
Abstract
At the heart of soul care is self-care. Being able to love God and love others is rooted in how we love ourselves. Each person’s understanding of self-care is informed by their personal belief system and their implementation practices. This article will provide a multi-phasic model that describes the self-care journey and focuses on how to implement self-care practices. A key distinction of this model is that it is used in an ongoing fashion. To avoid confusion between beliefs and practice, attention will be given to the decision-making process for self-care implementation. Specific activities that address the physical, mental, emotional, spiritual, and relational parts of people will be discussed. The article will also consider the nuances of assessing self-care and why it is important to value self-care, which is in keeping with the greatest commandments provided by Jesus in Mark 12:28–30.
How might you answer the following question: “What good is it for someone to gain the whole world, yet forfeit their soul?” 1 Jesus posed this question to his disciples after declaring that being his disciple meant denying self, taking up one’s cross and following him. Self-denial is understood and applied differently, depending on one’s philosophical or theological approach. 2 Yet, it seems that the parameters provided by Jesus for being a disciple can result in mistreatment of the soul, rather than care for the soul. Conversely, when one does care for the soul, it might be articulated through spiritual disciplines, rather than a holistic expression for one’s entire being.
Context
Having spent my life growing up in the Pentecostal church as a pastor’s daughter, I have seen people enter the doors of the church who were unclear on how their soul care was related to their self-care. For many of them, too much emphasis had been placed on a misunderstood application of self-denial. When I entered the mental health field, a similar experience was occurring for students, professors, and clinicians. One example that has stayed with me was an individual who spent a lot of time pouring into others at the expense of her health; to see a doctor meant neglecting those she was called to love.
My current context includes three primary spheres of activity: working in a doctoral program, being in private practice, and doing lay ministry at my church and other ministry settings. The doctoral program is at a liberal arts, Baptist university, training students from diverse theological and clinical backgrounds to work in the marriage and family therapy field.
My private practice offers Christian counseling; people of all beliefs are welcome, but the counseling is rooted in a biblical perspective. My church is Pentecostal. However, the other ministry settings that I provide training and instruction is variable. Regardless of which sphere I am operating in, the core of my identity is as a child of God and I recognize my role as His ambassador. 3
Practically, I believe that a proper understanding of soul care necessitates self-care, which I have defined as an intentional, proactive approach of personal care for the self, enacted by an individual that encompasses the physical, mental, emotional, spiritual, and relational aspects of life.
4
Mark 12: 28–30 states: One of the teachers of the law came and heard them debating. Noticing that Jesus had given them a good answer, he asked him, “Of all the commandments, which is the most important?” “The most important one,” answered Jesus, “is this: ‘Hear, O Israel: The Lord our God, the Lord is one. Love the Lord your God with all your heart and with all your soul and with all your mind and with all your strength.’ The second is this: ‘Love your neighbor as yourself.’ There is no commandment greater than these.”
Most people are busy living their lives, without taking the time to think about if their soul needs to be refreshed or restored. Therefore, a recitation of Psalm 23 might be given in less than a minute, as the reader quickly chants “The
In this article, I will begin by describing the model that I have developed for implementing self-care in one’s life. 6 I have used this model in several places, including the instruction of doctoral students, in churches, and other ministry settings. Next, I will provide the foundational teaching curriculum I use with these audiences, as well as the suggestions for implementation and practice. Finally, I will explain the nuances of assessing the curriculum.
The multi-phasic model that I use acknowledges the journey to beginning the implementation of self-care and the cycle of self-care that follows. I will explain each step, followed by the key categories and subcategories related to that phase. In order to gain an understanding of the specifics that will be discussed later, an overview of the process as a whole will be given here with a more comprehensive discussion following the explanation of categories inherent in the model.
The central phenomenon that will become evident throughout the discussion is that self-care is a journey. The multi-phasic model of self-care contains six steps that include a self-care cycle; the six steps are Unawareness of Self-Care, Initial Exposure to Self-Care, Assimilation of Values Associated with Self-Care, Conduits to Self-Care, Decision regarding Implementation of Self-Care, and Implementation of Self-Care. The sixth step leads into the self-care cycle of steps four through six, with an individual beginning to implement self-care but coming upon an interruption to self-care. This disruption, regardless of what manner it takes, is an experience that brings the individual to another point of decision as to whether self-care will or will not continue. For some, the choice will be to implement self-care; thus, the journey continues forward. For others, the roadblock does not necessarily deter the individual from implementing self-care, but it might take some time before the individual is able to get back on the road. Depending on how long an individual remains in limbo and how this impacts the individual, there might be a regression backwards before returning to self-care practices. Finally, some will find that the roadblock significantly interferes with self-care practices or might find it too difficult to continue self-care practices and will choose to get off the road until the individual has another experience that necessitates self-care, which reignites the cycle once more. 7
Following the completion of the first step, unawareness of self-care, the individual’s initial exposure to self-care occurs as a result of one or more experiences, which are Family of Origin, Religion, and Life Experience. These experiences contribute to the individual’s assimilation of values related to self-care, Negative, Neutral, and Positive. The first three steps are the model of formation because they inform the way that self-care is understood. After the individual moves beyond the second and third steps, in step four the individual may or may not be practicing self-care but encounters one or more experiences that will influence the individual’s eventual decision to practice self-care. Step five necessitates a decision on the part of the individual, which was described as Yes, Yes but, and No. Having made a decision regarding the implementation of self-care, the individual continues journeying through the self-care cycle, wherein the utilization of self-care transitions from theoretical idealism to actual practice determined by the individual’s values related to self-care. Steps four through six form the basis of the teaching curriculum and how it is implemented in one’s life.
Model of formation
Unawareness of self-care—step one
The old adage about how a journey of a thousand miles begins with one step is very true of the self-care journey; unbeknownst to many, the process of incorporating self-care into one’s life began before the individual was actively thinking about it. Thus, the journey to self-care actually begins before the individual realizes that steps have already been taken. Step one of this process is the briefest theme that is addressed here because the dynamics of self-care cannot be understood until one has been exposed to self-care. As long as someone is unaware of self-care, it will be difficult to comprehend that changes are needed. 8 Anyone’s initial exposure to the concept of self-care will eventually influence the values that they have about self-care. Consequently, an examination of step two provides the origin for how an individual will unconsciously assimilate certain values related to self-care that will eventually influence the level of ease or difficulty one has incorporating self-care into one’s frame of reference and actively working to care for their spirit, soul, and body. 9
Initial exposure to self-care—step two
While the concept of self-care is important all throughout one’s life, each individual has their own experience in being exposed to it. In some situations, people will describe how more than one category has added to or detracted from their view of self-care, which will inevitably impact their values about self-care. The exposure to self-care is not always consciously recognized; upon reflection, it seems that what resonates for most people includes the following three categories: family of origin, religion, and a specific life experience.
Family of origin
It is often when we think back to what was modeled in our family of origin that we can identify why we do what we do; this is especially true for the care we give to ourselves and the care we give to others. 10 We might mimic what our family did or do the direct opposite of what we learned. If self-care was not deemed important by the parents, children might grow up thinking it was not important. Sometimes what is seen in our families of origin makes it difficult for us to give ourselves permission to engage in self-care. The cultural influence of one’s family of origin can also prove to be paramount in how someone comes to hold certain values related to self-care. 11
Religion
One’s personal beliefs and connection to a particular religion, which includes the influence of the church, can be another exposure to self-care that influences our values. Self-care can be understood as a helpful practice with roots in one’s religion. 12 Some people find that self-care does not seem to fit with their religious teachings. If you are involved in church as part of your occupation or because of your spouse’s occupation, self-care could be difficult because you are doing the Lord’s work, caring for the souls of others without having time to care for your own soul. 13 The teachings of the church can also contribute to seeing self-care as unspiritual or having received mixed message about it. It is not a simple matter to find a definitive place for self-care in the context of church teachings.
Life experience
One other area that informs people’s beliefs about self-care is a specific life experience. An example of this could be receiving a medical diagnosis that encourages self-care as part of the recovery, which then fosters a positive belief about self-care. A different person could find that a family crisis serves as negative funnel for self-care. Unfortunately, sickness is often the catalyst for adjusting an individual’s unconscious or conscious views about self-care. 14 Since we all have our own life experiences, it is not surprising that these events influence how we think about self-care. Whether it is one’s family of origin, religion, or a specific life experience, they each affect the assimilation of values, negative, neutral, or positive, that an individual has about self-care.
Assimilation of values associated with self-care—step three
Considering the various factors that lead people to have beliefs and values about any number of areas, what is learned about self-care will nonetheless be influenced by the preexisting beliefs of each individual. 15 The assimilation of these values is generally an unconscious incorporation until directly confronted by a principle such as self-care, wherein one must try to determine what makes it easier or harder to engage in self-care. 16 Some will have negative beliefs about self-care, since experiences might have taught them to devalue self-care. In other situations, it is because people were taught to put others first and put themselves last. Not everyone will consider their initial perspective of self-care to be negative but there might still be a progression from a somewhat neutral position into an improved view of self-care. For example, one person might start with a neutral view of self-care because it was not modeled in their home. Another person would not identify the values as either negative or positive, which leaves that person approaching self-care from a neutral position. Lastly, some people will have a positive view about self-care. This could be because their families of origin taught them about self-care, the theology in their church emphasized self-care, or a life experience caused them to appreciate and value self-care.
Each person’s exposure to and experience with self-care will ultimately influence the journey of self-care that is explicated in steps four through six. The first three steps are necessary to understand what informs the way self-care is understood. As time goes on, self-care can shift from the unconscious to the conscious, regardless of how an individual is implementing it. Therefore, the next three steps are much more involved as they are the essence of the process as a whole and there is a cyclical nature to that process. In addition to the movement that is part of the process, elements such as intentionality, emotions, challenges, and rewards will constantly impact where an individual is in the journey. To that end, step four addresses life experiences but since steps four, five, and six are so interrelated, it is necessary to include references to each one whenever the fourth step is being discussed.
Teaching curriculum
Conduits to self-care—step four
Entering step four, self-care will henceforth have a greater or lesser role in someone’s life depending on the priority that it is given and the manner in which it is integrated and reintegrated throughout life. Unlike other, more tangible milestones that can be achieved, such as graduations or finding a job, self-care is not a box that gets checked as being finished. It is an ever-continuing, ever-evolving journey that will have its ups and downs. Distinguishing between self-care as a forced activity or “to-do list item” and self-care as part of one’s lifestyle is necessary for differentiating how it is can benefit one’s life. 17
We can all attest to the fact that life does not slow down on its own so we can step back and examine how best to continue. Within this part of step four, people will constantly arrive at a crossroad that necessitates the decision-making done in step five. Conduits to self-care may be part of a more formal learning experience, such as taking a class, or they may be informal, such as when you notice that you are experiencing burnout. 18 Perhaps you have been utilizing self-care and would identify being firmly rooted in the implementation aspect of step six. Nonetheless, life experiences, unexpected or planned, will cause you to pause on the journey and reevaluate self-care. Consider what happens when one person within a couple or family system receives a medical diagnosis. The decisions that are made next serve as an example of how interrelated steps four, five, and six are in this process. Faced with the illness of one spouse (step four), the other spouse or children could decide to work less hours or put school on hold, removing extra activities from their plate (step five) to take care of themselves and their family, essentially practicing self-care (step six) by recognizing their own limitations and implementing self-care in a manner that works for them. Self-care is not a cookie-cutter conception; it is unique to each person and their needs. 19
Life experiences do not have to be drastic to effect change. It could be that over the course of a year, you have more responsibilities than you did in the past. Working through the self-care cycle could help you to begin making different choices regarding self-care. When dealing with a difficult year that was full of responsibilities (step four), you might have initially decided to place the needs of others before your own (step five), which could prevent you from implementing self-care (step six). Vacillating between steps four and five, you can take stock of the situation and those experiences (step four) and made a different decision (step five) for yourself going forward that includes being intentional about self-care and doing things like saying “no” as a form of implementing self-care (step six).
In many situations, the life experiences that reignite the self-care cycle will not be one-time occurrences but are the constants in our lives. To be able to move from step four to step five, an individual must confront one of the hardest parts of the self-care process: giving oneself permission to engage in self-care. Recognizing that each person’s journey is different, it is still apparent that this is one of the first and one of the larger barriers a person will face; therefore, it is the first barrier represented in the diagram (see Figure 1). Permission does not come easily, even when one believes that self-care is important. Each person must interact with the messages received from their families of origin and other significant contributors to their value system about self-care. Quieting the voices, both internal and external, can be a helpful way of creating space to find what works for an individual.
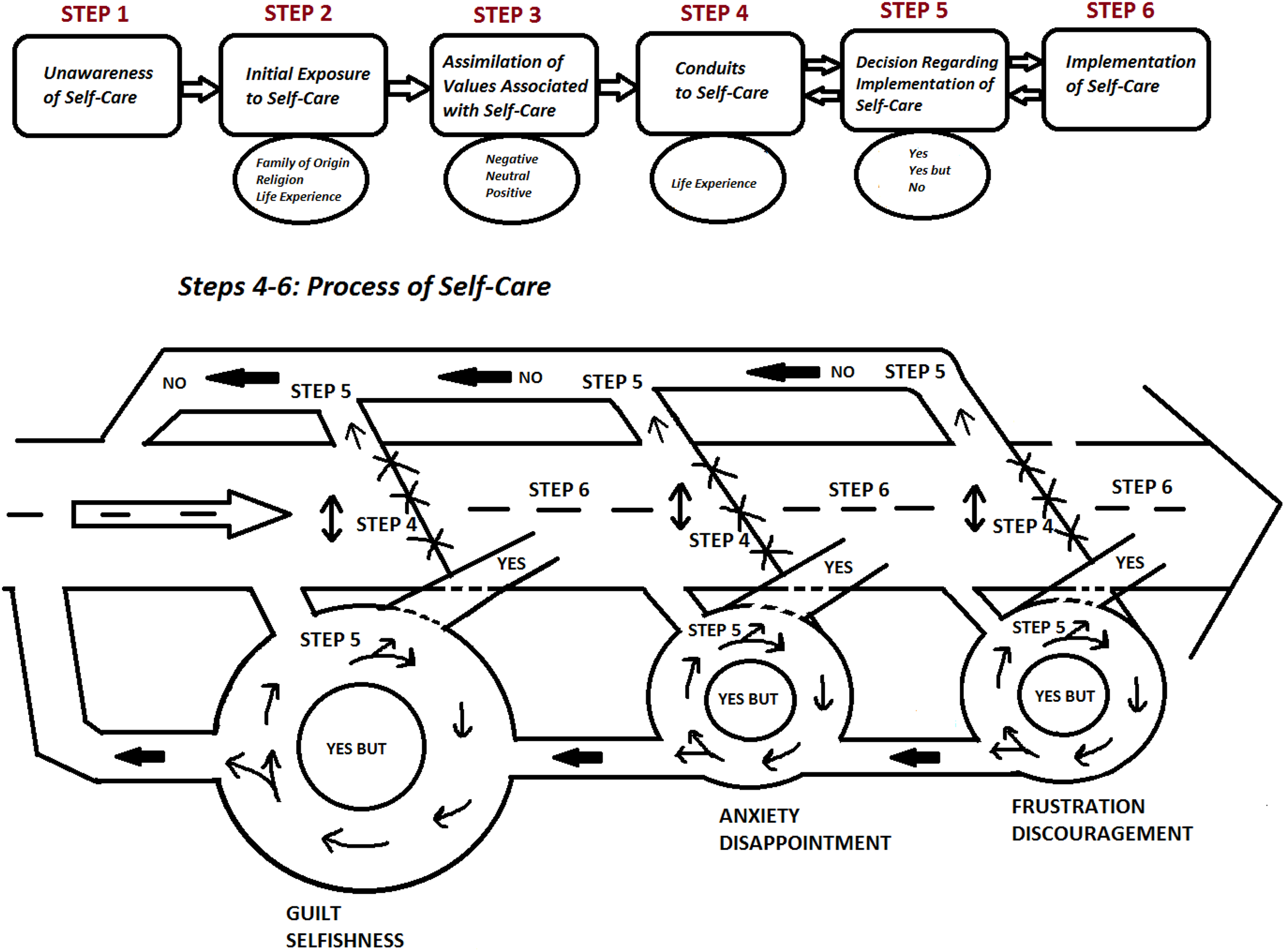
Visual Representation of the Self-Care Journey.
Knowing what to do is not equivalent to doing it, nor does it mean that one feels the freedom or the permission to practice self-care. Giving oneself permission to practice self-care is not as simple as making a logical argument for self-care. As noted above, emotions are integral in this process. Many people experience feelings of guilt and selfishness that must be overcome in order to make a decision in favor of self-care. 20 The emotional component of the self-care process remains present even when people deal with more tangible hindrances to the practice of self-care. Therefore, you must keep in mind that as other barriers to self-care appear, you will still be contending with a variety of feelings that discourage you away from self-care or encourage you toward self-care.
Discipline can be a hurdle that influences one’s decision and implementation of self-care. Because self-care is intentional, an individual must also have the discipline to be intentional about it. 21 Other challenges that can inhibit one’s ability to implement self-care include dealing with responsibilities, planning self-care, thinking about how self-care affects other people, especially family, lack of finances, anxiety, expectations, stage of life, houseguests, not comparing yourself with others, and seeking outside counsel.
Finally, there will always be things that are not planned or situations that are not in one’s control, such as being sick or additional work commitments. When that happens, even if a person has established a self-care routine, it can take some time to get back on track once the schedule has been disrupted. Stopping, pausing, and restarting self-care practices is determined by what happens in the next step: the decision to implement or not implement self-care. Like so many other areas, this is not a casual decision-making process as it involves many of the factors described above and might also look different each time a person reaches the crossroad point. Once again, since this part of the self-care process is connected to the others, there will be some overlap with steps four and six during the discussion of step five.
Decision regarding implementation of self-care—step five
When faced with decisions, there are levels of ease and difficulty depending on the situation one is confronted with, the feasibility to make it happen, and preferences of the person making the decision. If someone is deciding what to eat for dinner, some choices might be eliminated based on one’s predilection for a certain kind of food. Other choices might be more or less viable depending on the food one has in the house or willingness to spend money on take out or eat in a restaurant. Dealing with the issue of self-care, these same considerations are present on a much broader scale.
An important distinction must be made about the decision-making process of this step. Whether a person chooses “yes,” “yes but,” or “no” as their decision, the decision is not to self-care itself but rather to implementing self-care practices and strategies at that time. The decision about implementation should not be misunderstood as a decision for or against the importance of self-care or the need for self-care. 22 Nonetheless, believing something should be practiced and practicing it are not the same, and this step discusses how to deal with that difference. 23
The choices of “yes,” “yes but,” and “no” will be elucidated below. It is difficult to break them into separate parts since there are so many conditions that influence how one comes to a decision. Choosing between “yes,” “yes but,” and “no” links back to the experiences and barriers of step four. Even when someone says “yes” to implementing self-care it usually means that they are saying no to something else. In that case, saying no is not comparable with the “no” decision that you make at the crossroad of steps four and five. The decision to say “yes” to self-care leads into the implementation of self-care that corresponds with step six. While most of the self-care strategies will be addressed in that section, the dynamics of saying “yes” to self-care means “saying no” to something else will be addressed here because there is such an integral connection to the “yes” decision.
Yes
When a person makes a choice to go in one direction, it means that person cannot simultaneously go in the opposite direction. The same is true when you decide to say “yes” to self-care. The other responsibilities that a person faces do not simply take care of themselves because a person is utilizing self-care but there will come a point when an individual needs to say “yes” to self-care in order to be there for others. In order to decide “yes” for self-care implementation, one must also determine what types of situations constitute the need for more self-care and be willing to see it as a priority. Included in this “yes” decision is the understanding that each individual knows best what he or she needs. For some, it is seeking out friends and family to connect and rejuvenate, whereas others find it is helpful to spend time alone. Both situations constitute a “yes” to self-care but they differ in application.
As previously mentioned, the “yes” decision to implement self-care does not conclude one’s self-care journey. Each person must regularly reaffirm the “yes” decision each time a crossroads is reached. It would be ideal if an individual could make the “yes” decision every time but there are circumstances that make that an impractical expectation. Much the same way that you must give yourself permission to engage in self-care, you must also have the freedom to decide “yes but” so as to prevent self-care from becoming one other thing on the to-do list, making it a burdensome task rather than a healthy undertaking.
Yes but
Balancing acts are complex. Imagine a server brings two serving trays of food to a table. When they are equally laden, the weight distribution enables the server to maneuver through the restaurant. Very often what happens when the server reaches the table is that the trays are relocated from the server’s palm to a stand, to allow the server to distribute the plates without disrupting the equilibrium of the trays. If prior to placing the trays on the stand, another server begins taking plates off the trays without the first server’s knowledge or before the server is prepared or able to react, one can visualize what might happen. The weight that was keeping the tray balanced in the server’s hand will shift, often leading to a problematic outcome. While not an exact comparison, the picture of the server’s balance and imbalance holds true for the decision-making process of self-care. You must have a level of awareness regarding how much you can handle, when to add more to your plates, and when to take some away. Even well-meaning help from friends and family can cause a sticky situation, especially when the balance is newly acquired or you are unfamiliar with what lies ahead. In this respect, one can begin to comprehend how someone might choose the “yes but” option, as it gives them the time and space to adjust to the variables before transitioning into the “yes” that allows them to implement self-care.
Taking a closer look at the “yes but” decision of the self-care cycle, the diagram (Fig. 1) displays how a person might spend time regaining the balance that is needed to get back on the road to implement self-care. When someone loses their balance, it throws them off kilter and it takes time to reorient oneself before being able to proceed. Suppose that a person has been practicing self-care (step six) but reaches a point where they have a more intensive workload (step four). The pace that is required to complete this workload is demanding, leaving the person depleted in the five areas of their physical, mental, emotional, spiritual, and relational realms. The desire to do self-care is present, which lends itself to a “yes” decision but the person also has a sense of being overwhelmed and discouraged, both at the workload and their inability to continue the self-care practices that had previously been so refreshing. Consequently, the person makes a “yes but” decision for implementing self-care. Much like the server at the restaurant, the person cannot add something to an already full plate but also recognizes that this decision allows for a holding pattern of self-care until things change. Being proactive in recognizing the physical toll that a “yes but” decision is having on you could make it easier to transition into a “yes” decision that benefits you.
Before moving to the third decision that people can make, it is important to revisit the overarching feature that brings the process together. At the heart of soul care is self-care. The core of this model emphasizes that the application of self-care is not a sprint, but a marathon without a definitive finish line. People will find themselves at different points in the journey and may regress or progress, depending on a set of criteria and circumstances that is unique to each person. With that being said, it can be understood that when someone makes a “no” decision for implementing self-care, it is not the end of self-care or soul care for that person, nor is it the end of the process.
No
Much like saying “yes” to self-care meant “saying no” to something else, people will come upon situations where their “yes” to the situation also means “no” for implementing self-care. While it might be easier to suggest that people will choose “yes” and “yes but” given their understanding of the importance of self-care, the truth of the matter is that people who choose “no” also believe that self-care is important. However, it might take a longer period of time before they change their decision, such as when their lack of self-care propels them back into doing it again. Deciding “no” to implement self-care will catch up to people eventually. On some occasions, people will transition to a “yes” before reaching a point of burnout but they will still have experienced some problems.
When people choose “no” as their self-care implementation decision, they should not be viewed as inferior or ignorant. The longer they remain affixed to the “no” decision, the more the effects will be felt throughout their being, impact their work and become noticeable to others. People who choose to enter a helping profession, such as marriage and family therapy doctoral students, pastors in churches, and others in ministry settings, recognize that they need to be present when they are helping others. On some occasions, we might not even realize that we shifted out of saying “yes” to self-care practices and into a “no.” Because we have the right intentions, the “no” decision happened gradually as people required additional care or it became harder to focus on their needs because of our own weariness.
Overall, students and professionals will make each one of these decisions at different points in the journey. Even though they receive the most benefit from saying “yes” to implement self-care, the other options connote the practicality of the sustainable balance that we desire. Along with being proactive and intentional, self-care must continue to be something that is life-giving rather than life-draining. If self-care becomes a burdensome task on the to-do list, it has switched from being a freeing process to being its own deterrent.
One final illustration can shed light on this step in the journey. If the way to get to a friend’s house is for the driver to head east, the driver will do just that. Yet when the car reaches the halfway point, the driver sees a tree blocking the road ahead. The tree should not be viewed as a malicious obstacle but rather an unintended result of bad weather. Essentially, the driver had been implementing (step six) the path that would bring the car to the friend’s house but could no longer continue as planned because of the tree (step four). If this is the only way to the friend’s house, the driver may be forced to turn around and wait until the tree has been removed. In that case, the driver would have made a “no” decision (step five) because there were no other options available. Additionally, the driver could decide that even if there are other routes to visiting the friend, there are other things that take priority, leading the driver to stay with the “no” decision (step five). As time goes on, though, the driver might find that the friendship is missed, which moves the decision out of the “no” category and into one of the others. Perhaps the road that will take the driver around the tree will add a lot of time to the trip. The driver might decide to delay visiting the friend until another day when more time is available to take the alternate route. This would be considered a “yes but” decision (step five). However, the driver might be in a position where this visit was planned and has been anticipated for some time. In this case, the driver is willing to drive through the north-west-south detour that will bring the car to another eastward road. The “yes” decision (step five) demonstrates that even though the driver has other concerns, getting to the friend’s house is significant enough that it is worth dealing with the inconvenience to get around the tree.
Having studied the numerous routes of the decision-making process, the journey moves to the sixth step of the self-care process. This step is purposefully not labeled as the final step because there will always be a return to steps four, five, and six throughout one’s life. However, when people do choose to implement self-care, they open themselves up to a wide range of life-giving strategies, rewards, and motivations that can serve as an encouragement for continuing to make self-care a priority throughout their lives.
Implementation of self-care—step six
At this point in the process, the “yes” decision has been made to implement self-care. When this happens, you will experience the physical, mental, emotional, spiritual, and relational rewards that it brings. Since implementing self-care strategies is different for everyone, it is important that each person find out what works for them. 24 Nonetheless, there are some commonalities in self-care practices that might provide insight into some of the more readily available options people would want to consider when they implement their own self-care.
Returning to the holistic definition of self-care that addresses the physical, mental, emotional, spiritual, and relational components, most people can specifically identify physical, spiritual, and relational practices that have the mental and emotional pieces woven into them. Physical activities vary from person to person but, again, part of making self-care work for an individual is being able to discover what an effective practice is. Spiritual disciplines such as reading the Bible, going to a worship service, or starting the day with meditation and prayer can allow people to release their stressors in a different venue than the physical expressions. Connecting with others is also a significant self-care practice. One of the benefits of these relationships is having people who can encourage you when you are struggling or who help to normalize what you are feeling. It can be valuable to do little things like lighting a candle or writing in a journal. Finding little things and little blocks of time that work for you is part of how you can make time for self-care because self-care does not have to be an elaborate plan that consumes a sizeable part of the day. Objective tasks like cooking, sewing, or redecorating a room can be beneficial, especially for those in helping professions because, unlike other areas of life, these are things that have a clear start and end mark. The list could go on but ultimately, each person needs to find the strategies that fit with their needs.
The sixth step connotes that an individual is implementing one or more self-care strategies. Having incorporated a certain degree of self-care into one’s life does not constitute total achievement but instead suggests that an individual remains in the process of continual achievement. Employing more than one strategy can prove to be beneficial when reaching certain roadblocks that bring a person back to confront steps four and five. A concluding example of how someone on the sixth step will travel forward to a certain point before encountering steps four and five brings this process full circle.
Physical activity is one of the most commonly cited methods given by people as a self-care strategy, so it will be used in this illustration. 25 Whether you are a practitioner of yoga, Zumba, or prefers walking, jogging, or running, it is possible that a physical setback could be caused by the activity itself, such as a twisted ankle or a knee injury. Therefore, a person can be in the midst of self-care (step six) when the activity inadvertently requires the person to stop what is being done (step four) before the injury becomes greater. Once again, the barrier to self-care is not intended to be negative or destructive but it does require the individual to reevaluate how to proceed. The decision-making process is subject to the desires of the person making the decision. If physical activity was the sole self-care skill applied by that individual, the decision is not automatically “no” because there is still the option of learning or using other methods, especially while the injury heals. However, depending on what else the person is balancing at that time, the decision to implement self-care might be “no” (step five), especially if it seems like other activities do not offer the same degree of self-care relief or support offered by the physical actions.
A person might decide that self-care will not be derailed by the injury and enter the circle with a “yes” decision in mind. Yet, the injury could require more attention than what the person originally supposed, leading the person into a few revolutions in the “yes but” decision (step five) circle. The “yes but” decision is chosen by people who do not have other self-care skills in their repertoire and by those that do. The reality is that things like health complications, unexpected visits from friends and family, additions to the to-do list, or phone calls from someone who urgently requests help can and will have ripple effects that cannot always be accounted for and dealt with at that time.
Finally, the person is understandably frustrated by the physical inhibition but determines to continue with other forms of self-care, choosing “yes” (step five). This person can be earlier in the journey or further along but realizes that self-care must be done even more now that the injury has brought a disruption to normal everyday undertakings. With the injury, it will take longer to get up and down the stairs at home, to get ready for work and school, even getting in and out of the car. Energy that is usually available to deal with normal aggravations will be expended dealing with the ordinary routine. The reasoning behind why this individual might choose to continue implementing self-care also differs based on previous life experiences and the emotional outlook of the person.
Curriculum activities
The model is the essence of my teaching curriculum. With some populations, I will spend time in steps one through three, examining the underlying assumptions that led to current beliefs and values about self-care. However, most groups want to give attention to the last three steps, and how they can implement self-care. Two of the primary methods that I use to accomplish those goals are small group discussions and self-care activities. First, in the small groups, people respond to the following questions: Describe one or two of your current self-care practices. What are 1–2 of the most challenging aspects of incorporating self-care into your life? What are 1–2 of the most effective or rewarding aspects of incorporating self-care into your life? What would you recommend to others to help them with incorporating self-care into their life? If you had the opportunity to incorporate 1–2 aspects concerning self-care into [your specific context], what would they be?
Questions are tailored to the target population, but the five questions listed above get to the heart of the matter. The small group conversations allow people to connect with one another and recognize that they are not alone in trying to implement self-care strategies.
Second, I offer an opportunity for people to engage in five intentional self-care activities that touch on the five domains: physical, mental, emotional, spiritual, and relational. I use these activities to bring the material to life and to appeal to different learning styles. The first activity addresses physical self-care. Depending on the location, I have five stations arranged in the room. Each station has a sheet of paper with the word “physical,” “mental,” “emotional,” “spiritual,” or “relational” written at the top of it. Those in attendance are split into five groups; usually four–six people is the maximum number for a group. If there are more people in attendance, duplicate stations are set up to keep the subgroups in smaller numbers. Upon arriving at a station, the group is given a colored pen or marker that they will stay with their group and they are asked to come up with as many strategies as they can think of that fall under their topic. It is a time-limited activity, and participants are encouraged to write down all ideas, rather than debate if it belongs in another category.
After about two minutes, each group switches stations and brings their colored pen or marker with them. Ideally, they can move from one station to another without confusion about which stations have been completed. If this doesn’t happen, they look at the sheet to see if their color has already been used and they know that they need to switch with another group. Upon arriving at the new station, the group is prompted to respond as if there is nothing on the page, rather than to read what other groups have written. This keeps things moving and fosters creativity. After all groups have completed each station, everyone comes together and shares a few items on each list. Before proceeding to the next step, I collect all the papers and ask the whole group for permission to take what they’ve written and combine it into one document which I will return to them soon. While I make sure to request permission from the whole group and stipulate that I will not compile the list if anyone is uncomfortable, I have yet to have someone be opposed to it. The list allows each person to have an immediate resource of self-care strategies that they can use, which might provide ideas that are different than what one person would think of on their own. The activity itself allows for physical movement that is not overly strenuous and it serves as a reminder of the benefits of physical self-care. I have other activities that I use for physical self-care, however, this one remains the most popular.
The second activity addresses emotional self-care. When I teach on emotional self-care, people often turn to consider their feelings of selfishness and guilt over practicing self-care. Processing this is helpful to a point but a group setting is not always the best place to do it unless that is the purpose of the meeting. This is where laughter can be a great asset. Since there is a time to weep and a time to laugh 26 and a merry or cheerful heart is good medicine, 27 I have several comedy clips that I draw from; I play portions of them for each group. Individual and corporate laughter have healing properties. Even remembering one joke and laughing about it later is an example of a brief form of self-care.
Mental self-care is the third activity; sometimes I pair this with spiritual self-care, especially in Christian contexts. I use a deep breathing or a mental imagery exercise. 28 I tend to stray from the script and adjust to what seems to most fit the audience, rather than using the same instructions with everyone. The underlying principle is to give their minds a mental break. If I use this activity with spiritual self-care, I will invite them to stay in that place of calm if it is refreshing or give them permission to leave it and make plans to come back and visit it another time. During spiritual self-care, a song is played, and the words are available for anyone that wants to learn it for the first time, or to follow along and sing. Some people use this time to pray or worship. I have had several people start to sleep when the two are paired together, which speaks to the efficacy of the activity.
The final activity is focused on relational self-care. I believe this one is especially important for groups that are going to be together in other contexts outside of our meeting, especially students that take classes together or people that attend church together. Each person is given a handout, which asks them to find one or two people who share certain things in common with you or have certain likes or dislikes. What I like about this handout is that the primary focus is not on finding someone that has things in common with you but, instead, it is learning about others and building relational connections. For those looking to adapt this activity, there are icebreaker activity books that can provide a range of options. 29
Implementation
Terminology such as right and wrong or good and bad is often applied in discussions regarding what people do and how it should be done. Some people are still at the fourth step of the process and it is only a matter of time before they are confronted with a step-five decision for how to proceed in the step-six implementation of self-care. If this is the case, they should not be viewed as wrong, bad, or incompetent; they are not at a point where they fully grasp the efficacy of self-care, thus their own self-care approaches are, at best, limited and, at worst, ineffective. These people are only beginning to venture down the path of self-care.
Likewise, when people have undergone experiences that have influenced their beliefs about self-care so that they are already implementing it, these people are not superior to their peers; they are simply at a different point in the journey which has enabled them to begin taking advantage of the benefits of self-care earlier in their lives. They are still susceptible to the roadblocks and barriers of the process and will likely have times when they need to reincorporate the skills they already know and learn new ones to help self-care become more deeply ingrained. The beliefs that they have cultivated about self-care will continue to undergo refining and adjusting with other life experiences. Helping each individual to grasp that there is movement to the self-care process will allow them to identify where they are in the journey, rather than feeling as though they have failed, if they are not currently implementing self-care, or losing intentionality in their approach, if they are implementing self-care. To be clear, self-care certainly has the potential to be applied in a reparative fashion, but it is preferable to engage in self-care proactively. The same logic applies when considering that a child can ride a bike in one of two ways: with protective gear or without it. If the child falls off the bike without protective gear, bandages can be applied to make the child feel better, but the bumps and bruises will have to be dealt with in the days to come. However, if the child wears the protective gear and falls off the bike, the damage is minimalized, making it more likely that the child will get back on the bike sooner and be more likely to use the protection next time.
In addition to the self-care model and curriculum previously described, which includes steps four through six that address self-care implementation, I have implemented other self-care checkpoints, which have been primarily used with my doctoral students. Each new cohort that enters our program receives a self-care seminar within the first two weeks of the program. This seminar covers the self-care activities and briefly covers the model. After one year in the program, I discuss the self-care model in more detail and have some type of self-care debriefing for the cohort. At this point, students usually answer the questions that are given to small groups. Later in their second year, students write a paper that addresses ethics, self-care, and faith. The paper examines both the way that self-care is understood in their value system, and their plans for implementation. In their third and fourth year, as they begin working on their culminating assignment, students are asked to informally report on the status of their self-care. These informal reports are provided in group meetings and one-on-one meetings. Using the model as a guide, we examine the barriers to self-care and where students are in step five, saying yes, yes but, or no. The purpose is to keep self-care on their radar, not to elicit feelings of guilt or shame.
Assessment and evaluation
Assessing the effectiveness of the curriculum is a work in progress for two reasons. First, the self-care model that I use was not developed to create a curriculum but rather to understand what people were doing and why. Thus, I have been seeking to raise awareness about self-care, without fostering some of the counterintuitive messages that people are already facing. Second, I do not want self-care to become a “to-do” list item that derails its efficacy in people’s lives. When I speak to someone who feels guilty about not doing their “self-care activity” much like they feel guilty about not finishing an assignment by the deadline, chances are that the self-care activity is one more thing to do, instead of something that brings life.
Nonetheless, I regularly receive positive feedback on the self-care model and curriculum. Whether it is students in the doctoral program or people in churches and other ministries, the self-care strategy list that is compiled during the physical activity has been cited as an effective resource. Others have expressed appreciation for keeping self-care in the forefront of their thoughts, especially if they are in a “yes but” holding pattern. With my students in particular, I hear them talking about self-care more as they progress through their studies. I would like to find other ways to assess the efficacy of the self-care model without having it become an evaluation.
Conclusion
Self-care is best understood and enacted when it is intentionally and proactively integrated throughout the physical, mental, emotional, spiritual, and relational aspects of our life. The key to this integration originates in each person’s belief system about self-care. When self-care is seen as a Band-Aid, it is used like a Band-Aid: to address impairment and protect the individual until the recovery is complete, at which time the Band-Aid is discarded. People with this mentality will still work through the self-care cycle but will remain affixed to an earlier point in the journey until such a time as they are forced to reevaluate their self-care beliefs.
The belief system about self-care for others might be akin to sunscreen: the benefits are well known but it must be applied to receive the protection that it gives. Using self-care in this way, there will be times when it is easier to apply and times when it seems like a nuisance to a more pressing activity. If it seems like a nuisance, the next sunburn will remind an individual of the relief sunscreen brings. Conceivably, people do not have to experience sunburn firsthand to recognize the impact it has on others; if this happens, they are more willing to make adjustments to their self-care beliefs and continue further along in the journey.
Ultimately, the significance is best understood by those who have a self-care belief system that views it as the seatbelt in the car, the mitts used to remove food from the oven, and the bulletproof vest worn in combat. The seatbelt, mitts, and vest do not preclude the possibility of injury but, every time they are worn, they reduce the amount of harm that can be done. When something does happen, the damage is less severe and it reinforces the likelihood that the person will use it again in the future. As we come to believe in the value of self-care, physically, mentally, emotionally, spiritually, and relationally, we recognize that each step in the process helps us to live out the greatest commandments—to love God with all our heart, soul, mind, and strength and to love our neighbor as we love our “self”! 30
Footnotes
Acknowledgements
This model was first developed as a way of understanding the process that graduate marriage and family therapy students take to incorporate self-care into their professional development. It has since been adapted to use with other populations. I am grateful to my dissertation chair, Dr. Gwen White, for her invaluable guidance and wisdom, and to my committee members, Dr. Francesca Nuzzolese and Dr. S. Timothy Pretz, for their time and assistance.