
Abstract
Introduction
Digital ulcerations and pre-ulcerative lesions are common in individuals with diabetes mellitus, peripheral neuropathy, and toe deformities. Flexor tenotomy has been recommended to assist in the healing of pre-ulcerative or ulcerative lesions with generally high rates of healing, although variable rates of complications have been reported. This study aimed to evaluate the safety, efficacy, and outcomes of flexor tenotomy for the treatment of pre-ulcerative and ulcerative digital lesions.
Methods
A retrospective chart review was performed for patients who underwent percutaneous flexor tenotomy for treatment of digital ulcerations or pre-ulcerative lesions from January 2020 to January 2023. Outcomes assessed included healing of the index lesion and complications after tenotomy. Univariate analysis was performed to assess associations between clinical factors and outcomes
Results
A total of 50 patients underwent flexor tenotomy, 25 for treatment of an ulceration and 25 for treatment of a pre-ulcerative lesion. The average length of follow-up was 786.32 days (range 36-1654 days). Healing of the index ulcer or pre-ulcerative lesion was noted in 92%. Transfer lesions were noted in 28%, of which 85.7% required a subsequent flexor tenotomy to address the secondary lesion/ulceration. No patients with prophylactic flexor tenotomy developed a transfer lesion.
Conclusion
This study suggests the flexor tenotomy is a safe procedure with reliable rates of ulcer healing; however, it highlights a high risk of transfer lesions. Surgeons should remain vigilant for transfer lesions in the post-procedure period, and patients should be advised of the risk for transfer lesions after index flexor tenotomy.
Levels of Evidence
Level 4
“This study aimed to evaluate the safety, efficacy, and outcomes of flexor tenotomy for the treatment of pre-ulcerative and ulcerative digital lesions.”
Introduction
Digital ulcerations are a common occurrence in the insensate foot due to repetitive high shear and vertical stress to the toes in the setting of associated deformity. 1 The toes are the most common location to develop a diabetic foot ulceration (DFU), comprising about 50% of all DFU.2-5 Approximately 10% of foot ulcerations are localized to the plantar aspect of the lesser toes. 5 One of the primary etiologies for ulceration at the distal aspect of the lesser toes is excessive plantarflexion pressure and shear forces. These forces result from the flexor and extensor tendons overpowering the interossei and lumbrical muscles, leading to a toe deformity in the presence of peripheral neuropathy.6-8 Additional contributors include the plantar aponeurosis and metatarsophalangeal joint capsule, as well as biomechanical abnormalities, previous toe amputations, and rheumatologic, neurologic, or neuromuscular disorders.9-14
To reduce excessive pressure to the toe, conservative offloading measures such as the use of foam, rubber, felt, or silicone crest pads, as well as debridement of any thickened apical calluses, are commonly employed.15-22 These may be coupled with other measures including custom orthotics, bracing, and/or footwear modifications.23-25 If inadequately offloaded, pre-ulcerative calluses and apical lesions are at risk of ulcerating, progressing to infection, osteomyelitis, or even amputation. Flexor tenotomy is a minimally invasive surgical technique involving the transection of the flexor digitorum longus or the flexor digitorum longus and brevis tendons and has been shown to significantly reduce plantar pressure at the distal toes, facilitating wound healing. 26 The 2023 guidelines from the International Working Group on the Diabetic Foot (IWGDF) strongly recommend flexor tenotomy for the treatment of diabetic neuropathic ulcers located at the apex or plantar aspect of flexible lesser toe deformities, citing moderate certainty of evidence. 27 Multiple systematic reviews and clinical studies have demonstrated that flexor tenotomy allows for rapid ulcer healing with low recurrence rates and a favorable safety profile.28-30 Although generally considered safe, variability in complication rates has been reported.29,31-43
Despite growing support for the performance of digital flexor tenotomy, questions remain regarding the relative risk of complications and patient selection. Nevertheless, contemporary international guidelines now recognize digital flexor tenotomy as a viable surgical option for patients with non-rigid hammertoe deformities and ulcerative or pre-ulcerative lesions, particularly in high-risk populations. 27 The objective of this study was to evaluate the safety, efficacy, and clinical outcomes of flexor tenotomy performed for the treatment of digital ulcerations and pre-ulcerative lesions. Additionally, we aimed to assess the incidence of post-operative transfer lesions (TLs) and to explore the role for prophylactic tenotomy in high-risk populations.
Methods
A retrospective chart review was conducted on patients who underwent percutaneous flexor tenotomy at our institution between January 2020 and January 2023. A query of the electronic medical record was performed by Current Procedural Terminology (CPT) codes 28010 percutaneous flexor tenotomy, single, and 28011 percutaneous flexor tenotomy, multiple. Patients were included in the study if the procedure was performed for the treatment of a toe ulcer or a pre-ulcerative digital lesion. Patients were excluded if they did not undergo a percutaneous flexor tenotomy for these indications or if procedural documentation and follow-up were incomplete. Our Institutional Review Board approved the study (Protocol #2023P002420), and the need for informed consent was waived for this retrospective study of minimal risk.
Demographic and clinical data were collected, including age, sex, race/ethnicity, and medical comorbidities such as diabetes mellitus, peripheral neuropathy, peripheral artery disease, chronic kidney disease (CKD), and tobacco use. Diabetes mellitus and CKD were determined by International Classification of Diseases, Tenth Revision (ICD-10) diagnosis within the electronic medical record. Peripheral neuropathy was determined through evidence of an ICD-10 diagnosis in the chart and/or clinical examination findings demonstrating a loss of protective sensation as tested with a 10-g Semmes-Weinstein monofilament, or loss of vibratory sensation as tested with a 128-Hz tuning fork. Peripheral artery disease was determined as per ICD-10 diagnosis or ankle-brachial index (ABI) < 0.9. Ulcer characteristics were recorded, including duration, location, and toe involved, and the presence or absence of osteomyelitis. Osteomyelitis was determined as per radiographic findings and/or documentation within the electronic medical record. Physical examination findings were also collected including the rigidity of the toe deformity (categorized as flexible, semi-reducible, or rigid) and a history of prior digital amputation.
Procedures were categorized as being performed for an ulcer or pre-ulcerative lesion, confirmed via documentation stating pre-ulcerative lesion, pre-ulcerative callus, or callus with subdermal bleeding. A procedure was determined to be prophylactic if performed to prevent the development of a TL or ulcer on an adjacent digit in the absence of a current ulcer, typically in the setting of a digital contracture or hammertoe deformity on a toe(s) adjacent to the toe undergoing flexor tenotomy without evidence of an open wound at the time of the procedure. Procedural details were collected including the location of the procedure (office vs operating room), as well as the number of toes and which toes the flexor tenotomy was performed for.
Primary outcomes included healing of the digital ulcer or pre-ulcerative lesion, defined as complete epithelialization of the ulcer or index lesion without drainage or need for additional surgical intervention, as well as complications. Post-operative infection, digital amputation, ulcer recurrence, continued digital deformity, bleeding, and the development of TLs on adjacent toes were recorded. A TL was defined as the development of a pre-ulcerative callus or open ulceration on an adjacent digit after the index flexor tenotomy was performed. The need for additional procedures was also recorded for those patients who developed a TL. Follow-up duration was collected for each patient until continued wound resolution or final documented clinic visit.
Univariate analysis was performed to assess associations between clinical variables and the development of TLs following tenotomy. Chi-squared testing was used to evaluate differences between subgroups, with statistical significance set at P < .05. All analyses were performed using Microsoft Excel and Python.
Results
A total of 50 patients met the inclusion criteria (Table 1). Thirty-five (70.0%) were male with an average age of 71.02 years. Twenty-five procedures were performed for treatment of a digital ulcer, while the remaining 25 procedures were performed for treatment of a pre-ulcerative lesion. The average duration of the ulceration prior to the performance of flexor tenotomy was 89.94 days. Six patients had a prophylactic flexor tenotomy performed. Forty-five (90%) patients in the study had peripheral neuropathy, and 16 (32%) had a documented history of peripheral artery disease. Thirty-four (68%) had a history of diabetes mellitus with an average hemoglobin A1c of 7.07 within 90 days of the procedure. Chronic kidney disease was also noted in 16 (32%).
Patient Demographics/Characteristics (n = 50).
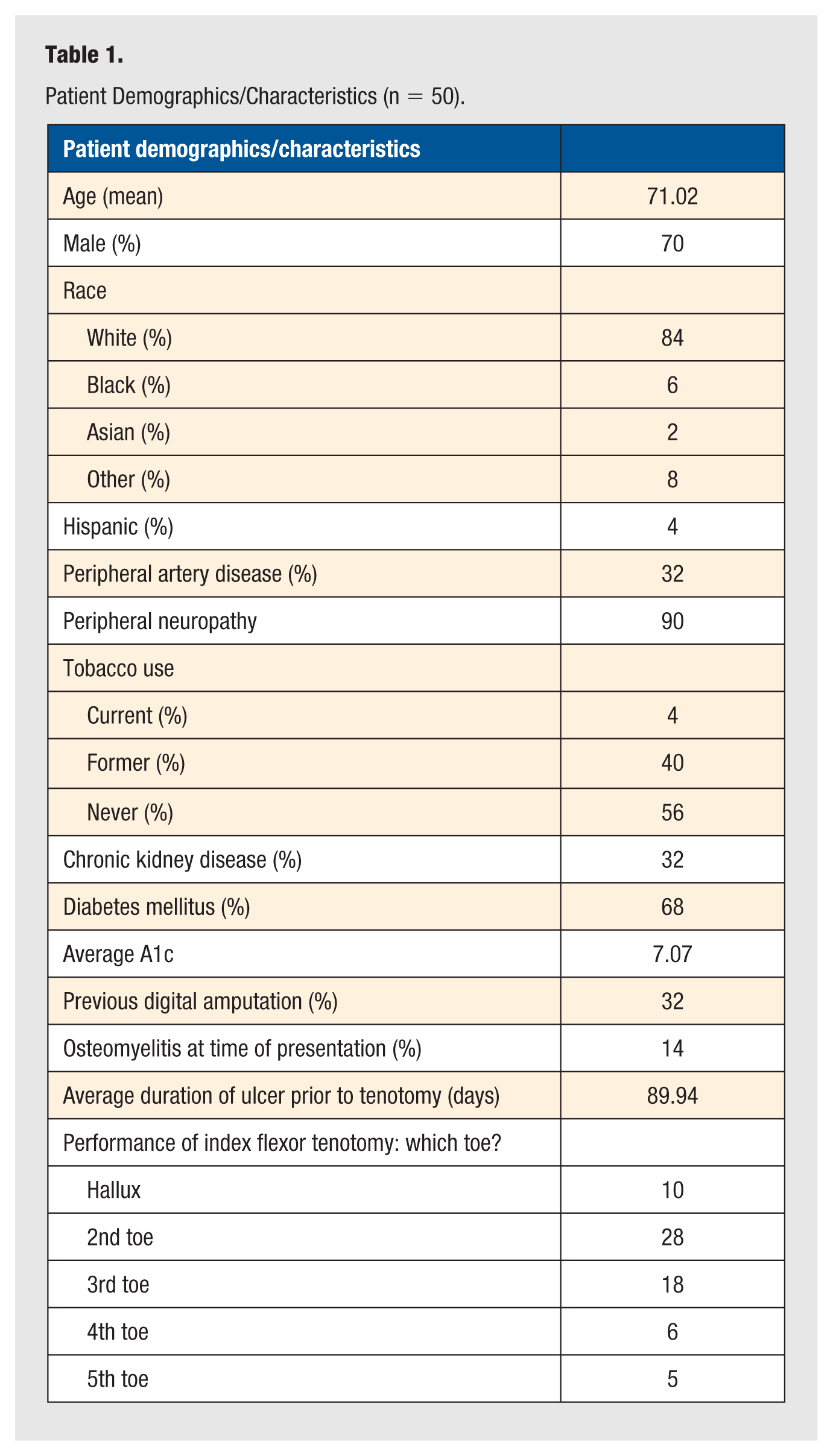
Index toe deformity was noted to be flexible in 11, semi-reducible in 23, and rigid in 2, while insufficient documentation regarding the reducibility of toe deformity was noted for 12. Forty (80%) were noted to have adjacent toe deformity, and 16 (32%) had a prior history of amputation on the ipsilateral foot (7 partial toe amputation, 7 toe amputation, 2 partial ray amputation).
Forty-seven procedures were performed in the office, while the remaining 3 procedures were performed in the operating room. Thirty-eight individual flexor tenotomies were performed, while 12 patients underwent multiple concurrent flexor tenotomies.
Twenty-four individuals (48.0%) had no complications after flexor tenotomy. Average length of follow-up time after the procedure was 786.32 days (range = 36-1654 days). Of the 25 patients with ulcers, 21 (84%) healed with an average time to healing of 47 days. Four (16%) digits with ulceration failed to heal after percutaneous flexor tenotomy and required an amputation. Of the 4 patients who required an amputation, 3 underwent amputation for a non-healing ulceration and concomitant osteomyelitis, while the remaining patient underwent amputation due to non-healing ulceration in the setting of continued toe deformity. The remaining 4/7 (57.1%) patients with osteomyelitis healed without the need for additional surgical intervention. Thirteen (26%) were noted to have ongoing digital deformity, and 5 (10%) were noted to have recurrence of their ulceration. A floating toe and bleeding were respectively noted in 1 each (2%). No post-procedure infections were noted. There was no increased risk of complications including amputation in those with peripheral artery disease (Table 2). In the analysis of those with osteomyelitis in which delayed ulcer healing was noted, there was no statistically significant difference when comparing individuals with and without peripheral artery disease (P = .3696).
Analysis of Complications in Patients With Peripheral Artery Disease (PAD) and Those Without PAD.
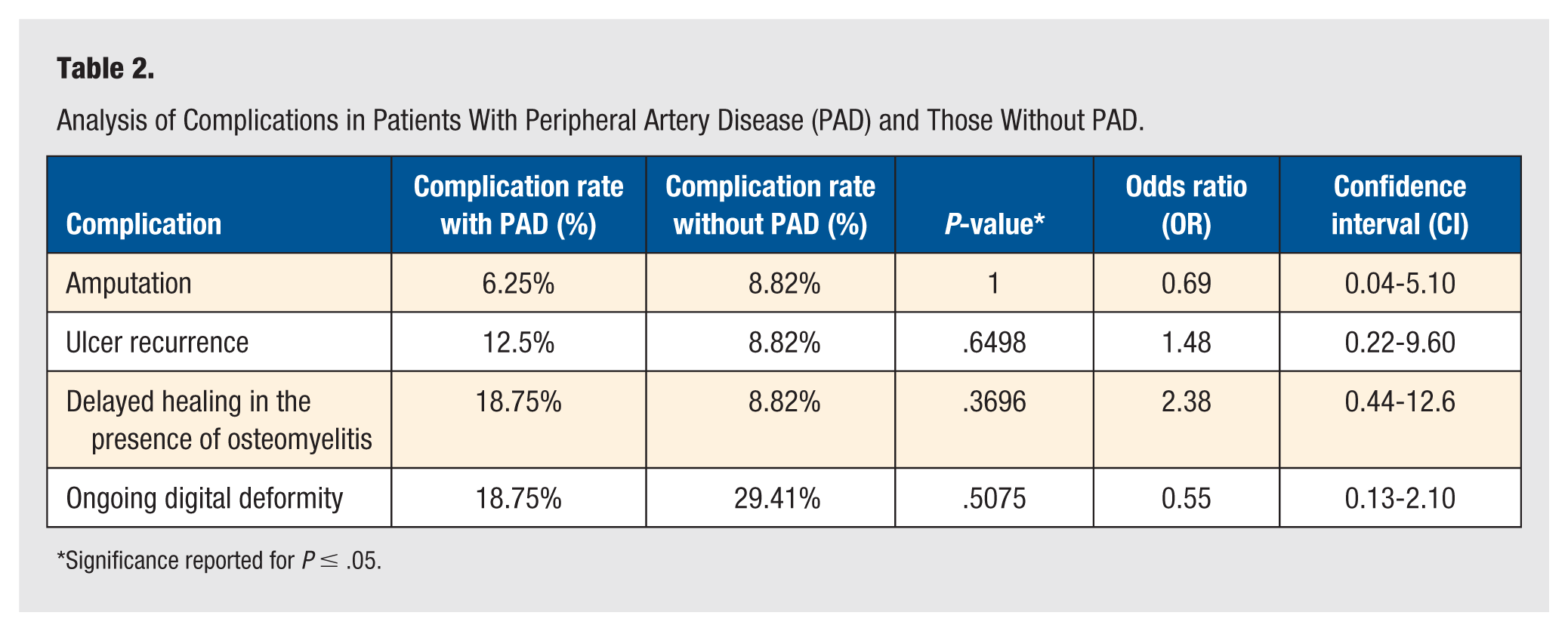
Significance reported for P ≤ .05.
Fourteen (28.0%) patients developed an ulcerative or pre-ulcerative TL after index flexor tenotomy. The average time to the development of TL was 168.68 days (range = 7-923 days). Of the 14 patients who developed a TL, 12 (85.7%) required a flexor tenotomy to address the secondary lesion. Univariate analysis determined that only CKD was protective of development of TLs. No other significant associations were noted between other patient factors and TL development (Table 3). No TLs were noted in those who had a prophylactic flexor tenotomy performed. In patients identified as undergoing a single flexor tenotomy, 26.3% (10/38) were noted to develop a TL as compared to 66.7% (4/6) of patients undergoing multiple flexor tenotomy without concomitant performance of a prophylactic flexor tenotomy. Additionally, 4 (8%) were noted to develop callusing without a pre-ulcerative lesion or ulceration on an adjacent digit after flexor tenotomy was performed.
Analysis of Transfer Lesion Development (TLD) and Subgroup Demographics.
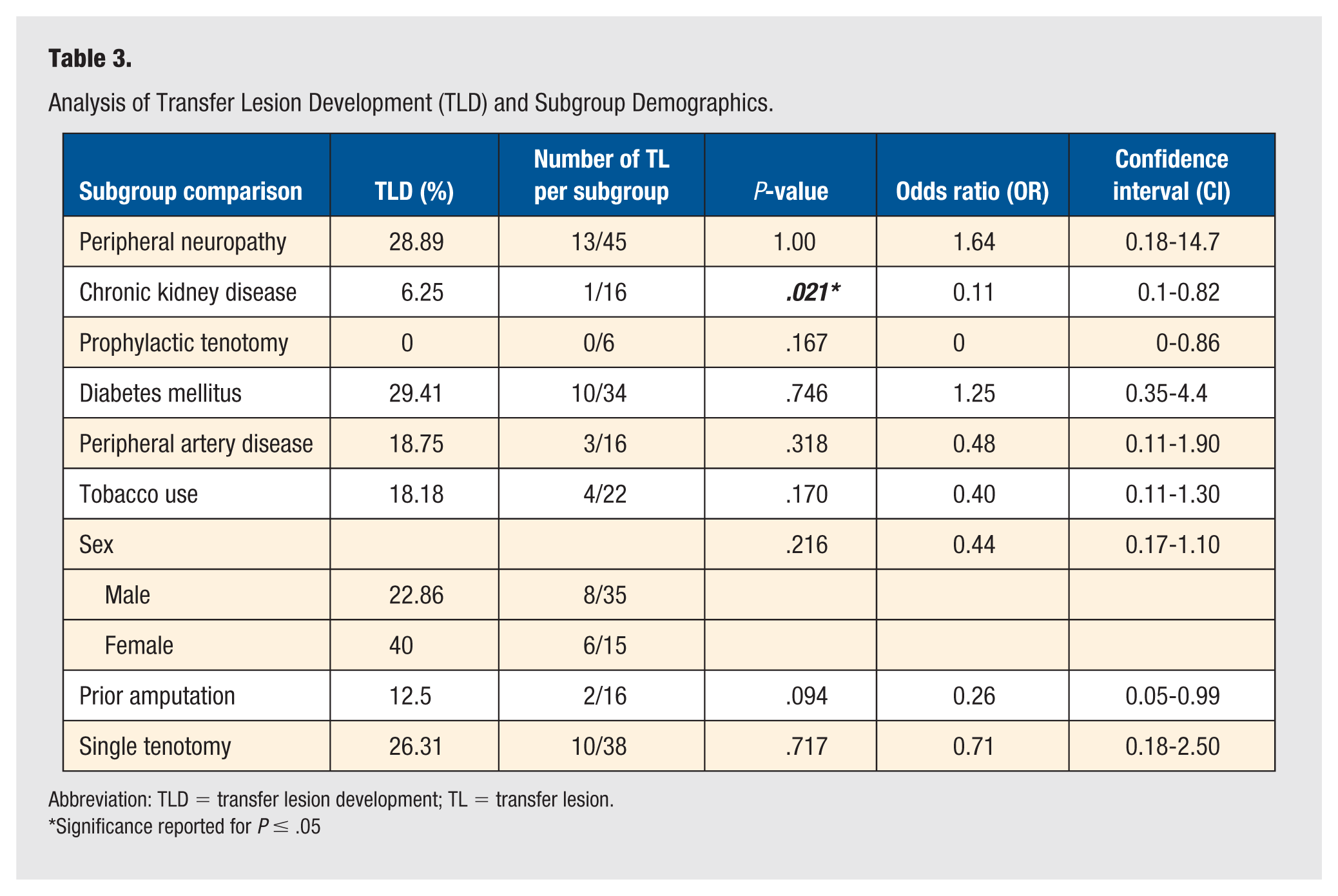
Abbreviation: TLD = transfer lesion development; TL = transfer lesion.
Significance reported for P ≤ .05
Discussion
This study adds to the growing body of evidence demonstrating that flexor tenotomy is a safe and effective procedure for treatment of digital ulcers and at-risk lesions, with high rates of ulcer healing and low rates of infection, amputation, and recurrence. In the present study of individuals with several comorbidities known to affect wound healing, only 4 digits failed to heal and required an amputation, 3 of which were performed in the setting of osteomyelitis. No infections were noted after performance of flexor tenotomy, and recurrence of ulceration at the same site was only noted in 10%. This is consistent with other flexor tenotomy studies noting a recurrence rate at the site of the initial ulcer of 11% to 19%.35,38-40
Flexor tenotomy has been suggested as a less invasive approach to addressing toe deformity and can be performed in the outpatient setting. This has been favored when compared to other open surgical approaches in the operating room for digital deformity in the diabetic foot, which have been associated with an increased risk of complications including infection and amputation. 42 A multicenter, randomized controlled trial has confirmed high rates of ulcer healing and an increased number of ulcer-free days after flexor tenotomy. 42 The benefits of the procedure have been thought to outweigh the risks, leading to a strong recommendation as per the 2023 International Working Group of the Diabetic Foot. 27 Our healing rate of 84% after performance for treatment of distal toe ulcerations was noted to be lower than prior studies, generally ranging from 92% to 100%,31,35,37-40 although when accounting for ulcer healing as well as resolution of pre-ulcerative lesions, healing rates were noted to be 92%, similar to the reported literature. We also noted no significant increased risk of complications in those with peripheral artery disease, suggesting the procedure may be safely performed in the setting of ischemia. Furthermore, nearly 60% of patients healed their ulceration without additional surgical interventions despite radiographic evidence of osteomyelitis, which lends support to the performance of flexor tenotomy in this patient population when clinically appropriate and suggests that flexor tenotomy may represent a viable alternative to amputation in the presence of osteomyelitis.
In the present study, 28% of patients developed a TL after having a flexor tenotomy performed, of which 85.7% required a subsequent flexor tenotomy to address the formation of the secondary lesion/ulceration. An additional 8% were noted to develop new callusing to the adjacent digits without evidence of a TL. Variable rates of development of TLs have been described but are generally reported to occur in approximately 8% to 15% of cases.34,36 Average time to follow up in prior studies reporting a lower rate of TLs is noted to be short-term, ranging from 7 to 22 months. It is possible that TLs may have been previously underestimated due to the length of follow-up and that TLs may develop both in the short and long term after index tenotomy, as evidenced by the timeframe of development of TLs in the current study, ranging from 7 to 923 days. Patient comorbidities including tobacco use, peripheral neuropathy, diabetes mellitus, and peripheral arterial disease were analyzed and demonstrated no association with increased risk of development of TL in this study. Only CKD was associated with reduced risk of TLs. Of the 16 patients who had CKD, only 1 developed a TL after flexor tenotomy, whereas the subset of patients that did not have CKD had 38% chance of developing a TL. We are unsure why CKD would be protective of development of TL, although we postulate this could be related to decreased ambulatory status or a more sedentary lifestyle.
Prior studies have suggested that the development of a TL is more common after an isolated flexor tenotomy procedure.36,41 This is thought to be secondary to increased peak plantar pressures to adjacent hammertoe or claw toe deformity in those non-tenotomized toes. 41 Due to concerns regarding a change in peak pressure to a toe with adjacent deformity, particularly for patients with a history of prior toe amputation, performance of prophylactic flexor tenotomy has been suggested. Some have suggested that all toes should undergo flexor tenotomy to lessen the likelihood of long-term complications. 41 Six (12%) patients in the present study had a prophylactic tenotomy, and none of these patients developed a TL. Of patients that did not have a prophylactic tenotomy performed, fourteen (32%) developed a TL. Further analysis of the risk of TL development determined no significant difference in patients undergoing single versus multiple flexor tenotomy procedures; however, 66.7% of patients who had multiple flexor tenotomies performed without a prophylactic flexor tenotomy developed a TL. While these findings were non-significant, they lend support to the performance of prophylactic tenotomy in high-risk populations, as suggested in other studies supporting multiple or prophylactic tenotomy procedures. Our results are limited by our small sample size; however, further prospective study of a larger number of patients undergoing prophylactic tenotomies may help to validate the findings of the present study.
While these findings provide valuable insights, several limitations inherent to this study warrant consideration when interpreting the conclusions. The primary limitation is the retrospective cohort design and small sample size. Retrospective reliance on existing records introduces risks related to data quality, completeness, and temporal ambiguity, compounded by limited control over the timing of follow-up visits. Consequently, reported time intervals may reflect scheduled appointment spacing rather than actual clinical progression. Additionally, the small sample size reduces statistical power and increases susceptibility to confounding effects, limiting the ability to detect significant associations. Future research should aim to mitigate these limitations by the performance of prospective studies implementing more frequent and standardized follow-up assessments and expanding the cohort size to improve robustness and control for confounding. Additionally, our study presented only short- to midterm follow-up, and studies regarding long-term outcomes of flexor tenotomy are lacking. Only 1 study of long-term follow-up of flexor tenotomy for treatment of diabetic ulcerations has been reported with an average follow-up time of approximately 149 months. 33 Interestingly, in this study, the authors noted recurrence of toe deformity in 26.7%, with 93% developing a diabetic foot ulceration and greater than 50% needing an amputation during the period of long-term study, although this was not directly associated with the performance of flexor tenotomy on the index toe. Greater than 50% were also noted to have died within the study period. This emphasizes the gravity of treating such high-risk individuals and the importance of close pedal monitoring, especially in the setting of peripheral neuropathy and diabetes mellitus.
In summary, this study suggests the flexor tenotomy is a safe procedure with reliable rates of ulcer healing and low re-ulceration rates in high-risk individuals; however, it highlights a high risk of TLs. We believe it is possible that the true rate of TLs may have been previously underestimated in those studies with short-term follow-up. Surgeons should remain vigilant for TLs in the post-procedure period, and patients should be advised of the risk for TLs after index flexor tenotomy.
Footnotes
Acknowledgements
None reported.
Author Contributions
JS: Conceptualization; Data curation; Formal analysis; Methodology; Visualizations; Validation; Writing.
DS: Conceptualization; Data curation; Formal analysis; Visualizations; Validation; Writing.
NS: Conceptualization; Data curation; Visualizations; Validation; Writing.
MH: Conceptualization; Data curation.
ZM: Conceptualization; Data curation.
AS: Conceptualization; Data curation.
SK: Conceptualization; Methodology; Visualizations; Validation; Writing.
SR-S: Conceptualization; Methodology; Visualizations; Validation; Writing.
AL: Conceptualization; Methodology; Visualizations; Validation; Writing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Review Board Protocol #2023P002420.
Consent Statement
Given the retrospective nature of the chart review, informed consent was waived.
Data Availability Statement
De-identified data are available from the corresponding author upon reasonable request and with appropriate institutional approvals.
Trial Registration
No randomized clinical trial was performed.