
Abstract
The aim of this article was to identify the perceptions of community-based organization (CBO) service providers regarding their experiences with Black women living with AIDS (BWLHA) during a global pandemic. Two CBO service providers were selected for the study through a purposeful sampling technique. Black feminist theory, informal learning, and trauma theory helped frame the study, and narrative and cultural analyses were used for data analysis. Social isolation, medical and telehealth concerns, perceived social categorization of us and them, and informal strategies for healing were the emerging themes. Findings from this study have implications for adult educators, health educators, and mental health professionals as the global COVID-19 pandemic has increased the need to develop a trauma care plan (TCP) for BWLHA.
Justice and equity are not established for Black women many times. There is also structural inequity within the healthcare system, making it difficult for Black women to receive the proper care and treatment. Black women have experienced intergenerational trauma because of the lack of concern for Black women. It is even worse for Black women living with HIV.
According to the Kaiser Family Foundation (2019), 1 in 941 White women and an alarming 1 in 54 Black women in the United States are living with a human immunodeficiency virus (HIV) diagnosis (See Appendix A for word abbreviations). As of 2021, Black women accounted for almost 60% of the newly diagnosed cases of HIV in the United States (Ojikutu & Mayer, 2021), whereas White and Latino women accounted for only 20 and 16%, respectively. Despite the increased prevalence of HIV/AIDS among Black women, these diagnoses continue to be associated with homosexuality, which impedes opportunities for healing justice work for BWLHA and further increases the marginalization of this population. Baumgartner and Niemi (2013) indicated Black women living with a chronic illness like HIV contemplate the impact of the illness. Threats posed by the coronavirus (COVID-19) for individuals who are immunocompromised led to a heightened awareness of their HIV status during the pandemic.
In early 2020, COVID-19 emerged with such intensity that it caused a global pandemic and claimed the lives of millions of people within the United States and globally (Centers for Disease Control and Prevention [CDC], 2022). In response to this global pandemic and to advance public health goals, shelter-in-place mandates were implemented, which required community-based organizations (CBOs) to alter the way in which they serviced their clients to avoid the further spread of the virus (Pinto & Park, 2020). The workforce of CBOs typically comprises social workers, case managers, navigators, and health educators. CBO service providers are considered adult educators as they offer formal, informal, and nonformal learning across the lifespan (Gailbraith, 1995). This abrupt change posed many challenges for people living with HIV/AIDS (PLWHA), particularly Black women. Therefore, the aim of this article was to identify the perceptions of CBO service providers regarding their experiences with BWLHA treatment and care during a global pandemic. There are a few reasons why this topic beckoned exploration.
First, the effect of stigma on Black women’s treatment and care has been well documented in the literature (Sangaramoorthy et al., 2017; Whiteside et al., 2014). There is also a significant amount of literature on Black women’s risk for HIV (Davis & Tucker-Brown, 2013). Last, there is a dearth of literature on the impact of the pandemic on HIV/AIDS efforts, the health and well-being of BWLHA, and the resulting trauma experienced by BWLHA. These gaps were discovered when beginning to research care efforts for BWLHA. Therefore, this study was designed to answer the following research questions: What impact has the global pandemic had on the health and well-being of BWLHA? What impact has the global pandemic had on CBO service providers’ treatment and care of BWLHA? What healing justice strategies guided by informal learning do CBO service providers offer?
Conceptual and Contextual Framing
Black feminist theory (BFT), informal learning theory, and trauma theory were used to frame the study. BFT offers a constructive lens to contextualize the intersecting sociocultural and interpersonal oppressive experiences and ideas of BWLHA shared from the perspectives of CBO service providers (Collins, 1990). Central to BFT is intersectionality, which is an analytic tool for exploring multiple intersecting oppressions such as race, class, gender, sexual orientation, ability status, and sometimes ageism that create unique lived experiences for the individuals and groups occupying these different identity characteristics (Collins & Bilge, 2020). BFT research expands the conversation by highlighting unique challenges as well as opportunities for empowerment for BWLHA. Informal learning is another lens used to inform the teaching and learning experiences of BWLHA in a social context (Merriam et al., 2007). Informal learning research expands the conversation to include BWLHA and how they learn to live with rather than die from a chronic illness, especially during times of uncertainty such as a global pandemic. Trauma is a disruptive experience that severely affects an individual’s emotional organization, which, in turn, can influence how they perceive the world. Trauma theory was used to frame the research and support the exploration of the traumatic experiences of BWLHA during a global pandemic and to learn to develop a care plan to address trauma for self-care. Several bodies of literature situated the study.
David Williams, a germinal health disparities scholar, has called attention to the health disparities for African Americans. Williams (2012) lamented that the patterning of racial disparities is due largely to the racism existing in individuals and, in a larger context, institutions. There is a growing body of evidence to support that unconscious and unintentional bias are significant drivers of these inequities, leading to differences in treatment and care across multiple domains (Sacks, 2018; Torres et al., 2019; Williams & Cooper, 2019). For Black women, their illness is likely to go undiagnosed, untreated, or not taken seriously due to misperceptions of hypochondria or possessing an addictive personality (Hoffman et al., 2016; Onos, 2020; Washington & Randall, 2022). Studies have revealed that Black women, whether low-income (e.g., Gonzalez et al., 2021) or unburdened by poverty (Sacks, 2018), experience discrimination or unfair judgment by healthcare providers or staff members. Beliefs about Black bodies (e.g., strong resistance to pain) have informed how healthcare professionals make medical judgments about African Americans (Hoffman et al., 2016). In some studies, scholars found that when Black women experienced chronic pain, they felt the severity of their pain was not being acknowledged, or they were being completely ignored by medical professionals, causing medical mistrust among the participants (e.g., Hoffman et al., 2016; Washington & Randall, 2022). Some argue that though there have been some improvements in Black women’s health, disparities remain pervasive (Braveman et al., 2011; Prather et al., 2018). Moreover, the intersecting structural identities of racism, sexism, classism, and sometimes ageism have contributed to increased rates of chronic illness (e.g., HIV/AIDS) among Black women.
In addition to the structural inequities Black women experience, BWLHA face intersectional stigma (Watkins-Hayes et al., 2012). The stigma associated with such a chronic illness implies that Black women are linked to substance abuse, are burdened by poverty, and have multiple sex partners, tarnishing the Black community’s reputation (Rice et al., 2018). Internalized stigma and provider assumptions can disrupt treatment and care, medication adherence, and engagement in the care continuum, which can lead to long-term health outcomes for BWLHA (Sangaramoorthy et al., 2017). Watkins-Hayes et al. (2012) indicated a correlation between marginalization of HIV status, structural inequities, and stress among BWLHA.
Though Black and White women experience psychological distress (e.g., anxiety and depression) associated with managing a chronic health disease like HIV/AIDS, BWLHA are more vulnerable to adverse health outcomes due to intersectional stigma. In other research, White women living with HIV/AIDS were more likely to talk about their feelings (Fletcher, 2016), model resilience (Fletcher et al., 2020), and engage in physical activity as methods for coping with HIV-related illnesses. However, BWLHA engaged in less self-blaming, practiced resilience, and viewed faith- or religious-based engagements as tangible coping strategies. Although the research indicates BWLHA have developed coping mechanisms, the unprecedented COVID-19 forced BWLHA to ponder their HIV diagnoses more intensely.
In one study, Hall et al. (2021) discovered that BWLHA experienced heightened fears of contracting COVID-19 due to immunosuppression when compared to other people living with HIV. Given the historical maltreatment and care among BWLHA, COVID-19 exacerbated the issues. BWLHA were less likely to seek medical care for COVID-19 (Williams, 2020). Access to CBO services (e.g., linkage to care) was no longer available, thereby causing a disruption in the care continuum for women, and particularly BWLHA (Pinto & Park, 2020). Watkins-Hayes et al. (2012) referred to CBOs as framing institutions that offer knowledge, skills, and language for coping with a chronic illness, while referring to CBO service providers as framing agents for implementing strategies for coping with a chronic illness. Many BWLHA have restricted social networks due to intersectional stigma. The devastating effects of COVID-19 greatly affected members of marginalized communities like BWLHA, leaving them detached from their framing agencies and agents, which can be traumatizing. For example, the systems of support once offered through CBOs provided the opportunity for BWLHA to surround themselves with other Black women with similar experiences to help address ongoing traumas were no longer available, leading to a drastic increase of social isolation and loneliness (Pinto & Park, 2020). Nydegger et al. (2020) expanded the conversation by noting that BWLHA face stressors associated with HIV/AIDS, including structural violence and intimate partner violence, which make their experiences associated with a pandemic (e.g., shelter-in-place mandates) even more traumatizing. Furthermore, BWLHA experience trauma exposure at disproportionately higher rates when compared to women of other races and ethnicities, as receiving an HIV diagnosis is a highly traumatic experience (Nydegger et al., 2020).
Cuca et al.’s (2019) findings signaled a correlation between trauma and the physical, behavioral, and social health of BWLHA. Johnson-Bailey (2021) indicated that when women engage in learning during difficult circumstances (e.g., living with HIV/AIDS during the COVID-19 pandemic), it fosters hope that leads to empowerment, especially among Black women. In a study by Baumgartner (2014), results showed BWLHA often engage in informal (e.g., incidental, self-directed, and tacit) and nonformal learning activities to address chronic illnesses like HIV/AIDS. In another study, the findings revealed that BWLHA engage in support groups for health management, advocacy education, and other HIV/AIDS training (Baumgartner, 2012), which can inform strategies for self-care. Developing a trauma care plan (TCP) for self-care can serve as a method for healing justice and healing work for BWLHA (Salloum et al., 2015). In another study, Baumgartner (2002) discovered that for participants in HIV/AIDS groups, social interaction was significant to their learning processes by providing opportunities for relational discourses that helped with stigma-related discrimination and empowerment. Baumgartner further noted that service providers applied adult learning principles when facilitating education programs. When examining the impact of CBO service providers on HIV/AIDS efforts within vulnerable communities, it was discovered through the application of adult learning principles that clients changed how they approached treatment and care efforts (Egan, 2012).
Methods
A narrative inquiry was selected as the research design for this study as it allows the lives and experiences of individuals to be the primary source of data (Bloom, 2002), especially for individuals who have experienced marginalization (Loo & Sairattanain, 2022). In this study, I attempted to understand the narratives of CBO service providers regarding their experiences with BWLHA during a global pandemic. Storytelling is a useful technique for data collection as it can help individuals make sense of their personal experiences and reveal some compelling moments (Brookfield, 2013). Reflections, published biographies, and conversations are storytelling sources (Benson, 2014). Engaging the sources for storytelling can help shape the narrative, influence beliefs and actions, clarify the story’s setting, and make apparent what is not immediately observable. According to Johnson-Bailey (2002), narrative research is a balancing act among the data, the story, the methodology, the participant, and the researcher, and in the end, a narrative is constructed. As such, narrative inquiry enabled me to holistically capture CBO service providers’ experiences with BWLHA during a global pandemic (Lani et al., 2014).
To solicit CBO service providers, I sent a study description to the Council of Governments’ HIV listserv to gather information on the characteristics of agencies providing services to BWLHA. I used a purposeful sampling technique to select participants who could “purposefully inform an understanding of the research problem and central phenomenon of the study” (Creswell, 2007, p. 125). The participants were required to serve as case managers, health educators, or mental health/therapy counselors, as individuals serving in these roles are likely to work closely with BWLHA (Operario et al., 2020; Pinto & Park, 2020). The participants were also required to be employed full-time and to have worked with the agency for at least 5 years. When potential participants responded, I sent them an email with information about the study. Those selected to participate were asked to return an email with the following statement—the return of email is an agreement to participate in the study. Notably, three individuals met the criteria, though the third participant had to withdraw from the study for personal reasons. The focus was, therefore, on the narratives of two CBO service providers—Minty and Dugan (pseudonyms)—who provided direct services to BWLHA, were employed full-time, and had been working with the agency for at least 5 years. Consistency, trust, and relationship building with providers are essential for people living with HIV/AIDS and influence how these individuals engage in the care continuum (HIV.gov, 2022). According to the Bureau of Labor Statistics (2022), a long tenure employee has worked for an organization for 5 or more years, understands the organization’s culture, and demonstrates a level of commitment. Therefore, CBO service providers who were employed full-time and had been working with their agency for at least 5 years were chosen for the study as they were likely to have an established relationship with the women (i.e., BWLHA). Merriam (2009) indicated that selecting a small number of participants who can inform the phenomenon under study is a common practice. The narratives of these two participants provided various examples to describe the experiences of BWLHA.
A semi-structured interview process was utilized. Data collection efforts occurred over the phone and via Zoom and lasted approximately 60 to 90 minutes. The narrative interviews were audio-recorded and transcribed. The participants were asked to respond to open-ended questions. The interview questions were framed with prompts such as “Share with me how the women came under your care,” “Take me back to the day when your organization began adhering to the shelter-in-place mandates,” or “Paint a picture of the impact of the pandemic on the treatment and care efforts for BWLHA.” During the interviews, after each question, I encouraged the participants to continue telling their stories until they indicated they had finished. I constructed each narrative from the transcribed interview and field notes, resulting in nearly three and a half pages, single-spaced. When developing the narratives, I summarized what was perceived to be the highlights of the CBO service providers’ experiences with BWLHA, thus creating categories. When analyzing the CBO service providers’ responses in text form, I ignored the questions so emphasis could be placed on the participants’ responses. As the questions were removed from the transcripts, the text began to take the shape of a cohesive statement. More specifically, the oral narrative resembled a written account (De Medeiros & Etter-Lewis, 2020). Moreover, in the newly developed transcript, I coded the data based on the themes identified. Then, I grouped and analyzed the data describing the themes.
I analyzed the narratives using three approaches. The first was Alexander’s (1988) narrative analysis approach. I read the narratives multiple times, used salience principles, and focused on word meaning instead of the specifics of the language. Alexander introduced eight principles: frequency, primacy, emphasis, isolation, uniqueness, incompletion, omission, and negation. However, four were significant to the analysis process for understanding the participants’ stories within this study: frequency, omission, incompletion, and emphasis. Frequency refers to topics that are often repeated in communication, patterns and actions, and thoughts and symbols (e.g., “It felt like [repeated three times], we were against them by preventing them from coming to the organization”).
Conversely, omission refers to the communication, patterns, actions, and symbols that are omitted from the narrative (e.g., “You know, it was pure you know what [hell] for these women . . . pure you know what [hell] just to see them going through this . . .”). Incompletion often refers to the missing pieces of a narrative or story (e.g., “My primary care doctor . . .”). The narrator begins to describe their experiences or tell a story, then fails to complete the story, leaving the interviewer wondering whether there are secrets, surprises, or mysteries. Emphasis refers to the underscoring or highlighting of a statement or topic (e.g., “You call me so the hospital can charge my Medicare, but what did you really do for me?”). I chose these tenets as they helped me fully explore the participants’ narratives. Primacy, negation, and uniqueness are elements manifested in the selected principles.
Denzin’s (1989) life narrative approach was the second method I used for analysis. This approach helped me identify important events and verbalize insights or epiphanies within the participants’ narratives (e.g., “They [pharmacies] are not taking walk-ins. I have not been able to take my meds for about 8 or 9 days. Don’t they know I need my medicine?”). Denzin indicated such elements could be identified in most narratives allowing the researcher to gain more insight into the participants’ stories.
Last, I used a linguistic approach that was culturally specific for narrative analysis. More specifically, I used culture as a tool for analysis (Johnson-Bailey, 2002). Johnson-Bailey (2002) indicated that a cultural approach to analysis gives meaning to participants’ stories. Because I obtained narratives from Black CBO service providers, there was an assumption of a cultural connection to the Black women to whom they provided services (e.g., “You know Black women have it hard already. They [BWLHA] were used to coming in and receiving services and just visiting with the other ladies, but the virus just shut all of this down”). As a result, for this research, culture offered a lens to make meaning of the lives of BWLHA as told from the perspective of CBO service providers. Moreover, the cultural analysis focused on Black English, how Black people communicate, word emphasis, and repetition of language (Etter-Lewis, 1993; Johnson-Bailey, 2007; Tarone, 1973).
I implemented several techniques to address trustworthiness and rigor (Goings, 2016), including memoing, rich thick descriptions, and member checks. After and during each interview, I used the technique of memoing to record and preserve my thoughts, ideas, impressions, and feelings that could prove to be significant for the research. For example, I documented noticeable lowered tones at different parts of the participants’ conversations. I later learned a lowered tone meant adhering to confidentiality policies. In addition, I used the technique of thick descriptions (i.e., direct quotes from participants) to contextualize the participants’ responses. Finally, I used member checks to increase the dependability of the findings. For example, there were times I misunderstood aspects of the conversation (e.g., issues with medication during the pandemic). Member checking allowed me to identify and clarify the most salient points about the issues of medication rather than making personal assumptions and projecting my personal experiences.
Description of Participants
As a full-time health educator, Minty (self-identified as an African American female) provides health education, counseling, health literacy (e.g., uptake of PrEP and other anti-retroviral therapy), food bank services, and other support to BWLHA within a CBO in the central region of the United States. Minty has been working at the organization for over 10 years. The organization provides services to people living with HIV/AIDS across five counties.
Dugan (self-identified as an African American male) serves as a full-time case manager within a CBO in the southern region of the United States. As a case manager, Dugan assesses clients’ wellness, develops care plans, provides counseling and intervention services, charts referrals, and conducts home visits. Dugan has been working at the organization for nearly 7 years. The organization provides services to people living with HIV/AIDS across three counties.
Findings
Data analysis led to four themes that described CBO services providers’ experiences with BWLHA during the global pandemic, including social isolation (e.g., deprivation of face-to-face contact and group therapy, concealing diagnosis, and reverting to old habits of substance and alcohol abuse), medical and telehealth concerns (e.g., disregard for health concerns and accessing medication), perceived social categorization of us and them, and recommendations for healing work (e.g., meditation, informal learning engagements, self-advocacy, and trauma care plans [TCPs]). In the following section, the findings were developed to answer the question regarding the impact of the global pandemic on the health and well-being of BWLHA.
Social Isolation
According to Singer (2018), humans are wired to engage in social networks. Levels of anxiety and depression may increase when people become socially isolated, especially for extended periods of time, and these increased levels of depression and anxiety can lead to other health concerns. According to the participants in the current study, some of the women with whom they worked experienced feelings of anxiety and depression because of the prolonged shelter-in-place mandates.
Minty reported that a woman indicated, “I am 39 years old, but I feel like I am 90. I have a heart issue, cholesterol, and high blood pressure. I cannot take it [being isolated] any longer. I am going nuts.” At the onset of the COVID-19 pandemic, the women could not participate in their regular weekly face-to-face group therapy sessions. The participants indicated that the inability to connect physically with individual group members adversely affected the women’s mental health. Dugan reported that a woman stated, “Not being able to talk to the other women has done something to me. I really need this time to talk through some things.” Minty indicated that women called the agencies practically begging to engage in face-to-face group therapy. For example, the women made such statements as, “When can we come back to the group?” and “Do you know how long it will take for us to be able to come back [to the agency]?” It became difficult for the service providers to respond because they lacked certainty about how they would move forward in their treatment and care efforts during the pandemic, which exacerbated the issues related to social isolation.
The participants shared instances of women dialing the suicide prevention hotline to solicit the assistance of a qualified person to offer needed support. Minty indicated, “I have to get someone to provide next-level care the women need. It can be difficult for the women when these professionals are unavailable.” Additionally, there were instances when the women needed immediate care, and the group facilitator had to be contacted. Dugan stated, “In some instances, the group facilitator organized a meeting with the woman in distress along with other support group members through a media platform. The assistance offered through impromptu meetings helped clients to manage feelings of depression better.” Dugan also indicated one of the women stated, “Thank you for connecting me with the group. To hear their voices and to see their faces gave me the opportunity to get some human interaction I am not getting.” In addition to experiencing bouts of depression, the shelter-in-place mandates made it increasingly difficult for the women to conceal their diagnoses, as many lived with roommates.
The balancing act of being withdrawn without raising suspicions became increasingly difficult, which increased some women’s anxiety levels. Dugan indicated one of the women stated, I live with my cousins. They do not know I am HIV positive. I try not to be around them too much. It is crazy. I must think about my health and, at the same time, try to stay away from them.
The participants also indicated that some women experienced difficulties concealing their diagnoses from family members who had a reputation for divulging others’ personal information. According to Minty, a woman explained, “Some of my family members live with me. They say I am too private. I cannot tell them I am HIV positive. They will tell everybody. So, I distance myself from them.” Dugan indicated another woman explained, “They talk too much. When I am talking to you all [CBO service providers], I have to go and hide. They do not know I am HIV positive.” Apart from being confined to spaces with individuals who could divulge their HIV identity, the prolonged inability to engage socially with members outside the home also increased the women’s anxiety levels.
Their inability to engage with individuals outside the home caused some women to consider reverting to their old habits and addictions. Dugan indicated that one woman stated, “I am so stressed out. Not being able to speak to people face to face makes me want to go back to drinking and smoking.” Other women were confined to spaces they shared with their abusers, which also increased anxiety levels and caused them to consider revisiting their former addictions. Minty revealed the women would make such statements as “My daughter mistreats me. I just feel like drinking” or It gets tough for me sometimes. The arguing back and forth is driving me insane. If I say blue, he says green. Everything does not have to be an argument. It is enough to make you want to have a drink.
Sheltering in place also meant medical visits would transition to digital platforms, which also posed a challenge for the women.
Medical and Telehealth Concerns
The participants reported that many women experienced an abrupt change in their medical care as they were forced to visit many of their healthcare providers through various media platforms (i.e., telehealth). These extended visits with healthcare professionals through media platforms caused the women to feel their health concerns were not being taken seriously. The participants recalled the women making such statements as, “Medical professionals are working from home. If you are working from home, you are not dealing with me” (Dugan), or You called me so the hospital could charge my Medicare, but what did you really do for me? What did you really accomplish with me? You did not get to put me on a scale. You did not get anything effective going on. (Minty)
Another example was: My primary care doctor—I expect them to look at the whole of me. The pandemic started in March. I need some labs done, not just for HIV. Labs can tell a lot about a person’s health. I have 11 different doctors that I see. (Minty)
Additionally, women experienced difficulty accessing their medication in a timely manner.
Dugan indicated a woman revealed, “They [pharmacies] are not taking walk-ins. I have not been unable to take my meds for about 8 or 9 days. Don’t they know I need my medicine?” Minty indicated that another woman stated, What am I supposed to do if I cannot get my medicine? I have been trying to call the pharmacy but have not gotten in touch with anyone. I do not want to go all the way up there and not be able to get my medicine.
Notably, when PLWHA experience a disruption in their anti-retroviral therapy (ART), it can affect their viral load suppression. The lack of ART uptake can affect how clients engage with the care continuum, which can be traumatizing when treatment and care are inaccessible or inadequate. Moreover, adherence to the shelter-in-place mandates separated the women from their needed services, health care providers, and medication, which led to perceived social categorization. In the following section, the findings were developed to answer the question regarding the impact of the global pandemic on CBO service providers’ treatment and care for BWLHA.
Perceived Social Categorization of Us and Them
The women were denied in-person access to the CBO, which was analogous to a wall separating the service providers from the women, creating us and them effect. Though there was the appearance of an us and them narrative, the CBO providers were empathetic. Dugan indicated, When the virus emerged, it disrupted the care and treatment I provided for women. It [mandate] separated “the agency” from the women, and the women were no longer able to come to the center and receive services . . . very heartbreaking.
Similarly, Minty indicated, You know, Black women have it hard already. They [BWLHA] were used to coming in, receiving services, and visiting with the other ladies, but the virus shut all of this down. It felt like [repeated three times] we were against them by preventing them from coming to the organization.
Dugan indicated, “It was almost like we had shut the doors overnight. They were immediately denied access to the organization for a long time without answers. That is traumatizing.” Minty indicated, “You know, it was pure you know what [hell] for these women and pure you know what [hell] just to see them going through this . . . when you are Black and a woman, it is altogether different.” Separation from the women meant separating from the services they were used to receiving from their organization.
For example, Minty indicated, “The women could no longer come to the agency and get tested. Instead, the tests were mailed to them, and they had to mail the specimen to us or drop it off at the agency.” Dugan indicated, “We could no longer visit the women in their homes. This took away from the private conversations that would occur between us. We could not go anywhere.” The service providers offered informal learning strategies to help the women navigate the drawbacks of the pandemic. The following section was developed to answer what healing justice strategies guided by informal learning principles CBO service providers offer.
Informal Strategies for Healing
Although the service providers could recognize signs and symptoms of various mental health conditions, they did not identify as mental health professionals. Instead, they referred to themselves as educators. Minty explained, I am not a [mental health] professional. I have certifications that will allow me to educate the women and others and implement strategies that can serve as a safety net until I get some professional help for the women. However, I am not a mental health professional. I want to make that clear.
Dugan indicated, I have taken continuing education courses to identify different signs and symptoms of depression and other mental health concerns. I am here to teach the women self-care strategies. But I am not a mental health professional. I dare not go around diagnosing any of the ladies. I may be able to tell you what something “appears” to be, but I am not a professional.
In the role of educator, strategies for meditative practices were offered to help the women manage depression and anxiety. Dugan stated, I do not profess to be an expert or an instructor. However, practicing meditation has helped me to become more relaxed and focused. Through meditation, I am better able to address issues that may occur. I am still learning various techniques.
In adherence to COVID-19 regulations, clients were mailed copies of meditation strategies and websites that offered similar techniques. Dugan shared some of the women’s responses to meditation, including, “It [meditation] takes some real concentrating, but the activities kind of relax your body.” Another indicated, “It [meditation] gives me something to do. Meditation takes my mind off the world. I am glad you gave us this information.” Minty said some women found meditation difficult because they lived with roommates. Dugan recalled a woman suggesting meditation in their support group, indicating, “These activities would be great for the women’s group.” The women also were encouraged to engage in various learning activities, including online workshops, panel discussions, webinars, and review reading materials online and in hard copy. Virtual participation in “sister circles” and other networking systems providing current information on HIV/AIDS-related issues was another recommendation.
It was also recommended that the time spent in isolation be used to learn strategies for self-advocacy. The women were allowed to listen to calls to learn techniques for self-advocacy, such as how to demand specific services. The women were taught strategies for becoming informed consumers, asking probing questions, responding to statements, and adjusting their tone of voice. Minty indicated, “Developing skills for advocacy is important. See, when women can stand up for themselves, it gets people’s attention. It also builds self-confidence because many BWLHA have developed learned helplessness.” Dugan stated, I tell them there is always a way to say everything to get your point across, and sometimes you have to take the low road. You really do. That does not have to happen all the time, but it gets people’s attention and lets them know you are serious.
The CBO service providers also recommended that when providing treatment and care for BWLHA, it is important to help the women develop TCPs to navigate their traumatic experiences.
Both CBO service providers recommended that service providers develop an understanding of the prevalence of trauma, the variations of trauma, and how trauma affects individuals differently and put the knowledge into practice. Dugan stressed the importance of a care plan and how authenticity is significant to the healing process: Although I am not a therapist, I can be therapeutic in my relationship with the women. All of us are experiencing some form of trauma, especially during this pandemic. If you look in the mirror, all of us are experiencing something. They [the women] need to know that I am human . . . need to see that I have some form of a care plan to see how I address my personal trauma. The one thing their plan has to reflect is strategies for how they can address their traumatic experiences.
Minty explored the usefulness of care plans and compared the plans to an Individualized Education Plan (IEP) for students indicating, BWLHA experience more trauma than you can imagine. The changes brought on by the pandemic have really made matters worse for them. We have talked about a trauma plan, but it does not have to be formal. It can just be some strategies to help them [women] get through some of the tough times . . . personal . . . reflect their pain and suffering. Because we don’t know what that means for them, I cannot pull a plan from the internet and give it to them. Some people have an IEP; a care plan can be viewed in the same way.
While the women were encouraged to engage in informal learning activities, they were also advised to avoid engaging in activities that could hinder their learning. Minty indicated, I told them [women] sitting in front of the television is not doing anything for you. You need to keep your brain functioning . . . . reading and learning. There are all sorts of materials, webinars, listening sessions . . . support groups for Black women.
Discussion
Findings from this study lead to several discussion points for understanding the impact of the global pandemic on CBO service providers’ treatment and care of BWLHA. For this study, BWLHA, as described by the CBO service providers, were forced into spaces where they had to be more strategic in concealing their diagnosis from family members and friends and co-existing with their abusers for extended periods. These findings indicated these women (BWLHA) were marginalized from the margins, which aligns with Fletcher et al.’s (2016) research indicating BWLHA are reluctant to disclose their HIV status for fear of alienation at both the interpersonal (e.g., family, friends, and networking systems) and community (e.g., the Black church) levels. Based on the CBO service providers’ responses, the impact of social isolation led to increased levels of anxiety and depression, creating trauma among the BWLHA. Additionally, the women received medical care in a digital environment and felt their physical health was no
According to the CBO service providers, during the telehealth visits, the taking of vitals was not administered, a complete examination was not conducted, and the examination (i.e., touch, feel) of any pain sites was eliminated, creating a traumatic experience for the women managing a chronic health disease. Notably, many people were traumatized by the impact of the pandemic. However, African American women living with a chronic disease like HIV face intersecting challenges in sociocultural (e.g., racism) and interpersonal (e.g., HIV stigma) contexts, making them more vulnerable to adverse health outcomes. The use of telehealth was especially traumatizing given the historical mistreatment in the healthcare system, HIV-related discrimination, and the desperate need for community. When health establishments create barriers for BWLHA to access proper healthcare and medication, it can also be traumatizing, which affects how they engage with the care continuum (HIV.gov, 2022).
During the pandemic, each of the service provider’s (Minty and Dugan) organizations was forced to close their doors, creating another barrier to treatment and care for women living with HIV/AIDS. For example, Minty indicated, You know, Black women have it hard already. They [BWLHA] were used to . . . receiving services . . . visiting with the other ladies, but the virus just shut all this down. It felt like [repeated three times] we were against them.
As a Black woman, Minty was empathetic toward the women’s experiences, which aligns with the work of Johnson-Bailey (2021), which indicated that due to persistent societal subjugation, Black women have developed a concept of community bound by positional connectedness, which can be a tool for transformative learning. As well, Dugan indicated, “It was almost like we had shut the doors overnight . . . In an instant, they were denied access to the organization . . . That is traumatizing.” Dependent on the person, such abrupt changes can create trauma (Leonard, 2020; Morin, 2020), especially for BWLHA (Nydegger et al., 2020). Although Minty and Dougan did not identify as framing agents, they offered unique ways to continue the informal learning support for the BWLHA they serviced while separated from their framing institution and framing agent during the pandemic.
Johnson-Bailey (2021) indicated that good teaching is not about one person being the subject matter expert but rather understanding the exchange of knowledge taking place and acknowledging what “others” can bring to the learning. Minty and Dugan were learning through the experiences of BWLHA about how to continue learning while adhering to the pandemic mandates. Moreover, the current findings do not parallel much of the literature focusing on social categorization, where there is often an ingroup and an outgroup (Leonardelli & Toh, 2015; Liberman et al., 2017). Instead, the current study’s findings highlight the empathy the CBO service providers demonstrated, which made it more difficult for them to close their doors, preventing the BWLHA they serviced from engaging fully in informal learning for treatment and care. Baumgartner (2012) indicated that BWLHA learn best through informal learning engagements, including guest speakers, support groups, websites, and printed materials. Meditation, networking systems or “sister circles” (Collins, 1986, p. 2), associations, self-advocacy, avoiding activities that increase stress, and developing a TCP were all informal learning strategies the CBO service providers recognized as healing work for BWLHA. When women, particularly BWLHA, engage in learning strategies for self-care to address trauma, they are being self-directed in their learning as they take responsibility for their healing (e.g., developing a TCP; Baumgartner (2012, 2014).
Implications
BWLHA can learn to develop a TCP for healing justice, especially during a pandemic. Borrowing from Marchi’s (2020) strategies for care, I have developed strategies specific to BWLHA. Figure 1 illustrates nine elements adult and health educators might use to improve treatment and care and to offer healing justice for BWLHA, including exploring Black women’s histories of trauma, exploring the experiences of BWLHA, presenting a rationale or purpose for a TCP, creating a safe space, demonstrating transparency and trustworthiness, facilitating reflection on women’s personal trauma experiences, including mental health professionals, developing a TCP, and empowering women to act. BFT, informal learning, and trauma theory frame these nine elements. For adult educators assisting adults like BWLHA to learn to develop TCPs, it is important to consider BFT. BFT can help frame the intersectional experiences of BWLHA; explore the intergenerational trauma experienced by Black women to develop a critical lens for understanding Black women’s history of pain, violence, and trauma; explore Black women’s experiences living with an HIV/AIDS diagnosis; and assist BWLHA with developing personal strategies for healing justice. When developing personal strategies for healing justice, CBO service providers should consider the following strategies: allow the women time for reflection about real-life experiences to inform their TCP, create a safe space to be vulnerable and demonstrate trustworthiness and transparency, make professional therapists available who are knowledgeable about the intersectionalities of BWLHA, encourage BWLHA to think about personal symptoms of trauma (e.g., cognitive, emotional, behavioral, spiritual, interpersonal relationships, etc.), collaborate with BWLHA to determine risk factors that may evoke primary or secondary trauma (e.g., personal, work, cultural, etc.), encourage reflection on personal coping strategies for navigating traumatic experiences, and create opportunities for BWLHA to think about ways to engage in meaningful work within their traumatic experiences. Strategies from the work of Moss (2020) were used to help adults like BWLHA develop a TCP.
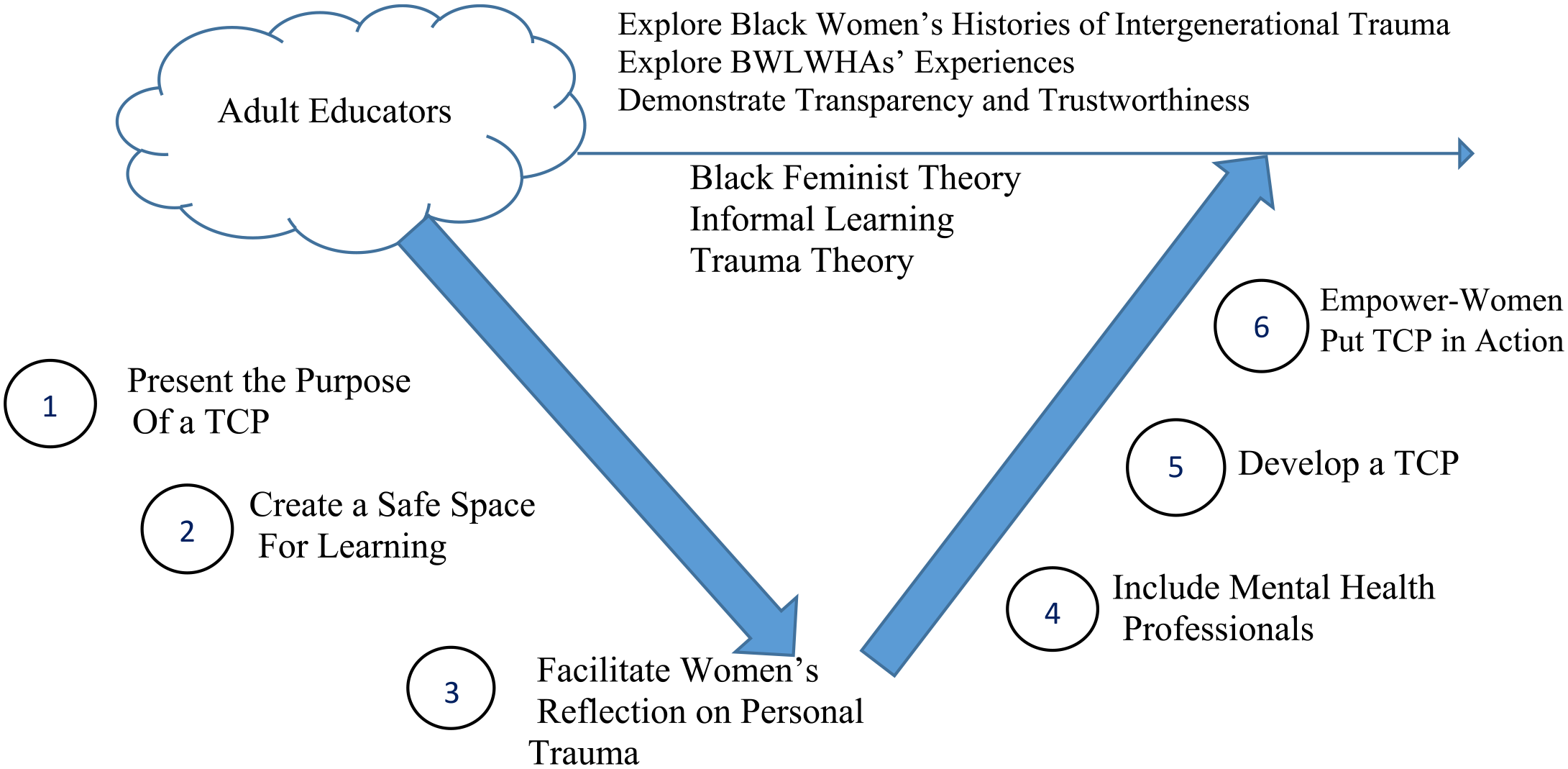
A nine category model for healing justice for BWLHA and experiencing trauma.
Adult educators, including CBO service providers and health educators, can do the following. First, explain the rationale and intent for developing a TCP. Adults need to know why they are engaging in a particular activity. Then, post examples of real-life experiences to inform the development of a TCP. Many adults are visual learners who need to see charts or diagrams. Next, using “I will” statements, have the BWLHA write two personal coping strategies and two ways to engage in meaningful work within their trauma. Afterward, using “I will” statements, ask the BWLHA to write at least two sentences that can be referenced whenever they experience a traumatic event. It is important to encourage adults to write realistic and measurable strategies. Next, have the BWLHA identify barriers that may cause them to abandon their strategies for addressing trauma. Then, using “I will” statements, ask the BWLHA to identify strategies that can assist them in overcoming obstacles that can prevent them from addressing their trauma. Afterward, using “I will” statements, have the BWLHA identify support systems (e.g., spouse/partner, children, parents, friends, and other family members) and be specific about their roles within the support system. Last, empower BWLHA to be self-directed learners by encouraging them to put their TCP into practice.
For this research, three adult learning principles can be associated with constructing a TCP for BWLHA. Adults desire to learn strategies for immediate application, are goal-oriented and focused on life-centered tasks, and are motivated by internal factors (Knowles et al., 2020). When BWLHA create a TCP, they are addressing an immediate life situation, focusing on life-centered tasks for healing. They are internally motivated and self-directed in their learning for healing. For BWLHA, teaching them to develop a TCP is a step toward healing, indicating that their health is being taken seriously (Hoffman et al., 2016). As such, BWLHA may feel internally motivated to engage in activities to learn strategies to address trauma. Moreover, when the health of BWLHA is prioritized, it can reduce stress and increase self-efficacy.
Findings from this study can guide educators and mental health providers when engaging with Black women living with a chronic illness like HIV/AIDS. Adult educators can serve as a resource for service providers to support BWLHA in their engagement in self-directed learning to manage HIV health-related issues. For health educators, it is essential to understand adult learning and the significance of informal learning in the contexts of self-directed and incidental learning and serve as a catalytic agent for these learning opportunities to occur tailored to the unique health needs of BWLHA. As emotional support is essential for Black women living with a chronic disease like HIV/AIDS, it is essential for mental health providers to understand Black women’s life histories and experiences and to be transparent to help BWLHA begin the healing work for living with rather than dying from a chronic illness.
Conclusion
I designed this study to add fresh findings to the existing literature, as Black women’s health remains at the bottom of the healthcare agenda. BFT can guide scholars to begin interrogating which women’s experiences are being prioritized by placing the experiences of BWLHA at the research nucleus. Trauma has been threaded throughout Black women’s experiences, and the challenges faced during the pandemic have exacerbated trauma issues, especially for BWLHA. Building on BFT, CBO service providers recognized the intersections of BWLHAs’ experiences as they offered strategies for healing justice to navigate traumatic experiences in the context of informal learning. More specifically, it was important for adult educators to teach BWLHA to develop a TCP guided by BFT. It was also important for BWLHA to learn to develop a TCP informed by personal experiences that intersected race, class, gender identity, ageism, HIV/AIDS, and trauma amid a global pandemic.
As with any study, this study had some limitations. For example, the voices of BWLHA were told in the second person. Also, studies including larger cohorts of service providers would enhance generalizability. However, this study offers trauma-informed care strategies to help BWLHA navigate trauma events. The findings can be used by adult educators in CBO settings, academe, and beyond and inform curricula developed by adult education and human resource development professionals. Future research may focus on critical health literacies for Black women to raise awareness of Black women’s issues, engage in critical dialogue, and become involved in the nuances of Black women’s health for decision-making purposes. Typically, the leadership of CBOs often comprises staff who are White men and men who identify as gay. At the same time, many people receiving services are people of color, often low-income, and cisgender women. This phenomenon and its effect on client service and education may be a topic that deserves further study.
Footnotes
Appendix A
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.