
Abstract
Background
Ligament and tendon pathology of the ankle is frequently complicated by chronic instability, poor tissue quality, and prior failed repairs. Augmentation devices have been introduced to reinforce primary repair and protect healing tissues during the early postoperative period. A novel synthetic augmentation device was used as an adjunct in primary ankle ligament repair across a range of clinical presentations.
Methods
This retrospective case series evaluates early clinical outcomes in 5 patients who underwent ankle ligament repair augmented with TEKBRACE (Theramicro, Cordova, Tennessee). The cohort included 3 males and 2 females with a mean age of 52 years (range, 37-65) and mean body mass index of 29.9 (range, 22.7-39.1). Diagnoses included acute lateral instability (n = 3), acute-on-chronic instability (n = 1), and chronic instability with concomitant tendinopathy (n = 1). All diagnoses were confirmed by clinical examination and magnetic resonance imaging. Mean follow-up was 18 weeks (range, 16-24 weeks). All patients followed a standardized postoperative immobilization and rehabilitation protocol.
Results
At early follow-up, all patients demonstrated stable clinical courses without device-related complications. There were no postoperative infections, wound complications, thromboembolic events, skin reactions, or mechanical failures. Visual Analog Scale pain scores improved from a mean of 4.8/10 preoperatively to a mean of 0.6/10 at final follow-up. Range of motion was within normal limits compared to preoperative baseline in all patients. Four of 5 patients returned to full unrestricted activity. No gross instability was detected on clinical examination at any postoperative visit.
Conclusion
Early outcomes following TEKBRACE augmented ankle ligament repair were encouraging in this small preliminary series, with no device-related complications observed. These findings support the feasibility of the technique and provide rationale for prospective investigation with standardized outcome collection and longer follow-up.
Keywords
An ideal augmentation device should provide sufficient mechanical support, integrate with host tissue, maintain long-term structural integrity, minimize bulk, and avoid inflammatory or foreign body reactions.
Introduction
An ideal augmentation device should provide sufficient mechanical support, integrate with host tissue, maintain long-term structural integrity, minimize bulk, and avoid inflammatory or foreign body reactions. 1 The modified Broström procedure has been the benchmark for chronic lateral ankle instability (CLAI) for decades. When augmented with the InternalBrace suture tape system, the construct provides a load-sharing internal splint that protects the biological repair during early healing.2,3 Published failure rates for lateral ankle ligament repair range from 5.7% to 28.5%, depending on patient risk factors including generalized laxity, poor tissue quality, and prior failed repair. 4 These limitations have driven continued interest in alternative augmentation strategies. Among the emerging options, the Artelon FlexBand (Stryker, Kalamazoo, Michigan) is a synthetic, degradable polycaprolactone-based polyurethane urea (PUUR) matrix that has been used as an augmentation device in over 50 000 orthopaedic soft tissue procedures. Kelly et al 5 reported a favorable safety profile in 105 patients undergoing FlexBand-augmented foot and ankle reconstruction, with no device-related foreign body reactions, osteolysis, or graft failures at greater than 6 months of follow-up. Scott et al 6 subsequently reported significantly lower Visual Analog Scale (VAS) pain scores at 2, 6, and 12 weeks in patients undergoing FlexBand-augmented Broström repair compared with Broström alone, with a meaningfully shorter time to full weight-bearing in the augmented group (9.0 vs 11.8 weeks, P = .027). Critically, FlexBand is a degradable material, designed to resorb over time as host tissue ingrowth occurs. TEKBRACE, by contrast, is a permanent non-degradable scaffold. Whether permanent augmentation offers clinical advantages over degradable alternatives in terms of long-term stability, recurrence prevention, or late complications remains an open and clinically important question that the current series is not powered to answer.
TEKBRACE (Theramicro, Cordova, Tennessee) is an open-weave permanent synthetic scaffold designed to address these failure modes. Unlike suture tape, which functions as a flat braided ultra-high-molecular-weight polyethylene load-sharing splint, TEKBRACE is a 3-dimensional porous scaffold designed to permit cellular infiltration and tissue ingrowth, functioning as a biological scaffold rather than a passive mechanical restraint. To date, no published clinical data exists describing the use of TEKBRACE in ankle ligament repair. This series represents the first clinical description of its application and is intended to provide early feasibility and safety data to support future prospective investigation. No conclusions regarding comparative efficacy are drawn.
Materials and Methods
Study Design
This retrospective case series includes 5 consecutive patients who underwent ankle ligament repair augmented with TEKBRACE. All procedures were performed by a single fellowship-trained, board-certified orthopaedic surgeon. Follow-up ranged from 16 to 24 weeks. The goal of this study was to evaluate early postoperative outcomes following TEKBRACE-augmented ankle ligament repair.
Patient Cohort
Inclusion criteria were age 18 years or older; clinical and magnetic resonance imaging–confirmed diagnosis of lateral ankle ligament instability, acute or chronic; failure of minimum 3 months of conservative management (physical therapy and bracing) in chronic cases; primary ligament repair augmented with TEKBRACE by the senior author; and minimum 6 weeks of postoperative follow-up. Exclusion criteria included prior ipsilateral ankle surgery, concurrent hindfoot deformity requiring osteotomy, and inflammatory arthropathy. Patient demographics and outcomes are summarized in Table 1.
Patient Demographics and Early Clinical Outcomes.
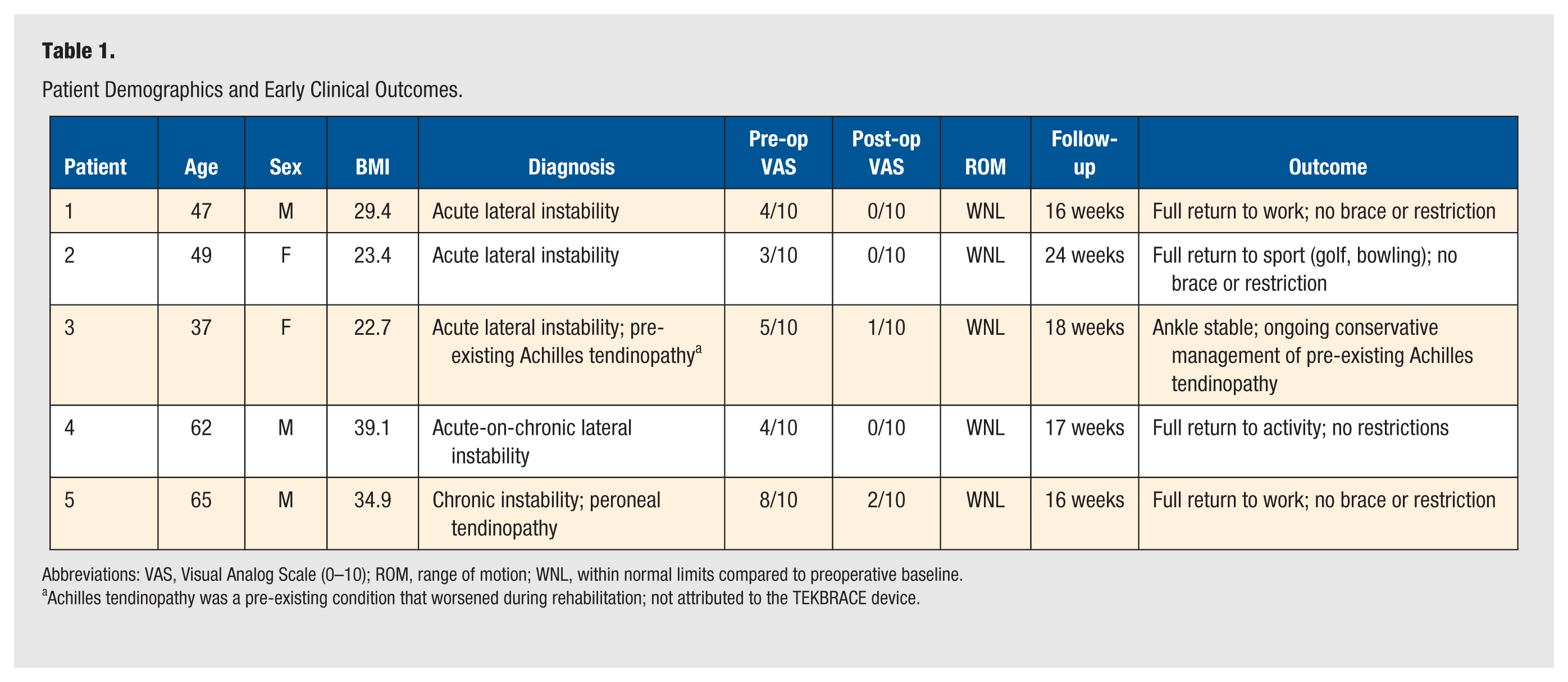
Abbreviations: VAS, Visual Analog Scale (0–10); ROM, range of motion; WNL, within normal limits compared to preoperative baseline.
Achilles tendinopathy was a pre-existing condition that worsened during rehabilitation; not attributed to the TEKBRACE device.
Surgical Technique
Positioning and exposure
The patient was positioned supine with a bump under the ipsilateral hip. A thigh tourniquet was utilized. A curvilinear incision was made just anterior to the distal fibula. Dissection was carried out to the extensor retinaculum, which was preserved to reinforce the repair.
Ligament repair (modified Broström)
The anterior talofibular and calcaneofibular ligaments were identified and transected from their attachment points. Hypertrophic scar tissue was removed. The distal fibula was lightly decorticated in preparation for repair. Suture anchors were placed into the distal fibula at the anatomic ligament origin. The ligaments were imbricated and advanced back to bone with the ankle held in neutral dorsiflexion and slight eversion.
TEKBRACE augmentation with knotless interference fixation
A knotless interference anchor was used to secure the TEKBRACE into the talus at the anterior talofibular ligament (ATFL) footprint (Figures 1, 2 and 3). The same technique was utilized proximally to secure the TEKBRACE into the distal fibula (Figure 4). The device was not over-tensioned; the ankle was held in neutral dorsiflexion and eversion throughout fixation. The inferior extensor retinaculum was then advanced, reinforcing the repair.
Postoperative Protocol
All patients followed a standardized postoperative rehabilitation protocol: 1 week of immobilization in a well-padded posterior splint at 90 degrees, followed by 2 to 3 weeks in a cast, then protected weight-bearing in a controlled ankle motion boot beginning at 3 weeks postoperatively for 4 weeks. Transition to physical therapy occurred at approximately 7 weeks, with use of a lace-up ankle support until the patient had full confidence outside of the brace.
Device Description
TEKBRACE (Theramicro, Cordova, Tennessee) is an open-weave synthetic graft engineered to be highly porous, facilitating cellular infiltration and tissue ingrowth throughout the scaffold (Figure 5). Unlike resorbable augmentation materials, TEKBRACE is designed to maintain structural integrity for the lifetime of the patient, providing sustained reinforcement to the repaired ligament. The implant delivers sufficient tensile strength to support repair while remaining flexible enough to align with native ligament biomechanics. Corded ends allow efficient passage through knotless interference anchor eyelets. The graft features a low-profile footprint measuring less than 1 mm in thickness, delivering reinforcement with minimal bulk. These characteristics are particularly relevant in anatomic regions with limited soft tissue coverage, creating prominence and potential wound complications, such as the anterior talofibular and calcaneal fibular ligament footprints.
Resorbable augmentation devices composed of poly-
Results
At early follow-up, all 5 patients demonstrated stable clinical outcomes without evidence of mechanical failure. There were no postoperative infections, wound complications, thromboembolic events, skin reactions, or adverse inflammatory responses attributable to the device. Visual Analog Scale pain scores improved in all patients, with a mean preoperative score of 4.8/10 (range, 3-8) decreasing to a mean of 0.6/10 (range, 0-2) at final follow-up (Table 1). All patients achieved protected weight-bearing in a controlled ankle motion boot at 3 weeks postoperatively, transitioning to physical therapy at approximately 7 weeks. Range of motion at final follow-up was within normal limits in all 5 patients, with no evidence of restricted dorsiflexion attributable to the augmentation construct. No gross ankle instability was identified on clinical examination in any patient at any postoperative visit.
Four of 5 patients returned to full unrestricted activity, including return to work and sport. Patient 3, a 37-year-old female with a pre-existing Achilles tendinopathy, experienced a flare of that condition during rehabilitation that is ongoing and managed conservatively. This is not attributed to the device; her ankle remained stable without gross instability on clinical examination at final follow-up.
Discussion
This case series presents early clinical outcomes following the use of TEKBRACE as an augmentation device in ankle ligament repair. The purpose of this series is not to demonstrate comparative efficacy but to describe the first clinical experience with a device for which no prior published data exists, and to establish that its application is technically feasible without early safety issues.
The InternalBrace suture tape system represents the most studied augmentation device in this space. Coetzee et al 2 reported favorable outcomes in 81 patients undergoing augmented Broström repair, with high satisfaction and a mean return to activity of 84 days. Comfort et al 8 reported comparable outcomes between augmented and non-augmented Broström repair at a median follow-up of 5 years, highlighting that the long-term benefit of augmentation remains uncertain. A systematic review by Anaspure et al 9 confirmed low complication rates across multiple augmented repair cohorts, with return-to-sport typically under 12 weeks in athletic populations. Cho et al 10 reported favorable outcomes following suture tape-augmented Broström repair specifically in patients with generalized ligamentous laxity, a subpopulation in whom standard repair carries higher recurrence risk. Kulwin et al 11 conducted a prospective comparative study of suture tape augmentation versus modified Broström alone and found that augmentation did not demonstrate a statistically significant advantage in functional outcomes. Lewis et al 12 reached similar conclusions in a systematic review, finding no clear difference in clinical or radiological outcomes between augmented and standard Broström repair. Taken together, this data confirms the clinical benefit of augmentation remains an active area of investigation. 11 - 14 The Artelon FlexBand (Stryker, Kalamazoo, Michigan) is the other primary augmentation device currently in use. Kelly et al 5 reported no device-related complications in 105 FlexBand-augmented foot and ankle procedures at greater than 6 months of follow-up. Scott et al 6 published multicenter retrospective data on 152 FlexBand-augmented Broström repairs with low complication rates and no device-related adverse events. A retrospective comparison of FlexBand versus InternalBrace in 43 patients showed equivalent time to full activity in both groups with no complications in the FlexBand cohort. 15 Stryker has initiated a multicenter prospective randomized trial (NCT06638138) with 2-year follow-up and standardized outcome collection, demonstrating the demand for rigorous prospective data across all augmentation platforms. 16 TEKBRACE is a newer device in this space. Unlike FlexBand, which is designed to degrade as biological incorporation occurs, TEKBRACE is a permanent scaffold. The clinical implications of permanent versus degradable augmentation have not been established and represent a key area for future investigation.
The permanent, low-profile nature of TEKBRACE warrants further evaluation in anatomic regions with limited soft tissue coverage where implant bulk is a clinical concern. The history of earlier generations of synthetic grafts is instructive in this regard. These materials initially showed attractive biomechanical profiles but were abandoned due to synovitis, foreign body reaction, and mechanical failure at longer follow-up. This history confirms that a 16- to 24-week observation window is insufficient to draw meaningful safety conclusions and that longer follow-up is essential before broader clinical adoption.
Limitations
This study has several limitations that must be acknowledged. The sample size of 5 patients is insufficient for any statistical inference, and no power analysis was performed, consistent with the descriptive intent of a preliminary feasibility case series. The retrospective design, single-surgeon experience, absence of a control group, and heterogeneous patient population introduce meaningful risk of selection and observer bias. Prospectively collected patient-reported outcome measures, including American Orthopaedic Foot & Ankle Society, and Foot and Ankle Outcome Scores (AOFAS and FAOS), were not obtained at the time of treatment and cannot be retroactively generated. This is acknowledged as a primary weakness of the study and future prospective studies should be performed. The follow-up window of 16 to 24 weeks is inadequate to assess ligament healing, long-term mechanical durability, late inflammatory reactions, or foreign body response. Caution is warranted in interpreting the absence of early complications as evidence of long-term device safety.
This study was conducted in a private practice setting. Formal institutional review board oversight was not applicable. The included patients provided informed consent for treatment and for the use of de-identified clinical information for research purposes, consistent with applicable standards for retrospective case series reporting.
Conclusion
In this preliminary case series, TEKBRACE augmentation in ankle ligament repair demonstrated technical feasibility in 5 consecutive patients, with no device-related infections, mechanical failures, thromboembolic events, or adverse tissue reactions observed at a mean follow-up of 18 weeks. Given the small sample, short follow-up, and absence of prospectively collected standardized outcome measures, no conclusions regarding efficacy or long-term safety can be drawn. These findings support further investigation through prospective study with standardized outcome collection, objective stability testing, and minimum 12-month follow-up.
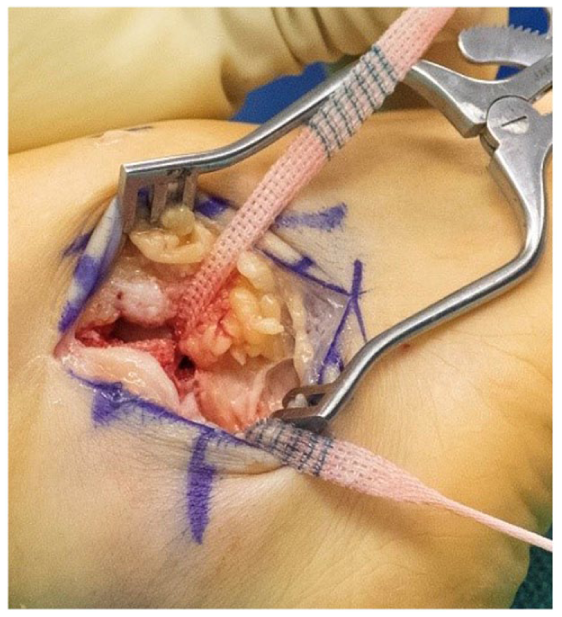
Intraoperative photograph demonstrating TEKBRACE placement at the anterior talofibular ligament (ATFL) footprint.
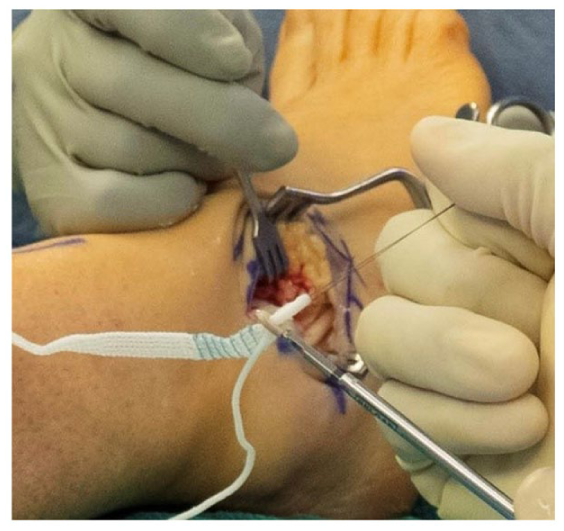
Completed construct following TEKBRACE augmentation and inferior extensor retinaculum advancement.
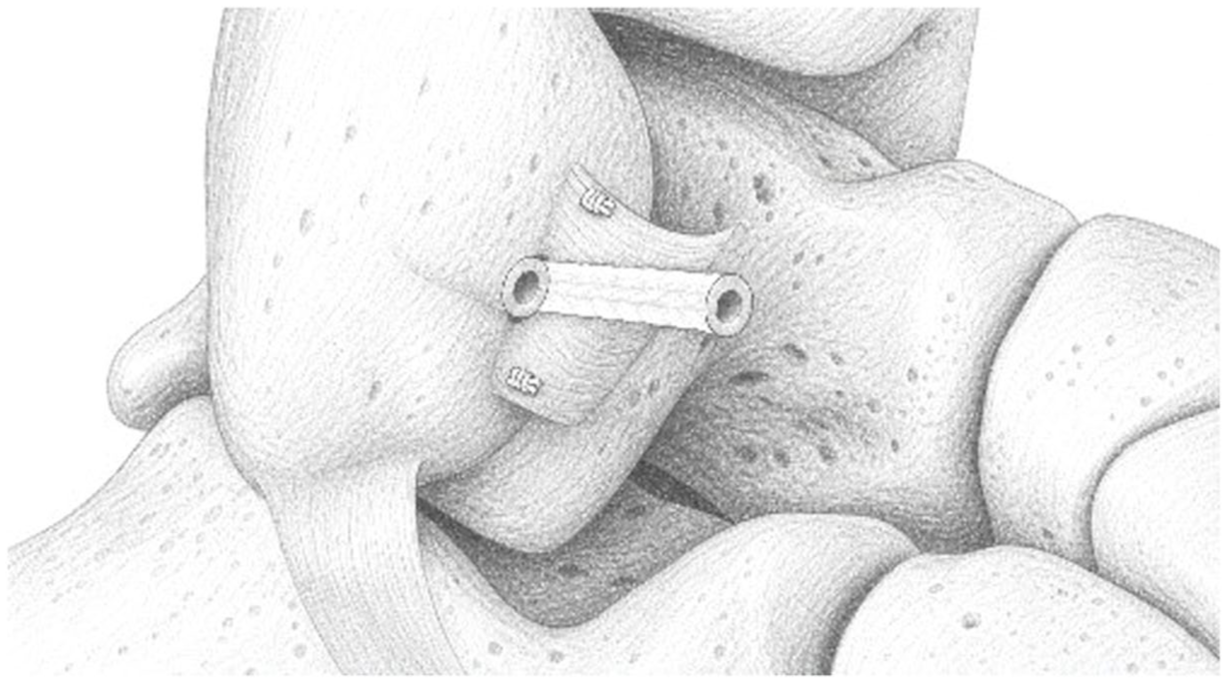
Illustration of the completed TEKBRACE augmentation construct at the anterior talofibular ligament (ATFL) footprint following isolated ATFL repair.
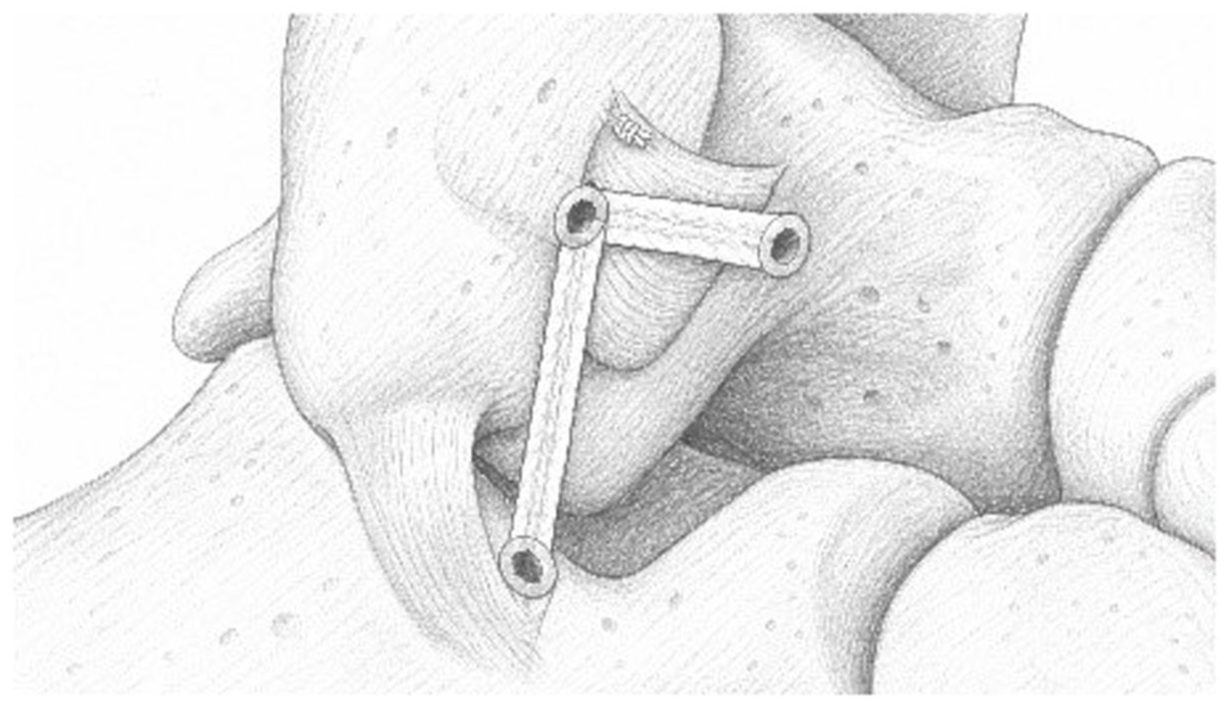
Illustration of combined ATFL and calcaneofibular ligament (CFL) augmentation using the TEKBRACE system.
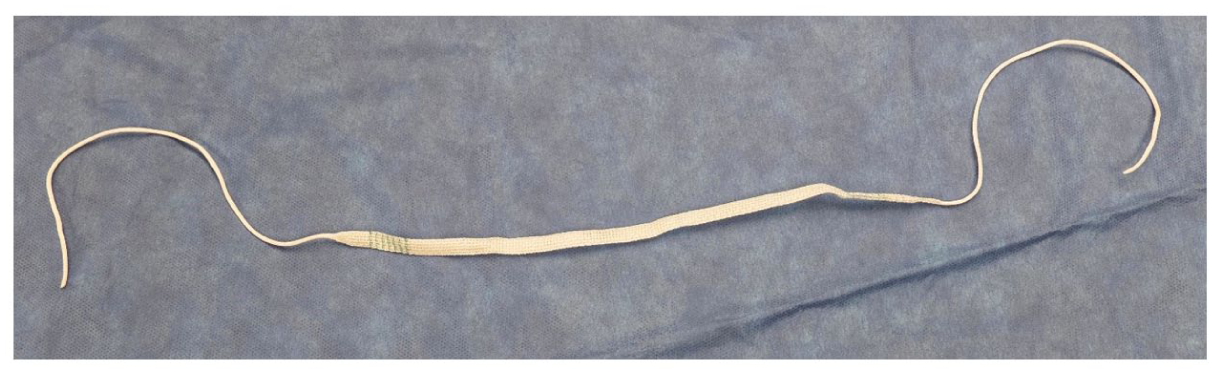
TEKBRACE synthetic augmentation device (Theramicro, Cordova, Tennessee).
Footnotes
Acknowledgements
The authors wish to thank Alexa Simpson for her assistance with literature search and manuscript preparation.
Declaration of Conflicting Interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The senior author discloses that they serve as a paid consultant for Theramicro (Cordova, TN), the manufacturer of the TEKBRACE device.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.