
Abstract
Background
Bone grafting is a commonly used adjunct in foot and ankle surgery to enhance osseous healing in fracture fixation and arthrodesis. Although autologous corticocancellous bone is commonly used, donor site morbidity and limited graft availability have driven the development of allogenic alternatives such as demineralized bone matrix (DBM).
Formulations
Demineralized bone matrix is produced through decalcification of donor bone, preserving a collagen-rich scaffold and biologically active proteins that support osteoconduction and osteoinduction. Commercial formulations vary in carrier systems, structural properties, and quality control processes. Products such as DBX (DePuy Synthes/MTF Biologics) and AlloSync (Arthrex) incorporate lot-specific osteoinductivity testing, whereas others including AlloMatrix (Stryker), OrthoBlast II (SeaSpine/Orthofix), and Grafton (Medtronic) use carriers to improve handling. Carrier-free and structural grafts, as well as injectable systems, further expand available options.
Clinical Applications
The strongest clinical evidence for DBM exists in fracture fixation, where high union rates have been consistently reported. In arthrodesis procedures, DBM demonstrates union rates comparable to autograft, though without evidence of superiority. Applications in osteochondral lesions of the talus and hallux valgus correction remain less clearly defined, with variable outcomes reported in predominantly small case series. Limited evidence also suggests a potential role in calcaneal bone cysts.
Conclusion
Demineralized bone matrix is a safe and versatile adjunct that avoids donor site morbidity and provides favorable handling characteristics. However, the current literature is dominated by level III-IV evidence, with no high-quality comparative studies demonstrating superiority over autograft. Demineralized bone matrix is best used in fracture fixation and selective arthrodesis, while further studies are required to define its role in cartilage-related and forefoot procedures.
Keywords
Introduction
“Demineralized bone matrix has also shown potential in the treatment of calcaneal bone cysts, although this is based on limited case series.”
Bone grafting is a common adjunct in foot and ankle surgery and is most often used to enhance osseous healing in fusion procedures and displaced fractures. 1 The benchmark source for graft material remains autologous corticocancellous bone, usually obtained from the ipsilateral iliac crest. 1 Its appeal lies in the combination of osteoconductive scaffolding, osteoinductive signaling, and limited osteogenic potential. However, autograft harvest is associated with substantial donor site complications in 8% to 39% of cases 2 and variable quantity of viable graft material, prompting the development of allogenic substitutes.
Demineralized bone matrix (DBM) is one such substitute. Following decalcification and sterilization of donor bone, DBM retains its collagenous scaffold with osteoconductive properties and bone morphogenic proteins (BMPs) with osteogenic potential.3-5 Demineralized bone matrix has become increasingly widespread in orthopaedic practice aided by regulatory environments that facilitate rapid release of new formulations. 3
Within foot and ankle surgery, DBM has been incorporated into procedures including ankle arthrodesis, hindfoot and midfoot fusions, and fracture fixation. This narrative review summarizes available clinical evidence on DBM in foot and ankle surgery, with studies organized by clinical indication and interpreted in the context of level of evidence.
Mechanism of Action and Biological Basis
Demineralized bone matrix is derived from allogenic bone that has undergone acid decalcification, which removes the mineral content while preserving the collagen-rich extracellular matrix and noncollagenous proteins. This preparation retains key bioactive molecules, such as BMPs, transforming growth factor β (TGF-β), and insulin-like growth factor (IGF-1).3,6,7 Demineralized bone matrix supports bone repair through 3 complementary mechanisms: (1) osteoconduction by providing a collagen scaffold that allows vascular and cellular ingrowth 3 ; (2) osteoinduction, via retained signaling proteins such as BMPs, TGF-β, and IGF-1 that promote mesenchymal stem cell differentiation into bone-forming cells4,7 and a limited osteogenic potential, as DBM contains no viable cells. This limitation can be offset by combining DBM with autologous bone marrow aspirate (BMA) or other cellular sources, which provide osteogenic cells to complement its inductive and conductive properties.8,9
Clinical performance can depend on the carrier system. Additives such as sodium hyaluronate (HA), calcium sulfate, or reverse-phase mediums influence injectability, cohesion, and protein release. 6 Carrier-free formulations such as cancellous sponges or fiber-based matrices rely on the graft’s structure alone, but can be augmented with autologous biologics such as BMA8,9 or allogenic growth factors. 10
Finally, the osteoinductive potential of DBM varies significantly between products, likely owing to differences in donor tissue, decalcification methods, sterilization, and carrier composition. 11 These biologic and handling differences form the basis for the range of DBM formulations now in use (Table 1).
Clinical Applications of Demineralized Bone Matrix in Foot and Ankle Surgery.
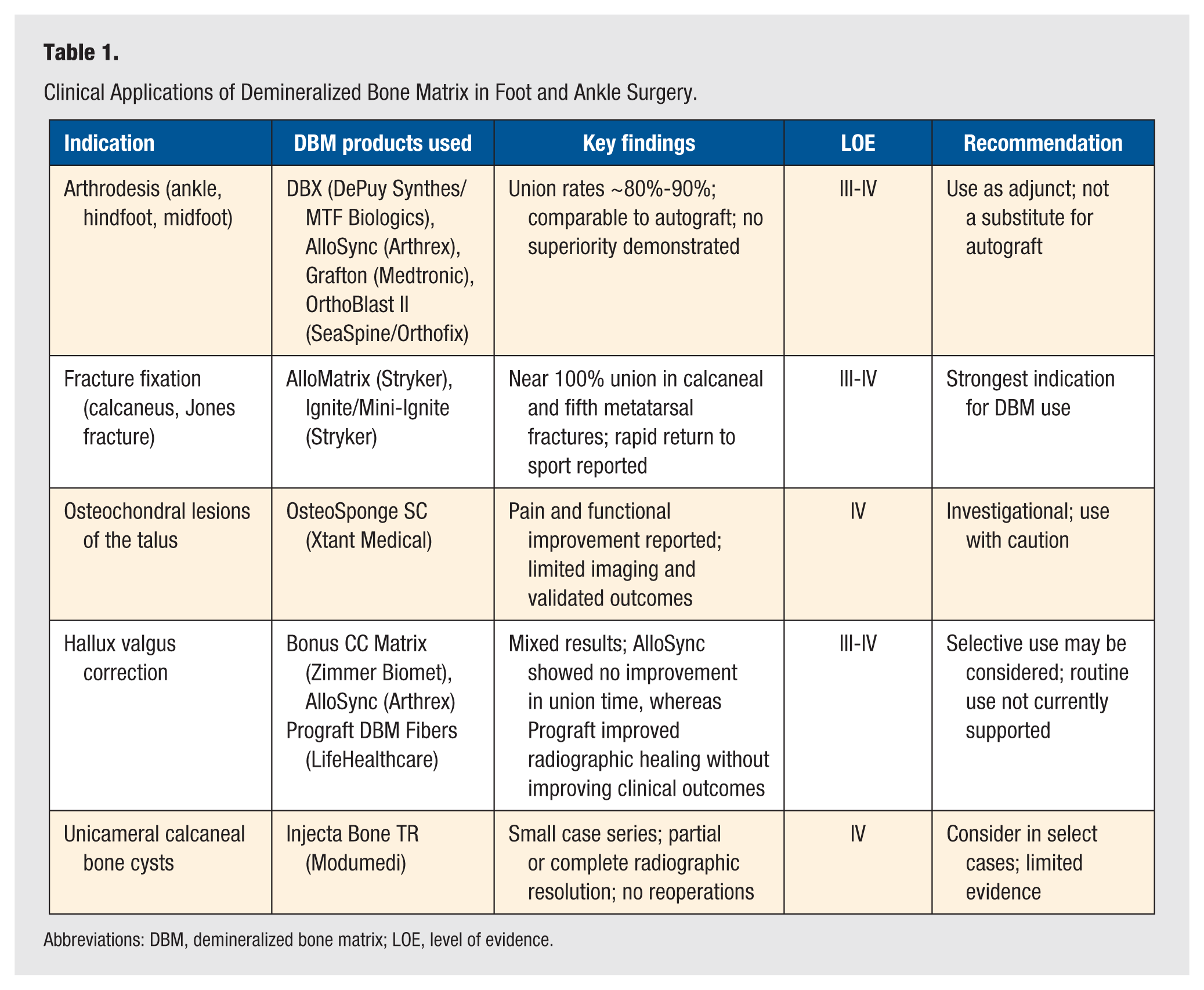
Abbreviations: DBM, demineralized bone matrix; LOE, level of evidence.
Overview of Commercial DBM Products
Commercial DBM formulations vary in composition, carrier systems, and quality control processes, as summarized in Table 1. Products with lot-specific osteoinductivity testing include DBX (DePuy Synthes/MTF Biologics) and AlloSync (Arthrex). DBX incorporates DBM with a sodium HA carrier and is available as putty, strips, or injectable paste. AlloSync is available in multiple formats, ranging from carrier-free DBM (AlloSync Pure) to putty, paste, and gel formulations with a poloxamer reverse-phase medium carrier, as well as structural wedges, darts, and cortical fibers. Both products are distinguished by batch-specific osteoinductivity testing to improve consistency in biologic performance.
Products using cohesive carriers include AlloMatrix (Stryker), OrthoBlast II (SeaSpine/Orthofix), and Grafton (Medtronic). AlloMatrix combines DBM with calcium sulfate to create a biocomposite that hardens in situ and resists irrigation washout. OrthoBlast II incorporates DBM with cancellous chips in a reverse-phase medium to enhance cohesion and handling, and Grafton is available as putty, paste, and a carrier-free injectable fiber formulation.
Carrier-free or structural DBMs include OsteoSponge SC (Xtant Medical), Bonus CC Matrix, and Triad (Zimmer Biomet). OsteoSponge SC is made of demineralized cancellous scaffolds or preformed plugs designed for subchondral defects, such as in osteochondral lesions.12,13 Bonus CC Matrix incorporates mineralized cancellous chips, and Triad includes cryopreserved viable cells.
Injectable DBM formulations include Injecta Bone TR (Modumedi) and the Ignite systems (Stryker). The Ignite and Mini-Ignite are designed to be used in combination with BMA at the time of surgery, providing an osteogenic cell source in addition to the DBM scaffold.
Emerging nonstructural allograft formulations, such as AlloStat GFx (TheraMicro), aim to enhance osteoinductive and biologic signaling through preservation of growth factors and extracellular matrix components, such as from the BMP and TGF families. However, clinical evidence in foot and ankle surgery remains limited.
Clinical Applications
Arthrodesis of the Ankle, Hindfoot, and Midfoot
Demineralized bone matrix has been widely incorporated into fusion procedures. Pooled reported union rates across studies average 85%.9,14-17 Products that can be used in this setting include DBX (DePuy Synthes/MTF Biologics), 15 AlloSync Pure (Arthrex), 16 Grafton (Medtronic), 9 and OrthoBlast II (SeaSpine/Orthofix). 17 No comparative studies have been performed assessing graft performance relative to each other. Tricot et al 9 found similar nonunion rates between autograft/DBM (18%) compared with allograft/DBM with concentrate BMA (13%) in hindfoot and ankle arthrodesis. Sherman et al 8 reported high fusion rates in tibiotalocalcaneal arthrodesis augmented with DBM, concentrated BMA, and structural allograft (92.9%) and recent computed tomography (CT) evaluation of hindfoot fusions using AlloSync Pure demonstrated fusion rates between 80% and 100% across various fixation constructs. 16 The available evidence is predominantly level III-IV, and DBM should be considered an adjunct rather than a substitute for autograft in routine arthrodesis.
Fracture Fixation
The evidence for DBM appears to be strongest in acute fracture management. In calcaneal fractures, AlloMatrix (Stryker) has shown to achieve 100% union, with superficial wound complications in 15% of cases. 18 For Jones fractures of the fifth metatarsal, the Ignite (Stryker) injectable systems paired with BMA reported 100% union, including in elite athletes,19,20 with a return to play of less than 10 weeks. 20 This represents the strongest clinical indication for DBM use in foot and ankle surgery, although evidence remains limited to level III and IV studies.
Osteochondral Lesions of the Talus
Cystic osteochondral lesions of the talus (OLTs) have been treated with DBM plugs and scaffolds. OsteoSponge SC (Xtant Medical) provides presized plugs for subchondral voids, and demonstrated significant reductions in pain (visual analogue scale [VAS] 7.6 ± 0.9 to 0.4 ± 0.6, P = .01) and function (VAS 7.3 ± 1.0 to 0.2 ± 0.8) scores; however, most reports lacked validated outcome measures or advanced imaging to confirm tissue restoration.12,13 Given the predominance of small case series (level IV), the use of DBM in OLTs remains investigational.
Hallux Valgus Correction
In hallux valgus corrections surgery, 3 different products were reported. Bonus DBM (Zimmer Biomet) was used in proximal medial opening wedge osteotomies for hallux valgus correction, where osteotomy healing was achieved, but deformity recurrence occurred in 65% of cases. 21 AlloSync DBM (Arthrex) was recently studied in minimally invasive surgery for hallux valgus correction and showed that while union was achieved in all cases, the addition of the graft did not shorten time to union compared with controls (5.69 ± 3.16 months vs 6.0 ± 3.95 months, P = .731). 22 More recently, Prograft DBM Fibers (LifHealthcare) were evaluated in a retrospective comparative study of minimally invasive hallux valgus surgery comprising 316 feet, and were associated with improved radiographic healing and remodeling, although no clinically meaningful differences were observed in patient-reported outcome measures, deformity correction, or complication rates. 23 Collectively, these level III-IV studies suggest that DBM may enhance radiographic osteotomy healing in minimally invasive hallux valgus surgery; however, consistent improvements in clinical outcomes have not been demonstrated. Routine use therefore cannot currently be recommended, although selective use may be considered in patients where enhanced osteotomy healing is desired.”
Unicameral Bone Cysts
Injecta Bone TR (Modumedi, Korea) was used for unicameral calcaneal bone cysts in 10 cases at 34-month follow-up. No perioperative patient-reported outcome measures were reported. Two cases (25%) had painless persistent cystic defects postsurgery, with no secondary surgical procedures reported. 24 These findings are based on limited level IV evidence, and DBM may be considered in select cases, though data remain sparse.
Conclusion
Demineralized bone matrix is a widely used biologic adjunct in foot and ankle surgery that avoids donor site morbidity and offers favorable handling characteristics. The most consistent clinical benefit is observed in fracture fixation, where high union rates have been reported in both calcaneal and fifth metatarsal injuries. In arthrodesis procedures, DBM demonstrates union rates comparable to autograft; however, no studies have shown superiority, and it should therefore be considered an adjunct rather than a replacement, particularly in cases with limited graft availability or compromised biology.
In contrast, the role of DBM in OLT and hallux valgus correction remains less clearly defined, with variable outcomes reported in small, heterogeneous studies. Current evidence does not support routine use in these settings. Demineralized bone matrix has also shown potential in the treatment of calcaneal bone cysts, although this is based on limited case series.
Importantly, the available literature across all indications is dominated by level III-IV evidence, with no high-quality comparative trials demonstrating superiority over autograft or other grafting strategies. In addition, no individual DBM product has demonstrated superior clinical performance relative to others. Based on the current evidence, DBM is best used as an adjunct in fracture fixation and selective arthrodesis, while its use in cartilage-related and forefoot procedures should be approached with caution. Further high-quality comparative studies are required to define its optimal role and guide product selection in foot and ankle surgery
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.