
Abstract
Background
The role of arthroscopy in the management of ankle fractures is controversial. This study aims to evaluate the prevalence of intra-articular pathologies detected during arthroscopically assisted reduction and internal fixation (ARIF) of ankle fractures, stratified by fracture classification, for indirect comparison to current literature. We also present short- to mid-term patient-reported outcomes (PROs) for a subset of the participant cohort.
Methods
We retrospectively analyzed the intra-articular findings of 134 patients who underwent ARIF of ankle fractures. A statistical analysis was performed to assess for significant differences in the proportions of affected patients across fracture types for each intra-articular pathology. PROs included Visual Analog Scale (VAS) ratings and Foot and Ankle Ability Measure scores for Activities of Daily Living (FAAM ADL).
Results
Intra-articular pathologies were noted in 92.5% of patients including sources of anterior impingement such as synovitis (52.2%), soft tissue (29.9%), and loose bodies (33.6%), as well as syndesmotic injury (47.0%), deltoid injury (26.1%), and osteochondral defects (29.1%) (Figure 1). Deltoid injury was more frequently detected in Weber C fractures than in any other fracture type. Syndesmotic injury occurred significantly more frequently in Weber C fractures than in Weber A (P < .01) and Weber B fractures (P < .001) (Table 1, Figure 2). PROs obtained for a subset of patients at the final follow-up reflected low VAS scores (mean = 1.78, n = 49) and high FAAM ADL scores (mean = 71.1, n = 14).
Conclusion
Arthroscopy during ankle fracture surgery is valuable in the detection of intra-articular pathologies that may require treatment to ensure positive patient outcomes. Furthermore, fracture type may be correlated with higher incidence of certain intra-articular pathologies. While future direct comparison is necessary between open reduction and internal fixation (ORIF) and ARIF, our study proposes that ARIF detects issues that may otherwise remain undetected during ORIF and suggests that concomitant arthroscopy is beneficial for ankle fracture fixation.
Level of Evidence:
Level IV—Case series
Keywords
“Open reduction and internal fixation (ORIF) is the standard of care for ankle fractures, but patients have been shown to suffer from residual symptoms.”
Introduction
Ankle fractures are the most common type of fracture of the lower extremities, so optimizing their management is an important goal. 1 While the popularity of arthroscopic techniques for the treatment of traumatic ankle injuries continues to rise, arthroscopy is rarely utilized in trauma cases. According to a query performed by the American Board of Orthopedic Surgery from 2010 to 2019, only 1.1% of ankle fractures treated with surgical intervention were performed with arthroscopic assistance, and 4.5% of foot and ankle fellowship-trained surgeons utilized arthroscopy for the treatment of ankle fractures. 2 Routine use of arthroscopy in evaluating and treating fractures is uncommon, likely due to the concern about added surgical complication risk and healthcare costs associated with the additional procedure.
Open reduction and internal fixation (ORIF) is the standard of care for ankle fractures, but patients have been shown to suffer from residual symptoms. Reports suggest that up to 20% of ankle fracture patients have lingering complaints following radiographically corrective ORIF. 3 In one study, substantial untreated intra-articular pathologies were observed in patients who presented with residual complaints following a traditional surgical intervention through arthroscopic evaluation performed postoperatively between 2 and 185 months. 4 Gross inspection and fluoroscopic assessment of ankle fractures may be insufficient in the detection of intra-articular pathologies, which may explain the failure of some patients to achieve good or excellent outcomes following ORIF. 5 Macera et al 6 also reported major complications such as residual pain, deep infection, malunion, and advanced post-traumatic ankle osteoarthritis in 31.5% of ORIF cases. The overall complication rate for arthroscopically assisted reduction and internal fixation (ARIF) is between 6% and 17%, with the most common complication being neurologic injury. 7 Zhang et al 8 aimed to compare the feasibility and benefits of ARIF versus ORIF for ankle fractures. Although ARIF had a longer surgery time (median = 15 minutes), lower complication rates were observed compared to ORIF (odds ratio [OR] = 0.53, P = .02). The researchers concluded that the two techniques are comparable in terms of providing pain relief and improving function. Shibuya and Jupiter, 9 however, concluded that the concurrent use of ankle arthroscopy during the surgical treatment of malleolar fractures had a statistically significant preventative effect on postoperative repeat surgery (OR = 0.13) and wound dehiscence (OR = 0.18).
Growing evidence suggests that concurrent arthroscopy has the potential to detect and treat intra-articular pathologies, and therefore may improve patient outcomes . 3 This study aims to investigate the incidence of intra-articular pathologies during ARIF of four types of ankle fractures to provide support for the use of arthroscopy. In addition, this study reports relevant patient outcomes related to pain and postoperative abilities from a subset of the total cohort.
Methods
Three centers operating under the approval of local institutional review boards prospectively compiled a database of patients who underwent foot and ankle surgery. From September 2017 to December 2023, 153 patients had acute ankle fractures that required surgical intervention as determined through x-ray visualization and, when applicable, CT and magnetic resonance imaging (MRI) scans. All surgeries were ARIF performed by fellowship-trained foot and ankle orthopedic surgeons. Intraoperative identification of osteochondral defects (OCDs), loose bodies, synovitis, and soft-tissue impingement was performed by direct arthroscopic visualization. Arthroscopic probing was used to evaluate the deltoid and the syndesmosis in every case, and upon identification of potential tears, rotational instability was inspected with stress tests to confirm arthroscopic findings. Widening of the syndesmosis was determined by fitting a size-specific 4.0 arthroscopic instrument within the syndesmosis as a sign of instability and by intraoperative radiographs.
Upon retrospective analysis, 12 cases were excluded due to work-related injuries or ongoing litigation, 2 cases were excluded due to being revision surgeries, and 5 cases were excluded due to insufficient data collection. Of the remaining 134 patients, intraoperative findings were analyzed with a breakdown of intra-articular findings in relation to the type of fracture. Fractures of the distal fibula were classified according to the Danis-Weber classification system. A statistical analysis in the form of an Omnibus-Fisher-Freeman-Halton exact test was performed to assess for significant differences in the proportions of affected patients across the four fracture types for each intra-articular pathology. In the case of statistical significance, the test was followed up by pair-wise Fisher’s exact tests to identify the specific group pairs that differed, as well as the Holm’s step-down procedure to maintain the family-wise type I error rate (α = .05).
Primary patient outcome data was requested at 1-, 2-, and 5-year postoperative intervals in the form of Visual Analog Scale (VAS) ratings and Foot and Ankle Ability Measure for Activities of Daily Living (FAAM ADL). Of the 134 patients included in the study, at least one form of patient-reported outcome (PRO) data was collected for 49 patients. Eighty-five patients were lost to follow-up despite much persistence on the part of the research team.
Results
Analysis of the intra-articular findings revealed concomitant intra-articular pathologies in 92.5% of patients. The most prevalent pathologies detected and removed were sources of anterior ankle impingement such as synovitis (52.2%), soft tissue (29.9%), and loose bodies (33.6%), which is defined as any free-floating fragment of bone or cartilage. Syndesmotic injury was identified in 47.0% of cases and required fixation in 29.1% of cases. Deltoid injury was identified in 26.1% of cases and required fixation in 12.7% of cases. Of the total, 29.1% of patients presented with OCDs, which were addressed through chondroplasty, microfracture, and/or orthobiologic in 17.2% of cases (Figure 1).
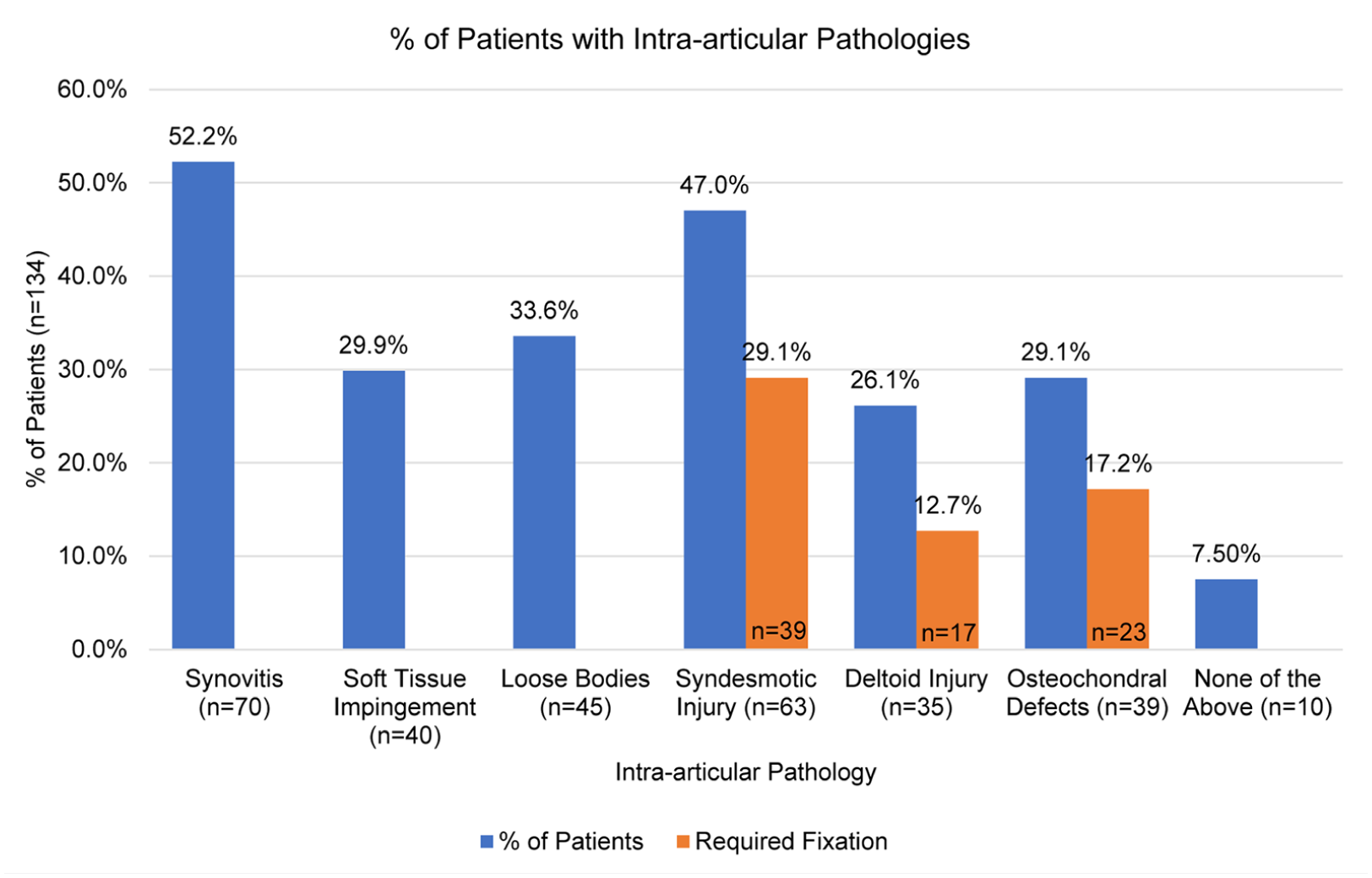
Displays of the percentage of total patients (n = 134) that presented with specific intra-articular pathologies, as well as those requiring fixation in the case of syndesmotic injury, deltoid injury, and OCDs.
Within the 129 patients who sustained distal fibula fractures, 10 were classified as Weber A, 81 as Weber B, and 38 as Weber C. The remaining 5 ankle fractures were isolated fractures of the medial malleolus. Notably, 18 Weber B patients and 10 Weber C patients had an associated medial malleolus fracture, but only 2 and 3 of these patients, respectively, also had deltoid injury. Six total patients (4 Weber B and 2 Weber C) also had an associated talus fracture (Table 1)
The Number and Percentage of Patients From Each Fracture Type That Presented With Each Intra-articular Pathology.
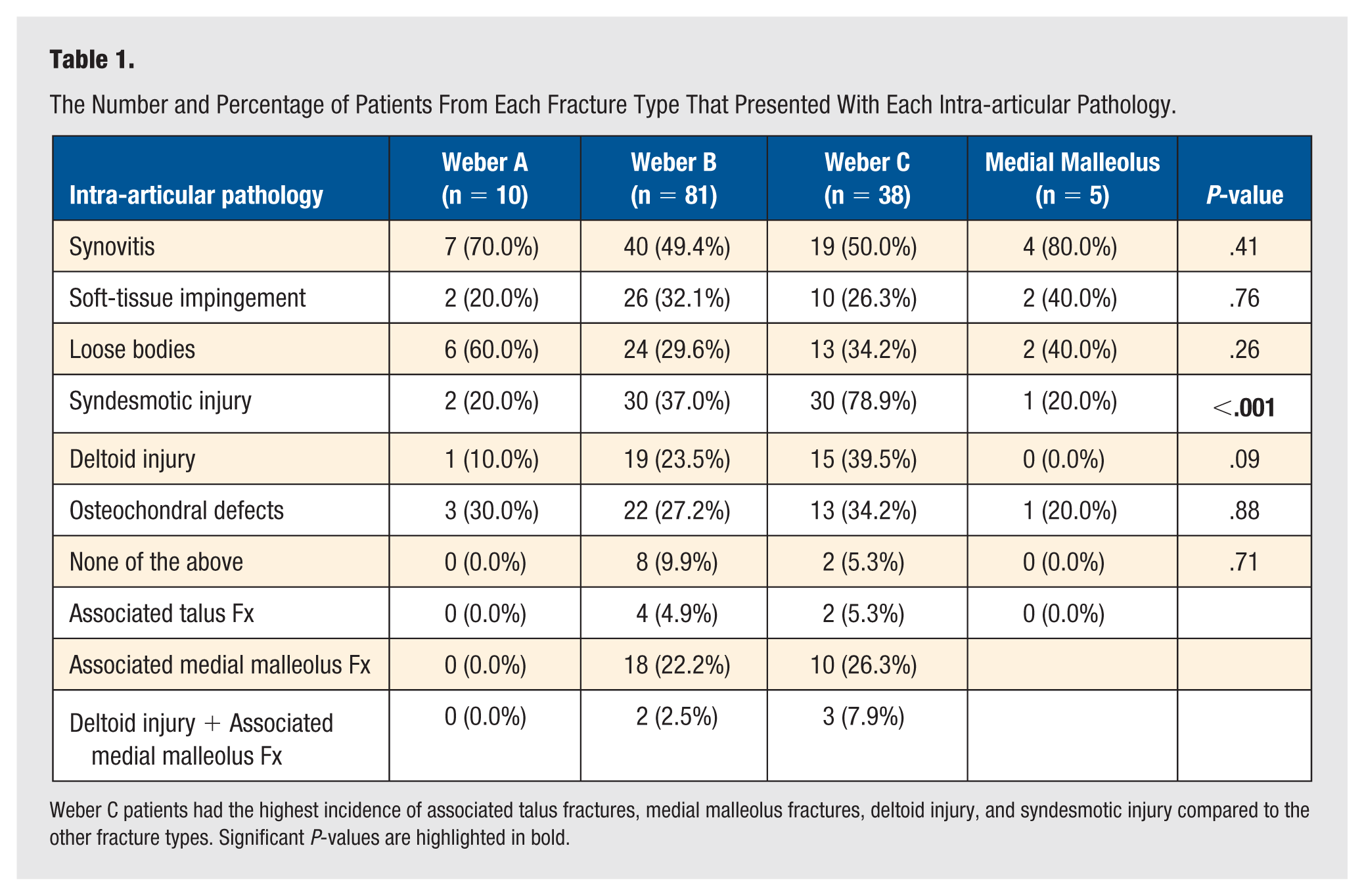
Weber C patients had the highest incidence of associated talus fractures, medial malleolus fractures, deltoid injury, and syndesmotic injury compared to the other fracture types. Significant P-values are highlighted in bold.
The intra-articular findings for each of the four fracture types were compared, with significantly higher rates of syndesmotic injury in Weber C patients than in Weber A (P < .01) and Weber B patients (P < .001) (Table 2, Figure 2). In addition, deltoid injury was more frequently detected in Weber C patients than in Weber A, Weber B, and medial malleolus fracture patients (Table 1, Figure 2).
The Number and Percentage of Patients From Each Fracture Type That Presented With Each Intra-articular Pathology.
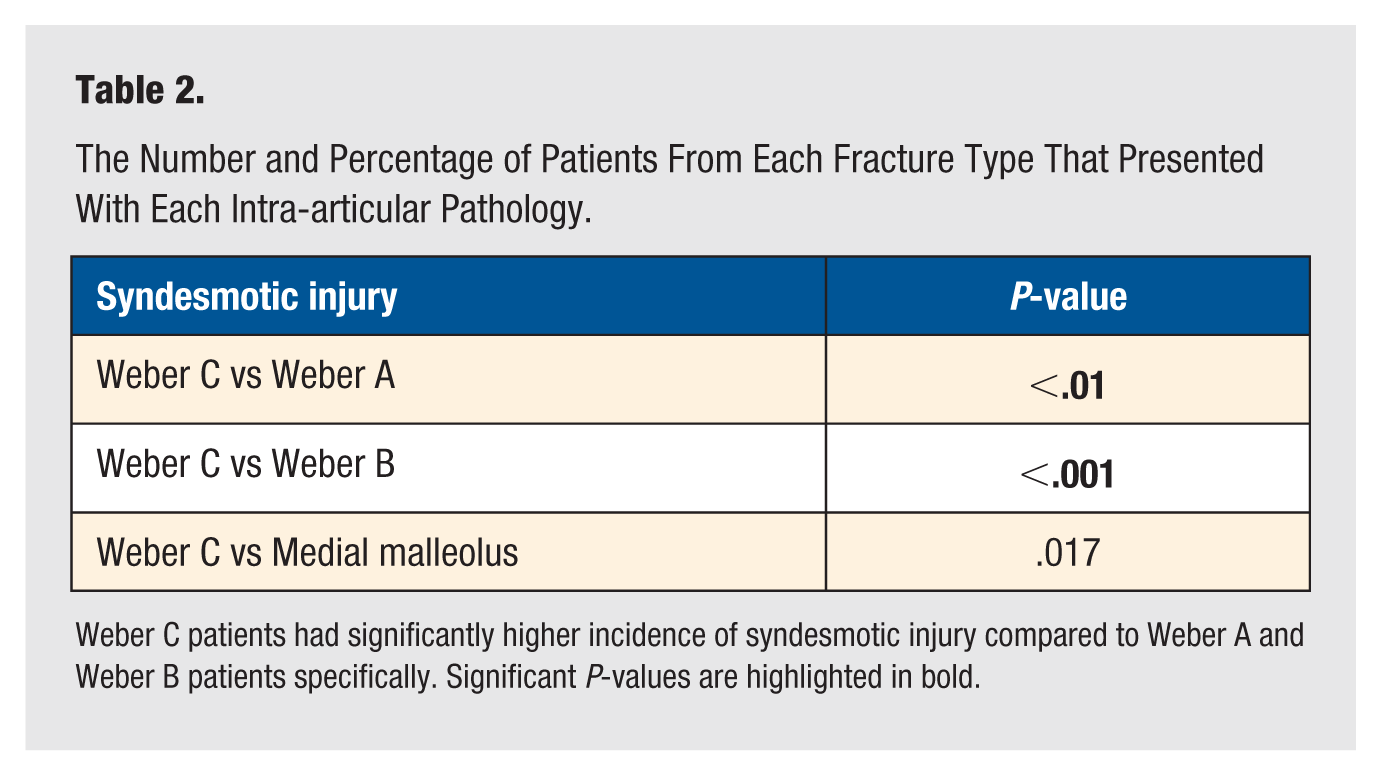
Weber C patients had significantly higher incidence of syndesmotic injury compared to Weber A and Weber B patients specifically. Significant P-values are highlighted in bold.
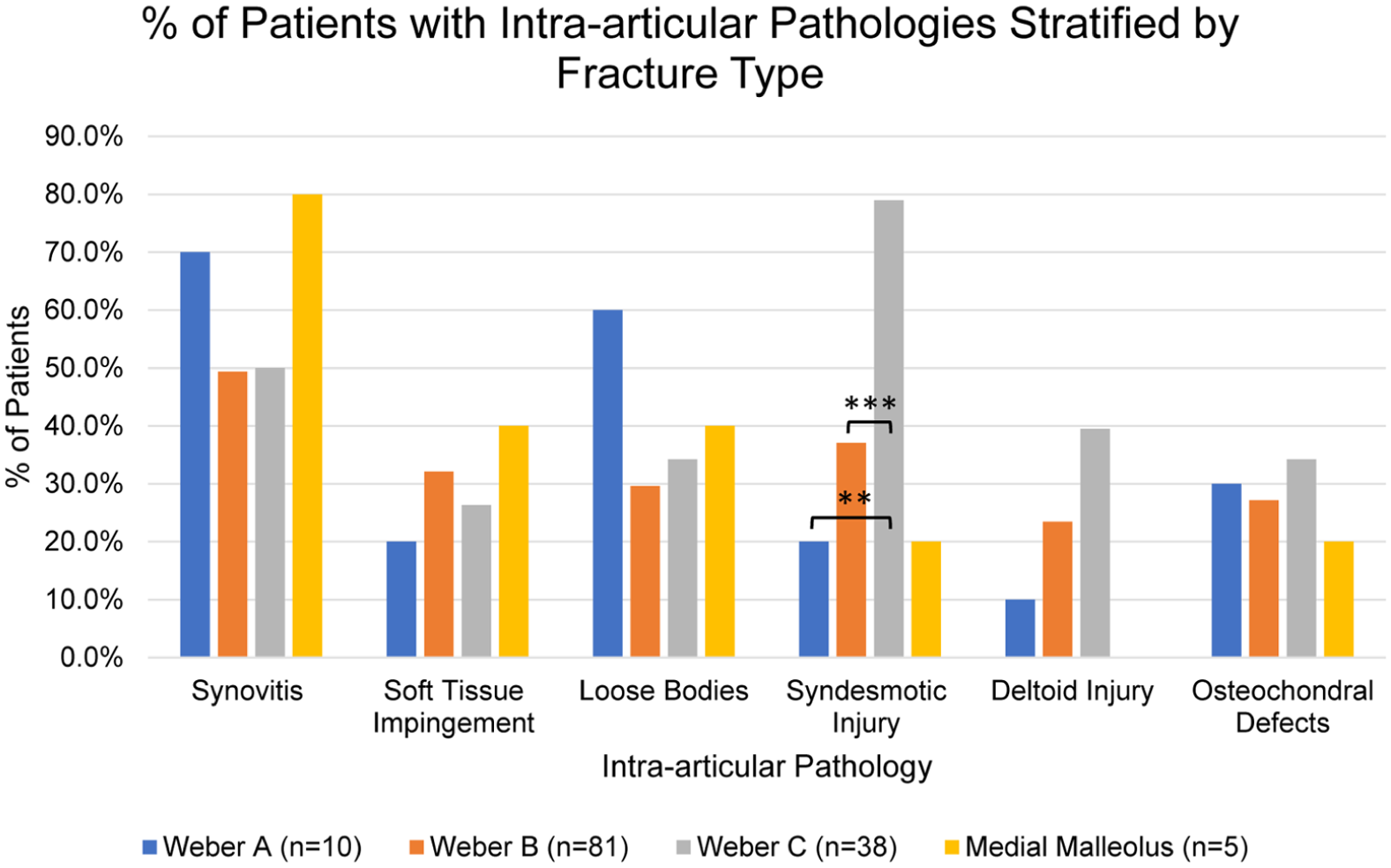
Graphical display of the percentage of patients from each fracture type that presented with each intra-articular pathology.
At follow-up, a subset of 49 patients rated their mean pain levels a 1.78 out of 10 on the VAS. A subset of 14 patients received a mean FAAM ADL score of 71.1 out of 100, indicating a generally positive postoperative foot and ankle ability during daily activity (Table 3, Figures 3 and 4). Due to the small sample size, further work is necessary to confirm these findings.
Displays Postoperative PROs for Subsets of the Participant Cohort Also Stratified by Fracture Type.
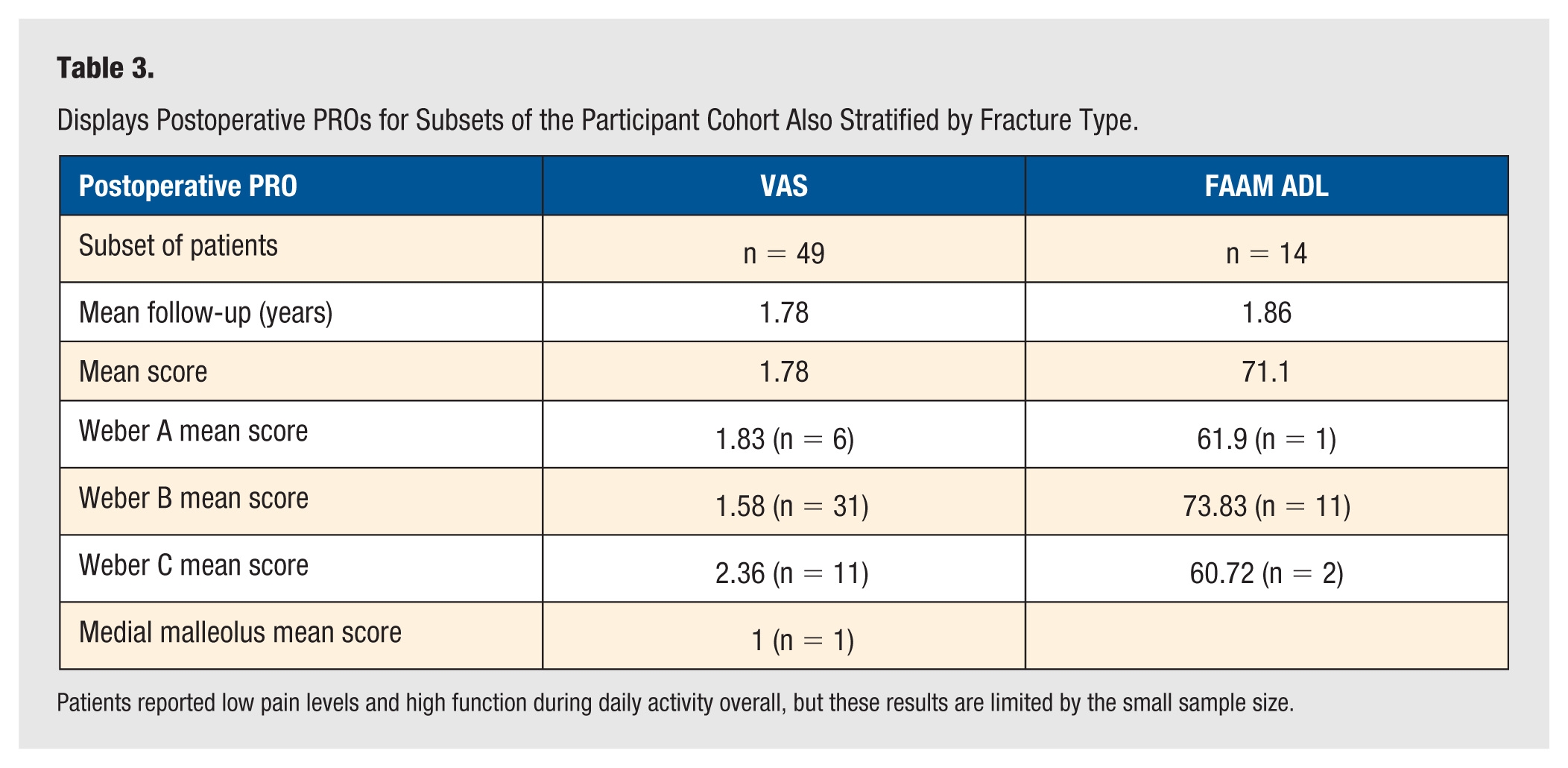
Patients reported low pain levels and high function during daily activity overall, but these results are limited by the small sample size.
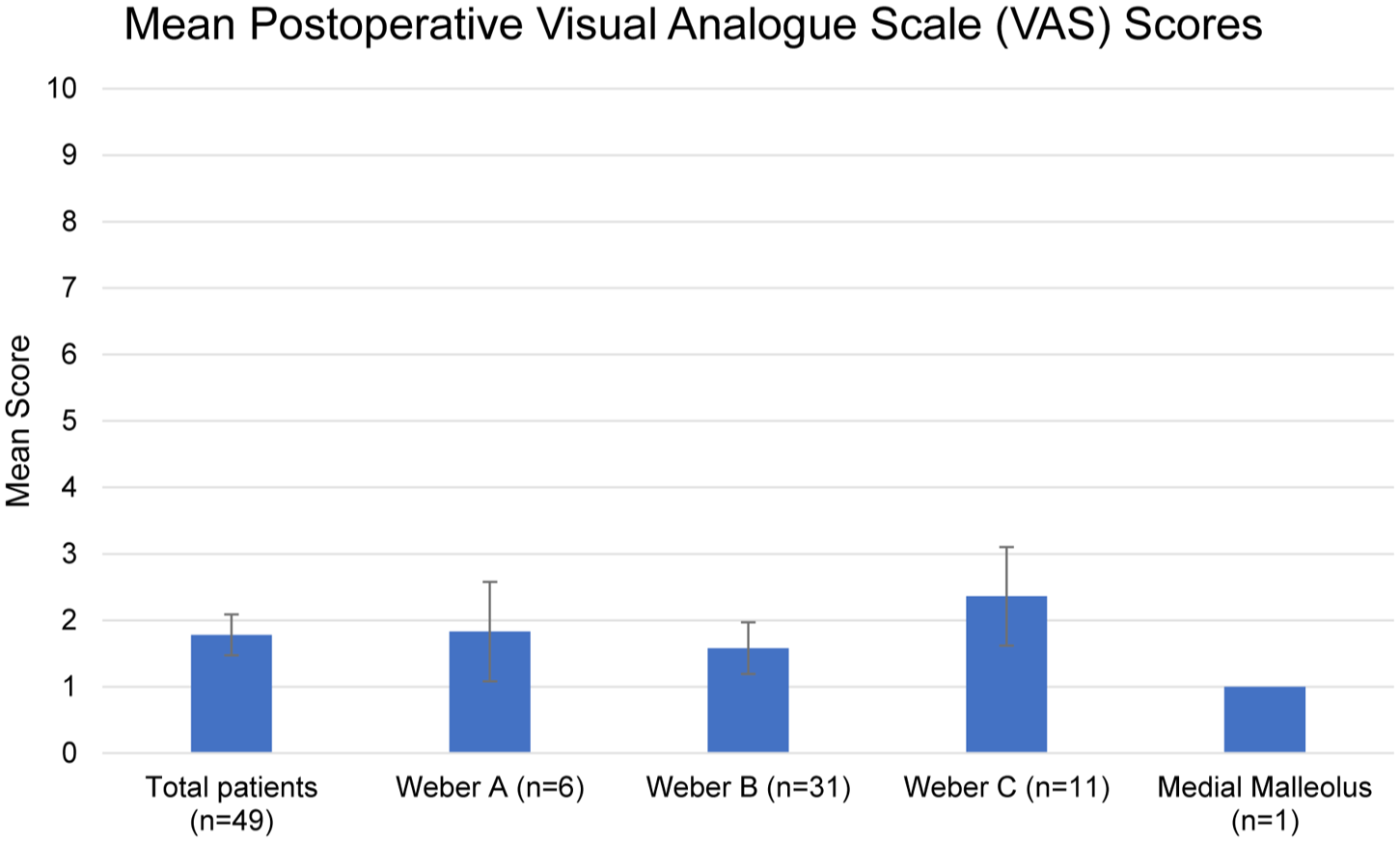
Graphical display of the mean VAS scores for a subset of 49 patients obtained at a mean of 1.78 years postoperatively and stratified by fracture type.
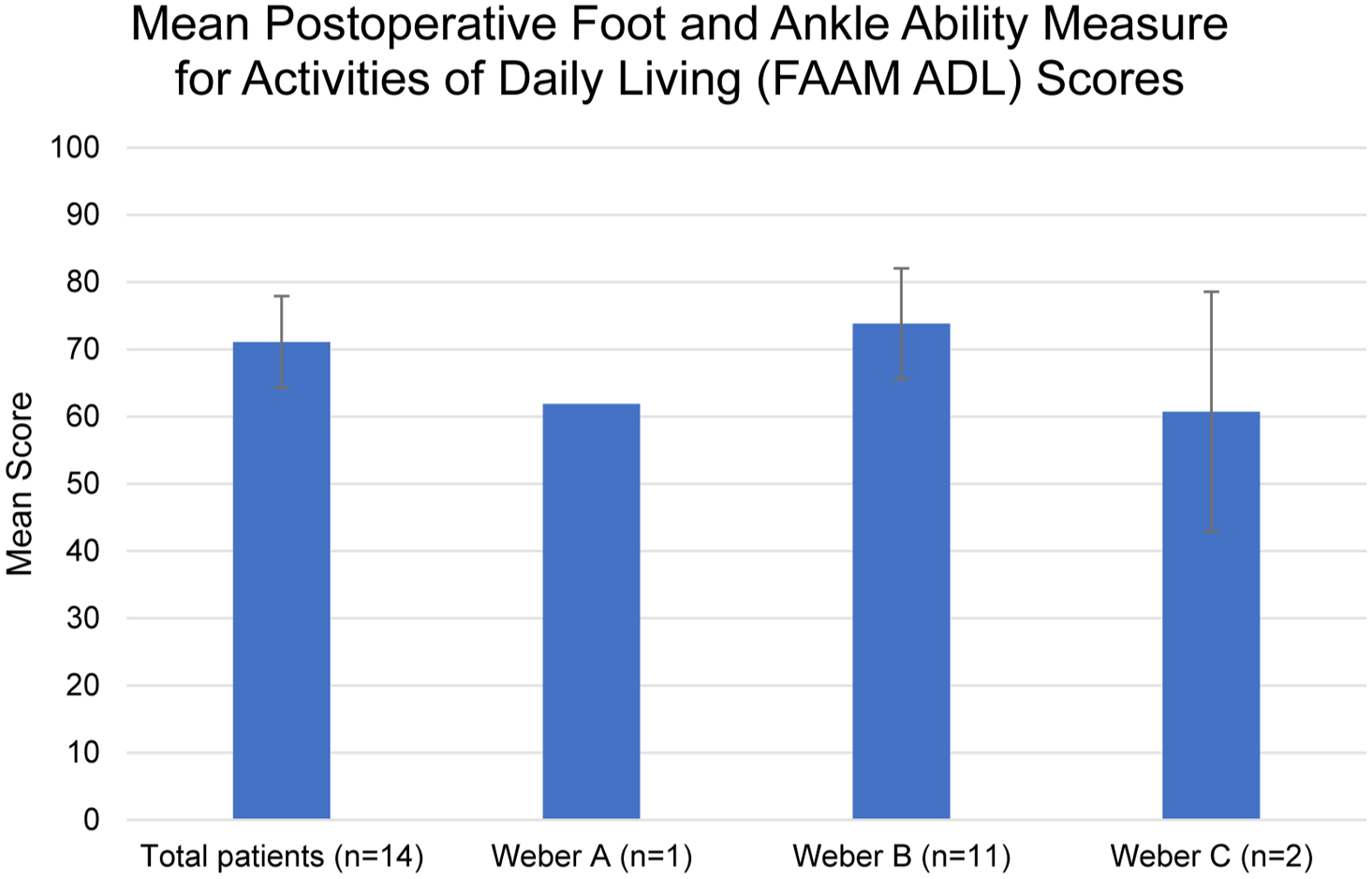
Graphical display of the mean FAAM ADL scores for a subset of 14 patients obtained at a mean of 1.86 years postoperatively and stratified by fracture type.
Discussion
Arthroscopic Detection of Intra-articular Pathologies
Previous literature has demonstrated the role of arthroscopy in the detection of intra-articular pathologies during ankle fracture surgery. Howard et al 10 showed that 84.2% of 57 total patients had intra-articular pathologies including syndesmotic injury (59.6%), loose bodies (52.6%), and OCDs (38.6%). Loren and Ferkel 11 found traumatic articular surface lesions (TASLs) and syndesmotic ligament disruption in 63% and 47.8% of 48 total cases, respectively. Braunstein et al 3 detected and treated chondral lesions in 91% of their 32 patients, and Leontaritis et al 12 reported chondral lesions in 73% of their 84 cases. Our study detected intra-articular pathology in the form of anterior ankle impingement (loose bodies, synovitis, or soft tissue), syndesmotic injury, deltoid injury, or OCDs in 92.5% of our 134 cases. The present study reinforces and builds on the current literature not only by analyzing a larger sample size of patients undergoing ARIF but also by stratifying patients based on fracture type for comparison of intra-articular pathology incidence. The following sections dive deeper into our findings for each intra-articular pathology and their relevance to clinical practice.
Anterior Ankle Impingement
Our study reported anterior ankle impingement in the form of synovitis, soft tissue, and loose bodies, which was detected in 52.2%, 29.9%, and 33.6% of cases, respectively. The incidence of anterior impingement was comparable between the fracture types.
Anterior ankle impingement may cause pain and limited range of motion during dorsiflexion following surgery. 13 Loose bodies that move freely in the joint cavity can cause joint locking, hinder mobility, and pain. 14 We removed loose bodies and debrided synovitis and soft tissue in all cases where these intra-articular pathologies presented. According to previous literature, arthroscopic debridement successfully treats soft-tissue impingement in 75% to 96% of cases. 15 Due to arthroscopic visualization, we were able to treat these issues intraoperatively to decrease the chances of postoperative anterior ankle impingement symptoms.
Syndesmotic Injury
Syndesmotic injury has historically been detected in up to 80% of all Weber C fractures and up to 40% of all Weber B fractures.2,16 Egol et al 17 reported that a greater percentage of Weber C fractures required syndesmotic stabilization compared to Weber B fractures. Our results reinforce the findings of previous studies, as we both detected syndesmotic injury and required syndesmotic fixation at the highest incidence in Weber C fractures compared to the other fracture types.
The presence of syndesmotic injury following an ankle fracture is associated with more pain and poorer function 1 year after the injury. 17 Kohake et al 18 determined that syndesmotic rupture following Weber B fractures leads to a significant restriction in dorsiflexion of the ankle joint with a mean difference of 5° (15° vs 20°, P = .028). Assessing syndesmotic injury in the clinic involves tests such as the squeeze test and the crossed-leg test, which are not directive in the diagnosis since induced pain can limit its development when a fracture is present. A syndesmotic injury diagnosis should be made based on physical examination in conjunction with imaging, as well as intraoperative evaluation. 16 Several studies have demonstrated that an intraoperative assessment of syndesmotic reduction cannot be reliably achieved with two-dimensional fluoroscopy or radiographs given insufficient visualization of rotational and anteroposterior displacement. Direct visualization of the syndesmosis through arthroscopy is helpful to reduce rates of malreduction. 19 Watson et al 20 reported that ankle arthroscopy has the potential to evaluate even partial disruption of the syndesmotic ligament complex, including in the sagittal and transverse planes which traditional evaluation methods can not properly visualize. Arthroscopic evaluation during fracture fixation allowed us to detect subtle syndesmotic instability, and offer treatment when necessary, that might have been overlooked with traditional ORIF techniques.
Deltoid Injury
The deltoid ligament ruptures in 36% of Weber C fractures and 20% of Weber B fractures according to previous literature. 21 We similarly detected deltoid injury in 39.5% of Weber C patients and 23.5% of Weber B patients. Notably, our patients with deltoid injury rarely had an associated medial malleolus fracture. We also noted a higher incidence of deltoid injury in Weber C fractures than in Weber A and medial malleolus fractures. While our data did not show statistical significance, the general trend of deltoid injury incidence supports previous studies.
Failure of the deltoid ligament to heal can lead to substantial ankle instability and post-traumatic osteoarthritis. In addition, when the deltoid ligament is disrupted, there is increased opportunity for syndesmotic instability. Diagnosing deltoid injury in ankle fractures is of utmost importance. However, clinical examination is a poor indicator for deltoid ligament injury, with an accuracy rate of only 42%. 21 Knowledge of the extent of deltoid tearing, which requires further imaging or direct visualization through arthroscopy, is necessary to determine if fixation is required. Arthroscopy provided us with the ability to both detect and treat deltoid ruptures in order to prevent negative postoperative outcomes.
Osteochondral Defects
The incidence of OCDs in ankle fracture patients has been reported in other studies to be between 60% and 70%.11,22 Leontaritis et al 12 detected chondral lesions in 73% of cases and analyzed the presence of chondral lesions based on the Lauge-Hansen classification of fractures. Type IV fractures, which are sustained through the pronation external rotation mechanism of injury characteristic of Weber C fractures, 23 were associated with the highest frequency of chondral lesions. Their findings suggest that the severity of the fracture strongly correlates with the likelihood of intra-articular damage in the form of OCDs, which may lead to poorer clinical outcomes. Thomas et al 4 similarly observed a higher occurrence of tibial lesions in type C fractures.
Our study detected OCDs in only 29.1% of total patients and found comparable incidence of this intra-articular pathology across the fracture types. These findings are inconsistent with previous literature. The higher overall incidence in the prior studies may be due to the use of MRI for lesion identification, which likely detected smaller, more subtle lesions that were not visible in our study’s intra-articular assessments. In our study, OCDs were predominantly surface-level lesions identified through direct arthroscopic visualization. Overall, detection of OCDs in trauma cases is important due to the strong link that previous studies have found between OCDs and chronic ankle instability. 24
Limitations
Our study only offers indirect comparison of ARIF to ORIF literature. Direct comparison of ARIF to ORIF, which has been historically accomplished through relatively small, comparative cohorts in prospective randomized trials, remains a gap in the literature. Takao et al 22 performed either ORIF or ARIF on 72 patients with Weber B fibular fractures. Arthroscopy revealed osteochondral lesions in 73.2% of cases and syndesmotic ligament disruptions in 80.5% of cases. The ARIF group reported statistically greater American Orthopaedic Foot and Ankle Society (AOFAS) scores than the ORIF group upon follow-up, and the authors concluded that the diagnosis and treatment of intra-articular disorders through arthroscopy is essential to achieving favorable clinical outcomes. While our study does not build upon studies like these due to lacking an experimental ORIF group, we do succeed in demonstrating that arthroscopy can reliably detect intra-articular pathologies that may require debridement or fixation to ensure positive outcomes.
Furthermore, of the 134 patients included in the study, we only have at least one form of PRO follow-up data for 49 patients. The majority of our patients were lost to follow-up, making difficult any meaningful comparison between clinical intraoperative data and mid-term PROs. Another limitation of the present study stems from being a retrospective analysis, which resulted in incomplete records in the form of both demographic data and intraoperative data.
Conclusions
The present research explores the critical role of arthroscopy in the detection of intra-articular pathologies. Although additional research is necessary to directly compare ARIF to ORIF, this study builds upon the existing body of literature to substantiate the benefit of concomitant evaluation of arthroscopy in ankle fracture fixation. This is evidenced by our diagnosis and treatment of an abundance of intra-articular pathologies that are known to affect patient outcomes if not properly handled. We also began to bridge intraoperative clinical findings with PROs, but additional research is necessary. Furthermore, by placing focus on the relative rates of pathology based on fracture type, including the Weber classifications of distal fibula fractures, this research builds upon our understanding of ankle fracture prognoses.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Carreira reports relationships with Linvatec Corporation, Zimmer Biomet Holdings, Inc., and AlloSource, and Dr Acevedo reports a relationship with Arthrex Inc. which includes consulting or advisory and speaking and lecture fees. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval for this study was obtained from Piedmont IRB (1912840-4).
Consent to Participate
Written informed consent to participate was obtained from all study participants prior to their inclusion in the research.
Consent for Publication
All participants (or their legally authorized representatives) provided written informed consent for the publication of de-identified data. No personally identifiable information is included in this manuscript.