
Abstract
Background
Plantar fasciitis (PF) is the leading cause of chronic heel pain in adults, impairing mobility and quality of life. Radial extracorporeal shockwave therapy (rESWT) is widely used in physiotherapy for its practicality and cost-effectiveness. However, heterogeneity in study designs and protocols limits conclusions regarding its efficacy compared with other electrophysical modalities (EPMs). This systematic review and meta-analysis aimed to synthesize the immediate effects of rESWT, alone or combined with conventional physiotherapy, versus other EPMs, focusing on pain and functional outcomes.
Methods
A systematic search of PubMed, CINAHL, Scopus, Web of Science, and PEDro was conducted up to April 2025 to identify randomized controlled trials (RCTs) comparing rESWT, alone or combined with non-electrophysical interventions, versus other EPMs in adults with PF. Pain intensity and functional disability were the primary outcomes. Meta-analyses were performed using random-effects models, with sensitivity analyses conducted according to outcome type and comparator. Certainty of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation approach.
Results
Fourteen RCTs (n = 797) were included, of which 12 contributed to the meta-analysis. Radial extracorporeal shockwave therapy did not demonstrate superiority over other EPMs for pain reduction (standardized mean difference [SMD] = −0.03; 95% confidence interval [CI]: −0.39 to 0.33) or functional improvement (SMD = −0.11; 95% CI: −0.47 to 0.25). Low-level laser therapy showed small but statistically significant advantages over rESWT for functional outcomes. Overall risk of bias (RoB) was high across most studies.
Conclusions
Radial extracorporeal shockwave therapy, alone or combined with physical therapy, does not appear superior to other EPMs for PF. The high heterogeneity and overall elevated RoB limit the certainty of these findings, highlighting the need for high-quality trials to guide clinical recommendations.
Level of Evidence:
Level I: Systematic Review
Keywords
“High heterogeneity and overall elevated RoB limit the certainty of these findings, highlighting the need for highquality trials to guide clinical recommendations.”
Introduction
Plantar fasciitis (PF) represents the most common etiology of chronic heel pain in adults, imposing substantial limitations on mobility and diminishing overall quality of life.1,2 Its point prevalence is estimated at 0.85% in the general population, being higher in women, individuals aged 45 to 64 years, and those with obesity or diabetes, with lifetime prevalence reaching up to 10%.3,4 Additional risk factors frequently reported include limited ankle dorsiflexion, elevated body mass index (BMI), prolonged standing or weight-bearing occupations, excessive foot pronation, and high running volume. 5
The condition typically manifests with gradual-onset pain localized to the medial calcaneal tuberosity, which is most severe during initial weight-bearing after prolonged rest (eg, morning steps) and intensifies with sustained activity. 6 Contrary to traditional pathophysiological models emphasizing inflammation, current histopathological and biomechanical analyses have redefined PF as a degenerative fasciopathy.7,8 Emerging evidence reveals repetitive microtrauma-induced collagen degeneration, characterized by fibroblastic hyperplasia, disordered fiber architecture, and extracellular matrix remodeling—all hallmarks of a failed healing response rather than classical inflammation. 6 This paradigm shift underscores the need for targeted therapeutic strategies addressing tissue repair rather than anti-inflammatory interventions.
The diagnosis of PF remains predominantly clinical, relying on a detailed patient history and targeted physical examination. Key diagnostic findings include point tenderness over the medial calcaneal tubercle and pain provocation upon passive dorsiflexion of the metatarsophalangeal joints. 6 While characteristic symptomatology often suffices for diagnosis, advanced imaging modalities—particularly high-resolution ultrasonography—provide valuable adjunctive insights. Ultrasonographic evaluation not only confirms the diagnosis by visualizing fascial thickening, hypoechogenicity, and perifascial fluid but also quantifies structural degeneration, facilitating objective assessment of disease severity and longitudinal monitoring of therapeutic efficacy. 9
The management of PF encompasses a spectrum of conservative interventions, including strengthening and stretching exercises, 10 nocturnal dorsiflexion splinting, 11 foot orthoses, 12 nonsteroidal anti-inflammatory drugs, 13 corticosteroid injections, 14 and physical therapy. 15 Despite the wide array of available treatments, the optimal management strategy for chronic PF remains a subject of ongoing debate, with clinical evidence demonstrating heterogeneous efficacy across modalities.
Among the advanced physical therapy modalities, extracorporeal shockwave therapy (ESWT) has gained recognition as a viable second-line intervention for persistent PF. The therapeutic mechanism of ESWT involves the targeted delivery of acoustic pressure waves, which appear to mediate clinical improvement through multiple pathways: neuromodulatory effects via hyperstimulation, stimulation of angiogenic factors promoting neovascularization, enhancement of local microcirculation, and activation of tissue repair mechanisms at the cellular level. 16 It is generally considered a safe treatment with minimal transient side effects. 17
A critical distinction exists between the 2 principal forms of ESWT: focused (fESWT) and radial (rESWT) modalities. Although both modalities generate mechanical pressure waves, they exhibit fundamentally different physical characteristics and energy transfer mechanisms. fESWT delivers precisely calibrated high-energy acoustic waves that converge at a predetermined tissue depth, enabling accurate targeting of deep anatomical structures with concentrated energy deposition. 17 Conversely, rESWT employs a ballistic mechanism where a projectile strikes an applicator, generating radially propagating pressure waves that dissipate across a broader superficial area. The energy delivered by rESWT is typically lower and less focused than fESWT, making it suitable for treating superficial and broader painful areas. 17 Emerging evidence suggests that rESWT may exert its therapeutic effects through multiple pathways, including modulation of nociceptive signaling, attenuation of inflammatory mediators, and stimulation of tissue repair mechanisms through enhanced vascular perfusion.18,19 These fundamental differences in energy delivery and biological effects have important clinical implications, as they may significantly influence treatment outcomes for various musculoskeletal conditions.
Current systematic reviews and meta-analyses examining ESWT for PF20-25 often share a methodological limitation, which is the lack of differentiation between rESWT and fESWT modalities. This may mask important differences in clinical effectiveness, particularly for rESWT, the modality more commonly employed in physiotherapy practice due to its practical advantages, including simpler administration, larger treatment area coverage, and more favorable cost-effectiveness profile compared with fESWT.17,26 The unique physical properties and widespread clinical adoption of rESWT justify its independent evaluation. Existing studies have investigated rESWT’s therapeutic value for chronic PF, both as a stand-alone intervention and in conjunction with other electrophysical modalities (EPMs). Nevertheless, the available evidence presents considerable heterogeneity, with variations in study designs, treatment protocols, and outcome measures, highlighting the need for a systematic review to synthesize current knowledge and address this gap.
As far as the authors are aware, no previous studies have directly compared rESWT with other EPMs regarding pain and functional outcomes in PF, highlighting the novelty and clinical significance of this work. Accordingly, this review aims to synthesize the immediate therapeutic effects of rESWT, whether applied as a stand-alone intervention or in combination with conventional physiotherapy, compared with other EPMs, with pain and functional capacity as the primary outcomes due to their close association with treatment success and quality of life.
Methods
Protocol and Registration
This study was structured in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for systematic reviews and meta-analyses. 27 The protocol was registered in the International Platform of Registered Systematic Review and Meta-Analysis Protocols (inplasy.com) under the code INPLASY202570111.
Eligibility Criteria
Inclusion Criteria
The selection of studies was based on the PICO strategy, considering the following criteria:
Population. Adult patients (18 years or older) diagnosed exclusively with PF in its acute or chronic stage.
Intervention. Radial extracorporeal shockwave therapy administered either as a stand-alone treatment or combined with other interventions that do not involve EPM.
Comparator. Any EPM (excluding ESWT) that is not combined with topical or injectable treatments.
Outcomes. Pain intensity and functional disability (measured through physical tests or self-reports).
Study design. Randomized controlled trials (RCTs) published in English, with no date restriction.
Exclusion Criteria
Studies were excluded if:
Patients were diagnosed with PF associated with any other clinical condition.
They did not include any measure of pain and/or functional disability.
They were classified as gray literature (non–peer-reviewed sources).
Information Sources and Search Strategy
The electronic search was conducted without filters in 5 databases: PubMed, CINAHL, Scopus, Web of Science, and PEDro, from inception until April 6, 2025. Reference lists of selected studies were also screened, and an additional search was carried out in Google Scholar.
The search terms were organized according to the Population, Intervention, Comparison, Outcome (PICO) strategy and included both MeSH descriptors and commonly used terms in the field The detailed search strategy for all databases is provided in the Supplemental Material 1.
Study Selection Process
All records retrieved from the databases were managed using the Rayyan platform. 28 After removing duplicates, 2 independent reviewers (CCP and LRL) screened titles and abstracts to identify potentially eligible studies. Subsequently, the preselected articles were assessed in full text independently by the same reviewers (CCP and LRL). In case of disagreements, a third author (FGR) intervened to resolve them. Inter-rater agreement was calculated using the Kappa index.
Data Extraction
Relevant information was collected using a standardized form specifically designed for this study, which included: author, year, and country; participant characteristics; types of interventions, comparators, and applied protocols; assessment tools; and main outcomes. For the purposes of this meta-analysis, “immediate effects” were operationally defined as outcomes assessed at the first post-intervention time point reported in each included RCT, regardless of the exact follow-up interval. Two reviewers performed this task independently (CCP and LRL), and a third researcher (FGR) verified the consistency.
Risk of Bias
Risk of bias (RoB) was assessed using the Cochrane RoB-2 tool 29 to evaluate bias across 5 domains, classifying each as “low risk,” “some concerns,” or “high risk.” Two reviewers independently performed this assessment (CCP and LRL), and a third author (FGR) resolved any discrepancies. The figures were generated using the Robvis tool. 30
Certainty of the Evidence
The certainty of evidence for each main outcome was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. 31 Evidence from RCTs was initially rated as high certainty and downgraded based on RoB, inconsistency, indirectness, imprecision, and publication bias. The detailed GRADE evidence profiles and summary of findings tables are provided as Supplemental Material.
Data Synthesis and Analysis
Statistical analyses were conducted using RevMan 5 software (Review Manager [RevMan], Version 5.4, The Cochrane Collaboration, 2020). Effect sizes were expressed as mean differences (MD) or standardized mean differences (SMD), selected according to the homogeneity of the measurement instruments used in the primary studies. The default random-effects model was applied for all comparisons, given the expected clinical and methodological variability among the studies. However, a fixed-effect model was used in analyses where heterogeneity was minimal (I2 < 30%) and the studies were highly comparable.
When means and standard deviations (SDs) were not directly reported, conversions from medians and interquartile ranges were performed using validated methods.32,33 Statistical heterogeneity was quantified using the I2 (inconsistency index), interpreted according to the ranges suggested in the literature (not important: 0%-40%, moderate: 30%-60%, substantial: 50%-90%, considerable: 75%-100%). 34
Sensitivity analyses were conducted to evaluate the robustness of the findings, stratifying the meta-analyses by outcome type, comparator group, and outcome assessment instrument. Additional analyses were performed excluding outlier studies to assess the influence of extreme values on the overall effect estimates.
Results
Research Results
A total of 564 records were identified from the databases, of which 234 duplicates were removed. Subsequently, 330 records were screened by title and abstract, and 35 full-text articles were assessed in detail. Of these, 14 met the eligibility criteria.35-48 Of these studies, 12 were included in the meta-analysis.35-39,42-48 Inter-reviewer agreement at the eligibility screening stage was “almost perfect” (k = 0.826; SE = 0.096; 95% confidence interval [CI] = 0.639-1.014). Figure 1 presents the PRISMA flow diagram of the study selection process.
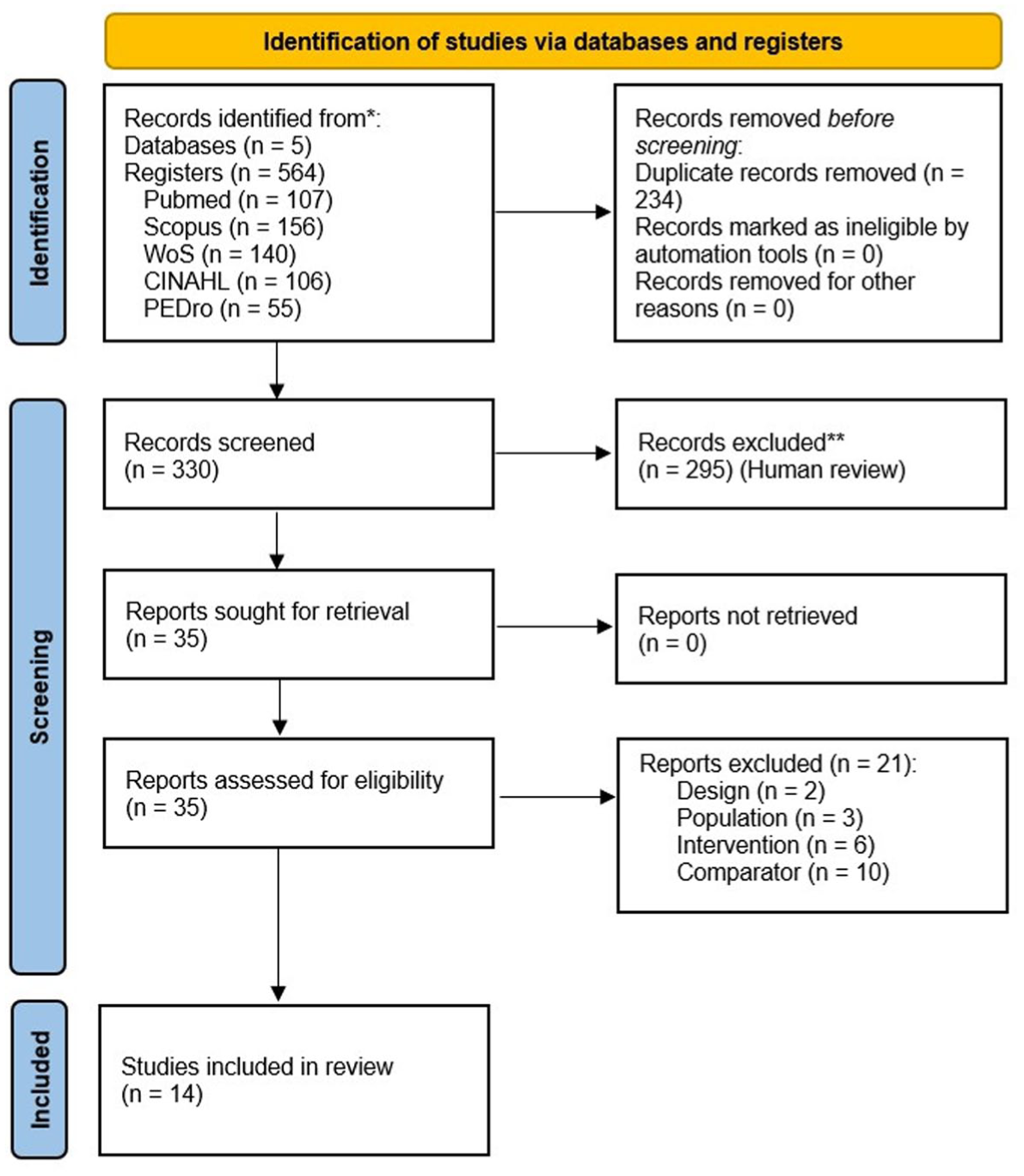
PRISMA flow diagram.
Characteristics of Included Studies
Of the 14 articles included in this review, 6 were conducted in Turkey,35-37,45-47 2 in Brazil,40,41 2 in Thailand,43,44 1 in Pakistan, 42 1 in Greece, 38 1 in Saudi Arabia, 39 and 1 in Iran. 48 The publication years ranged from 2009 to 2024, with 1 article published in 2009, 41 1 in 2013, 40 1 in 2015, 43 2 in 2017,35,46 3 in 2018,36-38 1 in 2019, 47 1 in 2020, 42 2 in 2023,39,44 and 2 in 2024,45,48 indicating sustained interest in this topic over time. The characteristics of these studies are summarized in Table 1. Although several of the included studies examined various outcomes, our meta-analysis focused specifically on pain and functional variables.
Characteristics of the Included Studies.
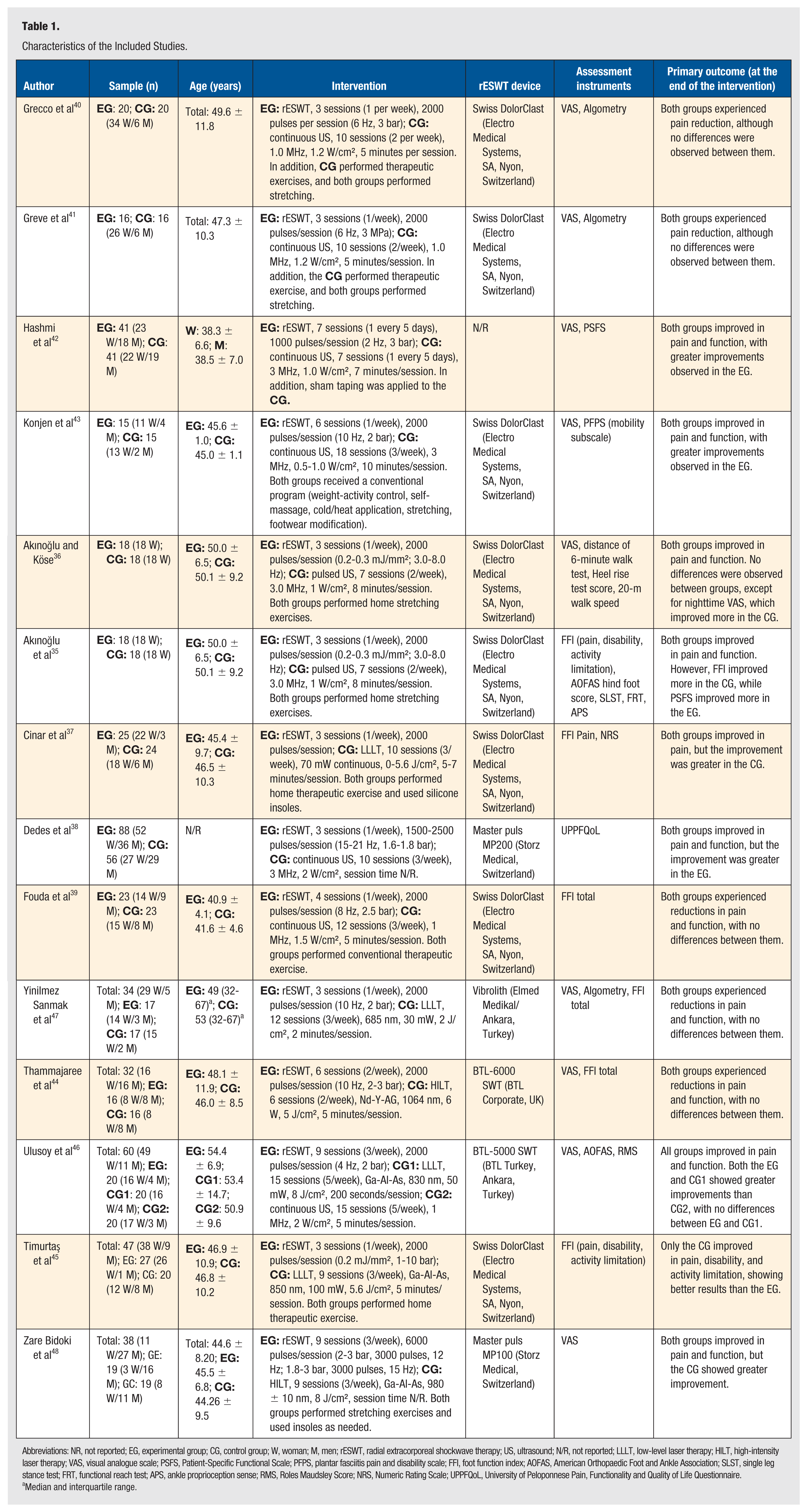
Abbreviations: NR, not reported; EG, experimental group; CG, control group; W, woman; M, men; rESWT, radial extracorporeal shockwave therapy; US, ultrasound; N/R, not reported; LLLT, low-level laser therapy; HILT, high-intensity laser therapy; VAS, visual analogue scale; PSFS, Patient-Specific Functional Scale; PFPS, plantar fasciitis pain and disability scale; FFI, foot function index; AOFAS, American Orthopaedic Foot and Ankle Association; SLST, single leg stance test; FRT, functional reach test; APS, ankle proprioception sense; RMS, Roles Maudsley Score; NRS, Numeric Rating Scale; UPPFQoL, University of Peloponnese Pain, Functionality and Quality of Life Questionnaire.
Median and interquartile range.
RoB
Based on the detailed assessment using the RoB-2 tool, 13 of the 14 studies were rated as having a high overall RoB. Only one study 37 was classified as having some concerns in its overall RoB. One study 38 showed a high risk in all domains, whereas 3 studies43,44,46 exhibited a high risk in a single domain.
Overall, domains D1 (7 studies) and D3 (10 studies) were the most favorably rated across most articles, while domains D2 (6 studies), D4 (8 studies), and D5 (6 studies) presented the highest RoB. Figure 2 provides a visual representation of the RoB for each study, and Figure 3 presents a summary assessment of each domain along with the overall RoB.
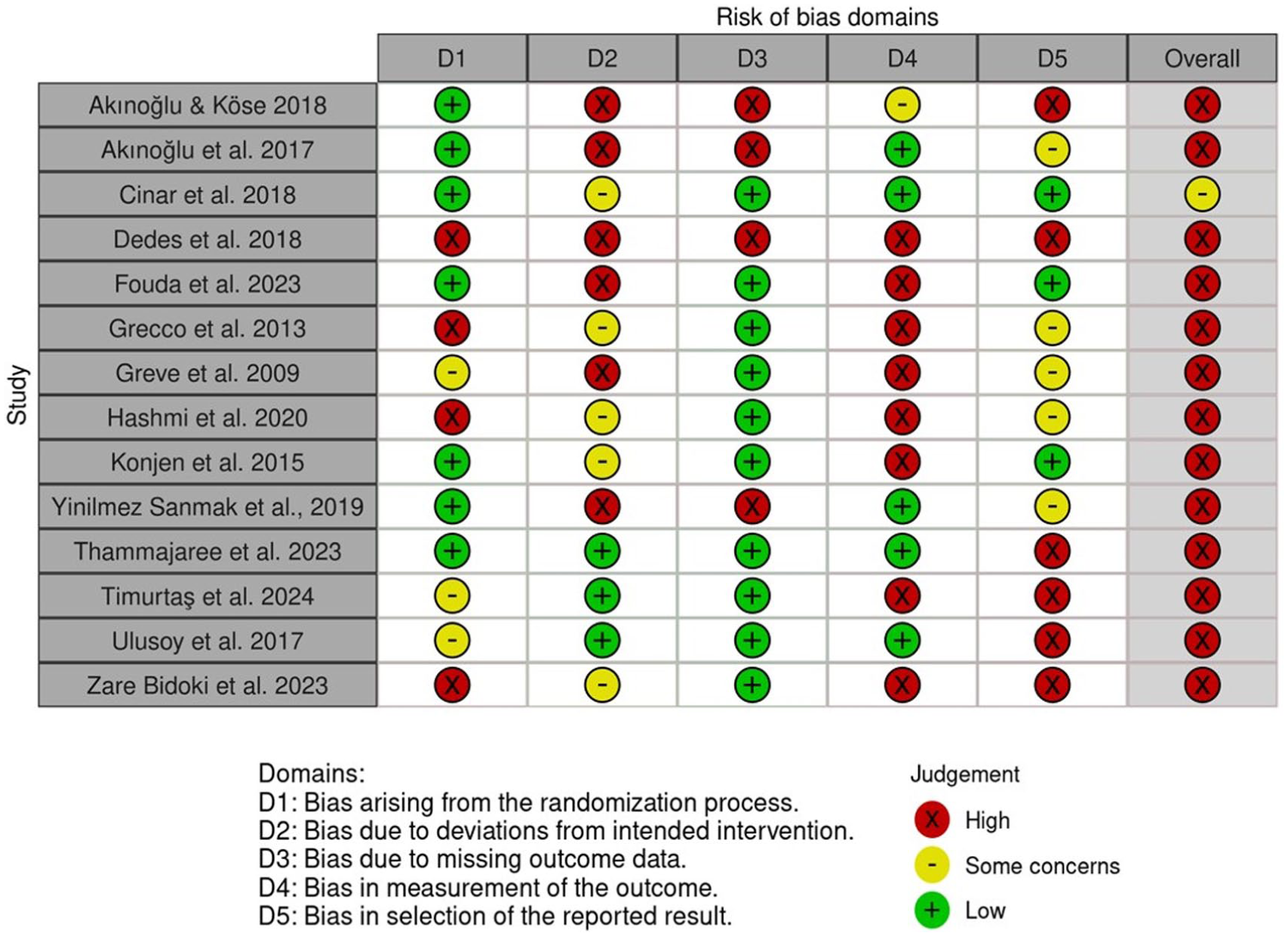
Risk of bias traffic light plot.
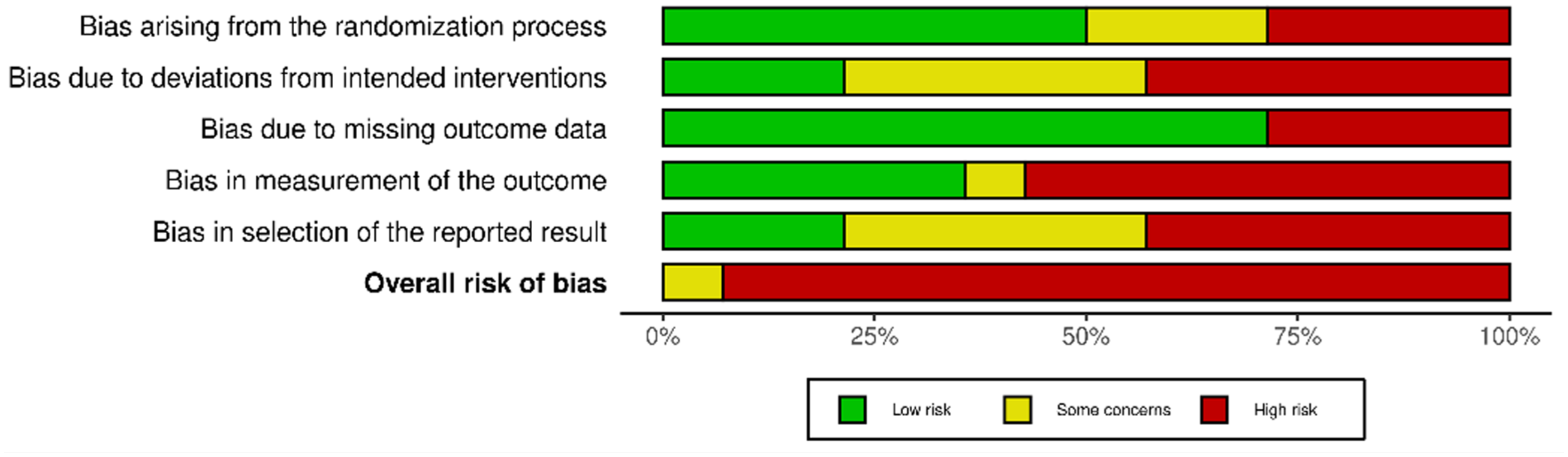
Risk of bias summary plot.
Characteristics of the Population
Among the 14 selected studies, a total of 797 individuals with PF were included. This cohort comprised 230 men and 567 women. Sample sizes varied across studies, ranging from 30 participants
43
Considering studies that reported participants’ ages, these ranged from 18 to 75 years, in accordance with the inclusion criteria. Seven studies required the presence of PF diagnosed based on baseline clinical parameters (commonly first-step pain or tenderness on plantar fascia palpation).37,39,43-47 Four studies required both clinical and imaging parameters (radiography showing calcaneal spur or ultrasound [US] confirming PF).35,36,40,41 One study required confirmation by a medical professional, 48 and 2 studies only required that participants had a PF diagnosis without specifying particular criteria.38,42 Seven studies included patients with PF symptoms of at least 3-month duration.35,36,39-41,43,46
Characteristics of Interventions and Outcome Measures
The interventions in the experimental groups (EGs) included rESWT either as a stand-alone treatment or combined with exercises. In the control groups (CGs), 9 studies used US,35,36,38-43,46 our used low-level laser therapy (LLLT),37,45-47 and 2 employed high-intensity laser therapy (HILT),44,48 either alone or in combination with other treatments. One study in particular 45 included 2 CGs with EPM (LLLT and US). 46
Regarding the EGs, 7 studies applied rESWT combined with home exercises (HE),35-37,40-42,45 4 applied rESWT alone,38,44,46,47 2 applied rESWT combined with conventional physical therapy (CPT)39,43 and 1 applied rESWT combined with stretching exercises in an unspecified context. 48 In the CGs, 4 studies applied US + HE,35,36,40,41 2 US + CPT,39,43 2 US alone,38,46 1 US + taping, 42 2 LLLT + HE,37,45 2 LLLT alone,46,47 1 HILT alone, 44 and 1 HILT + stretching in an unspecified context. 48
With respect to the devices used, 7 studies employed the Swiss DolorClast device (Electro Medical Systems, SA, Nyon, Switzerland),35-37,39-41,43,45 2 used BTL devices (BTL-5000 y BTL-6000 SWT [BTL Industries, Ltd., Stevenage, UK]),44,46 2 used Masterpuls MP200 (Storz Medical AG, Tägerwilen, Switzerland),38,48 1 used Vibrolith ESWT (Elmed Medikal Sistemler, Ankara, Turkey), 47 and 1 study did not specify the device. 42
Concerning rESWT dosing protocols, treatments were applied 1 to 3 times per week, with a total of 3 to 9 sessions over 3 to 6 weeks. Each session comprised 1000 to 3000 impulses, at frequencies ranging from 2 to 21 Hz (most commonly 6-10 Hz), and pressures of 1.6 to 3 bar or energy flux densities of 0.2 to 0.3 mJ/mm2 . Session duration ranged from 5 to 10 minutes, depending on the number of impulses and applied energy. Treatment was administered both at the origin of the plantar fascia and along its length or at the site of pain, with energy adjusted according to pain tolerance.35-48
Among the comparative interventions, the most frequently applied was US (in continuous or pulsed mode, typically at 20%), with intensities ranging from 0.5 to 2 W/cm2 and frequencies of 1 to 3 MHz, administered for 5 to 10 minutes per session, with a total of 7 to 18 sessions delivered 2 to 5 times per week.35,36,38-43,46 Low-level laser therapy was applied using Ga-As or Ga-Al-As devices, with wavelengths between 685 and 850 nm, powers of 30 to 100 mW, and energy doses ranging from 2 to 8 J/cm2 . Applications targeted the insertion and the body of the plantar fascia, with session durations of 1 to 7 minutes. Treatment frequency ranged from 3 to 5 sessions per week over 3 to 4 weeks, totaling 9 to 15 sessions.37,45-47 High-intensity laser therapy protocols included 6 to 9 sessions, administered 2 to 3 times per week over 3 weeks. Dosages involved segmented applications of 150 J per session in 3 phases (rapid scanning, focal impulses, and slow scanning), as well as Ga-Al-As laser at 980 ± 10 nm with a dose of 8 J/cm2 over 10 cm2 areas. In both cases, treatment was directed at the plantar fascia.44,48
Complementary interventions primarily consisted of exercises focusing on muscular and plantar fascia stretching, usually performed at home. Frequency ranged from 2 to 3 times per day for 3 to 4 weeks, including repetitions of 10 to 30 seconds per set. Some studies incorporated muscle strengthening, friction massage, orthotic insoles, night splints, and application of compresses. These adjunct strategies were common in both the rESWT and EPM groups, potentially influencing the interpretation of the specific effect of each primary intervention.35-37,39-43,45,48
Radial extracorporeal shockwave therapy interventions showed some variability in frequency and pressure, although most studies applied 2000 impulses per session once weekly for 3 weeks. Control groups were more heterogeneous regarding the type of EPM, number of sessions, and combination with exercises. Adjunct therapies and co-interventions, such as CPT, stretching, and orthotic insoles, were common across both arms.
Primary outcomes focused on pain assessment, predominantly using the Visual Analog Scale (VAS), applied at various time points such as first-step morning pain, at rest, or during physical activity.36,40-44,46-48 Some studies complemented this measure with pressure algometry40,41,47 or applied the Numeric Rating Scale (NRS).37,45 Regarding function, instruments included the foot function index (FFI),35,37,39,44,45,47 the American Orthopaedic Foot & Ankle Society Ankle-Hindfoot Score,35,46 the Patient-Specific Functional Scale (PSFS)42,43 and the Roles Maudsley Score (RMS). 46 Other studies incorporated specific functional tests such as the 6- and 20-minute walking tests, heel-raise test, static and dynamic balance assessments, proprioception using the Biodex III, and joint range of motion measured with an inclinometer.35,36,39 Some studies also reported quality of life, notably using the University of Peloponnese questionnaire 38 and the short form-36. 48 Overall, the studies demonstrated moderate diversity in assessment methods, with a predominance of validated scales for foot pain and function.
Effects of Interventions, Heterogeneity, and Sensitivity Analysis
For the meta-analysis, forest plots were generated from 12 studies, depending on the different outcomes reported in each of them.35-39,42-48 The studies by Greve et al 41 and Grecco et al 40 were excluded due to insufficient data for a robust quantitative synthesis. To enhance the sensitivity of the analysis, both the overall evaluation of the studies for each outcome (pain, function) and their subgrouping based on the type of comparator and method of functional assessment (questionnaire/scale, functional test) were included. When the same outcome was assessed in different contexts (eg, specific actions or times of the day), each measurement was included separately within the same meta-analysis to accurately capture context-specific variations. To complete all meta-analyses, the means and SDs of 3 studies37,45,47 had to be estimated indirectly using validated methods.
During data extraction, it was noted that one study 43 presented unusually low SDs for the VAS variable (measured in mm). Therefore, results are reported both including all studies and in a separate analysis excluding this study.
Meta-Analysis of Pain Outcome
rESWT Versus All EPMs
The overall meta-analysis on the effect of rESWT versus various EPMs (Figure 4) on pain reduction included 11 studies.35-38,42-48 The effect size was marginal and not significant (SMD = −0.03; 95% CI: −0.39 to 0.33; aP = .87), indicating that, overall, rESWT did not demonstrate superiority over the comparator interventions for this outcome. Heterogeneity was high (I2 = 86%; P < .00001), suggesting considerable variability among studies, possibly attributable to differences in application protocols, sample characteristics, and outcome measures. Excluding the outlier study, 43 yielded an estimate of SMD = 0.01; 95% CI: −0.36 to 0.37 (also including the null value) and I2 = 83%, indicating that these parameters remained largely unchanged. Therefore, although the direction of effect slightly favored rESWT (or the EPM when excluding the outlier), the width of the confidence interval and the lack of statistical significance limit its clinical interpretation.
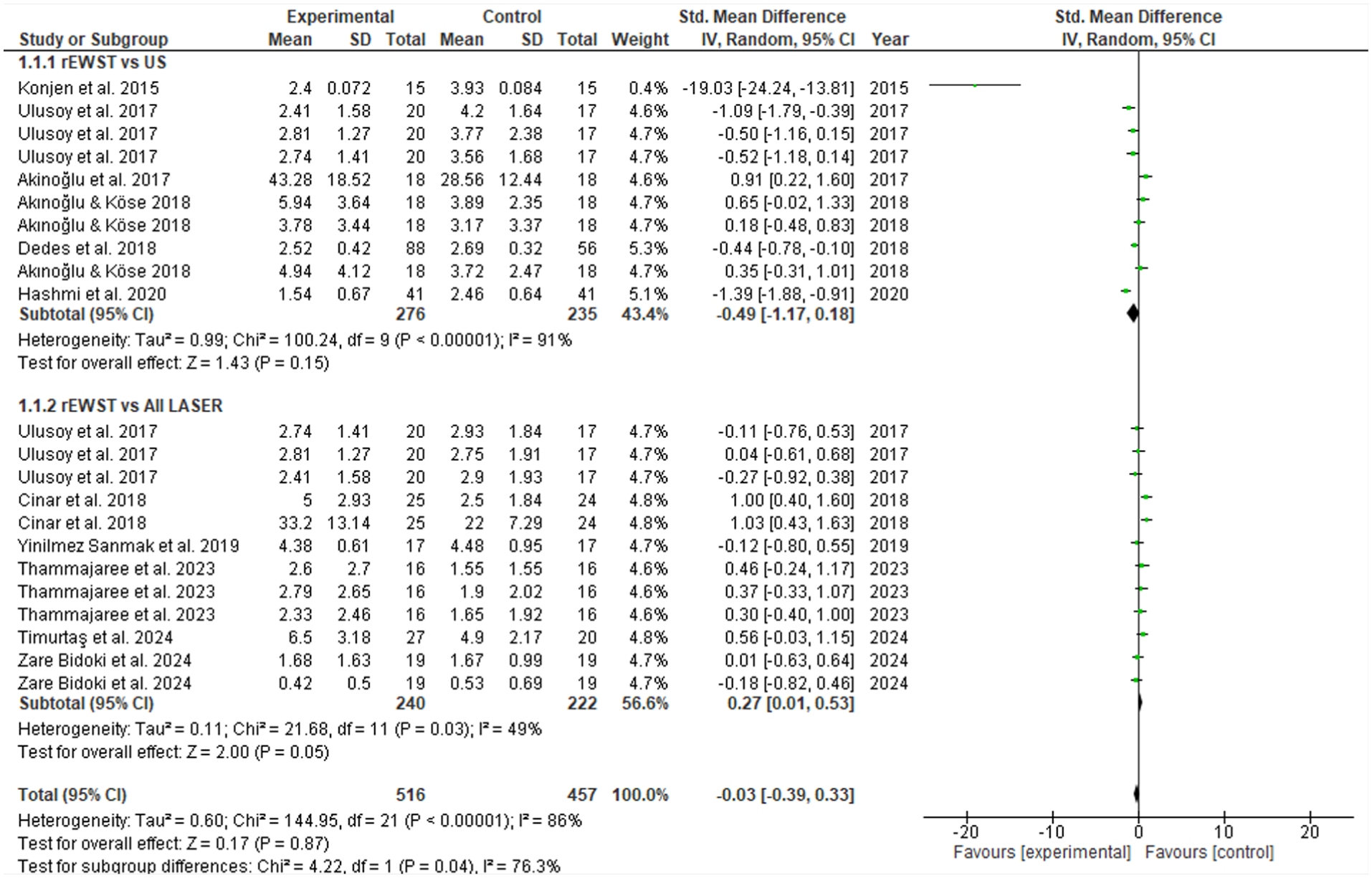
Forest plot of rESWT versus all EPM, and subgroups of US and all lasers, for pain.
rESWT Versus US
The subgroup analysis of rESWT versus US for pain reduction included 6 studies.35,36,38,42,43,46 The effect size was small and not significant (SMD = −0.49; 95% CI: −1.17 to 0.18; P = .15), with a direction favoring rESWT, although without reaching statistically or clinically conclusive relevance. Heterogeneity was high (I2 = 91%; P < .00001), indicating considerable variability among the included studies. Excluding the outlier study 43 resulted in a marginal change in SMD to −0.22 (95% CI: −0.71 to 0.27; I2 = 83%), without substantially altering its interpretability. In both scenarios, the degree of dispersion suggests differences in clinical characteristics, intervention parameters, or measurement scales used, limiting the robustness of the estimated effect (Figure 4).
rESWT Versus all Lasers
Figure 4 also presents the forest plot associated with the subgroup analysis of rESWT versus all laser modalities for pain reduction, which included 6 studies.37,44-48 A small but statistically significant effect was observed in favor of laser therapy (SMD = 0.27; 95% CI: 0.01-0.53; P = .045), suggesting that, in this set of studies, laser could provide a modest advantage over rESWT in terms of pain relief. Heterogeneity was moderate (I2 = 49%; P = .03), indicating intermediate variability among studies, possibly attributable to differences in application parameters, participant characteristics, and measurement scales used.
rESWT Versus LLLT
In the subgroup comparing rESWT with LLLT for pain treatment, 4 studies were included (Figure 5). The effect size was small and not significant (SMD = 0.32; 95% CI: −0.10 to 0.73; P = .13), with a direction favoring LLLT. Although the trend suggests a possible superiority of LLLT, the width of the confidence interval and the lack of statistical significance limit the certainty of this finding. Heterogeneity was moderate-to-high (I2 = 67%; P = .005), indicating substantial variability among the included studies. This inconsistency could be due to differences in dosage parameters, population characteristics, or measurement scales used.
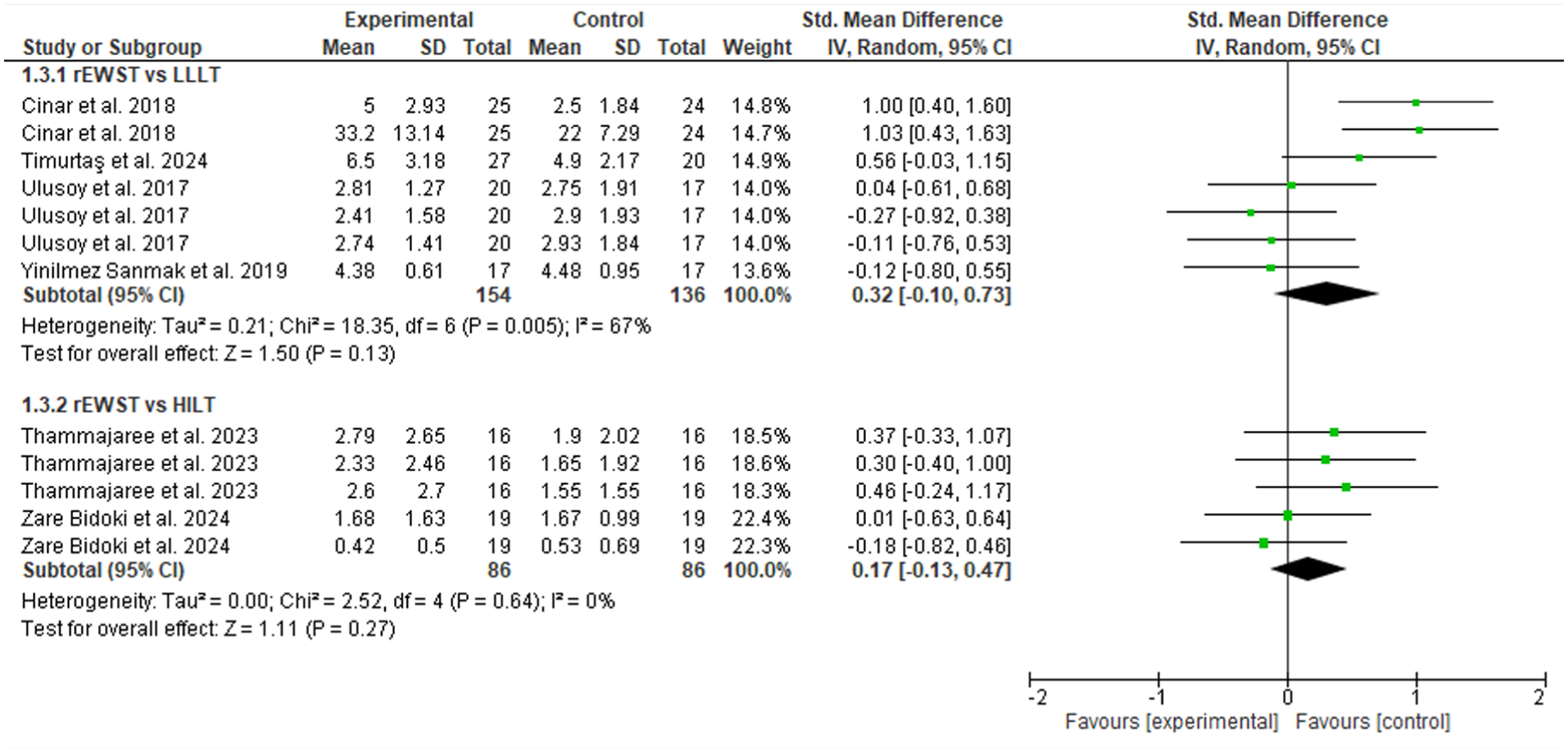
Forest plot of rESWT versus laser types: LLLT and HILT on pain. The comparison of rESWT versus HILT corresponded to an analysis using a fixed-effects model.
rESWT Versus HILT
Figure 5 also shows the comparison between rESWT and HILT, which included 2 studies. The effect size was small and not significant (SMD = 0.17; 95% CI: −0.13 to 0.47; P = .27), with a direction favoring HILT. Heterogeneity was null (I2 = 0%; chi2 P = .64, fixed-effects model), suggesting high consistency between the included studies. However, the small number of studies limits the statistical power and the generalizability of the findings.
Meta-Analysis of Function Outcome
rESWT Versus All EPMs
The meta-analysis evaluating the effect of rESWT versus various EPM on functionality included 10 studies35,36,38,39,42-47 and is presented in the forest plot in Figure 6. The effect size was very small and not significant (SMD = −0.11; 95% CI: −0.47 to 0.25; P = .55), with a direction slightly favoring rESWT. However, the width of the confidence interval and the lack of statistical significance preclude establishing a conclusive advantage. Heterogeneity was considerable (I2 = 85%; P < .0001), suggesting high variability among the included studies. This dispersion could reflect differences in intervention protocols, clinical characteristics of participants, or functional assessment scales used. Overall, the results do not support a clear superiority of rESWT over other EPMs in improving functionality.
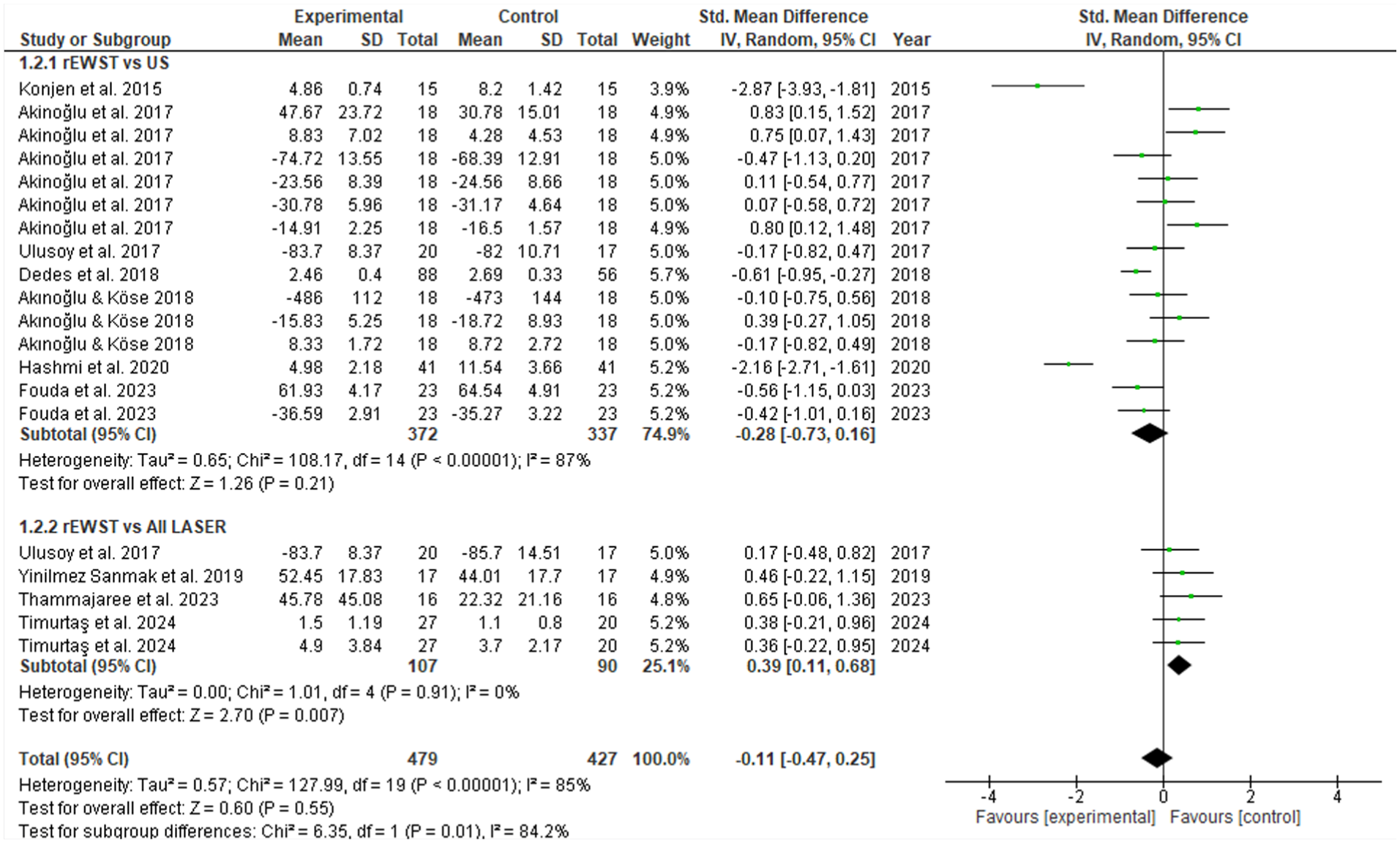
Forest plot of rESWT versus all EPM and subgroups (US and all laser) for function.
rESWT Versus US
The subgroup comparing rESWT with US for functional improvement included 7 studies35,36,38,39,42,43,46 (Figure 6). The effect size was small and not significant (SMD = −0.28; 95% CI: −0.73 to 0.16; P = .21), with a direction slightly favoring rESWT. However, the width of the confidence interval and the lack of statistical significance preclude establishing a conclusive advantage. Heterogeneity was high (I2 = 87%; P < .0001), indicating considerable variability among the included studies, which may reflect the differences observed in the overall meta-analyses.
rESWT Versus All Lasers
The subgroup comparing rESWT with different laser modalities (LLLT and HILT) for functional improvement included 4 studies.44-47 The effect size was small but statistically significant (SMD = 0.39; 95% CI: 0.11-0.68; P = .007), with a direction favoring the laser interventions. Heterogeneity was null (I2 = 0%; chi2 P = .91), indicating high consistency among the included studies and reinforcing the reliability of the estimated effect. These results suggest that, within this body of evidence, laser modalities may provide a significant advantage over rESWT in terms of functional improvement (Figure 6).
rESWT Versus LLLT and HILT
In the subgroup analysis of rESWT versus LLLT for functionality, 3 studies were included (Figure 7). A small but statistically significant effect favoring LLLT was observed (SMD = 0.34; 95% CI: 0.03-0.65; P = .03), suggesting that, within this body of evidence, LLLT may provide a modest advantage over rESWT in terms of functional recovery. Heterogeneity was null (I2 = 0%; P = .94, fixed-effects model), indicating high consistency among the included studies and reinforcing the reliability of the estimated effect. For HILT, only one study met the criteria for inclusion in this subgroup, 44 which showed a trend favoring laser therapy but was not statistically significant (Figure 7).
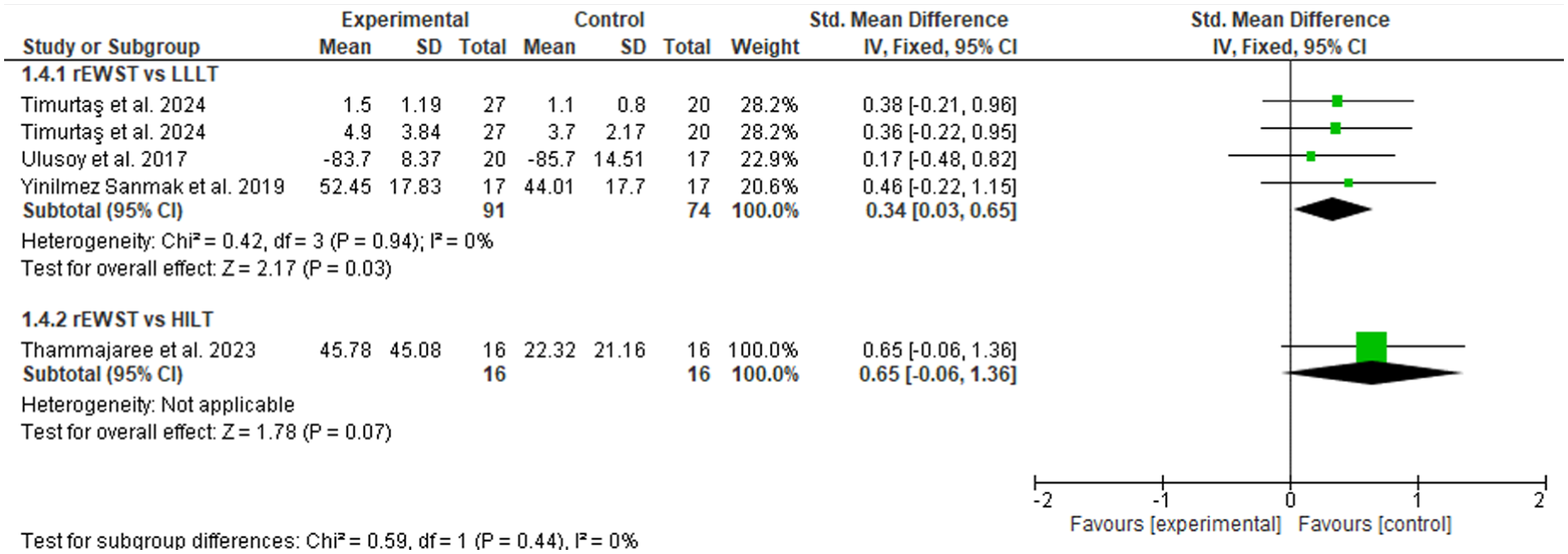
Forest plot of rESWT versus laser types (LLLT and HILT) for function.
Meta-Analysis Based on the Functional Outcome Assessment Tool
To enhance the sensitivity of the analysis, the impact of the outcome measurement tool on the estimated effect for functionality was explored. By separating the studies according to the type of instrument (self-reported questionnaires/scales versus functional tests), differences were observed in effect magnitude and direction, as well as in heterogeneity.
For functionality assessed with questionnaires or scales (9 studies), the meta-analysis showed a non-significant effect favoring rESWT (SMD = −0.23; 95% CI: −0.75 to 0.30; P = .40), with considerable heterogeneity (I2 = 89%; P < .0001), indicating high variability among studies (Figure 8). When functionality was assessed with functional tests (3 studies), the effect was also non-significant (SMD = 0.08; 95% CI: −0.22 to 0.38; P = .60), but with low-to-moderate heterogeneity (I2 = 32%; P = .19), indicating greater methodological consistency among studies using objective performance-based measures (Figure 8).
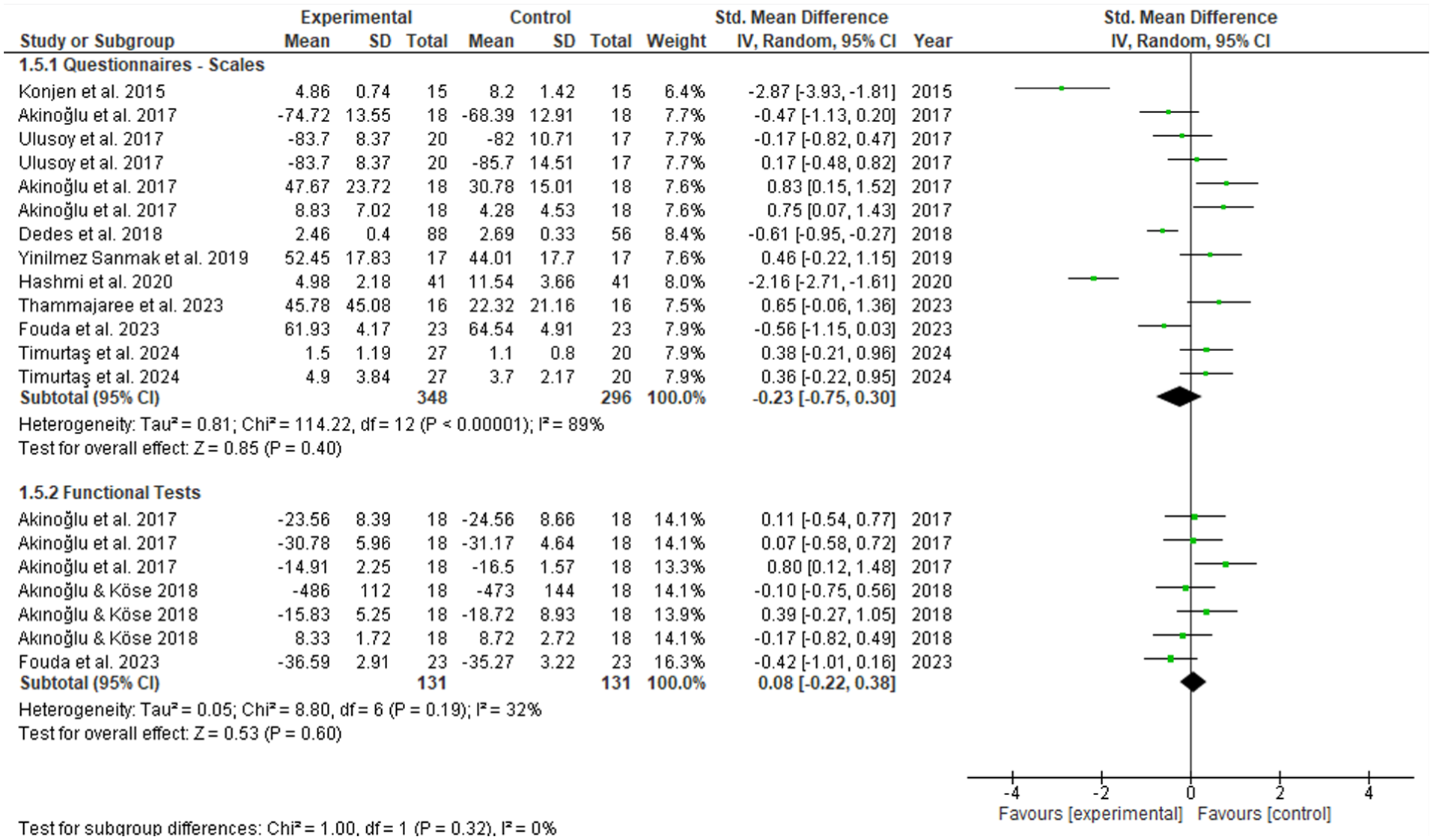
Forest plot of rESWT versus all EPM for function, grouped by type of functional assessment tool.
Most of the included studies did not report complications associated with rESWT, or failed to explicitly address adverse events. Among those that did, mild and transient effects were documented, including increased pain in 3 patients, 39 skin redness in 2 cases, 39 and 1 hematoma that led to participant exclusion. 48 These findings suggest a favorable safety profile for rESWT in the treatment of PF; however, inconsistencies in reporting limit the ability to accurately estimate the incidence of adverse events.
Certainty of evidence (GRADE)
Although no statistically significant differences were observed between rESWT and other EPMs for pain outcomes, the certainty of the evidence was rated as very low according to GRADE criteria. This rating was primarily driven by substantial inconsistency across studies, imprecision of the pooled estimates, and indirectness related to variability in intervention protocols and outcome assessment methods.
For functional outcomes, small and non-significant effects were observed across most comparisons. However, the overall certainty of the evidence was judged to be very low due to methodological heterogeneity, limited number of studies per comparison, and variability in the tools used to assess function (see Supplemental Material 2).
Discussion
This systematic review and meta-analysis aimed to evaluate the immediate efficacy of rESWT, applied either as a stand-alone intervention or combined with conventional physiotherapy, compared with other EPMs for the treatment of PF, with a focus on pain reduction and functional improvement. Our findings, derived from 14 RCTs, indicate that rESWT did not demonstrate significant superiority in pain reduction or functional improvement compared with other EPMs, while laser therapies may offer a modest advantage in certain functional and pain-related outcomes. The exclusion of the trial with atypical variance for pain intensity 43 marginally reduced both the observed effect size (particularly in the comparison with US) and heterogeneity, without altering the overall analytical interpretation.
Overall, a significant effect of time was identified for pain and function improvement, but no significant time-by-group interaction was observed. This indicates that, over time, there was a significant change in the dependent variable for participants in general, but this change was not differential between the rESWT and other EPM groups. However, it cannot be determined whether the observed effect was also influenced by contextual or placebo effects associated with the applied techniques.
Regarding pain, our findings contrast with previous meta-analyses that, when compared with placebo, reported a significant short-term 49 and long-term 20 reduction in PF-related pain following rESWT. In addition, the results differ from those reported by Guimarães et al, 50 who examined the efficacy of various interventions in a sample of over 15 000 patients with PF and concluded that rESWT is effective in reducing pain at medium- and long-term follow-up compared with a CG. Contrary to expectations of superiority, our results reveal a marginal and non-significant effect of rESWT versus other EPMs in pain reduction. This lack of a clear advantage persisted in specific subgroups, such as the comparison with US, where rESWT showed a direction favoring the intervention but without statistical or clinically meaningful significance.
Notably, a small but statistically significant advantage was observed for laser modalities in pain management. However, due to the limited number of trials within each subgroup, these findings must be interpreted with caution, as reduced statistical power restricts their generalizability to broader clinical settings. This trend favoring laser therapy may be partially explained by the inherent analgesic effects of laser therapy—particularly LLLT—for which short- and medium-term evidence exists. 51 Moreover, it is possible that the rESWT dosages used in the studies comparing both therapies were suboptimal for inducing a significant analgesic effect, as low-energy rESWT protocols were employed. In addition, Chow and Cheing 52 demonstrated that applying rESWT at the maximal tolerable energy density constitutes a more effective protocol than using a fixed energy density, both for pain relief and functional restoration in patients with chronic heel pain.
Regarding functionality, the overall results showed a very small and non-significant effect of rESWT compared with the totality of EPM. Similar to pain reduction, rESWT did not demonstrate a conclusive superiority over US in improving function. However, when analyzing laser modalities as a whole, a small but statistically significant effect favoring laser therapy was observed. These findings contrast with previous meta-analyses by Charles et al 20 and, more recently, Cortés-Pérez et al, 21 which reported that, in the short and long terms, ESWT is more effective than other interventions (eg, laser therapy or corticosteroid injections) in improving foot function. Notably, these studies did not differentiate between rESWT and fESWT.
These results invite a deeper reflection on the pathophysiology of PF and the mechanisms of action of these therapies. Plantar fasciitis, now redefined as a degenerative fasciopathy, requires interventions that promote tissue regeneration. Extracorporeal shockwave therapy is a widely used physical therapeutic modality in clinical practice for musculoskeletal injuries, such as fasciopathies, due to its theorized mechanism for repairing degenerated soft tissues. 19 While these mechanisms are consistent with the treatment of a degenerative fasciopathy, the absence of overall superiority in this meta-analysis suggests that other EPMs may act through similar pathways or that differences in dosage or tissue specificity were not sufficiently discriminative to demonstrate a clear advantage of rESWT. Tung et al, 25 in a very recent meta-analysis, support this hypothesis by concluding that ESWT aids in improving pain and function but does not outperform corticosteroid injections or custom orthoses, which further improve pain and function, respectively.
Proposed rESWT mechanisms include reducing pain mediators, 53 hyperstimulating nociceptors,54-57 and activating descending pain modulation, 58 reflecting a debate between analgesic and regenerative effects.59,60 However, since most trials included concurrent exercise programs 15 —a first-line treatment—it remains unclear whether observed benefits are specifically attributable to rESWT, the exercise, or their combined effect.
Finally, an important finding of this systematic review and meta-analysis is that the overall certainty of the evidence supporting the comparative effectiveness of rESWT versus other EPMs was rated as very low across all outcomes using the GRADE approach. This very low certainty reflects serious limitations related to inconsistency, indirectness, and imprecision. High levels of heterogeneity were frequently observed, likely attributable to differences in treatment dosage parameters, intervention protocols, patient characteristics, and outcome measurement instruments. In addition, many comparisons were based on a small number of studies with limited sample sizes, resulting in wide confidence intervals and reduced precision of effect estimates. Indirectness further contributed to downgrading, as functional outcomes were assessed using a heterogeneous mix of self-reported questionnaires and performance-based tests, limiting the comparability of results across studies.
Limitations
One of the main limitations related to the included studies is the high statistical heterogeneity observed in most overall comparisons for pain and functionality. This is underpinned by a marked clinical and methodological variability. First, the inconsistency in rESWT protocols (variations in pressure, frequency, and number of pulses) suggests critical fluctuations in the delivered energy flux density. Second, the disparate nature of the comparators (US, LLLT, HILT) introduces divergent mechanisms of action, complicating a unified comparison. Finally, population differences in chronicity and BMI act as confounding variables. This convergence of non-standardized protocols and diverse populations, combined with the high RoB, undermines confidence in the pooled estimates; therefore, the apparent equivalence between rESWT and other EPMs may reflect methodological noise more than a true therapeutic parity. Although a random-effects model was applied to account for this clinical and methodological variability, the high dispersion limits the robustness of the estimated effects and the generalizability of the findings.
The fact that 93% of the included studies (13 of 14) exhibit a high overall RoB compromises the internal validity of the findings. In particular, the observed deficiencies in the domains of deviations from intended interventions (D2), management of missing outcome data (D3/D4), and selective outcome reporting (D5) introduce substantial uncertainty into our pooled estimates. The presence of bias in domain 2 suggests that the implementation of rESWT and comparator modality protocols may have been altered, which potentially masks or inflates the true therapeutic effects. Similarly, the inadequate handling of missing data and the suspicion of selective reporting (D5) indicate that positive results may be overestimated due to publication or reporting bias within the individual studies. Consequently, confidence that the observed effect (or lack thereof) represents clinical reality is low. This methodological limitation is likely the primary contributing factor to the high observed heterogeneity and must be considered a critical caveat for clinicians when interpreting the apparent parity between rESWT and other EPMs.
A critical sensitivity analysis regarding functionality revealed that the type of measurement instrument influences the magnitude and direction of the effect as well as heterogeneity. Self-reported questionnaires, while valuable for capturing patients’ subjective perception, showed considerable heterogeneity and non-significance, suggesting higher subjective variability. In contrast, objective functional tests, although fewer in number, exhibited low-to-moderate heterogeneity and greater methodological consistency. While neither subgroup reached statistical significance, the contrast in effect direction and heterogeneity indicates that the choice of outcome measure may impact the estimated effect of rESWT. Questionnaires appear to capture greater subjective variability, whereas functional tests provide a more homogeneous assessment, albeit with lower sensitivity to change in this context. This methodological distinction underscores the importance of considering the type of outcome when interpreting clinical results and designing future research.
Variability in comparator interventions was also substantial, including US, LLLT, and HILT, often combined with home exercise programs or other adjunct therapies. This complexity in CGs makes identifying the specific effect of each primary EPM challenging and contributes to the observed heterogeneity. Moreover, most included studies (13 of 14) presented a high overall RoB according to the Cochrane RoB-2 tool. Specifically, domains D2 (bias due to deviations from intended interventions), D4 (bias due to missing outcome data), and D5 (bias in the selection of the reported result) showed the highest risk. This RoB, particularly in implementation and reporting, weakens confidence in the estimated effects and highlights the need for studies with more rigorous designs and better adherence to methodological standards.
Another limitation of the present review lies in its restrictive focus on short-term outcomes. This focus may lead to a potential underestimation of the actual efficacy of the interventions evaluated, whose effects may manifest or change substantially over longer follow-up periods. As the majority of the included trials focused on immediate or short-term outcomes, the long-term comparative effectiveness and durability of rESWT versus other EPMs remain uncertain. Consequently, these findings should be interpreted as a snapshot of acute response rather than sustained clinical recovery. In addition, although the search was conducted in 5 relevant databases, gray literature and studies published in languages other than English were not included, which could increase the risk of publication bias and limit the comprehensiveness of the available evidence. The high clinical and methodological heterogeneity of the trials also reduced the possibility of performing more specific subgroup analyses, for instance, based on rESWT dosage, patient characteristics, or type of comparator. Finally, in some cases, it was necessary to transform descriptive statistics (medians and interquartile ranges) into means and SDs, introducing an additional degree of uncertainty in the estimates. Collectively, these limitations and the very low certainty of the available evidence, suggest that the findings should be interpreted with caution and highlight the need for future research with more homogeneous designs, standardized protocols, and more consistent reporting.
Clinical Implications and Future Directions
Our meta-analysis indicates that rESWT is not superior to other EPMs for the management of PF. However, although statistical superiority was not established, rESWT remains a compelling clinical option due to its favorable safety profile, 61 high patient tolerance, and logistical efficiency; its ease of application and shorter treatment duration may offer practical advantages over more time-intensive EPMs in busy clinical settings.
Pain during treatment application is the most frequently reported adverse effect associated with ESWT. In this regard, Roerdink et al 61 reported that 50% of studies using high-dose ESWT and 20% of those using low-dose protocols documented this adverse effect. In the present review, only 3 studies reported minor adverse events (eg, local pain exacerbation, erythema, and hematoma). Its widespread adoption in physiotherapy practice is attributable to practical advantages, such as simpler administration, greater coverage of the treatment area, and a more favorable cost-effectiveness profile compared with fESWT. The absence of clear statistical superiority does not imply inefficacy; rather, it suggests that rESWT may achieve comparable clinical effects to other EPMs in many treatment contexts. Although laser-based interventions demonstrated statistically significant advantages over rESWT for pain and functional outcomes in certain comparisons, these findings must be interpreted with caution given the very low certainty of the available evidence. The observed trends favoring laser therapies are based on estimates with limited precision and consistency, which precludes the formulation of strong or definitive clinical recommendations. Consequently, no EPM can be considered superior based on the current body of evidence. Clinical decision-making should therefore be individualized and informed by clinician expertise, patient preferences, treatment availability, and cost considerations, rather than by small and uncertain differences in effect estimates. These findings may inform clinical decision-making based on equipment availability, therapist expertise, and patient preferences.
To advance the field, high-quality RCTs with low RoB are imperative. Specifically, studies are needed that standardize treatment protocols for rESWT and comparator modalities to reduce heterogeneity. These investigations should employ consistent and validated outcome measures, prioritizing objective functional tests for a more robust assessment of functionality. Moreover, it is crucial to explore comparisons with other modalities, particularly Transcutaneous Electrical Nerve Stimulation (TENS) and other electrotherapies, and to clearly differentiate between acute and chronic stages of plantar fasciopathy, as well as between patient subgroups that may respond differently to interventions. Increasing sample sizes in under-studied comparisons will also be necessary to enhance statistical power. To enhance the robustness and clinical significance of future evidence, trials should prioritize the integration of objective pain sensitivity or morphological assessments—such as pressure pain thresholds or ultrasonographic measurement of fascia thickness—alongside validated patient-reported outcome measures. Finally, research is required to elucidate the specific biological mechanisms through which rESWT and other EPMs influence tissue repair in the context of degenerative fasciopathy, with the ultimate goal of optimizing their clinical application.
Conclusion
Radial extracorporeal shockwave therapy, whether applied alone or in combination with conventional physiotherapy, did not demonstrate statistically significant superiority over other EPMs for reducing pain or improving functionality in individuals with plantar fasciopathy. Although laser-based therapies showed modest but statistically significant advantages in some comparisons, these differences should be interpreted cautiously. Overall, rESWT appears to provide clinical effects comparable with other EPMs. However, the certainty of the supporting evidence is very low, primarily due to substantial heterogeneity, imprecision of effect estimates, indirectness across studies, and the high RoB identified in most RCTs. These limitations restrict the strength of clinical inferences and highlight the need for well-designed, high-quality RCTs incorporating standardized intervention protocols and consistent outcome measures to generate more robust and clinically actionable evidence.
Supplemental Material
sj-pdf-1-fas-10.1177_19386400261449323 – Supplemental material for Effectiveness of Radial Extracorporeal Shockwave Therapy Versus Other Electrophysical Modalities on Pain and Functionality in Patients With Plantar Fasciitis: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-fas-10.1177_19386400261449323 for Effectiveness of Radial Extracorporeal Shockwave Therapy Versus Other Electrophysical Modalities on Pain and Functionality in Patients With Plantar Fasciitis: A Systematic Review and Meta-Analysis by Francisco Guede-Rojas, Leonardo Rodriguez-Lagos and Claudio Carvajal-Parodi in Foot & Ankle Specialist
Supplemental Material
sj-pdf-2-fas-10.1177_19386400261449323 – Supplemental material for Effectiveness of Radial Extracorporeal Shockwave Therapy Versus Other Electrophysical Modalities on Pain and Functionality in Patients With Plantar Fasciitis: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-2-fas-10.1177_19386400261449323 for Effectiveness of Radial Extracorporeal Shockwave Therapy Versus Other Electrophysical Modalities on Pain and Functionality in Patients With Plantar Fasciitis: A Systematic Review and Meta-Analysis by Francisco Guede-Rojas, Leonardo Rodriguez-Lagos and Claudio Carvajal-Parodi in Foot & Ankle Specialist
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Not required.
Consent to Participate
Not applicable.
Trial Registration
Data Availability Statement
The data supporting the findings of this study are available within the article and its supplemental materials. All data analyzed were extracted from previously published studies, which are cited in the reference list.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.