
Abstract
Introduction
Open reduction and internal fixation with plating is the most common surgical method of treatment for displaced intra-articular calcaneal fractures, but it has a high infection rate, which leads to chronic osteomyelitis, causing permanent disability; also, the postoperative complications are higher than those of percutaneous techniques. Thus, percutaneous fixation techniques using various indirect reduction methods provide an alternative to addressing these issues. Our study aimed to compare the functional outcomes of displaced intra-articular calcaneal fractures treated with percutaneous fixation using the Essex-Lopresti technique and 3-point distraction technique described by Forgon and Zadravecz.
Materials and methods
A prospective randomized superiority study of displaced intra-articular calcaneal fractures was conducted between July 2015 and June 2020. Patients were randomized into 2 groups; group A was operated using the Essex-Lopresti technique, and in group B, a 3-point distracter was used to aid reduction. Functional assessment was done using calcaneal fracture scoring system of Kerr et al and Maryland foot scoring system.
Results
There were 43 patients with 46 displaced intra-articular calcaneal fractures, with 27 males and 11 females. The mean duration of follow-up was 28 months. There were 20 patients with 23 calcaneal fractures in group A and 18 patients with 18 calcaneal fractures in group B. No statistically significant difference was found in functional outcomes of both techniques, but the operating time was significantly longer in group B patients.
Conclusion
Both the Essex-Lopresti technique and use of a 3-point distractor coupled with percutaneous cancellous screw fixation of displaced intra-articular calcaneal fractures provide good functional outcomes with minimal complications. There is no statistically significant difference in the functional outcomes, but outcome scores were better in the 3-point distractor group.
Keywords
“A randomized superiority trial of Essex-Lopresti versus 3-point distraction technique by Forgon and Zadravecz.”
Advances in Knowledge
Percutaneous fixation techniques are becoming more common in surgical fixation of displaced calcaneal fractures.
Essex-Lopresti and 3-point distraction techniques described by Forgon and Zadravecz are the most common techniques for percutaneous fixation of displaced calcaneal fractures.
First and only study as per our knowledge to compare functional results of these 2 most commonly used percutaneous techniques
Application to Patient Care
This study provides good evidence of functional outcomes of percutaneous fixation of displaced calcaneal fractures.
It also provides good evidence about the functional outcomes of 2 most commonly used percutaneous fixation techniques for calcaneal fractures.
Introduction
Calcaneus is the most commonly fractured tarsal bone and accounts for around 2% of all fractures occurring in adults. Of these, 60% to 75% of fractures are displaced with an intra-articular component. 1 Most common mechanism of injury for these fractures is axial loading, which occurs due to high-energy trauma as a fall from height or road traffic accidents; thus, around 10% of these fractures are associated with spine fractures and 26% are associated with other extremity injuries. 2 There are substantial economic implications of these fractures as 90% of them occur in young males between 21 and 45 years of age and frequently result in long-term disability. 3 This disabling nature of calcaneal fracture and its huge economic burden has been known since long, and it remains so even today.
Management of calcaneal fractures has been one of the most challenging and controversial issues in orthopaedic practice for many decades, and even today, it remains an enigma to be decoded. The irregular and complicated bony anatomy, multiple articular surfaces with complex joint mechanics, along with the delicate soft tissue envelop, makes the treatment of calcaneal fractures very difficult and challenging. 4 Multiple classification systems and treatment methods along with different postoperative regimens are proposed, but still there is very little consensus regarding the optimum treatment modality. Lack of consensus is documented also by the fact that so far more than 140 treatment methods have been described in the literature for calcaneal fractures. 5
The main goals of treatment for displaced calcaneal fractures are restoration of the anatomic alignment of the calcaneus as close to the normal as possible, maintaining the stability of the reduction, and reducing the postoperative complications to restore the normal functions of the foot and ankle. 6 These goals can be achieved by various methods such as nonoperative management in the form of cast, open reduction with internal fixation using plates or screws, percutaneous fixation techniques, or primary arthrodesis. There is ample evidence that patients with a displaced intra-articular calcaneal fracture (Sander’s type 2 and above) should preferably be treated surgically, as it is not possible to reduce and maintain the reduction using closed methods.7,8 Open reduction with internal fixation is the most common surgical method of treatment, but the reported infection rate of open reduction ranges between 6% and 27%, and amputations of limbs are not an exception due to chronic osteomyelitis causing permanent disability.9-11 Also, the postoperative complications are less in percutaneous fixation, even when compared with open reduction internal fixation using Sinus Tarsi approach. 12 Thus, percutaneous fixation techniques using various indirect reduction methods could provide a safer alternative addressing both the mentioned issues.
Our study aimed to compare the functional outcomes following displaced intra-articular calcaneal fractures treated with percutaneous fixation using Essex-Lopresti 13 and modified 3-point distraction techniques described by Forgon and Zadravecz,14,15 which are the two commonly used methods to aid fracture reduction for percutaneously fixing the calcaneal fractures.
Patients and Methods
A prospective randomized comparative study of 43 patients with 46 closed, displaced intra-articular calcaneal fractures was conducted between July 2016 and June 2020. Approval for the study was obtained from the Institutional Review Board (IRB), but the study was not registered in a randomized controlled trial (RCT) registry. Informed consent was obtained from each patient participating in the study. Initial radiographic assessment of all patients was done using standard anterior-posterior, lateral, and axial views for the calcaneus. Computed tomography (CT) scan was done for all patients, and fractures were classified according to Sander’s classification. 7 All skeletally mature patients with displaced intra-articular calcaneal fractures (Sander’s type 2 and type 3) were included in the study. Patients with extra-articular, undisplaced, intra-articular, severely comminuted fractures (Sander’s type 4), open fractures and patients having concomitant fracture at other sites were excluded. Extra-articular, undisplaced calcaneal fractures were excluded from the study as they are managed conservatively and do not need surgery, we excluded Sander’s type 4 fractures as they often need open reduction and this may have biased the study results.
Patients were randomized into 2 groups A and B. Patients in group A were operated and fracture reduced using Essex-Lopresti technique and in group B, a 3-point distracter was used to aid reduction (Figures 1 and 2). All the fractures were fixed with cancellous cannulated screws (Figures 3 and 4). Routine preoperative assessment was done, and patients underwent operative procedures within 7 days after the edema had settled and the wrinkle sign appeared. The average time since injury to surgery was 9.58 days. Surgery was performed under tourniquet control using spinal anesthesia. Patients received antibiotic prophylaxis at the time of induction. The patient was placed in the lateral decubitus position with the affected leg upward. Fracture was reduced and fixed with respective techniques under image intensifier guidance.

Clinical and radiological images of the Essex-Lopresti technique.

Clinical and radiological images of calcaneal 3-point distractor.
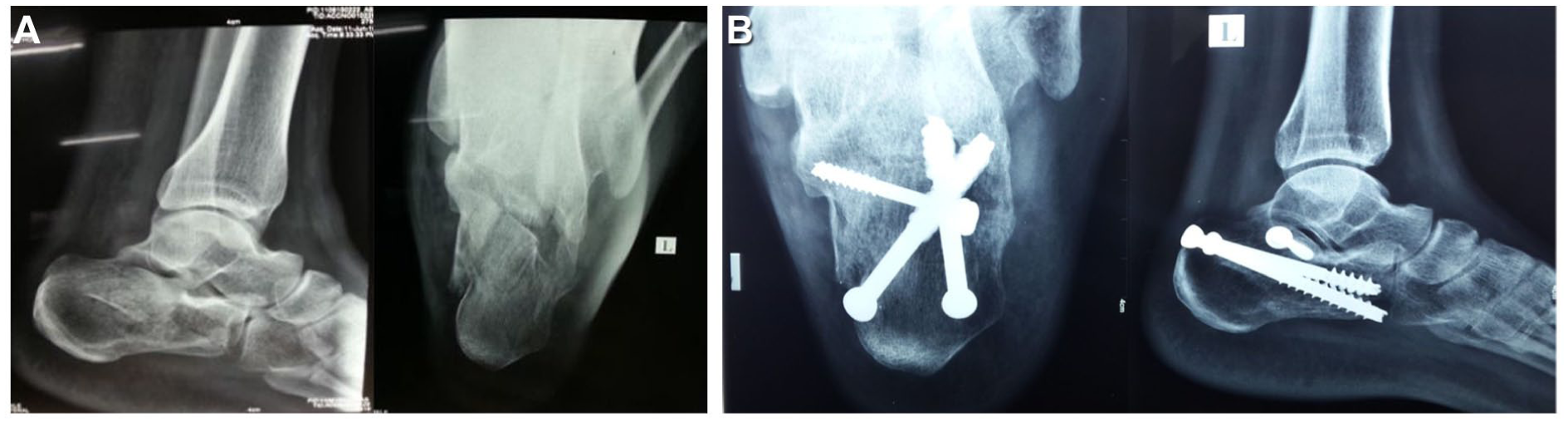
(A) Preoperative calcaneal fracture operated with Essex-Lopresti technique. (B) United calcaneal fracture at 2 years.
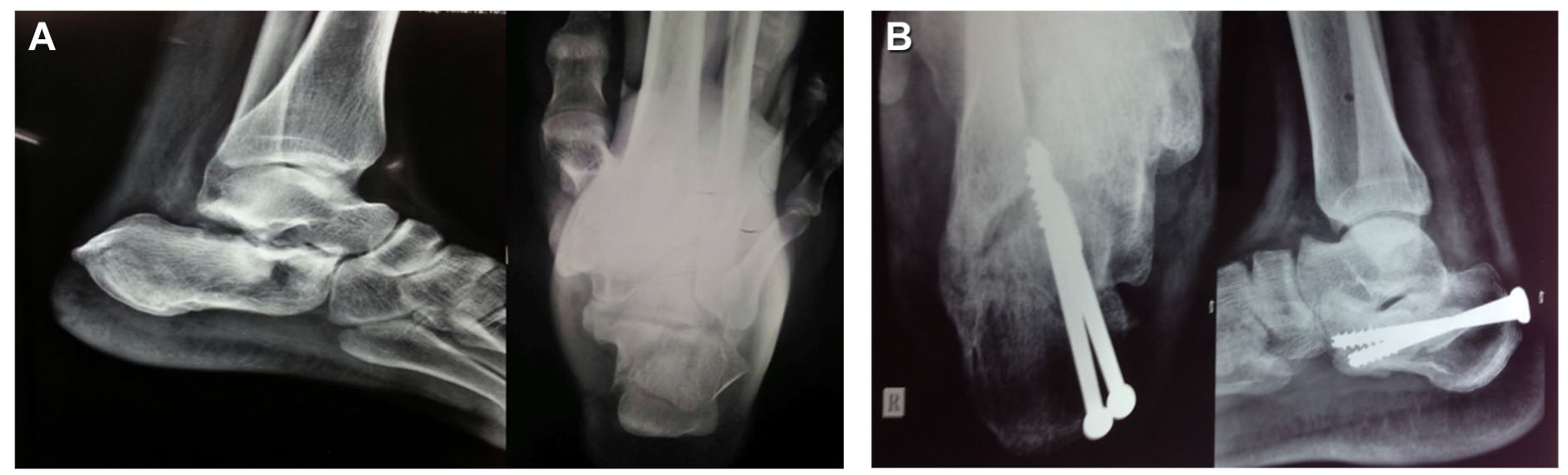
(A) Preoperative calcaneal fracture operated with 3-point distractor method. (B) United calcaneal fracture at 2 years.
Postoperatively, a below-knee plaster slab was applied. All patients were kept non-weight-bearing for 6 weeks. Ankle mobilization was started after the plaster slab was removed. The patients were followed up at 1, 3, 6, 12, and 24 months. Partial weight bearing was allowed after 6 weeks and full weight bearing on the affected limb was allowed after 3 months. Functional assessment involved the use of calcaneal fracture scoring system of Kerr et al 16 and Maryland foot scoring system17,18 by asking patients about pain during activity and rest, ability to stand and walk, ability to return to work, duration of absence from work, and any change in the size of the shoe. The difference of more than 10 points was considered a positive outcome. 11 An overall rating of excellent (90-100), good (80-89), fair (65-79), and poor (<64) according to Kerr et al scoring system and excellent (90-100), good (75-89), fair (50-74), and poor (<50) according to Maryland Foot Score was assigned to each fracture.
Statistical Analysis
The power analysis was conducted before the commencement of the study using an online tool Epi Info and the sample size was calculated assuming an SD of 15, α = .05 and a desired power of 0.80. The 2 groups were compared with respect to age, sex, Sander’s fracture type, operating time, bony union time, incidence of wound complications, calcaneal fracture scoring system of Kerr and Maryland Foot Score. The difference of 10 or more points was considered positive outcome. Statistical analysis was performed by a statistician who was not involved with the study. The parameters were compared between groups. A paired-sample t test was used for the interval data (age, operating time, length of hospital stays, bony union time). The Fisher 2-sided exact test was used to compare the functional outcome. The statistical analysis was performed using the open epi (online data analysis site). The chosen level of significance was P < .05.
Results
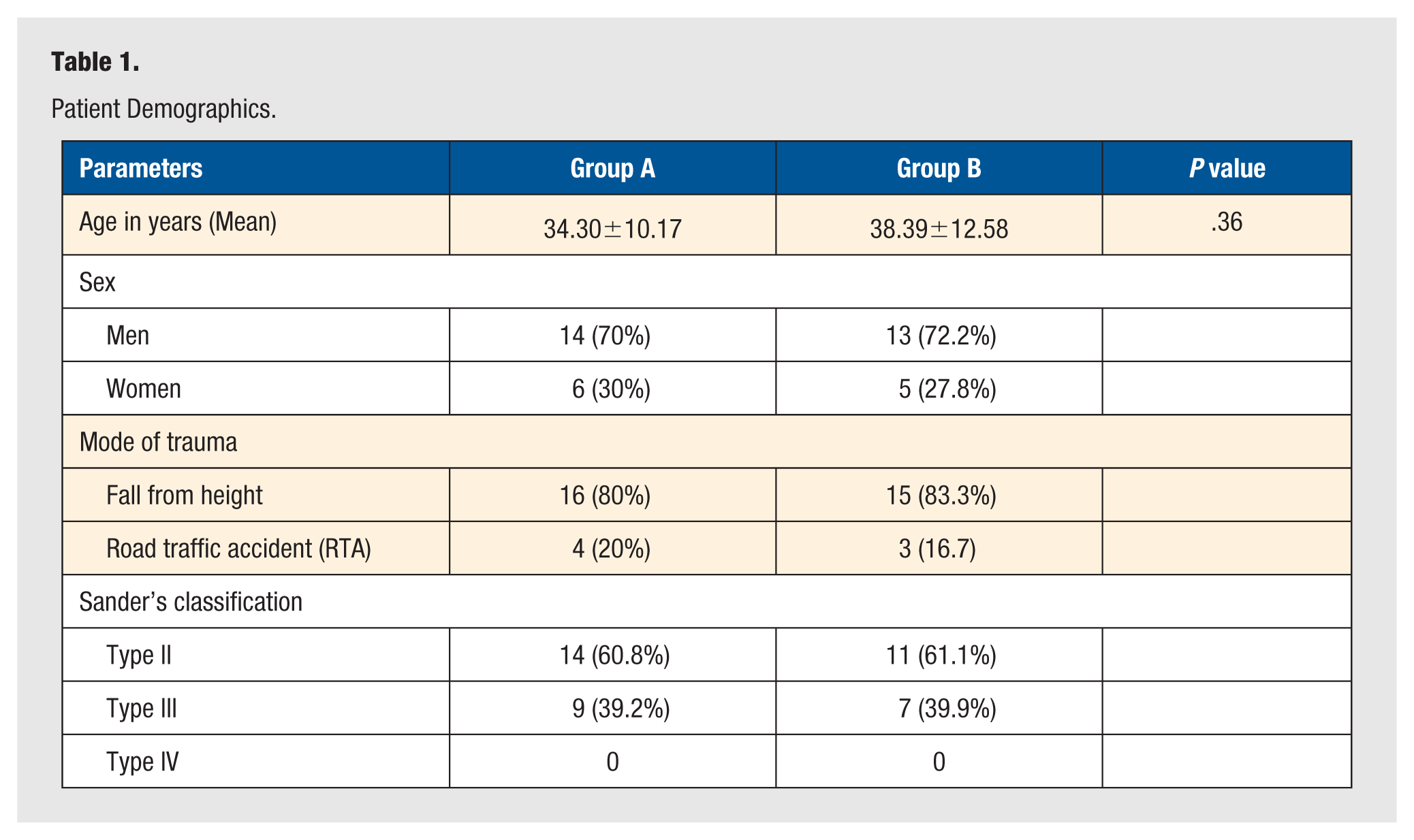
The age of the patients ranged from 21 to 62 years, with a mean age of 36 (±11.3) years. Twenty-seven patients were men and 11 were women. Thirty-one patients had sustained this injury as a result of a fall from height, while the remaining 7 as a result of road traffic accident. The mean duration of follow-up was 28 months. There were 20 patients with 23 calcaneal fractures in group A and 18 patients with 18 calcaneal fractures in group B. Five patients were lost to follow-up and thus were excluded from the study. Both groups were comparable with respect to age, sex, and fracture types (Sander’s classification). Patient demographics for 2 groups are described in Table 1.
Patient Demographics.
There was no statistically significant difference in overall functional scores at final follow-up at 2 years. The mean Maryland Foot Score being 75 (±11.6) in group A and 83 (±5.7) in group B at 1 year and 79.8 (±8.81) in group A and 83.62 (±6.54) in group B at 2 years. The mean Kerr et al score was 76.7 (±12.4) in group A and 84.8 (±5.6) in group B at 1 year and 84.83 (±9.33) in group A and 80.98 (±7.63) in group B at final follow-up at 2 years. But according to Maryland Foot Score, 94.4% patients in group B had good-to-excellent functional results compared with only 69.5% patients in group A at final follow-up. Also, according to Kerr et al scoring system, only 39.1% of patients in group A had good-to-excellent functional results as against 61.1% patients in group B at the end of 2 years (Table 2). Group B patients had better functional scores at 1 year, but there was no statistical difference at final follow-up at 2 years.
Postoperative Parameters and Functional Outcomes.
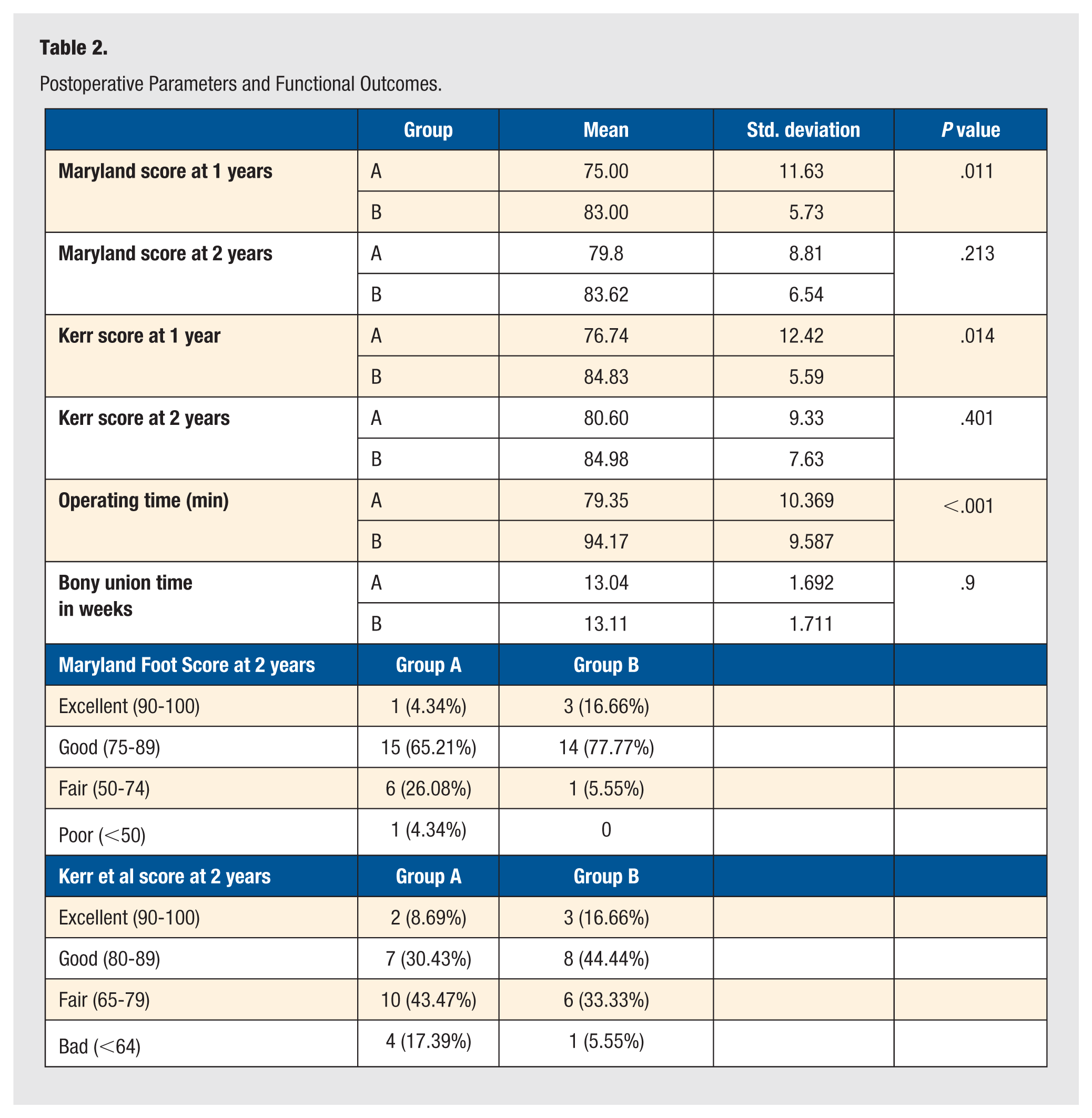
There was no statistically significant difference in mean bony union time between two groups. The mean bony union time in group A was 13.04 (±1.62) weeks, compared with 13.11 (±1.7) weeks in group B. But the operating time was significantly more in group B, where the 3-point distractor was used for aiding fracture reduction. All the fractures healed without any significant complications, except 2 patients in group B who had superficial wound infection, which was managed with regular dressings.
Discussion
Calcaneum is the most commonly fractured tarsal bone, and displaced intra-articular calcaneus fractures can cause serious disability to the patient and economic burden to the society as most of these fractures occur in young adults. It is also a treatment challenge for an orthopaedic surgeon. 19 It has been well established that patients with displaced intra-articular calcaneal fractures have poor functional outcomes when compared with other fractures. 20 This can be reflected from the fact that no single treatment method is universally recommended for calcaneal fracture management.
The open reduction and plating with conventional extensile lateral approach is considered as the “gold standard” in management of displaced intra-articular calcaneal fractures but it is associated with very high rates of wound complications and infection ranging between 6% and 32%.10,11,21-23 This has resulted in the recent popularity of the Sinus Tarsi approach, but still the postoperative complications are higher when compared with percutaneous techniques, including wound infection rates, 12 though it is significantly lower than the extensile lateral approach. Thus, many minimally invasive techniques such as limited incision approaches or percutaneous fixation techniques using indirect reduction of fracture fragments have been devised to overcome these wound complications associated with the conventional plating using lateral approach. Percutaneous reduction and screw fixation and minimally invasive open techniques resulted in significantly better outcomes compared with external fixation and open plating,24,25 and thus, these minimally invasive approaches are considered a better option in terms of postoperative complications for patients with compromised soft tissue envelop or who have co-morbidities like diabetes mellitus or smoking. 19
Thus, considering the evidence in favor of minimally invasive screw fixation techniques in the management of displaced intra-articular calcaneal fractures, we compared the two most commonly used reduction techniques: first, the Essex-Lopresti 13 reduction technique, which is based on indirect reduction of fracture fragments, and second, using the modified 3-point distractor—first described by Forgon and Zadravecz14,26—which applies the principle of distraction–reduction (ligamentotaxis) for the reduction of fracture fragments. The outcome of treatment of any calcaneal fracture can be assessed in two ways; first, by comparing various functional outcome scores, and second, by evaluating the complications associated with the treatment modality. We used Maryland Foot Score17,18 and Kerr et al 16 score to assess the functional outcomes of the above techniques and also took into account any complications associated with each technique.
Both these percutaneous fracture reduction techniques, coupled with screw fixation, provide substantially good functional outcomes with minimal complications in displaced intra-articular calcaneal fractures. This is clear from the fact that more than 95% patients in group A and 100% patients in group B had excellent-to-fair functional outcomes according to the Maryland Foot Score. Although there was no statistically significant difference in mean functional scores between the two groups, a significantly large number of patients in group B, where 3-point distractor was used, had excellent-to-good results when compared with group A. But the operative time was significantly more in group B for obvious reasons. We also found that the radio opaque rods of the distractor made it difficult for radiographic evaluation of fracture reduction intra-operatively and in four patients there was collapse of the fracture reduction after patients started bearing weight.
As with any study, our study also has few limitations; first, the sample size is small. The duration of follow-up is short, so the percentage of patients developing subtalar arthritis requiring subtalar fusion cannot be assessed. Further studies with longer follow-up are needed for this assessment. Second, we did not include radiographic evaluation of fracture reduction in our study. We did this for a couple of reasons, first and the most importantly, poor interobserver reliability in measuring both Böhler’s angle and the angle of Gissane on plane radiographs, 27 and second, it was not feasible to get postoperative CT scan for every patient due to economic constraints. Third, we did not include Sander’s type 4 fractures in our study as we feel that percutaneous reduction in such fractures is technically very demanding.
Conclusion
We believe that minimally invasive techniques for the treatment of intra-articular calcaneus fractures particularly Sander’s type 2 and 3 have several benefits. This study confirms that both the Essex-Lopresti technique and the use of 3-point distractor coupled with percutaneous cancellous screw fixation of displaced intra-articular calcaneal fractures provide satisfactory results, with most patients achieving good functional outcomes with minimal complications. Also, the use of 3-point distractor in the reduction of these fractures can provide better functional results, but it takes longer to operate and assessing intraoperative fracture reduction can be technically challenging.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
As the study is a case series where we are presenting the results of operated cases without exposing the identity of any patient, ethical committee approval was not taken. IRB approval number: NKPSIMS&RC and LMH/IEC-Pharmacology/16/2015 dated 25/06/2015. All the patients were contacted via telephone, and informed and verbal consent was obtained before submitting the manuscript for consideration.