
Abstract
Concentrated bone marrow aspirate (cBMA) is an autologous biologic increasingly used in orthopaedic surgery for its regenerative potential. It contains mesenchymal stem cells (MSCs), growth factors, and cytokines that contribute to tissue repair and immunomodulation. Mesenchymal stem cells primarily exert their effects through paracrine signaling and macrophage reprogramming, promoting a shift from a pro-inflammatory (M1) to a reparative (M2) phenotype. Emerging evidence also suggests a role for mitochondrial transfer in this process. In foot and ankle surgery, cBMA has been investigated in the management of osteochondral lesions of the talus, fracture healing, and tendon disorders. Early clinical studies suggest potential improvements in functional outcomes, healing rates, and revision rates; however, the available evidence remains heterogeneous and is largely limited to small, non-randomized studies. Variability in cBMA preparation and reporting further limits comparability across studies. As such, while cBMA represents a promising adjunct in foot and ankle surgery, its clinical role is not yet fully defined. Future research should focus on prospective, controlled studies with standardized methodologies and explore emerging cell-free approaches, including MSC-derived extracellular vesicles, to optimize regenerative strategies.
Keywords
“Concentrated bone marrow aspirate (cbma) is an autologous biologic increasingly used in orthopaedic surgery for its regenerative potential.”
Introduction
The use of biologic adjuncts in orthopaedic surgery has expanded significantly over the past 2 decades, with the goal of enhancing tissue healing, reducing recovery time, and improving clinical outcomes. Concentrated bone marrow aspirate (cBMA) has emerged as an increasingly utilized biologic due to its unique combination of mesenchymal stem cells (MSCs), hematopoietic progenitor cells, cytokines, and growth factors.1-3 Unlike platelet-rich plasma (PRP) or hyaluronic acid, cBMA provides both a cellular and signaling environment that may enhance tissue repair through immunomodulation, angiogenesis, and matrix regeneration. Preclinical studies have demonstrated its potential to improve bone healing, 4 cartilage repair,5,6 and tendon healing7,8 through paracrine signaling and macrophage polarization. 9
However, despite its growing use, clinical evidence remains heterogeneous. This can be partially explained by variability in preparation techniques, lack of standardization, and evolving regulatory considerations. Differences in harvest site, processing methods, and final cellular composition may significantly influence biologic activity, making comparisons across studies difficult.3,10-20 These factors, combined with the relative paucity of high-level foot and ankle-specific data, highlight the need for a focused synthesis of the available literature.
The present study was conducted as a narrative review of the literature to qualitatively summarize the available evidence of cBMA in foot and ankle surgery, including its biologic composition, mechanism of action, and clinical applications across common conditions such as osteochondral lesions of the talus (OLT), fracture healing, and tendon disorders.
Basic Science
Composition and Mechanism of Action
Bone marrow biopsy and aspiration (BMBA) was initially performed in the early 20th century to diagnose bone marrow disorders, with Alexander Friedenstein being the first to harvest bone marrow mesenchymal stem cells (BM-MSC) in the 1960s.5,21,22 Since that time, numerous preclinical studies have evaluated the role of bone marrow aspirate in bone and cartilage healing.4-6
Bone marrow aspirate (BMA) is obtained by percutaneous aspiration of the medullary cavity, most commonly from the iliac crest, although alternative sites such as the tibia, calcaneus, or humerus may be used. Bone marrow aspirate contains hematopoietic cells, plasma, and a small fraction of MSC, which comprise less than 0.01% of the nucleated cells but exert significant paracrine effects.1-3
Following centrifugation, the removal of red blood cells and plasma results in cBMA, resulting in a 5- to 10-fold increase in nucleated cells and cytokines compared to raw aspirate (Figure 1).3,15,16,23,24 Concentrated bone marrow aspirate contains supraphysiologic levels of platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), transforming growth factor-β (TGF-β), insulin-like growth factor-1 (IGF-1), as well as anti-inflammatory mediators such as interleukin-1 receptor antagonist protein (IL-1RA/IRAP).2,3,25 These factors promote chemotaxis, angiogenesis, and matrix synthesis while inhibiting catabolic pathways. 23
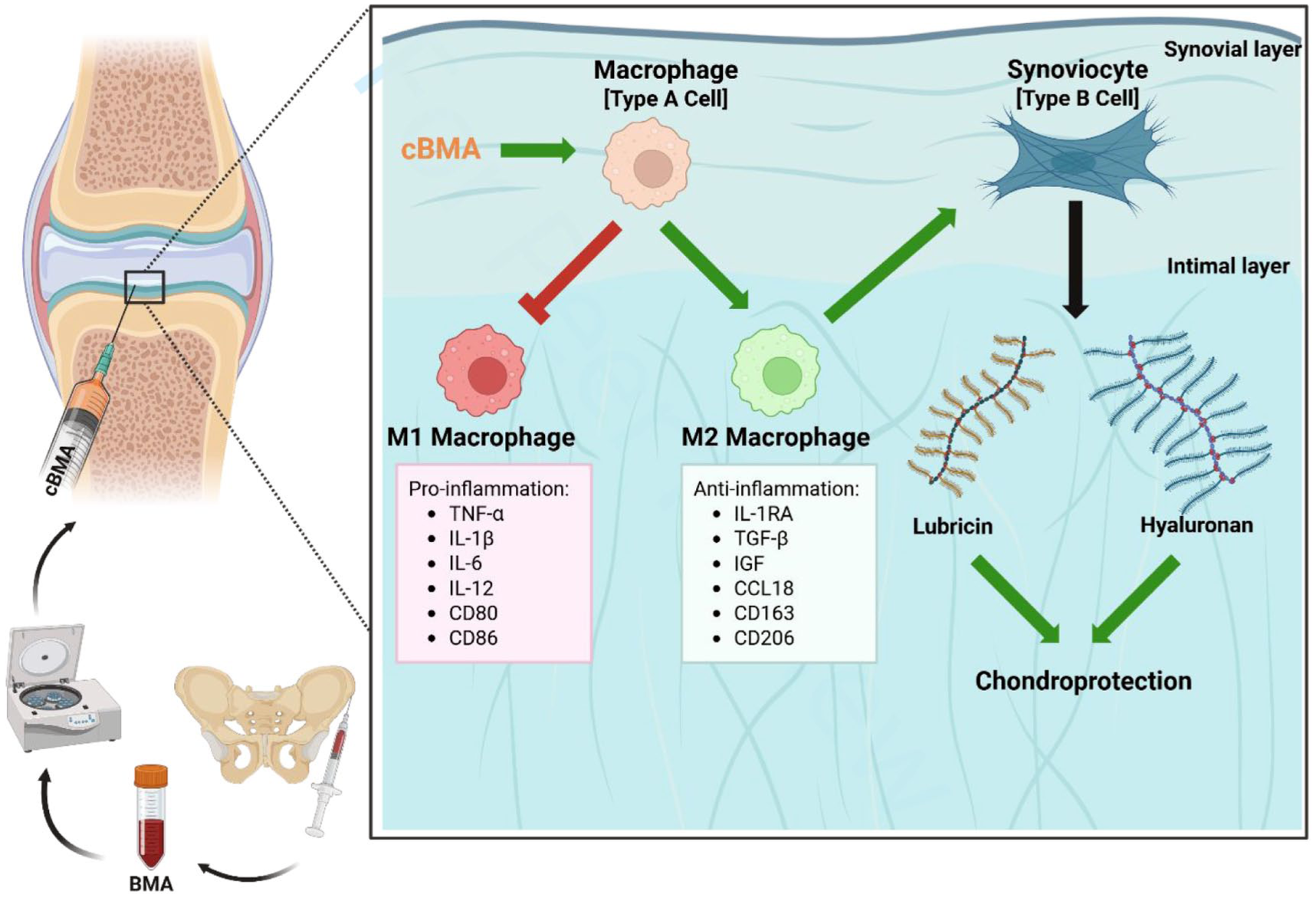
Illustration of extraction, processing, and proposed mechanism of action of cBMA in the joint.
Despite this anabolic profile, cBMA also contains pro-inflammatory mediators including interleukin-1β (IL-1β) and IL-8, which are secreted by activated leukocytes.2,3,23,26 As such, the biologic effect of cBMA is dependent on the balance between anabolic and catabolic signaling, particularly the ratio of IL-1RA to IL-1β (IL-1RA/IL-1β). This ratio is tightly regulated in healthy tissue3,9 but may be reduced in osteoarthritic environments due to increased pro-inflammatory activity. 27 Concentrated bone marrow aspirate has been shown to contain relatively high levels of IL-1RA relative to IL-1 β, distinguishing it from other autologous biologics such as PRP;2,23 however, there is considerable variability between individuals. 3
The cellular component of cBMA is primarily comprised of mononuclear cells, including lymphocytes, monocytes, and MSCs, hematopoietic stem cells, and platelets. 2 Although MSCs are present in low numbers, they exert potent immunomodulatory and regenerative effects, largely through paracrine mechanisms rather than direct differentiation into tissue-specific cells.26,28 These effects are mediated through a complex interplay of cellular signaling, cytokine release, and modulation of the local microenvironment.
The MSC secretome comprises a wide range of trophic factors that influence neighboring immune and stromal cells, resulting in immunomodulation, recruitment of endogenous MSCs, and angiogenesis. One of the primary mechanisms of action is macrophage polarization, whereby MSC-derived factors such as IRAP promote a shift from a pro-inflammatory M1 phenotype to a reparative M2 phenotype, in part through the suppression of the NF-κB signaling pathway. 29 A second proposed mechanism is phagocytic reprogramming, whereby viable and apoptotic MSCs are engulfed by circulating and resident macrophages. This interaction results in an upregulation of M2 markers (CD163+ and CD206+), suppression of tumor necrosis factor alpha (TNF-α) and IL-1β, and enhanced IL-10 and TGF-B secretion.30,31 More recently, mitochondrial transfer has been proposed as an additional mechanism of MSC-mediated immunomodulation. Through extracellular vesicles, MSCs transfer functional mitochondria to macrophages, promoting oxidative phosphorylation, reducing reactive oxygen species production, and further supporting M2 polarization.32,33
Collectively, these mechanisms create a pro-regenerative environment characterized by increased levels of IL-1RA, TGF-β, macrophage colony-stimulating factor (MCSF), and adhesion molecules such as vascular cell adhesion protein 1 (VCAM-1), which facilitate recruitment of endogenous MSCs and endothelial progenitor cells to the site of injury.23,25 This coordinated signaling promotes angiogenesis, extracellular matrix (ECM) organization, and integration of repair tissue. These are all processes critical for bone healing, fusion consolidation, and osteochondral repair in foot and ankle surgery.
Extraction and Processing
Bone marrow aspirate is most commonly obtained from the iliac crest, with the posterior superior iliac spine (PSIS) and anterior superior iliac spine (ASIS) yielding the best results.10-14 The aspirate is collected in heparin or Anticoagulant Citrate Dextrose Solution (ACD-A), processed via centrifugation to separate red blood cells from the buffy coat layer of mononuclear cells. 23 Removal of red blood cells has been shown to increase IL-RA expression and improve the biologic activity of the final product. 34 The yield and quality depend on several factors. Small-volume single-site aspirations, minimal red-cell contamination, and the use of heparinized saline have been shown to produce superior colony-forming units (CFUs) and cytokine profiles.34-37 Inter-device variability exists among commercial systems, which may affect cell yield and composition3,15,16 emphasizing the need for standardized aspiration and processing protocols to ensure consistency of cBMA product. Finally, patient factors such as age and systemic inflammation reduce progenitor cell counts, while sex and body mass index (BMI) have minimal influence on quality or yield.17-20
Basic Science in Foot and Ankle Surgery
Preclinical data supports the use of cBMA in musculoskeletal repair, demonstrating enhanced cartilage, bone, and soft tissue healing. In translational cartilage models, cBMA combined with bone marrow stimulation (BMS) has been shown to improve macroscopic, histologic, and imaging-based repair compared to BMS alone. 38 The addition of cBMA resulted in improved defect filling, tissue integration, and increased type II collagen and glycosaminoglycan (GAG) content.38,39
In bone healing models, cBMA provides osteoprogenitor cells and growth factors such as PDGF, VEGF, and TGF-beta, which promote osteoblast differentiation and neovascularization. Red blood cell depletion has been associated with increased IL-1RA levels and reduced inflammatory signaling, thereby improving the biological milieu for bone repair.9,40,41 These findings support the osteogenic and osteoconductive properties underlying the clinical use of cBMA in fracture healing.42-45
In tendon and ligament translational models, cBMA has been shown to enhance collagen fiber organization, improve tensile strength, and exert anti-inflammatory effects through M2 macrophage polarization.7-9 In ligament repair, cBMA has also been associated with increased cell adhesion and bone turnover. 46
Taken together, these findings suggest that cBMA exerts its effects through paracrine signaling, cytokine modulation, and immunoregulation, rather than direct MSC engraftment. 26 These biological mechanisms are the foundation for clinical application across a range of foot and ankle pathologies.
Clinical Evidence in Foot and Ankle Pathologies
Osteochondral Lesions of the Talus
Osteochondral lesions of the talus are focal injuries involving the articular cartilage and underlying subchondral bone, most commonly occurring following ankle sprains or repetitive microtrauma.47,48 These lesions may result in persistent pain, swelling, and mechanical symptoms and, if untreated, can progress to degenerative ankle arthritis. 49 Management remains challenging due to the talus’ limited vascular supply and inherently poor healing capacity of articular cartilage.
The use of cBMA has been most extensively studied in the treatment of OLTs, particularly as an adjunct to BMS, autologous osteochondral transfer (AOT), and scaffold-based cartilage repair techniques. Across several comparative studies, cBMA augmentation has been associated with improvements in radiologic and functional outcomes.12,50-63 In a retrospective comparative study of 34 patients, BMS augmentation with cBMA demonstrated higher Foot and Ankle Outcome Scores (FAOS) and improved Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) compared to BMA alone at 48 months’ follow-up. 50 Similarly, in a prospective cohort of 101 patients, clinical outcomes were comparable between groups; however, the cBMA cohort demonstrated a lower rate of revision compared to controls (12.2% vs 28.8%). 51
Augmentation of AOT with cBMA has also been associated with significant improvements in FAOS and Short Form-12 (SF-12) scores, with low donor-site morbidity reported (4%). 52 ECM scaffold-based techniques combined with cBMA, such as BioCartilage (Arthrex, Naples, Florida), demonstrated superior MOCART scores, enhanced defect fill rate, and lower revision rates compared to controls.54,55,59 Long-term follow-up studies suggest the durability of these results, with sustained improvements in clinical scores and graft survival rates exceeding 90% at 10 years.61,64 Concentrated bone marrow aspirate has been used with autologous matrix-induced chondrogenesis (AMIC); however, no differences in outcomes, complications, or secondary surgeries were demonstrated. 65
Despite these encouraging findings, the majority of studies were retrospective or non-randomized, with heterogeneity in surgical techniques, lesion size, and adjunctive therapies. Additionally, variability in cBMA preparation protocols, including harvest site, aspirate volume, centrifugation settings, and final cell concentration, is inconsistently reported. These limitations make it difficult to isolate the independent effect of cBMA and compare outcomes across studies. While existing data suggest that cBMA may enhance cartilage repair and reduce revision rates, higher-level evidence is required to establish its definitive role in OLT management.
Fifth Metatarsal Fractures
The use of cBMA as an adjunct in fifth metatarsal fracture fixation has been primarily described in athletic populations, particularly in zone II and III (Jones-type) fractures, where healing complications are more common.
In a retrospective series of 26 patients undergoing intramedullary screw fixation augmented with cBMA, significant improvement was observed in FAOS (51.1-90.9; P < .01) and SF-12 scores (28.2-58.4; P < .01), with a mean radiographic union time of 5 weeks, and a 92% return to sports. 42 A separate study of 25 professional athletes treated with fixation augmented with both cBMA and demineralized bone matrix (DBM) reported 100% union and return to play at a mean of 8.7 weeks, with a refracture rate of 12%. 43
While these results are promising, several limitations must be considered. Both studies are small, retrospective case series without control groups and involve concomitant mechanical stabilization with intramedullary fixation, which is known to yield high union rates independently. 66 Additionally, the combined use of DBM in some cases introduces further confounding, making it difficult to isolate the independent contribution of cBMA. As such, while cBMA may play a role in augmenting biologic healing in high-demand patients, current evidence is insufficient to establish a causal relationship. Prospective controlled studies are needed to better define its utility in this setting. 67
Medial Malleolus Stress Fractures
Medial malleolar stress fractures represent a relatively uncommon but clinically significant injury, particularly in high-level athletes. The use of cBMA as an adjunct to open reduction and internal fixation (ORIF) has been explored in this population. In a retrospective series of 16 professional soccer players treated with ORIF and cBMA augmentation, 100% radiographic union and return to sport were reported, with 81% achieving excellent outcome scores based on the Ogilvie-Harris score at 2-year follow-up. 44
Although these findings suggest a potential benefit, the study is limited by its small sample size, lack of a control group, and highly selective athletic population. It remains unclear whether the favorable outcomes are attributable to cBMA or to stable fixation and the intrinsic healing potential of this cohort. Therefore, while cBMA may represent a promising adjunct, its independent effect in medial malleolar stress fractures has yet to be clearly established.
Hallux Sesamoid Disorders
Hallux sesamoid disorders, including chronic sesamoiditis and stress-related pathology, can result in significant functional limitation, particularly in athletic populations. In a retrospective series of 15 patients, percutaneous cBMA injection was associated with significant improvement in FAOS scores (51.3-81.4; P < .001), with a 73% return to sport, and a low rate of persistent pain. 68
However, this study is limited by its small sample size, lack of a comparator group, and heterogeneity in underlying pathology. As such, while cBMA may provide a potential non-operative treatment option, further studies are required to determine its efficacy relative to established treatments and to better define patient selection criteria.
Achilles Tendon Disorders
The application of cBMA in Achilles tendon pathology has been described in both acute rupture repair and chronic tendinopathy.
In a retrospective case series of 27 patients undergoing Achilles tendon repair augmented with cBMA, a mean Achilles Tendon Rupture Score (ATRS) of 91 ± 4 was reported at a mean follow-up time of approximately 30 months, with 92% of patients returning to sport within 6 months. 69 For chronic tendinopathy, percutaneous cBMA injection was associated with significant improvements in Visual Analogue Score (VAS) pain at 6 weeks (VAS = 6.3 to 4.3; P = .04), 10 weeks (VAS 6.3 to 3.4; P = .03), and 48 weeks (VAS 6.3 to 2.6; P = .007) follow-up. No significant differences were observed between insertional and non-insertional tendinopathy, and no major complications were reported. 70
Despite these favorable outcomes, both studies are limited by the absence of control groups and relatively small sample sizes. Therefore, while these findings suggest a potential role for cBMA in enhancing tendon healing and reducing inflammation, definitive conclusions regarding efficacy cannot be drawn. Further comparative studies are needed to establish its role relative to standard surgical and non-operative treatments.
Limitations
This review is limited by the overall quality and heterogeneity of the available literature. Most clinical studies evaluating cBMA in foot and ankle surgery are small, retrospective series without control groups, limiting the ability to establish causality. Additionally, the frequent use of concomitant procedures or adjunctive biologics introduces confounding, making it difficult to isolate the independent effect of cBMA. There is also significant variability in cBMA preparation protocols, including harvest technique, processing methods, and final cell composition, which is inconsistently reported and likely contributes to differences in outcomes. Finally, there remains a paucity of high-level evidence, particularly randomized controlled trials, in foot and ankle–specific applications. As such, current findings should be interpreted with caution, and further prospective studies are needed to better define its clinical role.
Conclusions and Future Directions
Concentrated bone marrow aspirate has demonstrated promise in foot and ankle surgery due to its ability to modulate inflammation and support tissue repair. These effects are largely mediated by MSCs through paracrine signaling and macrophage reprogramming, with emerging evidence supporting a role for mitochondrial transfer. Together, these mechanisms promote a shift from a pro-inflammatory M1 phenotype to a reparative M2 phenotype, contributing to improved healing in conditions such as OLTs and fracture healing.
However, the current clinical evidence remains heterogeneous largely due to variability in cBMA preparation protocols. Standardization is paramount for improving clinical outcomes and reproducibility across studies. Future research should focus on well-designed prospective studies with standardized and transparent methodologies to better define the clinical role of cBMA. In addition, further investigation into MSC-derived extracellular vesicles and other cell-free approaches may offer alternative therapeutic strategies and help refine regenerative treatments in foot and ankle surgery.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.