
Abstract
Background. The purpose of this systematic review is to evaluate the clinical outcomes, complication rates, and failure rates following platelet-rich plasma (PRP) injections for lateral ankle ligament injuries. Methods. During June 2025, a systematic review of the PubMed, EMBASE, and Cochrane Library databases was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 guidelines to identify comparative clinical studies evaluating PRP for lateral ankle ligament injuries. Data extracted included patient demographics, clinical outcomes, complications, failures, and secondary procedure rates. Results. Five studies were included involving a total of 126 patients (126 ankles) who received PRP injections and 48 patients (48 ankles) who were in the control cohort, with a mean follow-up of 7.1 ± 4.3 months. Across studies, no consistent differences were found in clinical outcome scores between PRP and control cohorts at short-term follow-up. Significant heterogeneity in PRP preparation and administration protocols precluded a pooled meta-analysis from being performed. Platelet-rich plasma injections were associated with low complication (3.4%) and failure (5.1%) rates, and no secondary procedures were reported. Overall, the certainty of the available evidence was low, representing a limited and heterogeneous evidence base. Conclusion. Based on limited short-term data, the available studies do not demonstrate a clear or consistent difference in clinical outcomes between PRP-treated patients and controls. However, the evidence base is scarce, highly heterogeneous, and of low certainty. Substantial variability in PRP preparation and administration, small sample sizes, and short follow-up preclude reliable quantitative synthesis and comparative conclusions. Consequently, the current literature is insufficient to determine whether PRP provides any clinical advantage over standard care for lateral ankle ligament injuries. Further well-designed, adequately powered prospective studies with standardized PRP protocols and longer follow-up are warranted.
Level of Evidence: V
The purpose of this systematic review is to evaluate the clinical outcomes, complication rates, and failure rates following platelet-rich plasma (prp) injections for lateral ankle ligament injuries.”
Introduction
Lateral ankle ligament injuries are among the most common musculoskeletal injuries, with an estimated 27 000 cases occurring a day in the United States, accounting for approximately 30% of all athletic injuries. 1 Lateral ankle ligament injuries most commonly occur due to forced inversion and plantarflexion of the foot, most frequently injuring the anterior talofibular ligament (ATFL). The severity of injury ranges from sprain of the ligament to complete rupture, often associated with lateral ankle pain, swelling, and instability during ambulation. 2 Initial management is typically conservative and includes the rest, ice, compression, and elevation of the injured extremity, together with balance and proprioception training via formal physical therapy.3,4 Overall, 85% to 90% of cases resolve with conservative management. However, patients with persistent instability or collagen disorders require surgical intervention.
Although often labeled as a minor injury, lateral ankle ligament injuries can progress to chronic lateral ankle instability (CLAI) in approximately 10% to 15% of patients, resulting in persistent pain, instability, and impaired athletic performance.5,6 There has been a growing interest in the use of ortho-biologic therapies, such as platelet-rich plasma (PRP), as a potential adjunctive therapy in the conservative management of early lateral ankle ligament injuries and CLAI. The PRP is an autologous blood product containing anti-inflammatory proteins and cytokines that may enhance soft tissue healing and reduce pain; however, its efficacy in lateral ankle ligament injuries remains unclear. Previous systematic reviews, including those by Milo and Braganza 7 and Banerjee et al 8 have evaluated PRP for ankle sprains but are limited by clinical heterogeneity. Registered randomized controlled trials (RCTs) investigating PRP in both acute and chronic lateral ankle ligament injuries further highlight ongoing investigation, yet no definitive conclusions have been established (NCT02609308, NCT01518335, and NCT03197428).
Therefore, the purpose of this systematic review is to evaluate the clinical outcomes, complication rates, and failure rates following PRP injections utilized in the treatment of lateral ankle ligament injuries. Although previous systematic reviews have evaluated the use of PRP in ankle sprains, including lateral ankle ligament injuries, the available evidence remains heterogeneous and limited, precluding high-certainty conclusions regarding clinical outcomes. Therefore, an updated and methodologically rigorous synthesis focusing on clearly defined lateral ankle ligament injuries is warranted.
Materials and Methods
Search Strategy
In June 2025, a systematic review of the PubMed, EMBASE, and Cochrane Library databases was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The systematic review was not prospectively registered in PROSPERO; however, a predefined protocol outlining the study objectives, eligibility criteria, and data extraction methods was established by the authors prior to study selection and database screening. The following Boolean search strategy was utilized: (“PRP” OR “platelet-rich plasma” OR “biologic”) AND ([“ankle AND ligament”] OR [“ankle AND sprain”] OR [“lateral ankle ligament injuries”]). Studies met the inclusion criteria if they reported on outcomes after PRP injection for acute or chronic lateral ankle ligament injuries, were published in peer-reviewed journals, and were written in English. Studies were excluded if they were review articles, cadaveric studies, included patients with prior surgery to the ipsilateral ankle, or used biologic injections other than PRP (Supplementary Table 1). Once the data were retrieved, the titles, abstracts, and full-text articles were screened by 2 independent reviewers of all searched studies. If any disagreements arose, a senior author was consulted.
Assessment of Level of Evidence and Methodological Quality
The level of evidence (LOE) was assessed using previously accepted criteria in the Journal of Bone and Joint Surgery. 9 The risk of bias was assessed by 2 independent reviewers using the Risk of Bias 2 (RoB 2) for randomized control trials (Figure 1) and the risk of bias in non-randomized studies of interventions (ROBINS-I) for non-randomized studies (Figure 2). The certainty of evidence for each key outcome was assessed using the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) criteria (Table 1). Overall, the certainty of evidence across studies was very low. The certainty of evidence was downgraded due to the substantial risk of bias inherent in the predominantly small, non-randomized studies and the methodological limitations of the included studies. Additional downgrades were applied for imprecision, as most outcomes were reported from limited sample sizes. Furthermore, the heterogeneity in the reporting of outcomes downgraded studies for inconsistency. If any discrepancy arose for RoB 2, ROBINS-I, or GRADE criteria assessment, a senior author was consulted to evaluate the data for a final consensus.

Risk of bias 2 (RoB 2) for randomized control trials.
Risk of bias in non-randomized studies of interventions (ROBINS-I).
Summary of Grades of Recommendation, Assessment, Development, and Evaluation Certainty of Evidence.
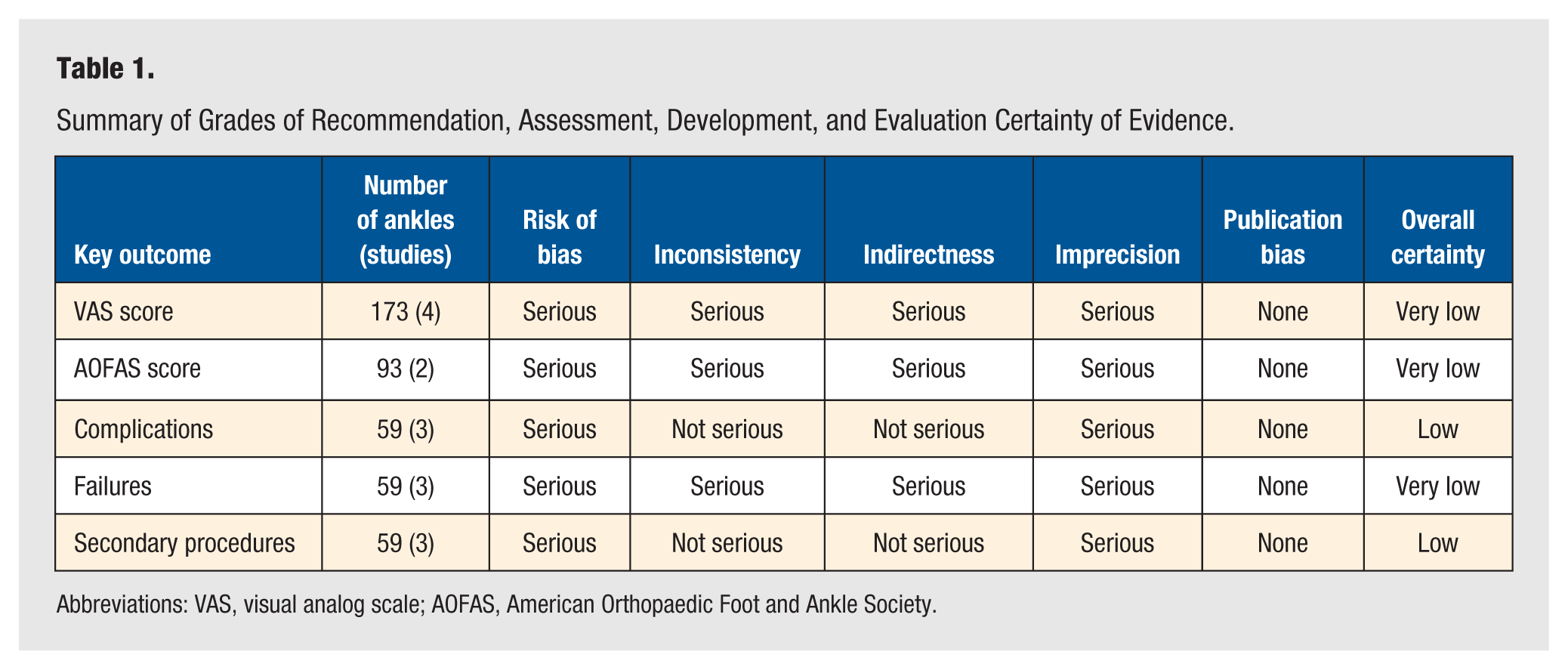
Abbreviations: VAS, visual analog scale; AOFAS, American Orthopaedic Foot and Ankle Society.
Data Extraction and Evaluation
Two reviewers independently extracted and assessed the data from each study. Data on patient demographics, including number of patients, number of ankles, laterality of injury, age, sex, body mass index (BMI), follow-up time, and grade of sprain were collected. Characteristics of the PRP injection preparation and administration were also collected. Clinical outcome scores, magnetic resonance imaging (MRI) outcome findings, complications, failures, and secondary procedures were also evaluated. For studies with multi-arm designs, intervention groups were extracted and reported separately for descriptive purposes. When multiple intervention arms shared a common control group, these comparisons were not considered statistically independent. Given the methodological and clinical heterogeneity across studies, including the presence of shared control groups in multi-arm designs, data were synthesized narratively without quantitative pooling.
Statistical Analysis
Statistical analyses were performed using RevMan software (version 5.4). Descriptive statistics were calculated for all continuous and categorical variables. Continuous variables were reported as weighted mean and estimated standard deviation, whereas categorical variables were reported as frequencies with percentages. A pooled meta-analysis could not be performed due to marked heterogeneity in the included studies, limited number of eligible comparative studies, and overall sample sizes, precluding meaningful statistical certainty with combined effect estimates.
Results
Study Characteristics and Patients Demographics
The search generated 539 studies. Following title and abstract screening, 14 full-text articles were assessed for eligibility. Nine studies were excluded due to study design limitations (review articles without original patient-level outcome data), inclusion of patients undergoing operative management of lateral ankle ligament injury, use of biologic therapies other than PRP, or cadaveric study design lacking clinical patient-level outcomes (Supplementary Table 1).
Of these, 5 met the inclusion and exclusion criteria (Figure 3). The 5 studies were published between 2015 and 2024. Study characteristics and patient demographics data are listed in Table 2. A total of 5 studies were included, of which 2 were LOE I,10,11 1 was LOE II, 12 1 was LOE IV, 13 and 1 was LOE V. 14 Four of the included studies evaluated patients with acute lateral ankle ligament injuries,10-12,14 and 1 study evaluated patients with chronic lateral ankle ligament injuries. 13 Control cohorts in this systematic review included patients who received a placebo injection 10 or no injection at all.11,12 Zhang et al 12 included 2 PRP intervention arms (single- and double-injection protocols) that shared a common control group. These PRP regimens were therefore described as separate intervention groups for descriptive purposes. However, because the control group was shared, these comparisons were not independent and were interpreted within a narrative framework rather than as separate comparative analyses.
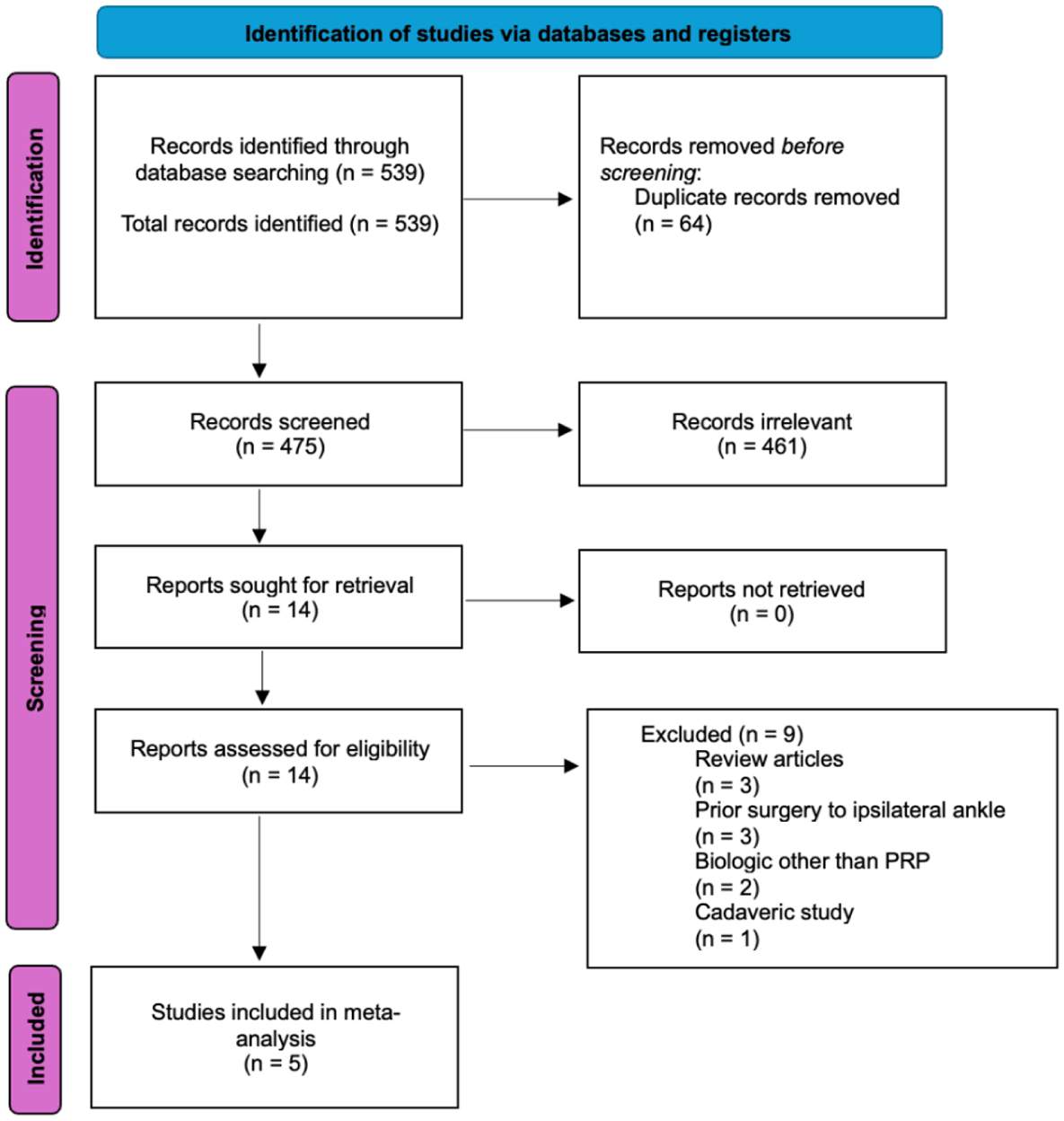
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) study selection flow diagram. Records were identified through database searching and screened for eligibility according to predefined inclusion and exclusion criteria. Of the 14 full-text articles assessed for eligibility, 9 were excluded due to study design limitations (review articles without original patient-level data), inclusion of patients undergoing operative management of lateral ankle ligament injury, use of biologic therapies other than platelet-rich plasma, or cadaveric study design. Detailed reasons for exclusion of full-text studies are provided in Supplementary Table 1.
Study Characteristics and Patient Demographics.
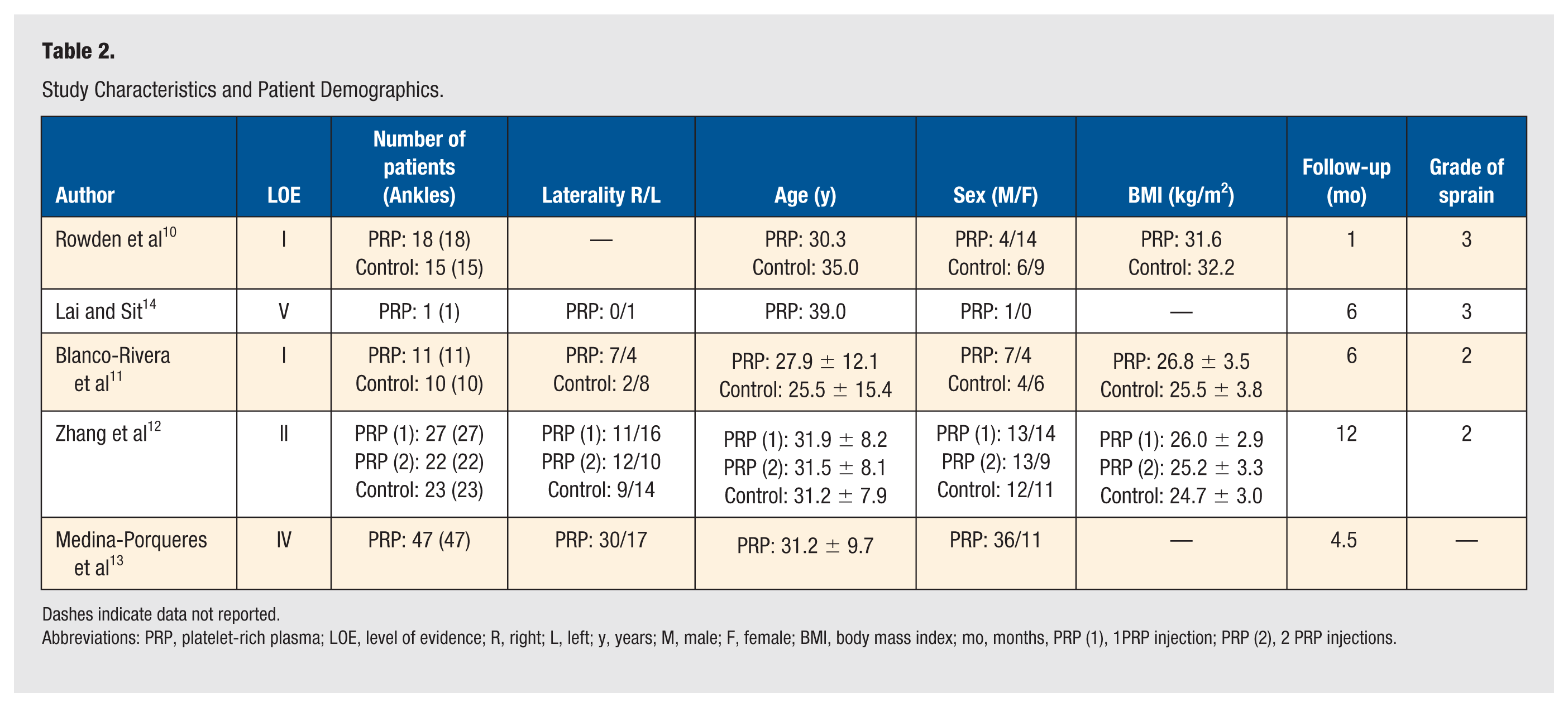
Dashes indicate data not reported.
Abbreviations: PRP, platelet-rich plasma; LOE, level of evidence; R, right; L, left; y, years; M, male; F, female; BMI, body mass index; mo, months, PRP (1), 1PRP injection; PRP (2), 2 PRP injections.
In total, there were 126 patients (126 ankles) who underwent PRP injection for lateral ankle ligament injuries and 48 patients (48 ankles) who did not receive PRP injection.10-14 Of the 4 studies that evaluated laterality on 126 ankles in the PRP cohort, 60 (55.6%) were right lateral ankle ligament injuries and 48 (44.4%) were left lateral ankle ligament injuries.11-14 Of the 2 studies that evaluated laterality on 33 ankles in the control cohort, 11 (33.3%) were right lateral ankle ligament injuries and 22 (66.7%) were left lateral ankle ligament injuries.11,12 The weighted mean age for the PRP cohort was 31.0 ± 1.9 years (range 27.9-39 years) and 31.2 ± 5.3 years (range 25.5-35.0 years) for the control cohort.10-14 There were 74 males (58.7%) and 52 females (41.3%) in the PRP cohort and 22 (45.8%) males and 26 (54.2%) females in the control cohort.10-14 The weighted mean BMI was 27.2 ± 0.3 kg/m2 (range 25.2-31.6 kg/m2) in the PRP cohort and 27.2 ± 0.6 kg/m2 (range 24.7-32.2 kg/m2) in the control cohort.10-12 The weighted mean post-injection follow-up time was 7.1 ± 4.3 months in both cohorts (range 1-12 months).10-14 Of the 4 studies that evaluated the grade of lateral ankle ligament injury, 75 patients had grade 2 sprains11,12 and 52 patients had grade 3 sprains in both cohorts.10,14
Platelet-Rich Plasma Injection Preparation Protocols, Procedures, and Techniques
Details regarding the preparation protocols, procedures, and techniques can be found in Table 3. Reporting of PRP preparation and administration characteristics was evaluated according to the adapted Minimum Information for Studies Evaluating Biologics in Orthopaedics (MIBO) 2017 guidelines, with adherence across studies summarized in Supplementary Table 2. All 5 included studies used between 30 and 50 mL of whole blood to prepare between 2 and 5 mL of PRP.10-14 Of these studies, only 1 protocol specifically used leukocyte-rich PRP. 10 Of the 3 studies that reported types of PRP kits utilized, 1 study used Magellan Autologous Platelet Separator Kit (Arteriocyte, Hopkinton, Massachusetts), 10 1 study used Harvest SmartPrep System (Harvest Technologies, Plymouth, Massachusetts), 14 and 1 study used WEGO PRP Kits (Wego Limited Company, China). 12 Three studies incorporated activators of PRP, including the use of calcium chloride or calcium gluconate.11,12,14 The revolutions per minute (rpm) and spin times during centrifugation ranged between 800 and 3200 rpm and between 3 and 10 minutes, respectively.11,12 Three studies utilized protocols with 1 centrifuge spin10,13,14 and 2 studies utilized protocols with 2 centrifuge spins.11,12
PRP Injection Preparation, Procedure, and Technique Characteristics.
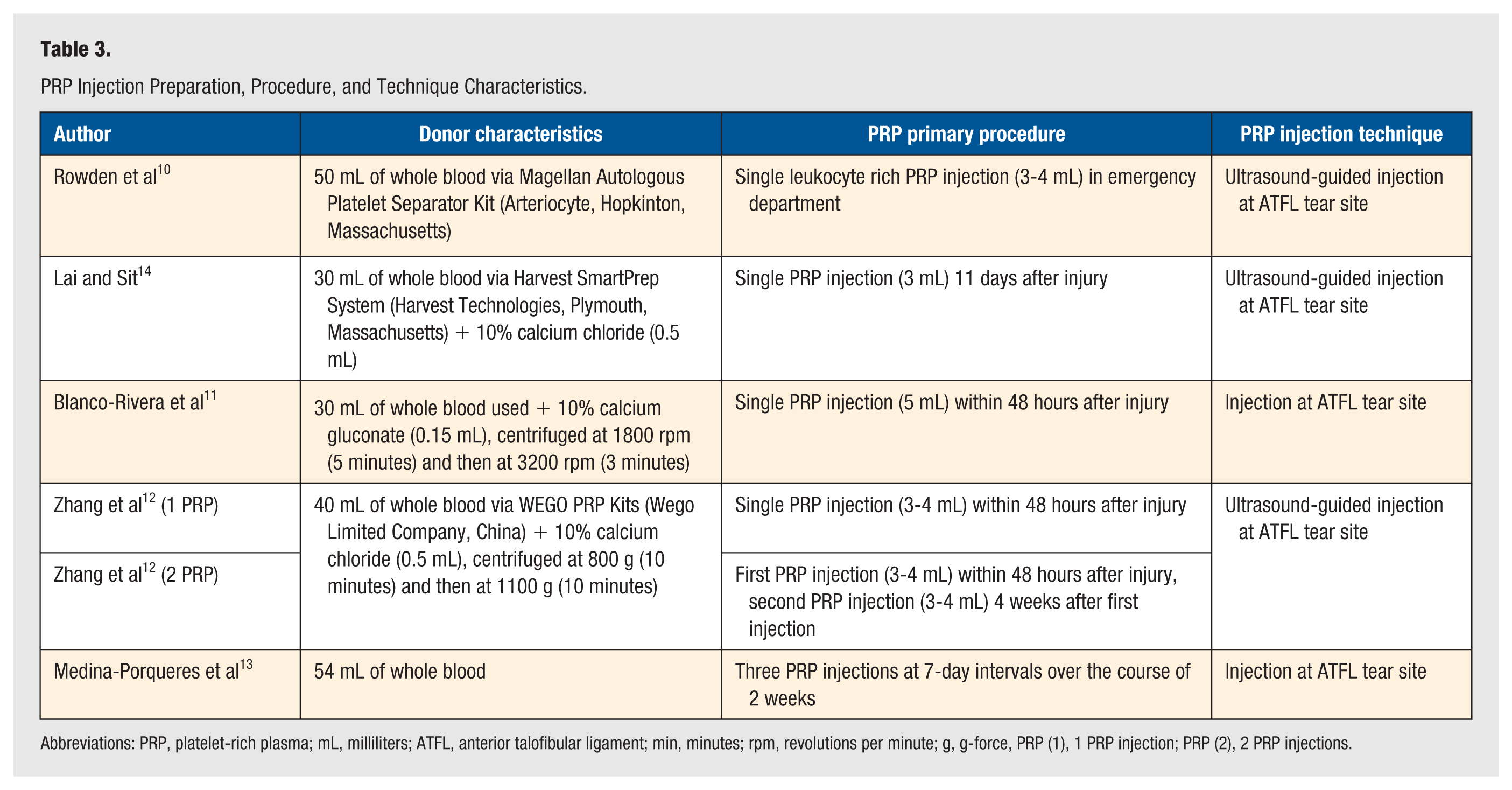
Abbreviations: PRP, platelet-rich plasma; mL, milliliters; ATFL, anterior talofibular ligament; min, minutes; rpm, revolutions per minute; g, g-force, PRP (1), 1 PRP injection; PRP (2), 2 PRP injections.
Three studies included patients with lateral ankle ligament injuries who received 1 PRP injection.10,11,14 For 2 of these studies, PRP injection was administered within 48 hours of the initial injury.10,11 For the third study, the PRP injection was administered 11 days after the initial injury. 14 One study included patients who received 3 PRP injections at 7-day intervals over the course of 2 weeks. 13 One study included 1 cohort of patients who received a single PRP injection and another cohort of patients who received 2 PRP injections. 12 In this study, patients received PRP injections within 48 hours of the initial injury. Three studies utilized ultrasound-guidance to inject PRP at the site of ATFL injury,10,12,14 while 2 studies injected PRP following the ATFL path under the lateral malleolus without imaging guidance.11,13
Clinical Outcomes
The clinical outcomes are summarized in Table 4. There were 6 different subjective scoring tools used among the included studies, including the visual analog scale (VAS), American Orthopaedic Foot and Ankle Society (AOFAS), lower extremity functional scale (LEFS), foot and ankle disability index (FADI), Karlsson score, and Cumberland Ankle Instability Tool (CAIT). The most commonly utilized patient-reported outcome measure was the VAS pain scores, applied in 4 of the included studies.10-13 For patients who underwent PRP injection, the weighted mean VAS score was 7.6 ± 0.6 (range 7.2-8.8) pre-injection and 0.6 ± 0.8 (range 0.1-1.9) post-injection.10-13 Overall, VAS improved 7 points for patients who received PRP injections. The weighted mean post-injection AOFAS score was 98.8 ± 0.6 (range 98.4-99.5) for the PRP cohort.11,12 One study reported LEFS, with a mean pre-injection score of 12.9 ± 9.5, improving to a mean post-injection score of 68.0 ± 9.1 for PRP patients. 10 One study reported FADI score of 135.4 ± 1.0 compared with a score of 122.0 ± 8.8 at 3 weeks of follow-up for PRP patients. 11 One study evaluated the Karlsson score, demonstrating a mean of 42.3 ± 14.9 prior to PRP injection and a mean of 96.5 ± 4.34 at final follow-up. 13 In addition, the authors utilized the CAIT and found an increase from pre-injection score of 10.3 ± 4.3 to 27.7 ± 1.7 at final follow-up. 13
Summary of Clinical Outcomes and Magnetic Resonance Imaging Outcome Findings.
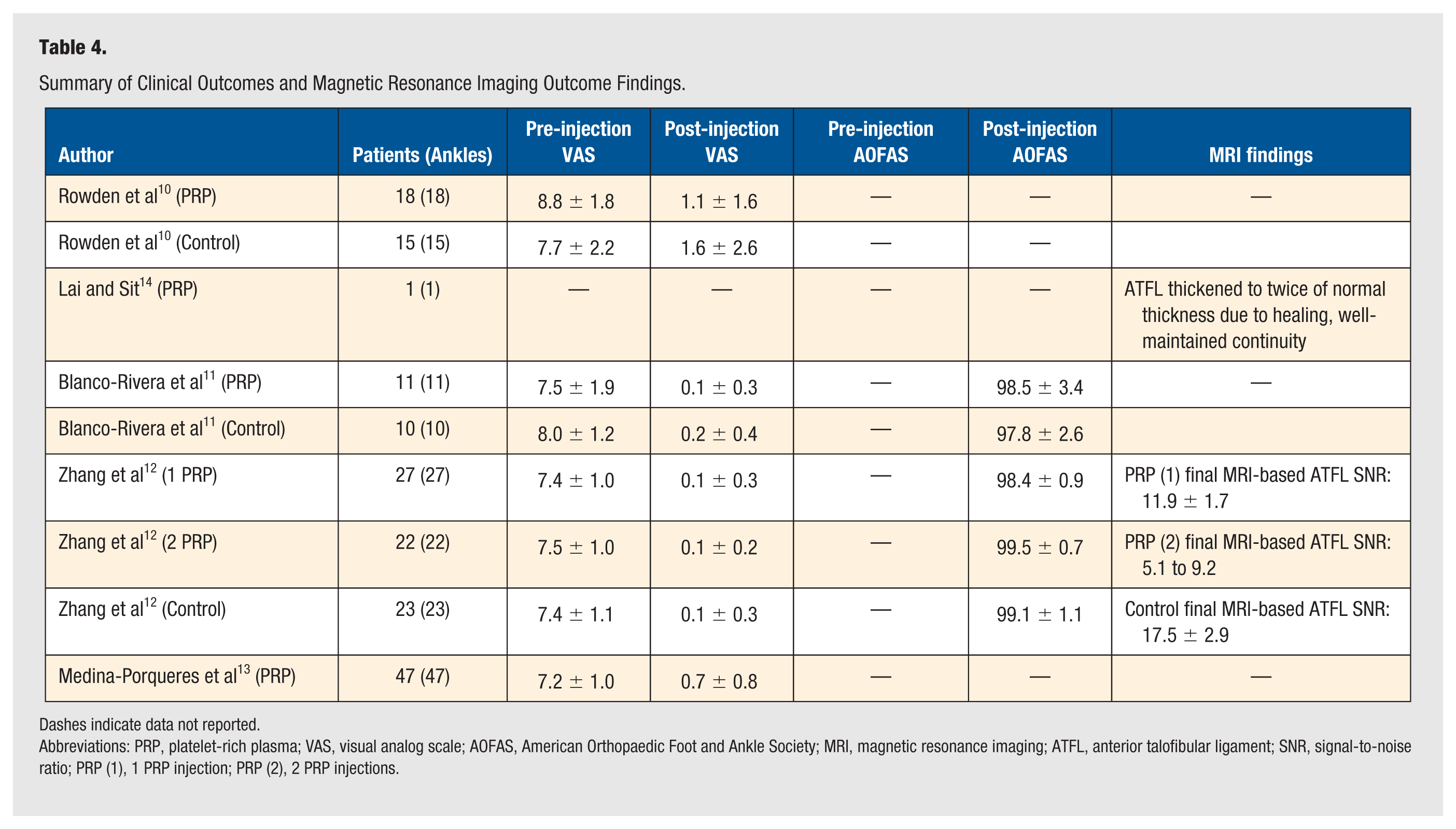
Dashes indicate data not reported.
Abbreviations: PRP, platelet-rich plasma; VAS, visual analog scale; AOFAS, American Orthopaedic Foot and Ankle Society; MRI, magnetic resonance imaging; ATFL, anterior talofibular ligament; SNR, signal-to-noise ratio; PRP (1), 1 PRP injection; PRP (2), 2 PRP injections.
For control patients, the weighted mean VAS score was 7.6 ± 0.6 (range 7.4-8.0) pre-injection and 0.6 ± 1.3 (range 0.1-1.6) post-injection.10-13 Overall, VAS improved 7 points for control patients. The weighted mean post-injection AOFAS score was 98.7 ± 1.1 (range 97.8-99.1) for the control cohort.11,12 One study reported LEFS, with a mean pre-injection score of 18.6 ± 12.2, improving to a mean post-injection score of 64.1 ± 14.0 for control patients. 10 One study reported FADI score of 135.3 ± 1.0 compared with a score of 117.1 ± 14.4 weeks of follow-up for control patients. 11
Magnetic Resonance Imaging Outcome Findings
The MRI outcome findings are summarized in Table 4. Two studies evaluated MRI outcome findings in patients who received PRP injections for lateral ankle ligament injuries. One study demonstrated that the ATFL thickened to twice of its normal thickness from the healing process after PRP injection. 14 For patients who received a single PRP injection, signal-to-noise ratio (SNR) values decreased from 28.4 ± 4.5 at 8 weeks following injection to 11.9 ± 1.7 at final follow-up. 12 Overall, SNR improved by 16.5 points for patients who received 1 PRP injection. For patients who received 2 PRP injections, SNR values decreased from 21.9 ± 5.1 at 8 weeks following injection to 9.2 ± 1.4 at final follow-up. 12 Overall, SNR improved by 12.7 points for patients who received 2 PRP injections. For patients who received no injection, SNR values decreased from 34.9 ± 5.5 at 8 weeks following injection to 17.5 ± 2.9 at final follow-up. 12 Overall, SNR improved by 17.4 points for patients who did not receive a PRP injection.
Return to Sport
Return to sport was recorded in 1 study, in which the authors demonstrated that 85.1% of patients returned to their preinjury physical activity levels by final follow-up. 13
Complications, Failures, and Secondary Procedures Following Platelet-Rich Plasma Injection
Data regarding complications, failures, and secondary procedures following PRP injection are listed in Table 5. Of the studies that reported complications for patients who underwent PRP injections, 2 (3.4%) patients reported transient dysesthesias that resolved 1 week after injection. 13 The same study reported 3 failures (5.1%) of the procedure. 13 None of the included studies recorded any secondary procedures required after patients received PRP injections for lateral ankle ligament injuries.11,13,14
Complications, Failures, and Secondary Procedures Following PRP Injection.
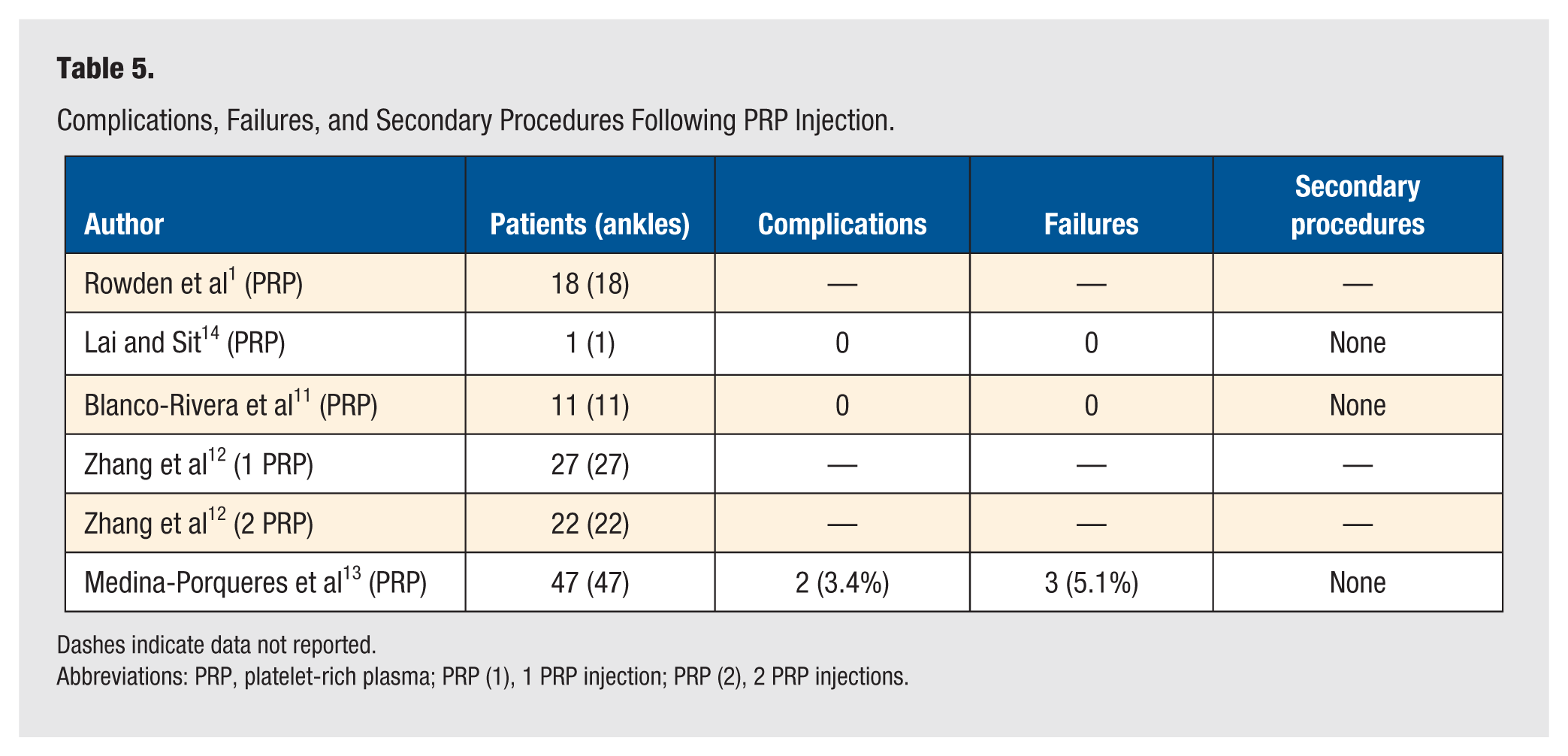
Dashes indicate data not reported.
Abbreviations: PRP, platelet-rich plasma; PRP (1), 1 PRP injection; PRP (2), 2 PRP injections.
Discussion
The main finding of this systematic review is that the currently available evidence is insufficient to determine whether PRP provides superior clinical outcomes compared with control treatments for lateral ankle ligament injuries at short-term follow-up. Overall, no consistent differences were observed in subjective clinical outcomes, complication rates, failure rates, and secondary procedure rates between the 2 cohorts. However, the significant heterogeneity in PRP preparation and administration protocols, the small sample sizes, and short-term follow-up of the included studies highlights that further, high-quality, adequately powered studies with long-term follow-up are warranted to determine the optimal role of PRP in the treatment of lateral ankle ligament injuries.
This systematic review found that while patients who received PRP for the treatment of lateral ankle ligament injuries demonstrated improvements in VAS and AOFAS scores, there seemed to be no difference in post-injection VAS or AOFAS scores between the PRP cohort and the control cohort. There are numerous reasons that account for the potential lack of significant benefit provided by the addition of PRP as a biological adjunct in the treatment of lateral ankle ligament injuries. First, the lateral ankle ligament complex is an extracapsular structure that receives a rich blood supply from the adjacent peroneal and anterior tibial arteries. 15 This facilitates the influx of local inflammatory cells, fibroblasts, and growth factors necessary for ligamentous tissue repair following injury. 16 As a result, approximately 90% of patients with ATFL injuries heal with conservative management alone due to this favorable biology, leaving little therapeutic margin for PRP to meaningfully improve outcomes. Another reason that may account for the potential lack of appreciable superiority in the PRP cohort is the short follow-up duration in the included studies in this review. Four of the 5 studies had follow-up times of 6 months or less, which may not be sufficient to capture the potentially superior clinical effects provided by PRP. Therefore, studies with longer follow-up periods may be necessary to detect clinically meaningful differences in outcomes following PRP treatment for lateral ankle ligament injuries.
This systematic review identified significant heterogeneity in the utilization of PRP across the included studies. Of the 5 included studies, only 1 study explicitly reported using leukocyte-rich PRP (LR-PRP). 10 LR-PRP contains higher concentrations of pro-inflammatory cytokines and white blood cells, which may enhance the early inflammatory phase of healing, particularly beneficial in ligament injuries where initial inflammation drives tissue repair. 17 Figueiredo et al evaluated the effect of LR-PRP on experimentally induced suspensory ligament injuries in an equine model. The LR-PRP-treated limbs demonstrated reduced lesion intensity, improved echogenicity, increased neovascularity, and higher type I collagen content, suggesting enhanced ligament repair compared with controls. 18 Conversely, leukocyte-poor PRP (LP-PRP), which may have been utilized in the remaining 4 studies included in this review, could have limited the biologic activity needed to stimulate a robust healing response, potentially contributing to the lack of significant clinical differences observed in this study. Such a lack of uniformity in reporting mirrors trends in the broader PRP literature, where Chahla et al 19 showed that poor and inconsistent documentation of PRP composition, such as leukocyte content, complicates interpretation and comparability across studies.
Furthermore, there was significant heterogeneity in the PRP preparation protocols across the studies included in this review, which may have impacted the composition and ultimate quality of the PRP delivered to patients. First, there was a significant discrepancy in the centrifugation spin rates utilized across the included studies, ranging from 800 to 3500 rpm. Higher centrifugation spin rates have been demonstrated to significantly alter the composition of PRP. Sabarish et al 20 previously studied 3 different protocols for spin rates and found that lower spin rates (closer to 800 rpm) had greater yield of platelets, concluding that higher spin rates (closer to 3600 rpm) could cause platelet aggregation and disintegration, thus potentially producing an inferior product. In this review, as several included studies used high centrifugation spin rates or failed to report their spin rates entirely, the resulting variability in platelet yield and suboptimal PRP formulations may have contributed to inconsistent clinical responses. In addition to the variable spin rates among the included studies, there were discrepancies in the number of spins across the different protocols, with 3 studies utilizing a single-spin centrifugation protocol10,13,14 and 2 studies utilized a double-spin centrifugation protocol.11,12 Saqlain et al 21 demonstrated that a double spin centrifugation protocol resulted in higher platelet counts and lower levels of undesired red and white blood cells compared with a single-spin centrifugation protocol. The variation of spin protocols for studies included in the current review may have affected platelet viability and quality, potentially diminishing the therapeutic effectiveness of PRP. In addition, 3 different commercial centrifugation kits were utilized across the included studies in this review.10,12,14 Jildeh et al 22 demonstrated wide variability among PRP kits, with platelet concentrations ranging from 2.7-fold to over 5-fold above baseline, potentially contributing to the potential lack of significant benefit identified in the PRP cohort. Similarly, the 3 different PRP systems used across included studies in the current review likely produced formulations with varying platelet concentration, which may have further contributed to the inconsistent findings. Importantly, the heterogeneity observed across studies is not merely statistical, but fundamentally clinical and biological. Platelet-rich plasma cannot be considered a single, uniform intervention. Substantial variability exists in PRP composition (leukocyte content, platelet concentration), preparation protocols, dosing regimens, timing of administration, and injury chronicity. These factors fundamentally limit cross-study comparability, independent of statistical heterogeneity metrics such as I 2 , and preclude meaningful quantitative synthesis.
The considerable heterogeneity in PRP preparation protocols and delivery, as highlighted in this systematic review, is consistent with the available literature on ligament injuries. 23 Despite recent efforts to standardize reporting of key factors related to PRP, such as the development of the MIBO guidelines in 2017, Butler et al 24 and Hedbany et al 25 found that the majority of studies reporting outcomes following the use of PRP for musculoskeletal pathologies fail to adhere to these standards, thereby limiting comparability and reproducibility. Non-adherence to MIBO reporting criteria represents a primary source of irreducible methodological heterogeneity, fundamentally limiting the interpretation of PRP efficacy in the included studies. To enable robust cross-sectional analyses, future research must rigorously follow standardized frameworks, such as the MIBO criteria, to ensure consistent reporting of PRP preparation and administration protocols to be able to draw definitive conclusions regarding PRP’s efficacy in treating lateral ankle ligament injuries.
Previous systematic reviews have evaluated PRP injections for ankle sprains with similarly limited and heterogeneous evidence. Banerjee et al 8 reported short-term improvements in pain and functional outcomes, but performed a pooled meta-analysis despite substantial variability in PRP preparation, dosing, and timing across included studies. Similarly, a systematic review by Milo and Braganza 7 suggested potential benefits in pain reduction and early return to play following PRP injections, but included both lateral and syndesmotic injuries, relied on a small number of studies, and did not adequately account for key sources of methodological and biological heterogeneity. While these studies offered preliminary insight, the current systematic review addresses key limitations and provides a more focused and methodologically rigorous evaluation of outcomes following PRP injections for lateral ankle ligament injuries. First, we include the study conducted by Medina-Porqueres et al 13 one of the few investigations providing a multi-injection PRP protocol with detailed clinical outcomes. Banerjee et al failed to include this study, thereby omitting important data that contribute to the current evidence. Second, both prior reviews included studies evaluating PRP for syndesmotic (high-ankle) injuries. High-ankle sprains (anterior inferior tibiofibular ligament tears) are a fundamentally different pathology from lateral ankle sprains (ATFL tears), with different mechanisms of injury, symptom patterns, and usual treatment protocols.26-29 Therefore, combining syndesmotic injuries with lateral ankle sprains introduces substantial clinical heterogeneity and further limits the validity of any pooled conclusions the authors performed. The current review incorporates all eligible PRP studies for lateral ankle ligament injuries, applies stricter inclusion criteria by excluding syndesmotic injuries, and clearly outlines the methodological limitations across studies that prevent a meta analysis from being performed with meaningful statistical certainty. Notably, several ongoing and registered RCTs evaluating PRP for lateral ankle ligament injuries have been identified. While the current body of published evidence remains limited, these high-quality studies will add to the existing data and help more clearly define the clinical role of PRP in lateral ankle ligament injury management.
Several limitations exist in this systematic review, and therefore the findings should be interpreted with caution. First, the overall sample size across included studies was small, with only 3 comparative cohorts available, limiting the strength and generalizability of the findings. Second, an important limitation of the current evidence base is that a substantial proportion of the comparative data derives from a single multi-arm study with a shared control group. While this design allows exploration of different PRP dosing strategies, the lack of independence between intervention arms limits the strength of comparative inferences and effectively reduces the amount of independent evidence available. This factor further contributes to the low certainty of evidence and supports cautious interpretation of the findings. Third, the included studies demonstrated substantial methodological heterogeneity, including differences in PRP preparation protocols, number and timing of injections, and variability in injury chronicity. Fourth, heterogeneity also existed among outcome measures utilized and follow-up times of the included studies, further preventing the valid pooling of effect sizes and a meta-analysis to be performed. Therefore, a narrative synthesis was required to avoid generating unreliable or misleading statistical estimates. Fifth, this review was not prospectively registered via PROSPERO, and a complete PRISMA-S search appendix detailing database-specific queries was not provided, which may limit methodological transparency and reproducibility. Finally, studies published in databases other than PubMed, EMBASE, or Cochrane, as well as those identified through trial registries and gray literature sources, are not represented in this systematic review.
Conclusion
Based on limited short-term data, the available studies do not demonstrate a clear or consistent difference in clinical outcomes between PRP-treated patients and controls. However, the evidence base is scarce, highly heterogeneous, and of low certainty. Substantial variability in PRP preparation and administration, small sample sizes, and short follow-up preclude reliable quantitative synthesis and comparative conclusions. Consequently, the current literature is insufficient to determine whether PRP provides any clinical advantage over standard care for lateral ankle ligament injuries. Further well-designed, adequately powered prospective studies with standardized PRP protocols and longer follow-up are warranted.
Supplemental Material
sj-docx-1-fas-10.1177_19386400261458588 – Supplemental material for Platelet-Rich Plasma for Lateral Ankle Ligament Injuries: A Systematic Review of Current Evidence and Limitations
Supplemental material, sj-docx-1-fas-10.1177_19386400261458588 for Platelet-Rich Plasma for Lateral Ankle Ligament Injuries: A Systematic Review of Current Evidence and Limitations by Jared Rubin, Ryan Rutherford, Alexander Tham, James J. Butler, Edward S. Mojica, Cameron Pow, Haider Ali Lakadawala and John G. Kennedy in Foot & Ankle Specialist
Footnotes
Acknowledgements
None.
Author Contributions
All of the authors (Jared Rubin, Ryan Rutherford, Alexander Tham, James J. Butler, Edward S. Mojica, Cameron Pow, Haider Ali Lakdawala, and John G. Kennedy) contributed to this publication and meet the criteria as defined by ICJME:
1. Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work.
2. Drafting the work or revising it critically for important intellectual content.
3. Final approval of the version to be published.
4. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr John Kennedy is a consultant for Arthrex and In2Bones. Dr John Kennedy receives research funding from Mr Winston Fisher, Ms Tatiana Rybak, and the Ohnell Family Foundation. Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. The authors report no other conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Ethics Approval Statement
No ethical approval was required for this study.
Patient Consent Statement
No patient consent was required for this study.
Data Availability Statement
Data for this study were sourced from articles identified on publicly accessible databases including PubMed, EMBASE, and Cochrane.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.