
Abstract
Background. Naviculocuneiform (NC) arthrodesis is indicated for multiple pathologies, including degenerative and traumatic arthritis, progressive collapsing foot deformity, and medial column instability. Despite its broad application, no consensus exists regarding the optimal fixation construct. Shape-memory dynamic compression staples offer potential advantages in midfoot fusion compared to static fixation. Purpose. To evaluate the feasibility of using 4-legged dynamic compression staples for NC arthrodesis and to characterize NC joint anatomy to guide implant selection and orientation. Study Design. Level IV cadaveric study. Methods. Twenty fresh-frozen cadaveric lower limbs (10 pairs) were dissected to expose the NC joint. Measurements of the medial and intermediate cuneiform and navicular facets were recorded. Four-legged staples (26 and 30 mm) were inserted, and adjacent joints were examined for proximal or distal penetrance. Statistical analysis was performed using Mann-Whitney U tests with significance set at P ≤ .05. Results. Staple fixation across the medial cuneiform-navicular articulation was safe in all 40 applications without talonavicular or tarsometatarsal breakthrough. In contrast, the intermediate segment demonstrated a significantly shorter length (35.83 ± 3.24 mm vs 46.40 ± 4.15 mm; P = .0002) and higher rates of talonavicular breakthrough at 20% for 26 mm staples and 60% for 30 mm staples. Longer intermediate segments correlated with reduced breakthrough (P = .0190). Conclusion. To our knowledge, this is the first study to quantify NC articulation lengths. Four-legged staples up to 30 mm in length were shown to be feasible for use in both dorsal-to-plantar or medial-to-lateral orientations at the medial cuneiform articulation. Due to breakthrough with the 4-legged staples, 2-legged staples (16-20 mm bridge) and staple legs ≤20 mm are advised for the intermediate segment to minimize iatrogenic injury risk.
To evaluate the feasibility of using 4-legged dynamic compression staples for NC arthrodesis and to characterize NC joint anatomy to guide implant selection and orientation.”
Introduction
The naviculocuneiform (NC) joint arthrodesis is a procedure that has been utilized in the treatment of various pathologies including degenerative and traumatic arthritis, progressive collapsing foot deformity (PCFD), medial column instability, cavovarus deformities, and Müller-Weiss disease.1-6 Despite the wide range of indications for the procedure, there remains no consensus on the optimal fixation construct. Reported variations include differing hardware orientations; combinations of plates, screws, and compressive staples; and debate over the necessity of incorporating the lateral cuneiform into the construct.7,8
In the absence of a universally accepted fixation construct, surgeon preference for shape-memory dynamic compressive staples in midfoot arthrodesis has increased. These staples are reported to offer advantages such as ease of implementation, reduced tourniquet times, shorter time to union, low-profile designs, and preservation of joint surface contact by avoiding violation of the fusion site.9-14 However, they are not without drawbacks, with staple breakage being a primary concern. Failures most often occur at the “shoulder” of the staple, where the bridge meets the leg and enters the bone, a region subjected to the highest concentration of bending and torsional stresses, ultimately leading to fatigue and failure.
To address these failures, 4-legged staples have been developed, demonstrating greater joint compression and stability, improved resistance to failure, and reduced construct motion compared to 2-legged designs.15-17 The purpose of this cadaveric study was to evaluate the feasibility of using 4-legged dynamic compressive staples in NC joint arthrodesis constructs. Secondary goals of the study included further characterizing NC joint anatomy and providing surgeons with guidance on optimal 4-legged staple orientations and lengths.
Methods
Ten cadaveric donors provided bilateral pairs, 20 total limbs, of thawed fresh-frozen cadaveric above-knee specimens, which were used at the Chicago Cadaveric Anatomic Research Symposium for this study. Approval for cadaveric use in research was obtained, and every effort was made to follow all local and international ethical guidelines and laws that pertain to the use of human cadaveric donors in anatomical research. As a cadaveric study, no Institutional Review Board (IRB) review was required. Cadaveric identification numbers were assigned, and demographic data for each limb was recorded, including sex, weight, height, and laterality.
A full-thickness incision was performed to expose the dorsal aspect of the NC joint, the talonavicular joint, and the first and second tarsometatarsal joints. The dorsal capsule and ligamentous structures were then released to allow for full access to the joint surfaces with our digital calipers, as shown in Figure 1. Using the digital calipers, multiple measurements were taken including the width (medial to lateral length) of the medial and intermediate cuneiforms, the width of the navicular at the medial and intermediate facets, the height (plantar to dorsal length) of the medial and intermediate cuneiforms, and the height of the navicular at the medial and intermediate cuneiform facets, as shown in Figure 2. A single fellowship-trained foot and ankle surgeon performed all measurements.
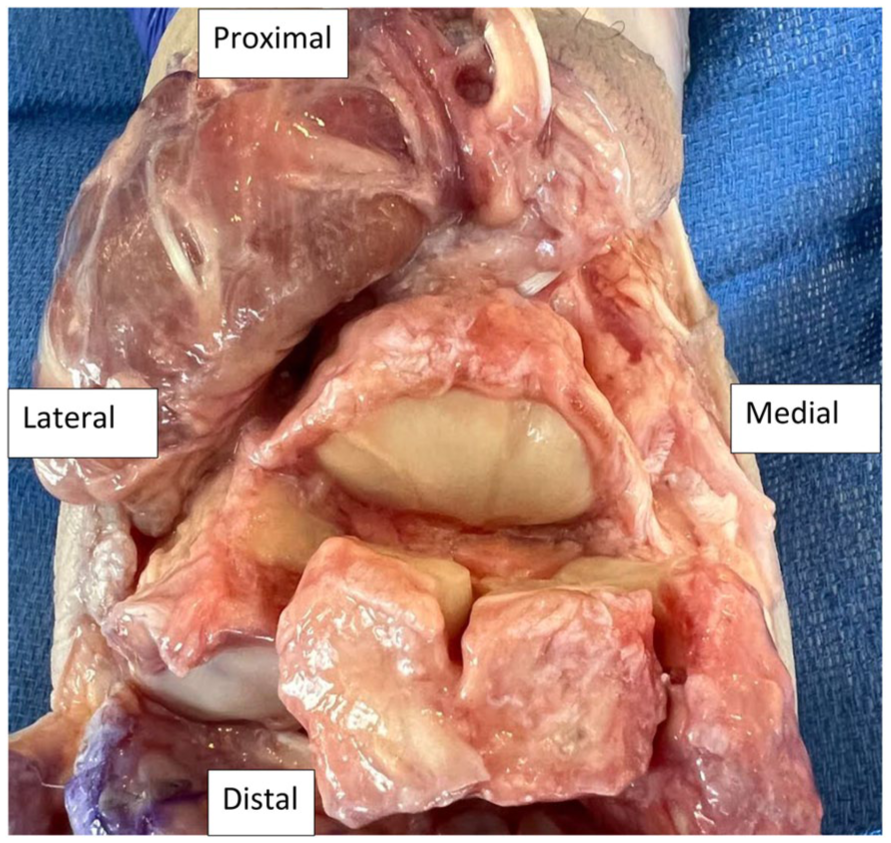
A cadaveric specimen following dissection.
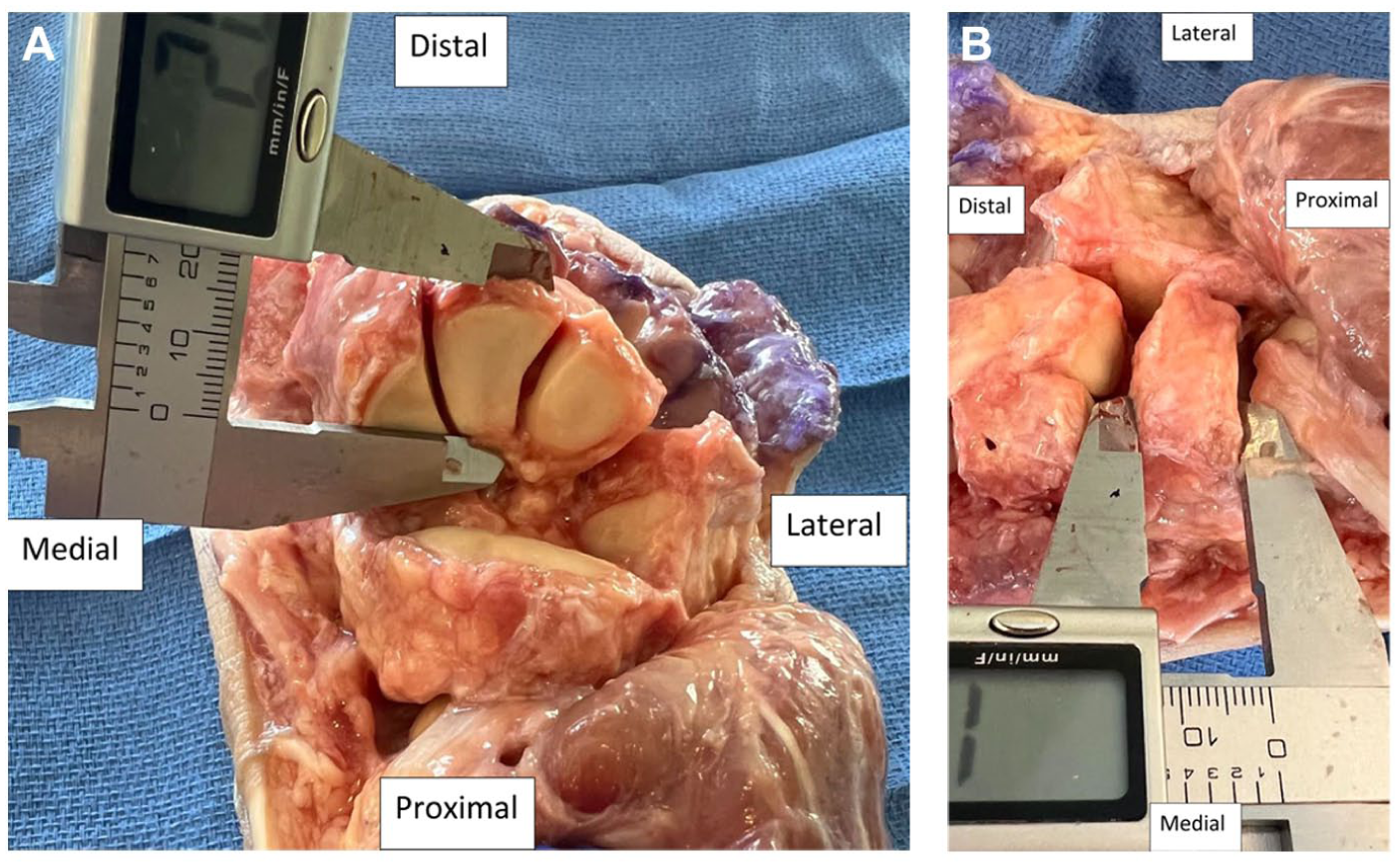
A cadaveric specimen undergoing height (A) and length (B) measurements with digital calipers.
After recording all measurements, 4-legged staples were placed in 3 different orientations. For consistency, all staples were placed by a single, separate, fellowship-trained foot and ankle surgeon per the standard technique of drilling through the staple guide, followed by tamping in of the staple. Staples were first placed in a direct medial-to-lateral orientation at the medial facet of the NC joint. Next, staples were placed in a direct dorsal-to-plantar orientation over the medial and intermediate facets of the NC joint, respectively. All right-sided specimens were tested with staples featuring a bridge length of 26 mm, while all left-sided specimens were tested with staple bridges measuring 30 mm in length. Figure 3 demonstrates a radiographic example of the staple application. After the placement of each staple, the adjacent joints were evaluated for penetrance of the staple legs into the tarsometatarsal and talonavicular joint spaces. If penetrance into an adjacent joint occurred, this was recorded as a proximal (talonavicular joint) or distal (tarsometatarsal joint) breakthrough.
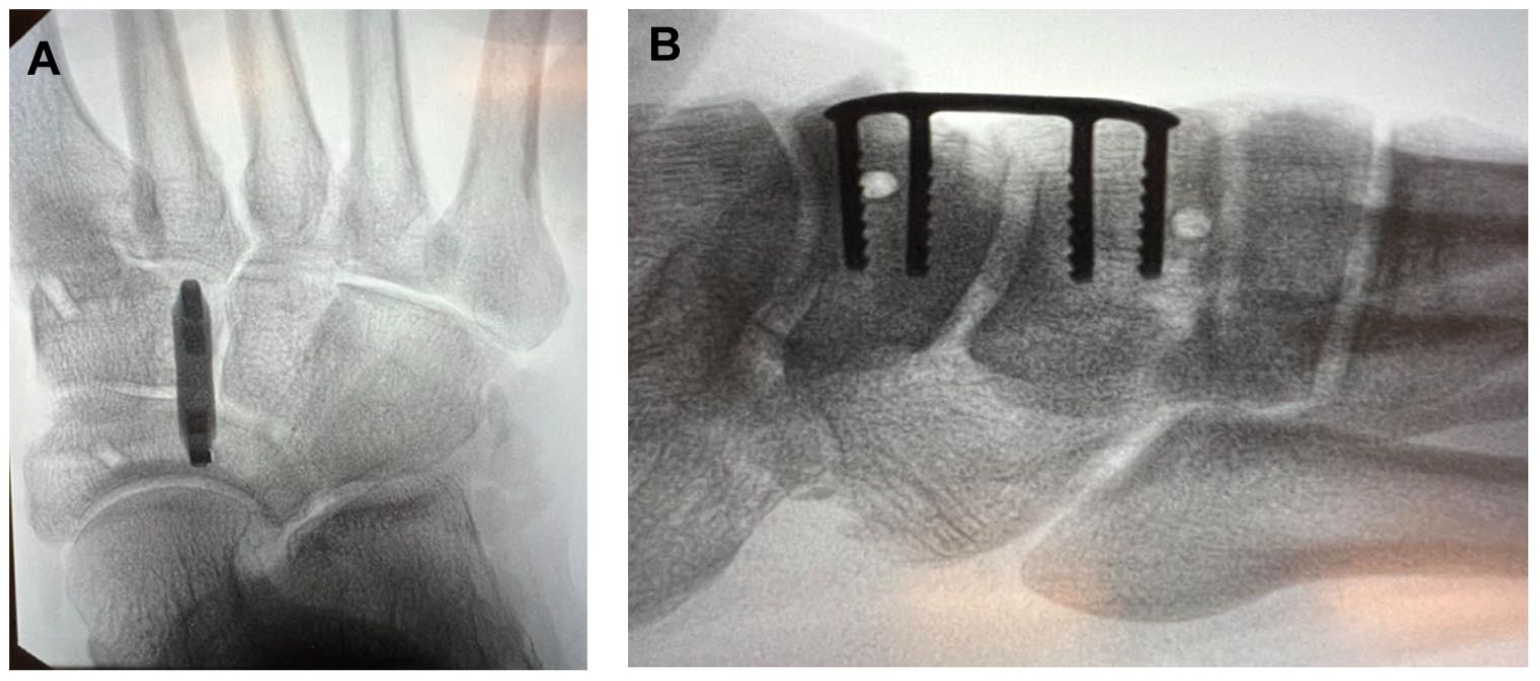
Radiographic images of the 4-legged staple following implantation into a cadaveric specimen.
To avoid investigator bias, separate and independent fellowship-trained foot and ankle surgeons individually performed each tasked portion of the study. Each was assigned an individual role of either cadaveric dissection, recording measurements, or placement of the staples.
Descriptive statistics including mean and standard deviation were used to describe cadaveric data and anatomic measurements. A Mann-Whitney U test was performed to compare the small sample size of interval variables between the length and height of the navicular cuneiform joint between the 26-mm vs the 30-mm staple group, the length and height of the medial vs intermediate cuneiform in each staple group, and the comparison of length and height of the navicular cuneiform joint when there was and was not staple breakthrough. The 95% confidence intervals were used throughout the statistical analysis. Statistical differences were significant when the P-value was less than or equal to .05. All statistical analyses were performed at Orthopedic Foot and Ankle Center by the authors of this paper; Microsoft Office Excel (Microsoft, Redmond, Washington State) was used for statistical analysis.
Results
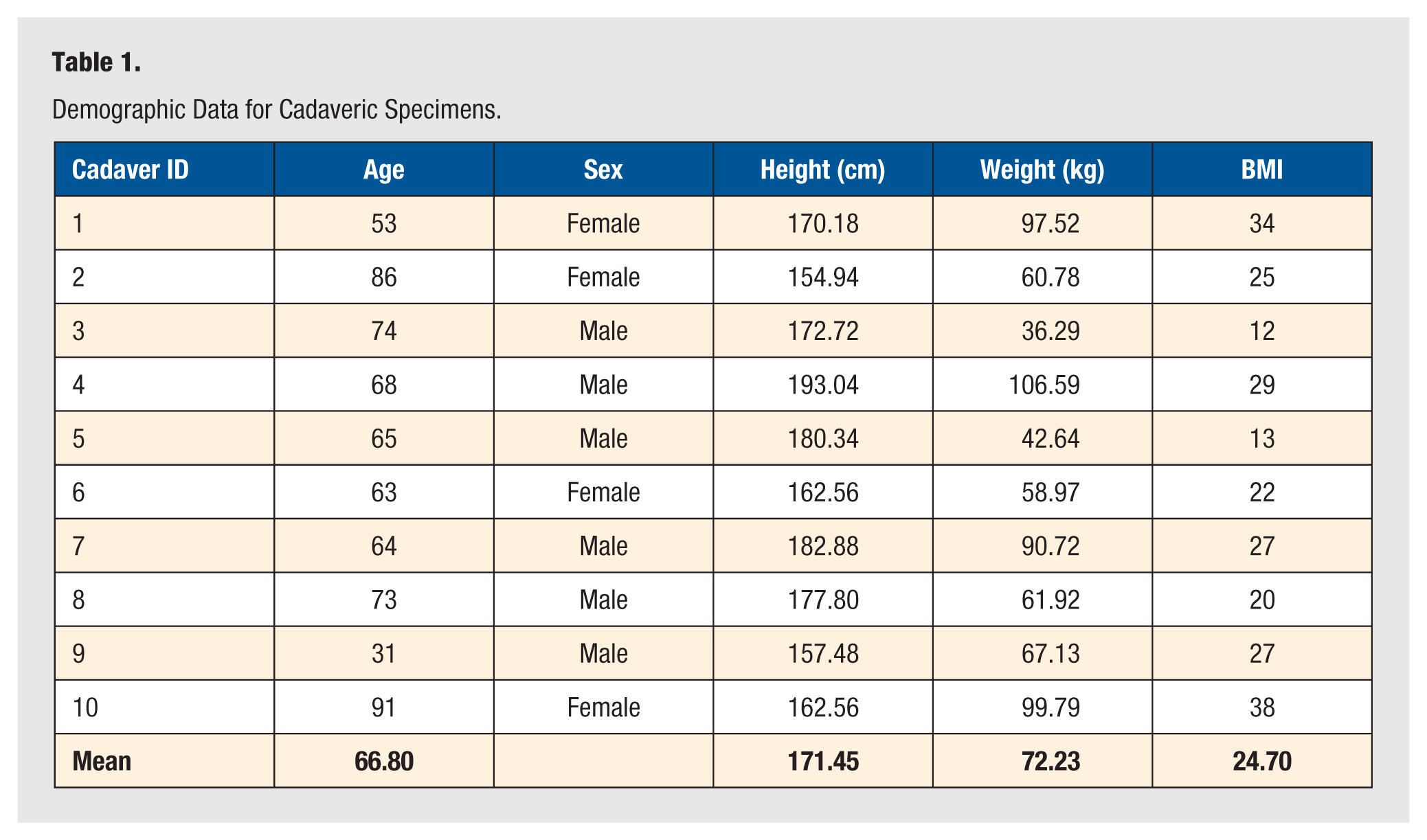
Data were obtained and recorded for all 20 specimens, including 10 pairs of matched limbs. Demographic data are shown in Table 1, with 6/10 (60%) donor pairs being male. The average (mean) age of specimens at time of expiration was 66.80 years of age, height 171.45 cm, weight 72.23 kg, and a body mass index (BMI) of 24.70 kg/m2.
Demographic Data for Cadaveric Specimens.
Measurements for the length and height of the medial cuneiform, intermediate cuneiform, and navicular are presented in Tables 2 and 3 for the 26-mm and 30-mm staple groups, respectively. There was no statistically significant difference in medial cuneiform length group (P = .0653); no statistically significant difference between the intermediate cuneiform length (P = .4965); no statistically significant difference in the navicular length at the medial cuneiform-navicular articulation (P = .2420), and no statistically significant difference between the navicular length at the intermediate cuneiform-navicular articulation (P = .9124) between the staple groups. Additionally, there was no statistically significant difference between the total length of the segment at the medial cuneiform-navicular articulation (P = .8493) and the total length segment of the intermediate cuneiform-navicular articulation (P = .5222) between the staple groups. There was also no statistically significant difference between the 26-mm staple group and 30-mm staple group in medial cuneiform height (P = .9681), intermediate cuneiform height (P = .3843), navicular height at the medial cuneiform-navicular articulation (P = .9681), and navicular height at the intermediate cuneiform-navicular articulation (P = .9681).
Measurements of the 26-mm Staple Group.
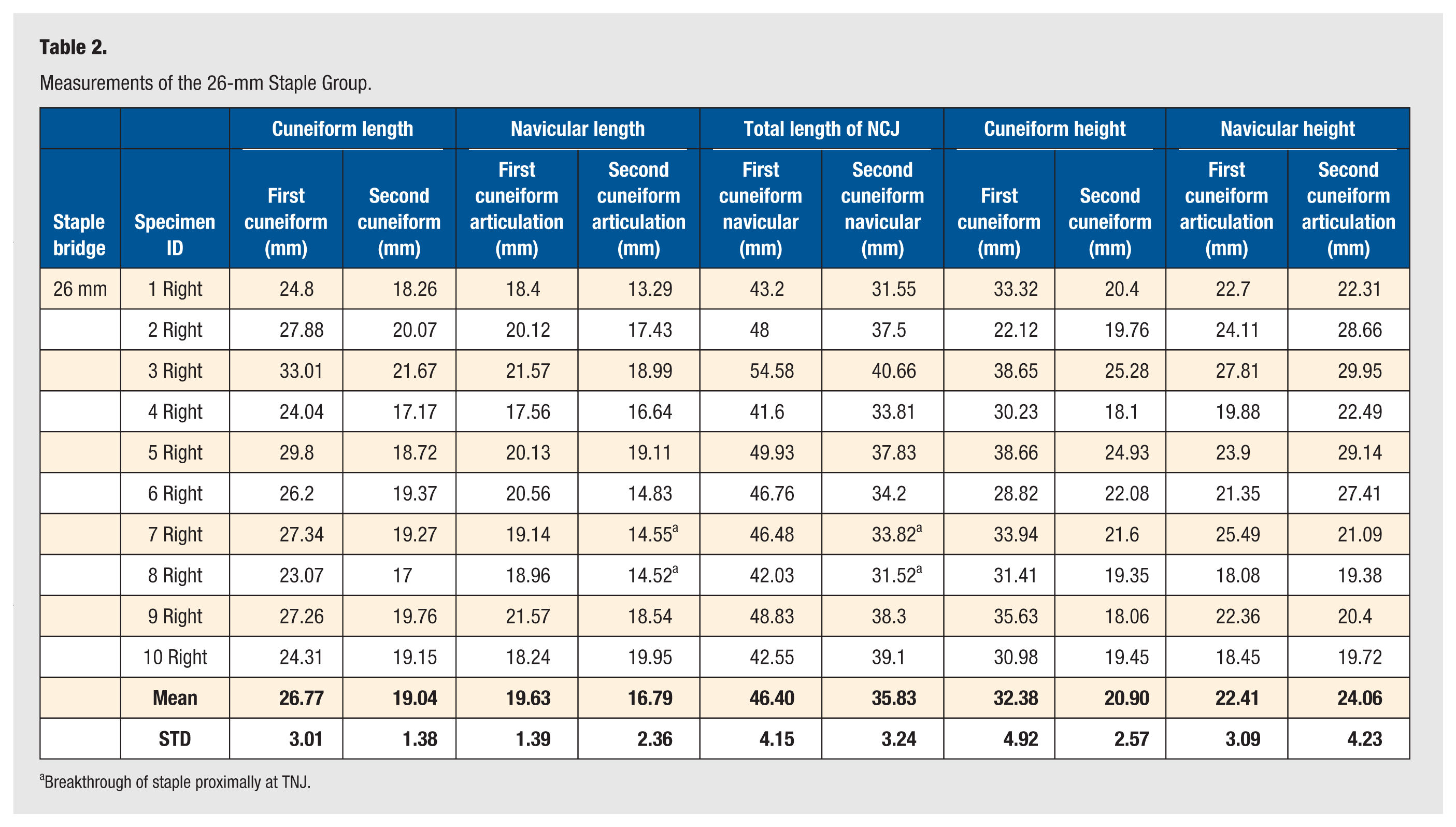
Breakthrough of staple proximally at TNJ.
The medial cuneiform length in the 26-mm staple group was significantly longer than the intermediate cuneiform group (26.77 ± 3.01 mm vs 19.04 ± 1.38 mm; P = .0002). The navicular length at the medial cuneiform articulation was statistically significantly longer than the navicular length at the intermediate cuneiform articulation (19.63 ± 1.39 mm vs 16.79 ± 2.36 mm, P = .0114). The total length of the medial cuneiform-navicular articulation was significantly longer than the total length of the intermediate cuneiform-navicular articulation (46.40 ± 4.15 mm vs 35.83 ± 3.24 mm; P = .0002). The medial cuneiform height was statistically significantly larger than the intermediate cuneiform height (32.38 ± 4.9 mm vs 20.90 ± 2.57 mm, P = .0034). There was no statistically significant difference in navicular height at the medial cuneiform-navicular articulation compared to the intermediate cuneiform-navicular articulation (22.41 ± 3.09 mm vs 24.06 ± 4.23 mm, P = .5687) (Table 2).
The medial cuneiform length in the 30-mm staple group was statistically significantly longer than in the intermediate cuneiform group (26.13 ± 3.03 mm vs 19.49 ± 11.61 mm; P = .0003). The navicular length at the medial cuneiform articulation was statistically significantly longer than the navicular length at the intermediate cuneiform articulation (20.64 ± 2.10 vs 16.92 ± 2.21 mm, P = .0022). The total length of the medial cuneiform-navicular articulation was statistically significantly longer than the total length of the intermediate cuneiform-navicular articulation (46.67 ± 36.42 mm vs 36.42 mm ± 3.55 mm; P = .0002). The medial cuneiform height was statistically significantly larger than the intermediate cuneiform height (33.37 ± 5.10 mm ± 21.80 ± 2.54 mm, P = .0002). There was no statistically significant difference in navicular height at the medial cuneiform-navicular articulation compared to the intermediate cuneiform-navicular articulation (22.65 ± 3.07 mm vs 223.22 ± 4.04 mm, P = .9681) (Table 3).
Measurements of 30-mm Staple Group.
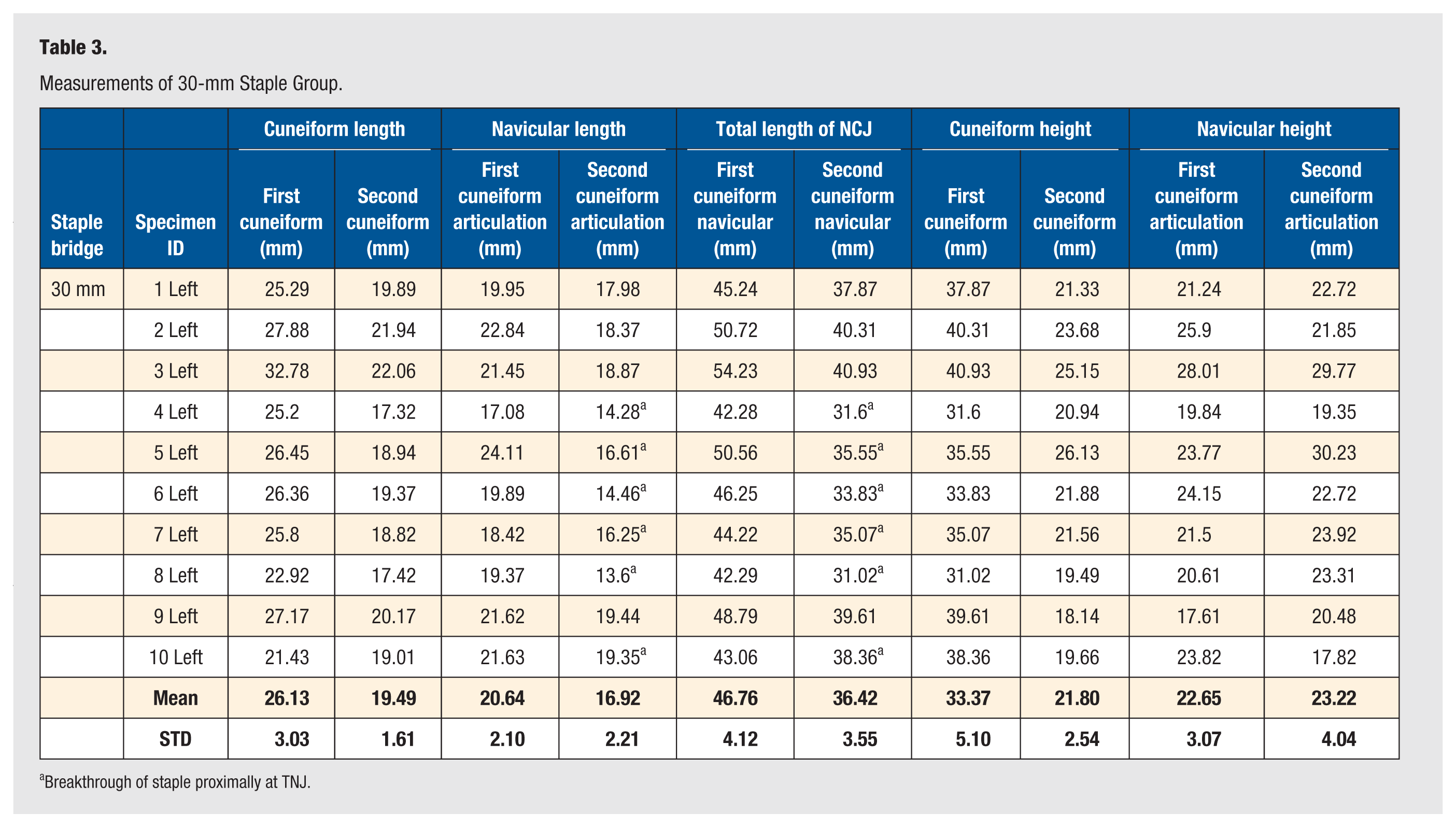
Breakthrough of staple proximally at TNJ.
There was a staple breakthrough at the talonavicular joint in 20% (2/10) of the 26-mm staples when the staple was inserted from dorsal to plantar at the second cuneiform-navicular joint. There was no statistically significant difference between the total segment length at the intermediate cuneiform-navicular articulation (36.62 ± 3.09 vs 32.67 ± 1.63 mm, P = .1778), the navicular length at the intermediate cuneiform-navicular articulation (17.35 ± 2.31 mm vs 14.54 ± 0.02 mm, P = .1778), and the inter-cuneiform length (19.27 ± 1.33 vs 19.05 ± 0.13 mm, P = .4000), respectively. There was no staple breakthrough proximally or distally when the 26-mm staple was placed from medial-to-lateral and from dorsal-to-plantar at the medial cuneiform-navicular joint articulation (Table 4).
Comparison of Measurements in the 26-mm and 30-mm Group With and Without Breakthrough at the Talonavicular Joint.
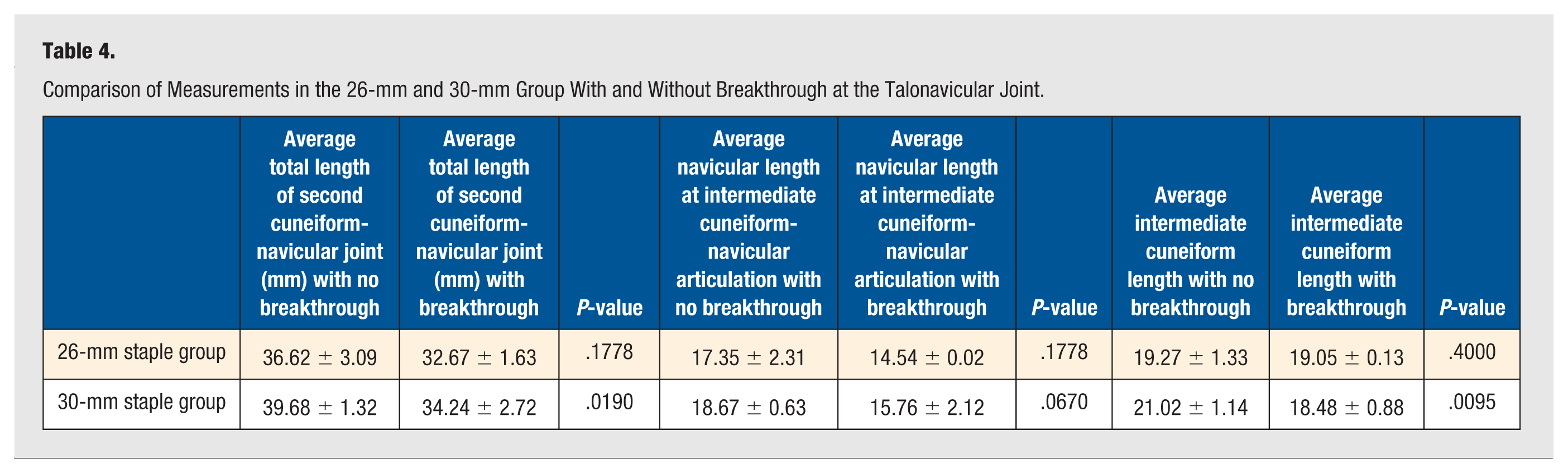
There was a staple breakthrough at the talonavicular joint in 60% (6/10) specimens when a 30-mm staple was inserted from dorsal to plantar at the intermediate cuneiform-navicular joint articulation. The total length of the intermediate cuneiform-navicular articulation was statistically significantly longer in those that did not have staple breakthrough vs those that did (39.68 ± 1.32 vs 34.24 ± 2.72 mm, P = .0190). The intermediate cuneiform length in the no breakthrough group was also significantly longer than in the breakthrough group (21.02 ± 1.14 vs 18.48 ± 0.88, P = .0095). There was no statistically significant difference in the navicular length at the intermediate cuneiform-navicular articulation (18.76 ± 0.63 mm vs 15.76 ± 2.12 mm, P = .0670). There was no staple breakthrough proximally or distally when the 30-mm staple was placed from medial-to-lateral or from dorsal-to-plantar at the medial cuneiform-navicular joint articulation (Table 4).
Discussion
The findings of this cadaveric study provide important guidance regarding the safe and effective placement of 4-legged dynamic compression staples in NC arthrodesis constructs. Our results support the safe use of 26- and 30-mm 4-legged staples for fixation of the medial cuneiform-navicular articulation in both the dorsal-to-plantar and medial-to-lateral orientations, as no instances of proximal (talonavicular) or distal (tarsometatarsal) joint breakthrough were observed in the 40 total staple applications. In contrast, the 4-legged staple construct proved ill-suited for fixation across the intermediate cuneiform-navicular articulation. The intermediate segment was significantly shorter in proximal-to-distal length compared to the medial cuneiform-navicular segment (46.40 ± 4.15 mm vs 35.83 ± 3.24 mm; P = .0002). This anatomic difference directly correlated with the high rate of proximal staple breakthrough observed, with 20% (2/10) and 60% (6/10) showing joint penetrance for the 26- and 30-mm staple groups, respectively. In the 30-mm group, specimens without breakthrough had a significantly longer total intermediate segment length in comparison to those with breakthrough (39.68 ± 1.32 vs 34.24 ± 2.72 mm, P = .0190).
The anatomic findings in this study correlate well with previous anatomic descriptions of the NC joint. In a study by Renner et al, 18 10 cadaveric specimens were measured, with the intermediate cuneiform facet exhibiting the greatest mean height (20.4 mm) compared to the medial facet (19.9 mm) and lateral facets (17.5 mm). This observation was further supported by a subsequent study reporting mean cuneiform articulation heights of 15 ± 1 mm, 17 ± 2 mm, and 15 ± 2 mm, from medial-to-lateral, respectively. 19 The present study demonstrated similar results with mean heights of 22.53 mm and 23.64 mm for the medial and intermediate navicular articulations, respectively.
The existing literature continues to expand regarding dynamic compression staples and their efficacy in arthrodesis procedures of the foot and ankle. Clinically, these devices have demonstrated promising radiographic fusion rates of 89.7% to 96.7% in foot and ankle surgery.11,12 A biomechanical study by McKnight et al 20 showed that a 2-staple construct more than doubled the effective compressive force while increasing bending strength by over 90%. In the context of our study, a biplanar 4-legged staple construct was safely achieved across the medial NC articulation using staple bridges up to 30 mm in length. This finding is particularly relevant given the complex, variable anatomy of the NC joint, where the medial and intermediate facets comprise approximately 67.2% of the total joint surface area, making these articulations critical for achieving a stable fusion. 18
Although a 4-legged staple is ill-suited for the intermediate cuneiform articulation, a 2-legged staple with a shorter bridge appears appropriate based on our results. With an average total segment length of 36.12 mm for the intermediate segment, we recommend a staple bridge of 16 to 20 mm to avoid breakthrough. Regarding implant height, McKnight et al 20 also noted that nitinol staples do not require bicortical purchase to achieve adequate compression, as the effective force extends approximately 2 mm distal to the staple tips. This suggests that the staples need only terminate within 2 mm of the far cortex to maintain compression, allowing flexibility in implant selection while minimizing iatrogenic risk. Based on these findings, we recommend dorsal-to-plantar legs of 20 mm or less when fixating the NC joint.
Limitations of this study include its cadaveric design and the number of specimens in each group. With only 10 cadaveric specimens per group, the sample size may have limited the statistical power of the findings. Additionally, the study evaluated only the medial and intermediate cuneiforms. This focus reflected the authors’ surgical preference to focus fixation to these articulations during NC arthrodesis, as they comprise more than two thirds of the total surface area. Nonetheless, inclusion of the lateral articulation would have provided additional anatomic characterization, regardless of the controversial nature of its clinical relevance. Another limitation is that all segments were measured and fixated without cartilage debridement. Although height measurements were unaffected, segment length and breakthrough rates may have been influenced by the absence of debridement, which typically removes an additional 1 to 2 mm from each articular surface. However, given the mean total segment length of the medial articulation (46.58 mm), we do not believe this would have altered the study’s overall feasibility conclusions.
This cadaveric study defines anatomic parameters and fixation guidelines for 4-legged dynamic compression staples in NC arthrodesis. Both 26- and 30-mm staples were safely applied across the medial cuneiform-navicular articulation without joint violation but proved unsuitable for the shorter intermediate segment due to adjacent joint breakthrough. To our knowledge, this is the first study to quantify the lengths of NC articulation segments, offering new anatomic insight. Based on these findings, we recommend limiting 4-legged staples to the medial articulation, using shorter 2-legged staples (16-20 mm) across the intermediate segment, and utilizing staple leg lengths of 20 mm or less to avoid iatrogenic penetration. Tailoring implant selection to NC joint anatomy may improve construct safety and reliability. Future biomechanical and clinical studies are warranted to validate these recommendations in vivo.
Footnotes
Acknowledgements
The authors recognize the support of Medline Unite Foot and Ankle for sponsoring the Chicago Anatomic Research Symposium by providing the cadaveric specimens and the lab. No financial compensation was provided to the investigators for this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics/Institutional Review Board/Consent
The authors state that every effort was made to follow all local and international ethical guidelines and laws that pertain to the use of human cadaveric donors in anatomical research. As a cadaveric study, no Institutional Review Board (IRB) review and consent were required.
Trial Registration
Not a randomized trial.