
Abstract
Introduction
Tourniquet use for ankle fracture fixation surgery is a common but not universally accepted practice due to concerns regarding soft tissue complications. Although prior literature has demonstrated increased short-term postoperative pain, tourniquet use’s association with other complications remains under-investigated.
Methods
A retrospective cohort study was performed of adult patients undergoing open reduction and internal fixation of a closed rotational ankle fracture (OTA Type 44) between 2012 and 2024 at an urban academic health system. Patients were stratified by tourniquet use. Demographic information, injury characteristics, and operative variables were collected. The primary outcome was the development of postoperative complications—wound dehiscence, fracture-related infection, superficial wound infection, delayed wound healing, peripheral nerve injury, venous thromboembolism, and nonunion. Secondary outcomes were operative time and estimated blood loss. Multivariable logistic regression was used to evaluate the association between tourniquet use and postoperative complications.
Results
A total of 617 patients met the inclusion criteria, including 446 who had a tourniquet inflated during surgery and 171 who did not. No significant differences in baseline patient demographics or comorbidity were observed. After multivariable logistic regression, tourniquet use was not associated with higher odds of any wound complication, fracture-related infection, delayed wound healing, or peripheral nerve injury. Among patients in the tourniquet cohort, 4 developed venous thromboembolism and 7 developed a fracture nonunion. No such complications were observed among patients treated without a tourniquet. Tourniquet use was associated with a modest decrease in estimated blood loss (47.3 ± 44.2 vs 33.9 ± 36.0 mL, P < .001) with no significant increase in operative time.
Conclusion
Tourniquet use during operative fixation of closed rotational ankle fractures was not associated with increased soft tissue or bony complications. The findings support the safety of continued tourniquet use per surgeon preference, provided that appropriate patient selection is employed.
Keywords
“Tourniquet use is a common practice during orthopaedic procedures due to intended benefits such as improved hemostasis and intraoperative field visibility.”
Introduction
Ankle fractures are common orthopaedic injuries that often require operative fixation. 1 Surgical repair of ankle fractures has a relatively high complication rate, with infections being observed in 4% to 10% of patients undergoing surgery and persistent pain being observed in approximately 30% to 40% of patients. 1 Tourniquet use is a common practice during orthopaedic procedures due to intended benefits such as improved hemostasis and intraoperative field visibility. 2 However, such benefits must be balanced against the risk of time or pressure-related soft tissue complications such as pain, nerve injury, venous thromboembolism (VTE), or wound complications. 2
The real-world clinical associations between intraoperative tourniquet use and soft tissue complications following ankle fracture repair are not well investigated. Prior literature examining short-term postoperative outcomes has established that tourniquet use during ankle fracture fixation surgery is associated with worse postoperative pain and swelling, albeit without changes to hospital length of stay.3-5 With regard to long-term soft tissue complications, one study by Benedick et al 6 evaluated the association between tourniquet use and risk of postoperative infectious and wound complications and found no association between tourniquet use and such complications.
The present study aims to further elucidate the relationship between tourniquet use during open reduction and internal fixation of a rotational ankle fracture and the development of soft tissue complications such as wound dehiscence and fracture-related infection (FRI)—both suspected and confirmed. The present study also expands existing literature by examining other complications such as VTE, peripheral nerve injury, and nonunion in a cohort of patients with a minimum of 6 months of clinical follow-up.
Methods
A retrospective review was conducted of adult patients (age ≥ 18 years) who underwent open reduction and internal fixation of a closed rotational ankle fracture (OTA Type 44) at a single urban academic health system between 2012 and 2024. Inclusion criteria required a minimum of 6 months of clinical and radiographic follow-up. Patients with open fractures, those treated with temporizing external fixation, and those undergoing arthroscopic procedures or nonunion repair as the index operation were excluded.
Collected demographic variables included age, sex, and body mass index (BMI). Clinical variables included American Society of Anesthesiologists (ASA) classification, Charlson Comorbidity Index (CCI), race/ethnicity, smoking status, diabetes mellitus, peripheral vascular disease, chronic kidney disease (CKD), chronic corticosteroid use, and preoperative anticoagulation. Baseline injury characteristics included malleolar pattern, initial site of presentation (emergency department, outpatient clinic, or urgent care), and fracture classification according to the Lauge-Hansen classification system based on initial injury radiographs. 7
Surgical Protocol and Intraoperative Data
Patients were positioned supine or prone for surgery. Tourniquets were applied to the proximal thigh and inflated following draping and site preparation according to surgeon preference. Surgical approach and wound locations, anesthesia type used (general, regional, or spinal), estimated blood loss according to surgeon estimate, and length of surgery were collected from intraoperative documentation. All tourniquets were applied to the ipsilateral thigh. Tourniquet parameters (time and pressure) were collected for cases where the tourniquet was inflated, including total duration of tourniquet inflation and pressure.
Postoperative Outcomes and Complication Data
At the study institution, patients are routinely scheduled for clinical follow-up visits at 2 weeks, 6 weeks, and 3, 6, and 12 months postoperatively. Medical records from postoperative follow-up visits were reviewed to identify soft tissue complications, including wound dehiscence, superficial wound infection, delayed wound healing, FRI according to consensus definition, VTE, peripheral nerve injury, and nonunion. 8
Wound dehiscence was defined as separation of the surgical wound margins without frank purulence or clinical signs of infection. A suspected FRI was defined as erythema or drainage, with or without purulence, that resulted in treatment with oral antibiotics. Peripheral nerve injury was defined as a postoperative sensory deficit affecting the distribution of a specific peripheral nerve. Delayed wound healing was defined as failure to achieve epithelialization of the surgical wound by 6 weeks postoperatively. Nonunion was defined as failure to demonstrate radiographic union by 6 months postoperatively or undergoing a nonunion repair surgical intervention.
Statistical Analysis
Statistical analysis was conducted using SPSS version 28 (Armonk, NY). Univariate analysis of categorical and continuous variables was conducted with chi-square testing and Student t tests for independent samples. Analysis of complication data, except for peripheral nerve injury, was conducted using binary logistic regression adjusting for age, sex, BMI, ASA, smoking status, diabetes, peripheral vascular disease, and wound location (posterolateral vs lateral). Binary logistic regression for peripheral nerve injury was conducted adjusting for age, sex, BMI, wound location, and anesthesia type (regional/neuraxial vs general anesthesia).
Results
A total of 627 exclusions occurred due to inadequate follow-up (n = 399), incomplete surgical/clinical data (n =9 9), nonoperative management (n = 70), open fracture (n = 14), not being treated for a rotational ankle fracture (n = 19), external fixator placement (n = 12), undergoing arthroscopic repair initially (n = 5), initial nonunion repair (n = 4), surgery at an outside hospital (n = 3), and being under 18 years old (n = 2). A total of 617 patients met the study inclusion criteria, among which 446 underwent surgery with tourniquet inflation (72.3%) and 171 without tourniquet inflation (27.7%). Initially, 1244 patients were reviewed for eligibility. Patient selection and exclusions according to study criteria are summarized in Figure 1.
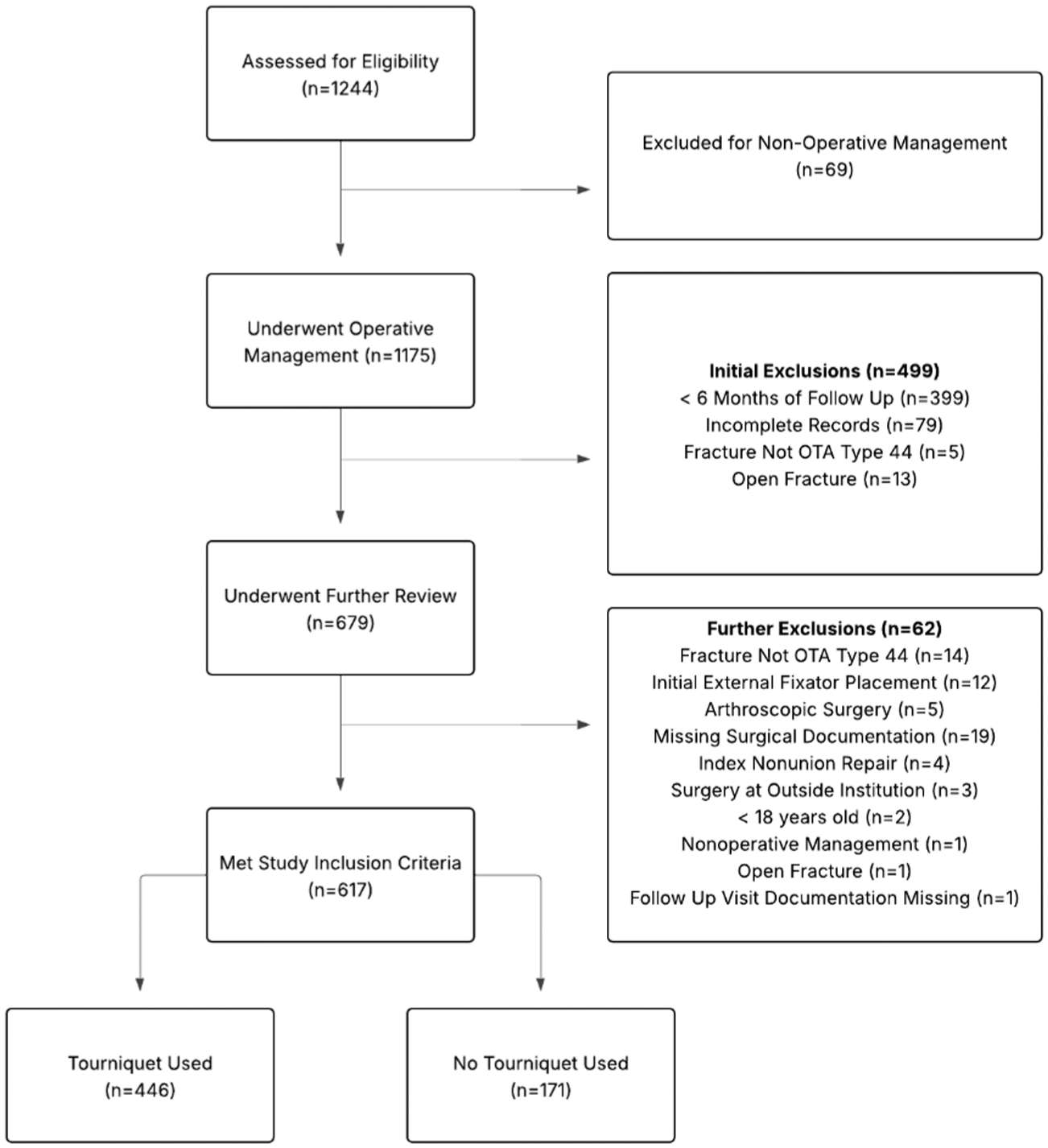
Flow diagram representing cohort selection and application of inclusion/exclusion criteria. 617 patients were included in the final analysis following exclusions for nonoperative management, follow-up, open fractures, external fixation, fracture type, incomplete records, age, arthroscopic surgery, or index nonunion repair. 446 patients underwent surgery with a tourniquet and 171 without.
With regard to demographics and baseline clinical characteristics (Table 1), there were no significant differences between the tourniquet and no-tourniquet cohorts in age (47.9 ± 17.4 vs 47.8 ± 16.3 years, P = .965), sex (35.7% vs 40.9% male, P = .221), BMI (29.0 ± 6.24 vs 29.2 ± 7.73, P = .735), race/ethnicity (P = .111), ASA class (1.90 ± 0.63 vs 1.92 ± 0.72, P = .731), or CCI (0.43 ± 0.89 vs 0.55 ± 1.35, P = .267). Similarly, no significant differences were observed in smoking status (P = .237), diabetes mellitus (P = .795), peripheral vascular disease (P = .114), CKD (P = .870), chronic corticosteroid use (P = 1.000), or preoperative anticoagulation use (P = .981).
Baseline Clinical and Demographic Characteristics of Patients Undergoing Open Fixation of Closed Rotational Ankle Fractures.
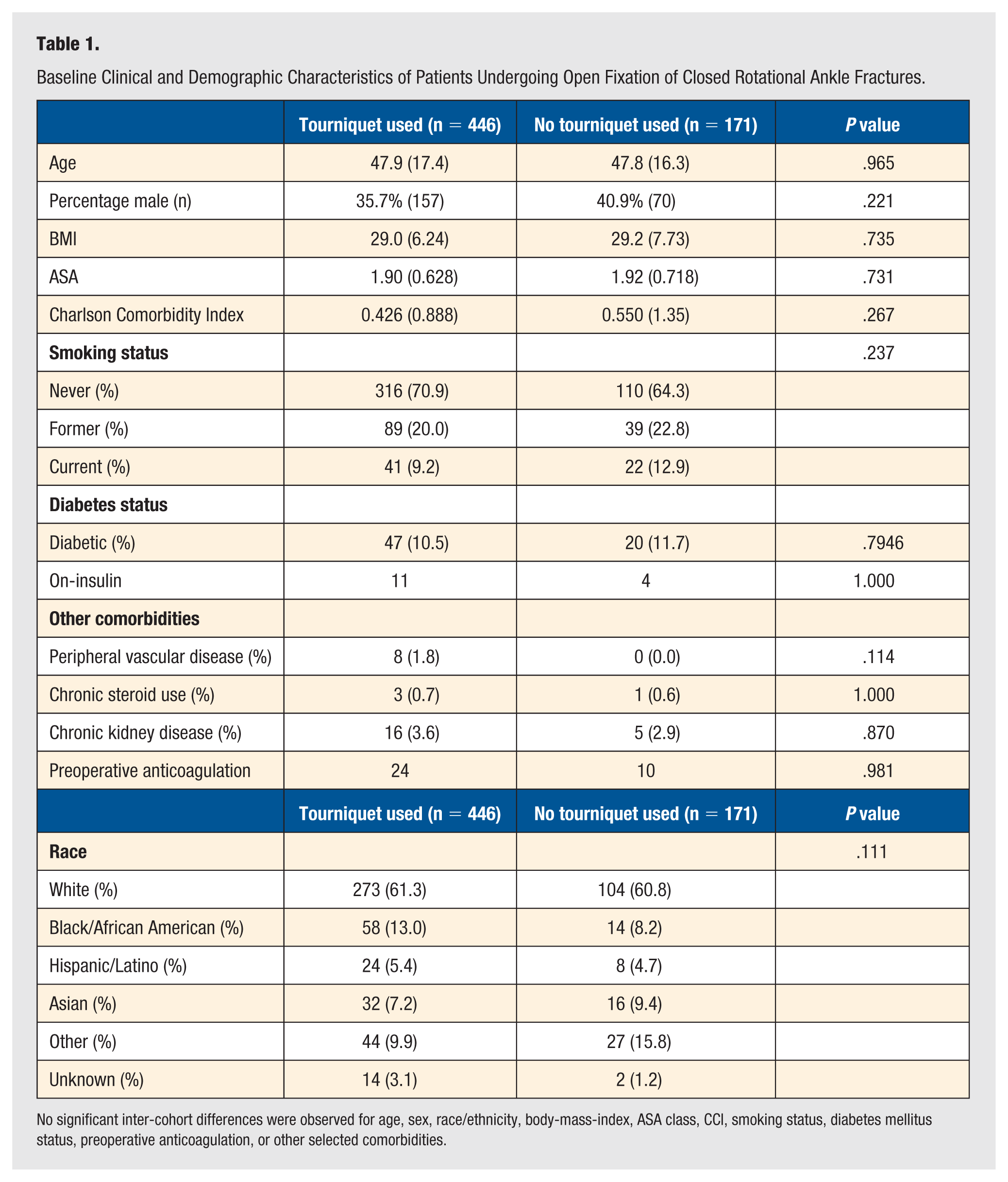
No significant inter-cohort differences were observed for age, sex, race/ethnicity, body-mass-index, ASA class, CCI, smoking status, diabetes mellitus status, preoperative anticoagulation, or other selected comorbidities.
No significant intergroup differences were observed in Lauge-Hansen classification (P = .380) or initial site of presentation (P = .198) (Table 2). However, patients in the tourniquet cohort were more likely to have sustained trimalleolar fractures, whereas isolated lateral malleolar fractures were more common in the non-tourniquet cohort (Table 2).
Additional Baseline Clinical Characteristics for Patients Undergoing Open Reduction and Internal Fixation of Closed Rotational Ankle Fractures.
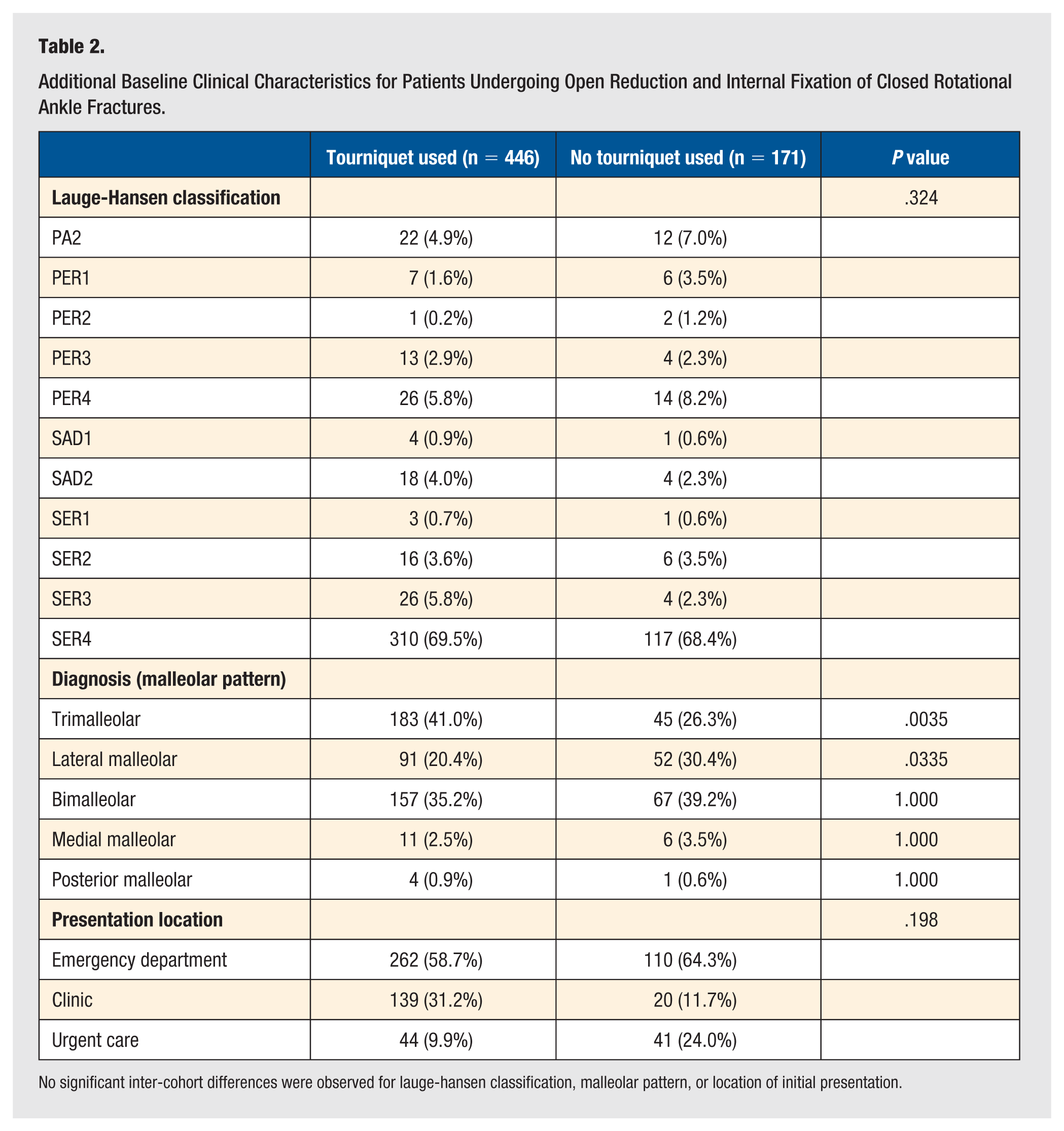
No significant inter-cohort differences were observed for lauge-hansen classification, malleolar pattern, or location of initial presentation.
Regarding surgical characteristics (Table 3), patients in the tourniquet cohort more frequently underwent fixation using posterolateral (48.9% vs 4.1%, P < .001) and posteromedial (4.9% vs 0.0%, P = .007) approaches. In contrast, patients in the non-tourniquet cohort were more likely to undergo surgery under general anesthesia (48.0% vs 33.0%, P = 0.02) and via a lateral incision (88.3% vs 47.1%, P < .001). Furthermore, patients in the tourniquet cohort were more likely to be positioned prone or be flipped from supine to prone position intraoperatively (P < .001), while non-tourniquet patients were more likely to be positioned supine (P < .001).
Baseline Surgical Characteristics of Patients Undergoing Open Reduction and Internal Fixation of Closed Rotational Ankle Fractures with and Without Tourniquets.
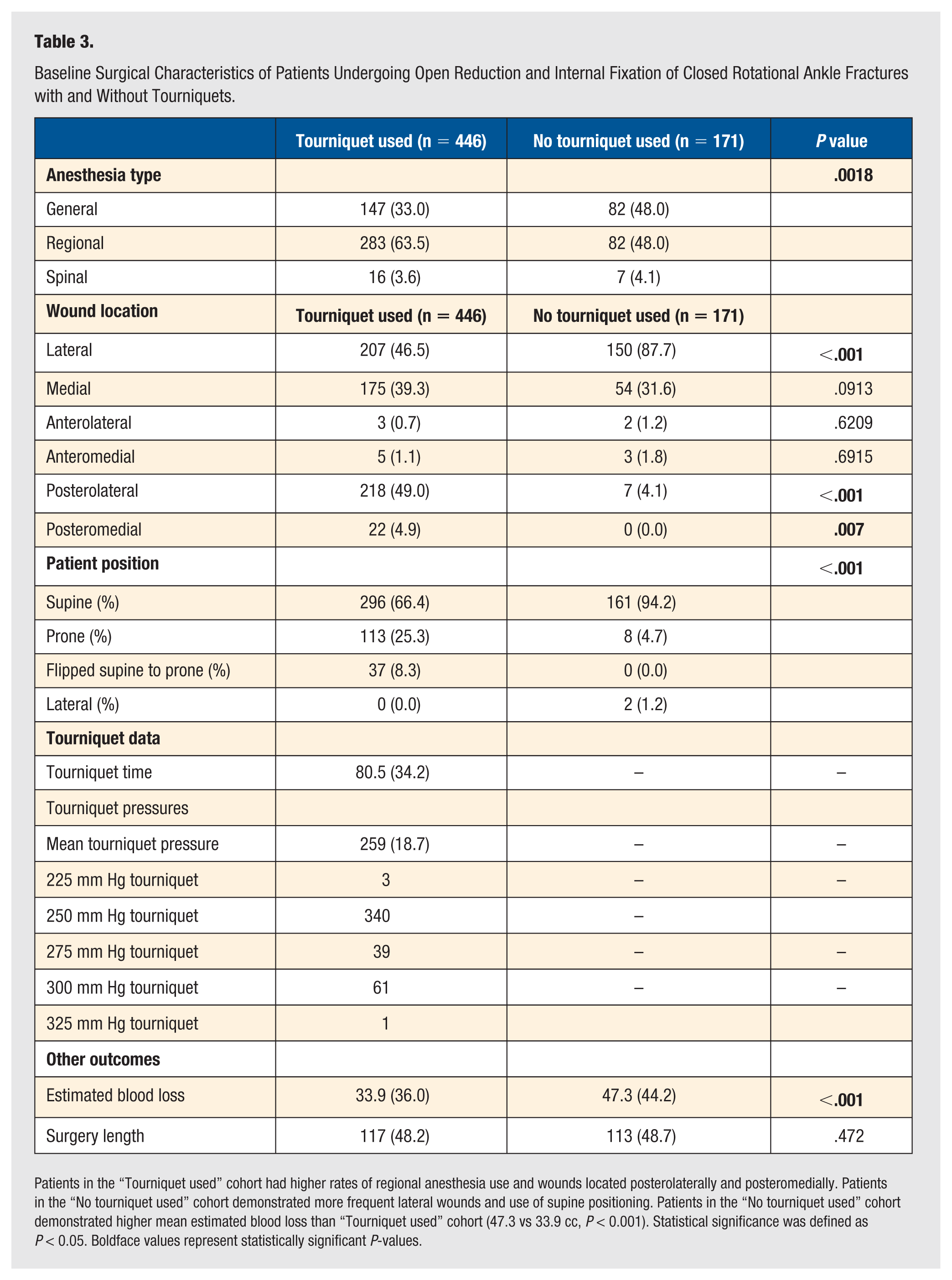
Patients in the “Tourniquet used” cohort had higher rates of regional anesthesia use and wounds located posterolaterally and posteromedially. Patients in the “No tourniquet used” cohort demonstrated more frequent lateral wounds and use of supine positioning. Patients in the “No tourniquet used” cohort demonstrated higher mean estimated blood loss than “Tourniquet used” cohort (47.3 vs 33.9 cc, P < 0.001). Statistical significance was defined as P < 0.05. Boldface values represent statistically significant P-values.
There was no significant difference in operative duration between the tourniquet and non-tourniquet cohorts (117 ± 34.2 vs 113 ± 48.7 minutes, P = .472). Estimated blood loss was higher in the non-tourniquet cohort (47.3 ± 44.2 vs 33.9 ± 36.0 mL, P < .001). Among patients treated with a tourniquet, mean inflation time was 80.5 ± 34.2 minutes, and mean tourniquet pressure was 259 ± 18.7 mm Hg, with most tourniquets inflated to 250 mm Hg (n = 340, 76.2%) and 300 mm Hg (n = 61, 13.7%).
After multivariable logistic regression, there were no significant differences between groups in the odds of any wound complication (adjusted OR = 0.80, 95% CI = 0.42-1.55, P = .51), wound dehiscence (adjusted OR = 0.65, 95% CI = 0.27-1.59, P = .35), suspected FRI (adjusted OR = 1.50, 95% CI = 0.38-5.87, P = .56), delayed wound healing (adjusted OR = 0.67, 95% CI = 0.19-2.36, P = .53), confirmed FRI (adjusted OR = 0.33, 95% CI = 0.08-1.32, P = .11), or peripheral nerve injury (adjusted OR = 2.14, 95% CI = 0.57-8.04, P = .26) (Table 4).
Soft Tissue Outcomes Following Multivariable Adjustment for Patients Undergoing Fixation of Closed Rotational Ankle Fractures.
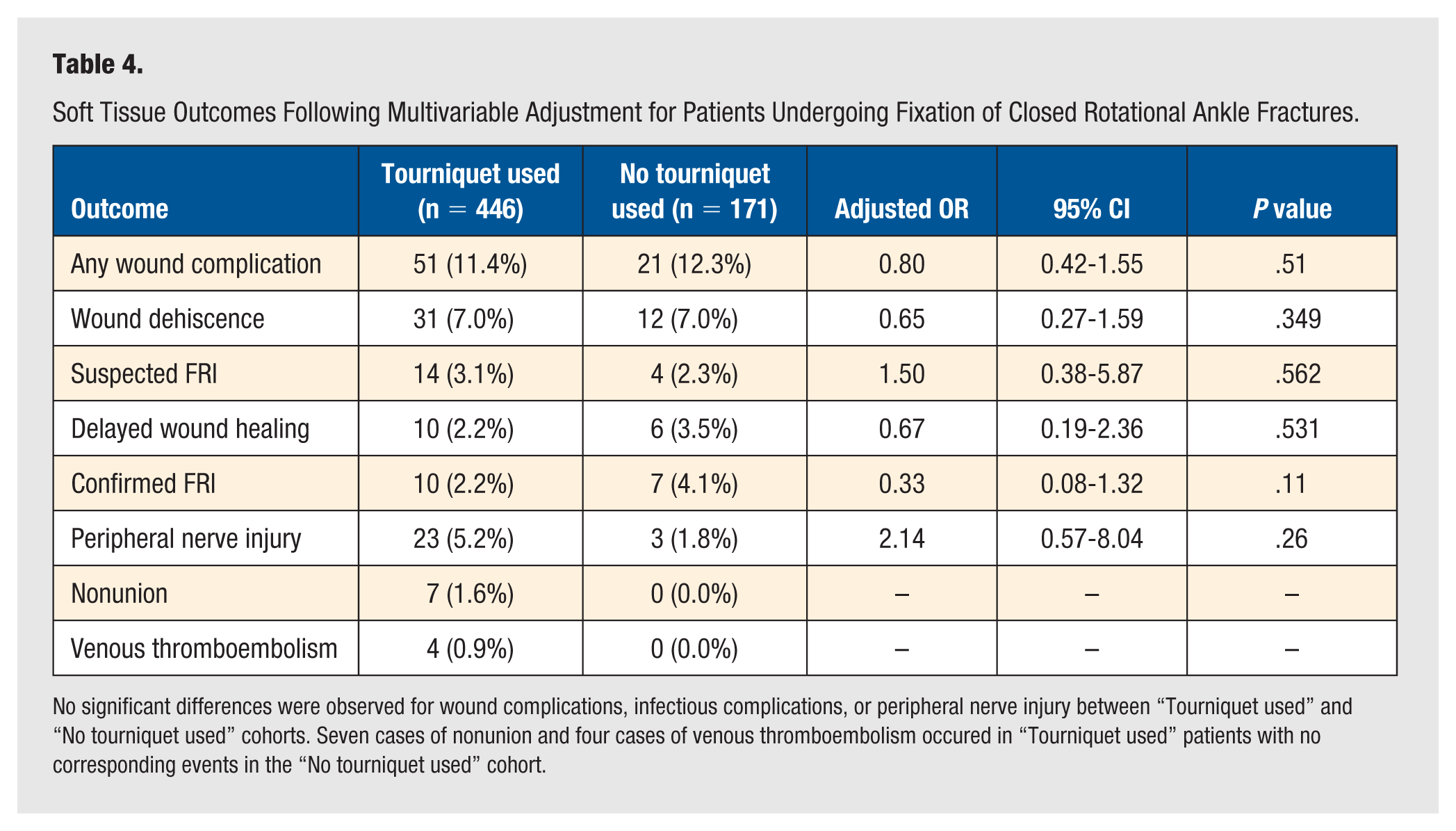
No significant differences were observed for wound complications, infectious complications, or peripheral nerve injury between “Tourniquet used” and “No tourniquet used” cohorts. Seven cases of nonunion and four cases of venous thromboembolism occured in “Tourniquet used” patients with no corresponding events in the “No tourniquet used” cohort.
There were 4 cases (0.9%) of VTE and 7 cases (1.6%) of nonunion in the tourniquet cohort, with no corresponding events in the non-tourniquet cohort. Due to the absence of events in the non-tourniquet group, these outcomes were not included in multivariable regression analysis. Among patients who developed peripheral nerve injury, the sural nerve was most frequently involved (n = 10, all in the tourniquet cohort), followed by the superficial peroneal nerve (n = 7; 5 in the tourniquet cohort) and the deep peroneal nerve (n = 6; all in the tourniquet cohort).
Discussion
The present study investigated the association between intraoperative tourniquet use and soft tissue complications following open reduction and internal fixation of closed rotational ankle fractures. A secondary objective was to determine whether omission of a tourniquet was associated with longer operative times as a marker of operative efficiency. In this retrospective cohort, tourniquet use was not associated with an increased risk of postoperative wound and bony complications, infection, nonunion, or peripheral nerve injury. In addition, forgoing tourniquet use was only associated with a modest, but not clinically significant, increase in estimated blood loss without increases to operative times. Finally, tourniquet use was not associated with increased risk for VTE.
These findings are consistent with those of Benedick et al, 6 who reported no association between tourniquet use and wound or infectious complications following ankle fracture fixation. In contrast, Maffulli et al 9 reported shorter operative times and higher complication rates associated with tourniquet use in a prospective randomized trial of isolated distal fibula fractures. Differences between these studies likely reflect variation in study design, fracture patterns, operative techniques, and the historical context of earlier investigations.
A substantial proportion of fractures in the present cohort were classified as supination–external rotation IV injuries, representing more severe stages of rotational ankle fractures. 10 Despite inclusion of higher-severity closed fracture patterns, tourniquet use remained unassociated with increased soft tissue complications, supporting the safety of tourniquet use in appropriately selected patients. The favorable outcomes observed may also reflect the overall health of the study population, which included a low prevalence of diabetes and a low mean ASA classification. Prior work has demonstrated that the absence of diabetes, younger age, and lower ASA classification are associated with improved outcomes following ankle fracture surgery. 11 Nonetheless, the observed complication rates in this cohort are consistent with previously reported rates of 4% to 10% among commercially insured patients. 1
Consistent with prior literature, postoperative wound complications were more strongly influenced by patient-related factors, including diabetes, smoking, and overall comorbidity burden, as well as injury-related factors such as open fractures and severe soft tissue compromise, than by tourniquet use alone. Surgical technique may also influence wound outcomes, including the number and location of surgical incisions. 12 Although the tourniquet and non-tourniquet cohorts differed in the proportions of lateral and posterolateral approaches, prior studies have not demonstrated clinically meaningful differences in wound-healing complications between these approaches, and the posterolateral approach has been associated with high rates of fracture healing and low complication rates.13,14
The overall incidence of peripheral nerve injury in this study was 4.2%. While the incidence of peripheral nerve injury following lower extremity surgery is not well defined in the literature, nerve injury remained relatively uncommon in the present cohort. Tourniquet-related nerve injury has been attributed primarily to mechanical compression from elevated cuff pressures and prolonged inflation times and is transient in most reported cases. 15 At the study institution, pneumatic tourniquets were routinely used, and tourniquet pressures were typically limited to 250 mm Hg, which is lower than commonly cited fixed inflation pressures of approximately 300 mm Hg for lower extremity surgery. 16 Nerve injury is more likely attributable to surgical approach rather than tourniquet use or patient positioning, 17 since 90% of sural nerve injuries (n = 9/10) occurred in patients undergoing posterolateral approaches 18 and 67% of superficial peroneal nerve injuries occurred in patients with lateral approaches. 19
From a clinical perspective, tourniquet use should not raise concern for an increased risk of ischemic or soft tissue complications in appropriately selected patients with closed ankle fractures and a low comorbidity burden, if tourniquet pressure and duration are not excessive. In contrast, greater emphasis should be placed on optimization of modifiable patient-related risk factors, such as smoking cessation and glycemic control, as well as careful consideration of injury-related soft tissue conditions. Decisions regarding tourniquet use may therefore reasonably be guided by surgeon preference and intraoperative considerations rather than concern for wound morbidity alone.
This study adds value to existing literature in several important ways. It represents the first modern ankle fracture study to report quantitative tourniquet parameters, including tourniquet inflation time and tourniquet pressure. In addition, heterogeneity in injury severity was reduced through exclusion of patients treated with external fixation and restriction to closed fractures. This analysis is also the first to adjust for incision location, an important potential confounder that has not been consistently addressed in prior studies. Furthermore, other theoretical disadvantages of tourniquet use, including peripheral nerve injury, were examined. The duration of clinical follow-up in this study was longer than that reported in much of the existing literature.
Several limitations warrant consideration. The retrospective design introduces the potential for residual confounding and selection bias. Although tourniquet pressure and duration were available, standardized tourniquet protocols were not enforced. In addition, patient-reported pain and early functional recovery metrics were not assessed. Future prospective studies incorporating standardized tourniquet parameters, patient-centered outcomes, and a greater focus on high-risk patient populations may further clarify the role of tourniquet use in ankle fracture surgery.
Conclusions
Intraoperative tourniquet use with a pressure below 300 mm Hg for less than 120 minutes was not associated with increased risk of soft tissue complications, infectious complications, or peripheral nerve injury following open reduction and internal fixation of closed rotational ankle fractures. Forgoing tourniquet use was only associated with a modest increase in estimated blood loss with equivalent operative time to intraoperative tourniquet use. These findings suggest that tourniquet use is safe in appropriately selected patients with closed ankle fractures, and that postoperative wound outcomes are more strongly influenced by patient- and technique-related factors than by tourniquet use alone.
Footnotes
Acknowledgements
The authors thank Jacob Linker, MD, for his assistance with data acquisition.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to institutional restrictions and the presence of protected health information but are available from the corresponding author on reasonable request, subject to institutional approval.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of New York University Langone Health (IRB approval: i06-581). This is an IRB-approved retrospective study.
Informed Consent
Patient consent was not required. The data used in this article is retrospective data.
Trial Registration
This is not a randomized clinical trial.