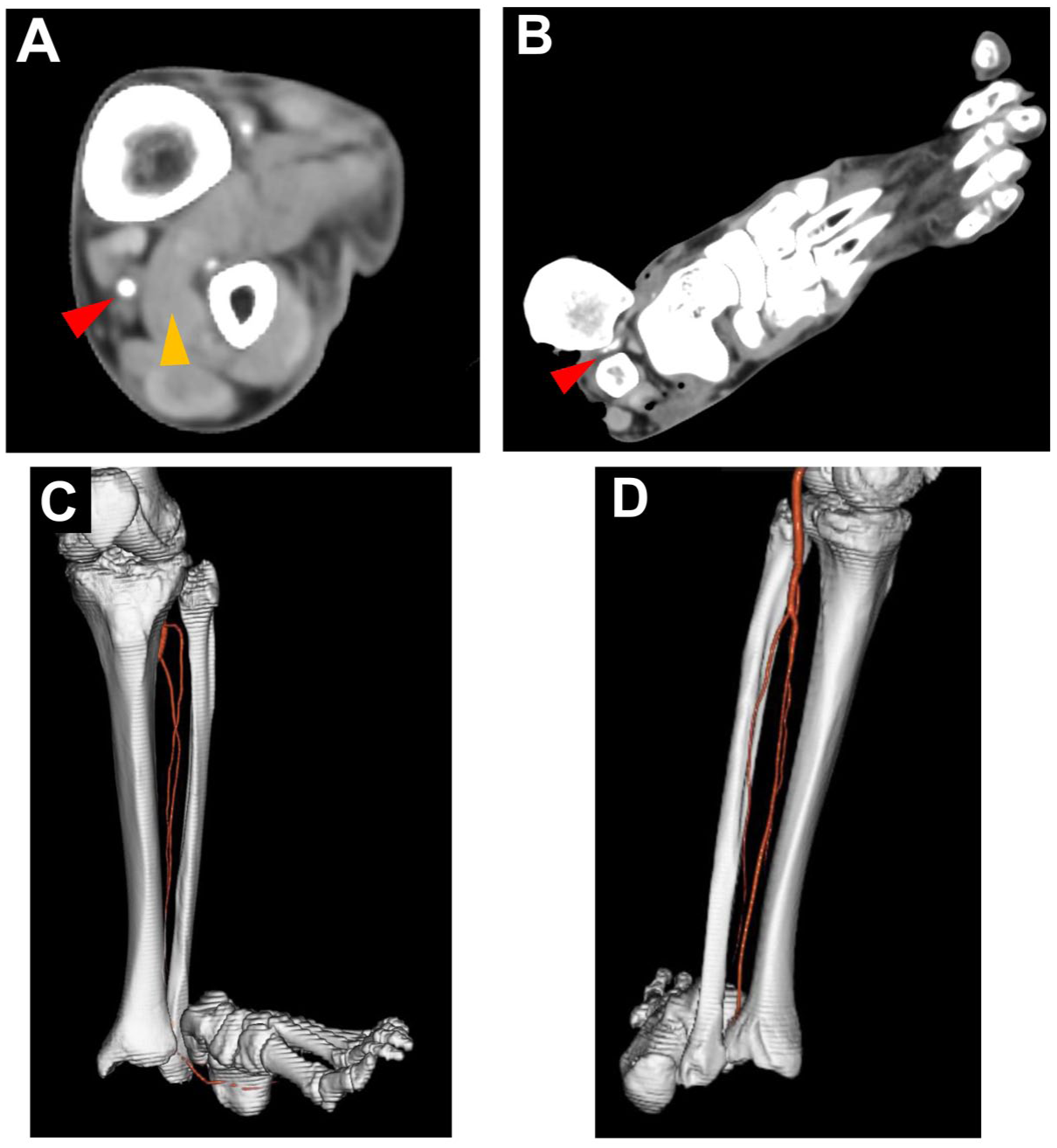
Axial CT angiography (CTA) and 3D CT reconstructions of the left ankle. (A) Axial CTA at the lower leg level, showing entrapment of the posterior tibial (PT) tendon within the widened distal tibiofibular syndesmosis. (B) More distal slice demonstrating the posterior tibial artery traversing the widened syndesmosis. (C) 3D CT (anterior tibial view) showing anterolateral dislocation of the foot and an abnormal course of the posterior tibial artery across the syndesmosis. (D) 3D CT (posteroinferior heel view) showing the posterior tibial artery running posterior‑to‑anterior across the syndesmosis.
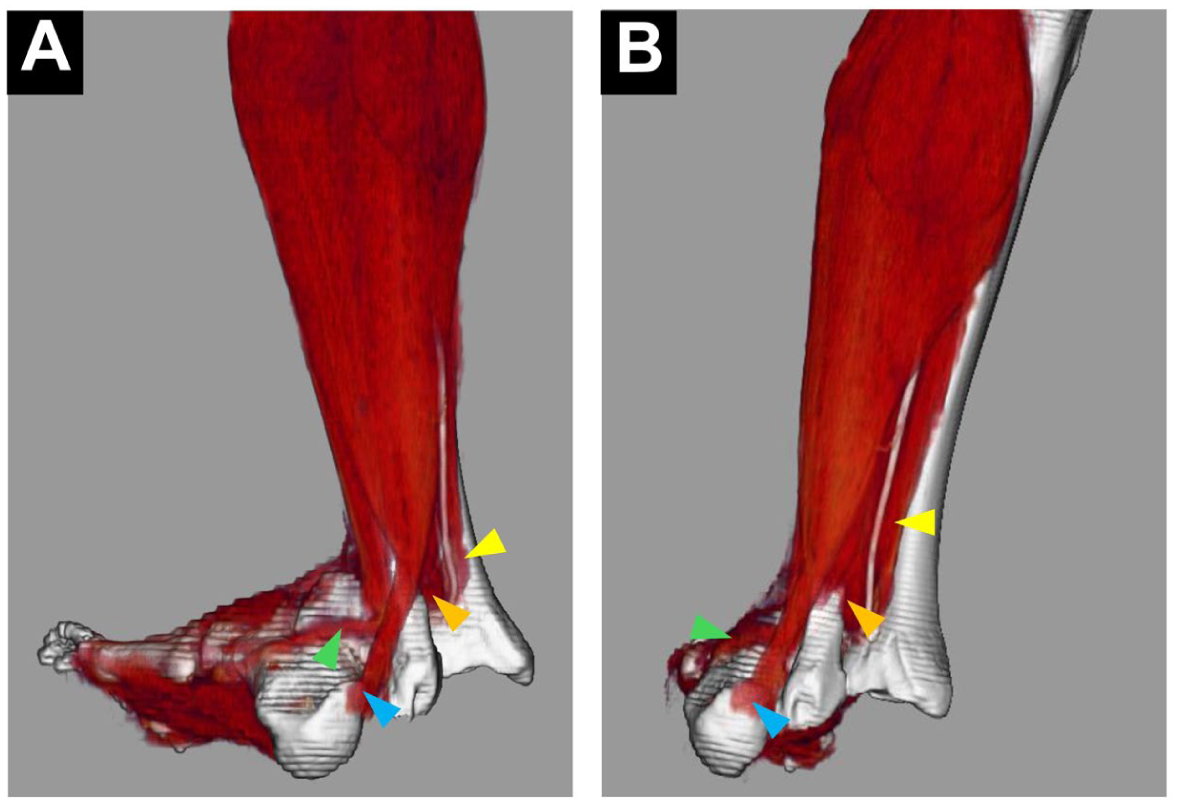
3D CT reconstructions of the left ankle including soft‑tissue structures. (A) Posterior view (tibial aspect) showing medial displacement of the Achilles tendon and dislocation of the peroneal tendons. (B) Posteroinferior view (calcaneal aspect) showing entrapment of the posterior tibial (PT) tendon, flexor digitorum longus (FDL) tendon, and flexor hallucis longus (FHL) tendon, together with the contrast‑enhanced posterior tibial artery/neurovascular bundle within the dislocated distal tibiofibular syndesmosis.
Emergency surgery under general anesthesia was performed with the patient in the supine position, initiated approximately 3 hours after injury. The medial wound was extended. No fracture was present. The deltoid ligament was completely ruptured at its medial malleolar (tibial) attachment. The anterior inferior tibiofibular ligament (AITFL) and posterior inferior tibiofibular ligament (PITFL) were also ruptured. The PT, FDL, and FHL tendons and the tibial neurovascular bundle were displaced from posterior to anterior and entrapped within the syndesmosis, with no gross injury to these structures. Using a blunt muscle hook, the entrapped soft tissues were gently retracted distally, and the talus was guided anterior to the fibula, achieving anatomic tibiotalar reduction. The peroneal tendons and Achilles tendon then reduced spontaneously. Three bone tunnels were created in the medial malleolus using a 1.5-mm Kirschner wire, and the deltoid ligament was repaired using No. 2 FiberWire (Arthrex, Naples, FL, USA) through these tunnels. Primary repair of the AITFL and PITFL was not feasible because of severe tissue damage. The wound edges were debrided by approximately 2 mm; as the surrounding soft tissues were viable, primary wound closure was performed.
Immediately after surgery, postoperative radiographs confirmed anatomic reduction (Figure 5), and distal circulation and sensation were intact. Intraoperative valgus (eversion/external rotation) stress testing demonstrated tibiotalar stability after deltoid repair, although syndesmotic instability persisted. The limb was immobilized in a short leg splint. Primary syndesmotic fixation was deferred given the extensive soft-tissue damage and contamination from the open injury. Our strategy involved a staged procedure. While management alternatives such as immediate trans-syndesmotic screw fixation or temporary external fixation were considered, we favored this approach to minimize implant-related risk in this high-energy open injury. The patient remained non–weight bearing until the second procedure. Serial neurovascular examinations at 24 and 48 hours after the initial emergency surgery confirmed palpable dorsalis pedis and PT pulses with intact plantar sensation and toe flexion (Table 1).
Immediate postoperative radiographs after emergency surgery on the day of injury, demonstrating anatomic reduction of the tibiofibular syndesmosis and the tibiotalar joint. (A) Anteroposterior view. (B) Lateral view.
Serial Vascular and Neurological Assessments After the Initial Emergency Surgery.
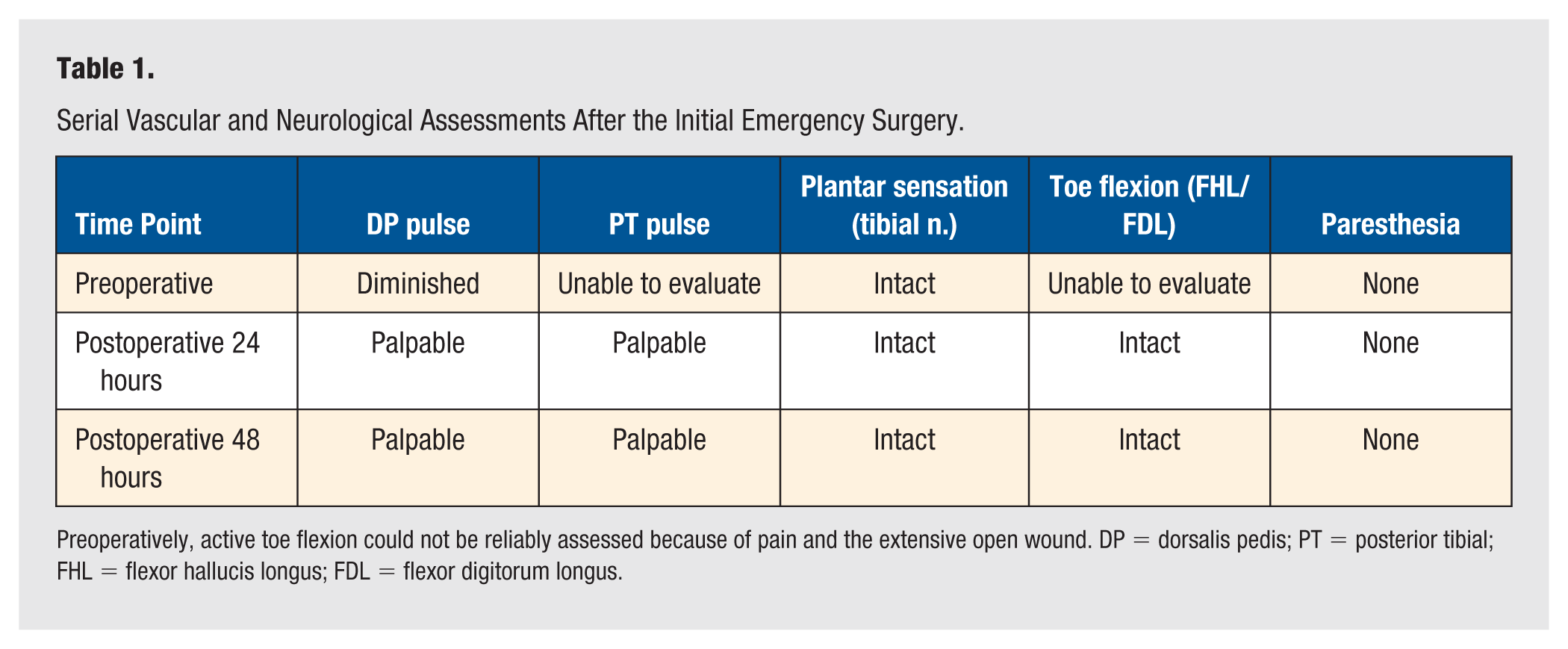
Preoperatively, active toe flexion could not be reliably assessed because of pain and the extensive open wound. DP = dorsalis pedis; PT = posterior tibial; FHL = flexor hallucis longus; FDL = flexor digitorum longus.
Given the persistent syndesmotic instability, staged dynamic syndesmotic fixation was performed on postoperative day 22 with two suture-button devices (ZipTight; Zimmer Biomet, Warsaw, IN, USA). To avoid the initial wound, a new anterolateral incision was made directly over the AITFL to approach the syndesmosis. The devices were placed 1.5 and 4.0 cm proximal to the joint line (Figure 6). Intraoperative fluoroscopy confirmed restoration of the syndesmosis. Partial weightbearing and ankle range-of-motion exercises began the next day, and full weightbearing was achieved 3 weeks after the second procedure. The patient returned to manual labor by 6 months. At 18 months, he had no pain, no motion limitation, no neurologic deficit, or tendon dysfunction, and his American Orthopaedic Foot & Ankle Society (AOFAS) Ankle-Hindfoot score was 90. Radiographically, the syndesmosis remained reduced (Figure 7), without clinical symptoms of instability.

Postoperative radiograph obtained after staged syndesmotic fixation performed 22 days after injury, showing resolution of syndesmotic instability following fixation.

Radiographs obtained at the final follow-up 18 months after injury, demonstrating maintenance of anatomic reduction without recurrent syndesmotic diastasis and without significant osteoarthritic changes.
Discussion
The mechanism in this case is most consistent with axial compression combined with valgus and external rotation applied to the ankle when a 250-kg load struck the thigh. We infer a sequence in which deltoid and tibiofibular ligament disruption produced anterolateral talar displacement with syndesmotic widening, into which the PT, FDL, and FHL tendons, along with the tibial neurovascular bundle, slid anteriorly and became entrapped, creating a firm mechanical block to reduction. Ankle fracture-dislocations in which soft tissues are entrapped in the tibiofibular syndesmosis share common characteristics such as high-energy trauma, Weber type C fractures, pronation external rotation fractures according to Lauge-Hansen classification, widening of the tibiofibular syndesmosis, and irreducible cases.5,6 Although syndesmotic soft-tissue entrapment is well described in high-energy ankle fracture-dislocations, our case highlights a crucial clinical principle. Regardless of the presence of a fracture, specific mechanical conditions can cause deep soft-tissue entrapment, rendering bedside reduction not only impossible but also unsafe because of the risk of iatrogenic neurovascular injury.
Given the extreme rarity of pure ankle dislocation, standardized treatment protocols are lacking. 4 Prior reports have documented irreducible fracture-dislocations due to PT tendon entrapment.7 -9 Concurrent entrapment of the PT and FDL tendons has also been reported.5,10 The interposition of multiple soft tissues can consequently impede reduction procedures. According to Nguyen Van and Nguyen Nang, 11 soft-tissue interposition should be suspected when an ankle dislocation is irreducible. While this injury pattern is exceptionally rare, the combination of a dislocation, widened syndesmosis, and altered neurovascular exam may warrant advanced imaging prior to reduction attempts to avoid iatrogenic injury or delays to the operating room.
Irreducible cases involving incarceration of multiple soft tissues of the ankle require appropriate preoperative imaging evaluation. We selected CTA over other options, such as magnetic resonance imaging (MRI) or Doppler ultrasound. In this acute trauma setting, CTA was the most practical modality that could rapidly and simultaneously provide three essential pieces of information: confirmation of the absence of fracture, delineation of the entrapped soft-tissue anatomy, and definitive mapping of the vascular course. While nerves are not directly visualized, an abnormal arterial trajectory, such as the PT artery traversing the syndesmosis in our case, is a strong indicator of neurovascular bundle displacement. Complementary noncontrast CT with soft-tissue windows and 3D reconstructions can further delineate the abnormal tendon paths and the three-dimensional relationship among the talus, fibula, and entrapped tissues, thereby informing a safe surgical approach. 5 The importance of this precise preoperative mapping is underscored by reports of persistent subluxation and chronic pain resulting from missed PT tendon incarceration.8,12,13
If CTA had not been performed in the present case, soft-tissue entrapment would likely have been suspected because of the firm mechanical block; however, the concurrent involvement and displaced course of the tibial neurovascular bundle within the widened syndesmosis might not have been anticipated preoperatively. This uncertainty could have encouraged repeated or forceful reduction attempts and/or less controlled exposure, increasing the risk of iatrogenic injury to the PT artery and the accompanying tibial nerve and delaying definitive management. Prior reports of missed or delayed recognition of deep tendon interposition describe persistent talar malalignment or subluxation, chronic pain or stiffness, and the potential need for extensive reconstructive or salvage procedures.6,11,12 In many of these previously reported cases, deep soft-tissue interposition was identified intraoperatively after failed closed reduction or recognized only after persistent malreduction on imaging; in contrast, CTA in our case enabled preoperative mapping of the entrapped tendons and the neurovascular bundle. Thus, delineation of the PT artery on CTA, although the nerve itself is not directly visualized, served as a useful landmark indicating the likely location of the accompanying tibial nerve and facilitated safer operative planning. Computed tomographic angiography should be used selectively, balancing radiation exposure and the risk of contrast-induced nephropathy, particularly when syndesmotic diastasis coexists with diminished or uncertain distal neurovascular findings and/or irreducibility with a firm mechanical block after a single gentle attempt (Figure 8).
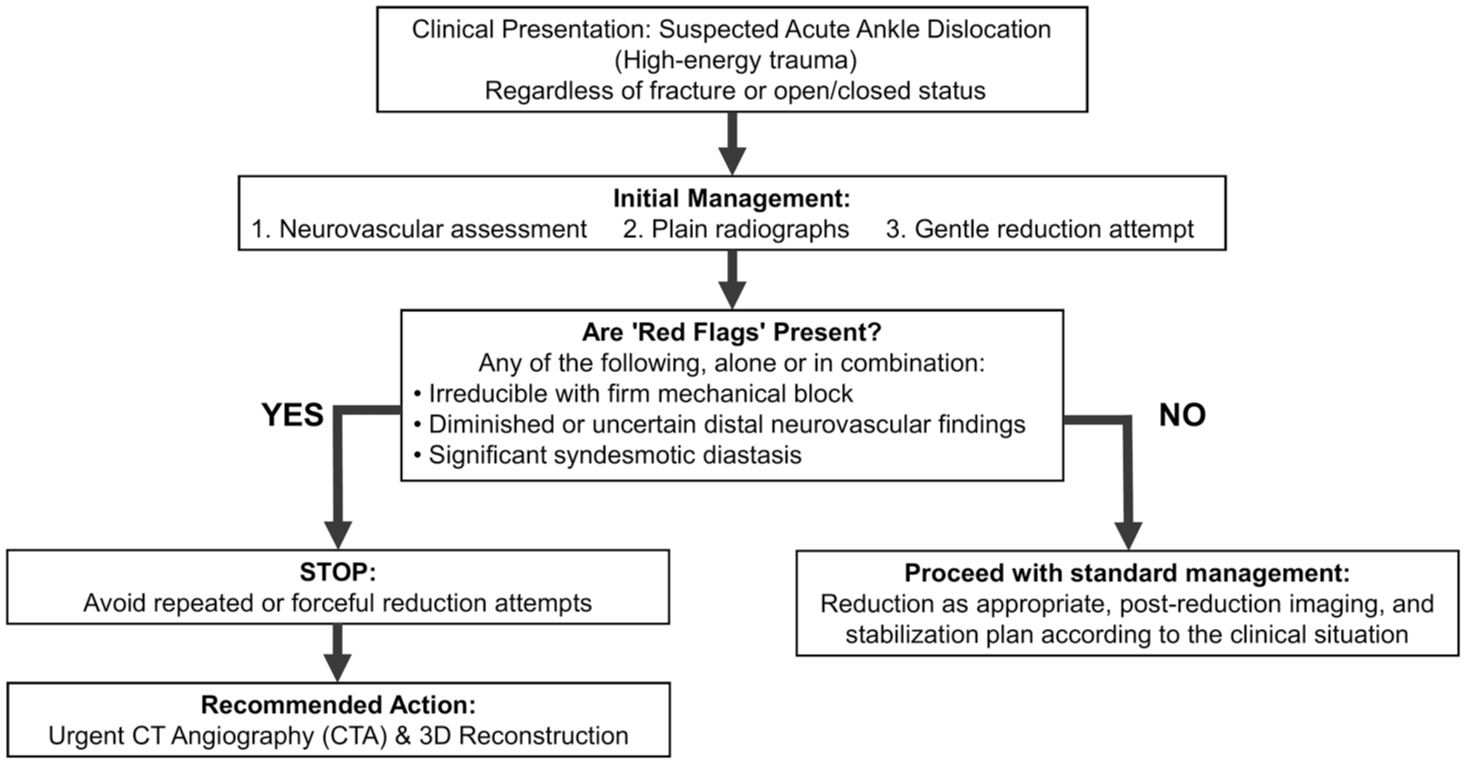
Suggested imaging algorithm for selecting computed tomographic angiography (CTA) in suspected pure ankle dislocation.
Our therapeutic strategy was predicated on the clinical diagnosis of an irreducible ankle dislocation with uncertain distal vascular status, with CTA providing essential anatomical detail for preoperative planning. The primary goals were a controlled open reduction with meticulous disengagement of the entrapped neurovascular bundle, primary deltoid repair to restore tibiotalar stability, and staged dynamic syndesmotic fixation after the soft-tissue envelope had recovered, a standard principle in managing severe open injuries. This approach facilitated early mobilization and, with an uncomplicated postoperative course, resulted in an excellent functional outcome. This report has limitations, including its single-case design and the inherent risks of radiation and contrast exposure with CTA, which necessitate careful consideration of its indications. Nevertheless, it underscores a crucial clinical lesson: in any irreducible ankle dislocation, soft-tissue entrapment involving the neurovascular bundle must be suspected, and preoperative CTA is an invaluable tool for ensuring a safe and effective surgical intervention.
Conclusion
In any high-energy ankle trauma with an irreducible dislocation, entrapment of multiple soft tissues, including the tibial neurovascular bundle, within the tibiofibular syndesmosis should be considered, regardless of the presence of a fracture. Selective preoperative CTA may be valuable for identifying this limb-threatening pattern, guiding controlled open reduction, and helping avoid iatrogenic injury, particularly when syndesmotic diastasis accompanies diminished or uncertain distal neurovascular findings and/or a firm mechanical block after a single gentle reduction attempt.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board (IRB) approval was waived in accordance with our institutional policy for single‑patient case reports, which are not considered human subjects research and therefore do not require prior IRB review or approval.
Informed Consent
Written informed consent was obtained from the patient for publication of the clinical details and accompanying images in this case report.
Trial Registration
Not applicable.