
Abstract
Background:
Pulmonary dysfunction in individuals with post-coronavirus disease-2019 (COVID-19) syndrome may impair aerosol deposition and pulmonary perfusion, compromising respiratory efficiency. Inspiratory muscle training (IMT) has been proposed as a strategy to improve respiratory mechanics and lung function.
Objective:
To compare aerosol deposition and pulmonary perfusion in individuals with post-COVID-19 syndrome before and after 8 weeks of IMT.
Methods:
This was a randomized controlled clinical trial involving 19 participants, divided into an IMT group (n = 10) and a control group (n = 9). The IMT group performed training with a load adjusted to 50% of maximal inspiratory pressure, while the control group used a device without resistance. Aerosol deposition and pulmonary perfusion were evaluated by gamma scintigraphy using the radioisotopes technetium-labeled diethylene-triamine-pentaacetic acid and technetium99-labeled macroaggregated human serum albumin, respectively. Total radiopharmaceutical activity in both lungs, as well as in the right and left lungs separately, was quantified pre- and post-intervention.
Results:
After 8 weeks, the IMT group showed a significant increase in total lung activity for both aerosol deposition (p = 0.028) and perfusion (p = 0.013). In the right lung, activity increased significantly for aerosol deposition (p = 0.005) and perfusion (p = 0.005). In the left lung, significant increases were also observed for perfusion (p = 0.007). No significant increases were observed in the control group. In the between-group analysis, the IMT group showed higher activity in both lungs combined and separately, compared with controls, for aerosol deposition (all p < 0.05) and in the right lung for perfusion (p = 0.010).
Conclusion:
IMT improved total aerosol deposition and perfusion in individuals with post-COVID-19 syndrome. These findings support the use of IMT as a rehabilitation strategy to enhance pulmonary deposition of inhaled agents and increase pulmonary perfusion in this population.
Keywords
Introduction
Pulmonary complications associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection can persist or develop even after initial recovery, varying in severity and clinical presentation, with a significant long-term impact on lung function. These complications may affect treatment due to the challenges in optimizing the administration of aerosolized medications and respiratory therapies. 1 In addition, pulmonary microcirculation dysfunction has been identified as a severe complication, contributing to hypoxemia and other respiratory impairments.2–4
Recognizing the variability of post-coronavirus disease 2019 (COVID-19) effects, personalized treatment has emerged as a crucial approach. Detailed mapping of patients’ pulmonary conditions has been deemed necessary for the development of targeted therapeutic strategies. This process includes the integration of clinical research, imaging studies, and histopathological analyses, enabling a deeper understanding of pulmonary deficiencies and underlying mechanisms.5–7 Specific studies on the behavior of radiopharmaceuticals during inhalation and perfusion testing in post-COVID-19 patients are lacking. In addition, inhalation therapy is known to offer significant advantages, such as higher drug concentration at the target site with lower doses, reducing side effects and promoting better therapeutic outcomes compared with other routes of administration.8,9
Additional therapeutic strategies, such as inspiratory muscle training (IMT), have demonstrated benefits in pulmonary function across various clinical conditions.10–15 IMT enhances respiratory muscle strength and endurance, reduces dyspnea, and improves functional capacity and quality of life. However, the effectiveness of IMT in individuals with post-COVID-19 syndrome remains unclear due to discrepancies in study results.16,17 Nevertheless, its therapeutic potential justifies further investigation.
The present study aimed to compare the pulmonary distribution of radiopharmaceuticals in post-COVID-19 individuals before and after 8 weeks of IMT. We hypothesized that IMT would increase aerosol deposition and improve perfusion, as evidenced by changes in radiopharmaceutical activity patterns.
Methods
Study design and ethical aspects
This study was a randomized controlled clinical trial, approved by the Research Ethics Committee of the Federal University of Pernambuco under protocol No. 4.983.173 and registered at clinicaltrials.gov (ID: NCT05282199).
The study was conducted in accordance with the CONSORT and CONSERVE guidelines.18,19 All participants received visually identical devices and were explicitly instructed not to open or manipulate them. Resistance load adjustments were performed by an investigator in a separate location, out of the participants’ view. These procedures were designed to minimize any perceptual cues that could reveal the presence or absence of inspiratory resistance.
Setting and participants
The study was conducted between October 2022 and March 2023 with individuals diagnosed with post-COVID-19 syndrome. A convenience sample was composed of individuals who sought care at major referral centers due to persistent post-infection symptoms. Recruitment was carried out through direct outreach and social media.
Volunteers of both sexes, aged over 18 years, who were not engaged in any form of physical activity, and who had been diagnosed with COVID-19 after the acute phase of the infection, were included. Their first infection had to be confirmed by reverse transcriptase polymerase chain reaction testing. Exclusion criteria included individuals with a history of pre-existing conditions before COVID-19 (i.e., orthopedic, neurological, uncontrolled cardiovascular or pulmonary diseases), pregnant women, and individuals in the active phase of infection.
Volunteers were classified according to the severity of post-COVID-19 syndrome, considering the severity, intensity, and persistence of symptoms after acute infection. A severity score was calculated based on self-reported symptoms, using a questionnaire composed of 12 symptom sets: chemosensory deficits, fatigue, exercise intolerance, joint or muscle pain, ear-nose–throat conditions, cough/wheezing, chest pain, gastrointestinal disorders, neurological conditions, dermatological diseases, signs of infection, and sleep disturbances. When a symptom from any of these sets was present, the indicators were multiplied by an individual point value, reflecting their contribution to the categorization of post-COVID-19 syndrome severity. The sum of the assigned points generated a total score, allowing for classification of severity into the following categories: none (0 points), mild (>0 to ≤ 10.75), moderate (>10.75 to ≤ 26.25), and severe (>26.25). 20 Baseline characteristics, including age, weight, height, gender, body mass index, time since COVID-19 infection, comorbidities, medications, and history of hospitalization, were recorded for participants in both groups.
Randomization and blinding
Block randomization was performed using the software Randomization.com, with a 1:1 allocation ratio between the IMT and control groups. A researcher, who was not involved in any other part of the study, generated the randomization sequence and assigned participants using sequentially numbered opaque envelopes, ensuring allocation concealment. Participants were randomly allocated to their respective groups and received training according to their assigned group. Initial and final assessments were conducted by an evaluator who was blinded to the participants’ group allocation and the type of intervention applied. Blinding was implemented to minimize biases. Only the researcher responsible for load adjustment was aware of the participants’ allocation, and measures were taken to standardize the adjustments and prevent any influence on blinding. Participants were assigned to the following groups: control group (n = 9): Participants in this group performed IMT for 8 weeks using a Powerbreathe® device without the internal spring installed. IMT group (n = 10): Participants in this group received the Powerbreathe® device and performed training with a load adjusted to 50% of their maximal inspiratory pressure (PImax) for 8 weeks.
Before participating in the study, invited volunteers were provided with detailed information and signed an informed consent form, agreeing to their participation. Both groups were evaluated weekly at the laboratory in individual sessions with the researcher responsible for load adjustments; however, only the intervention group received incremental load adjustments.
Scintigraphy
Inhalation
For inhalation, a mesh nebulizer (Aerogen® Solo, Aerogen Ltd., Galway, Ireland) was used. According to the manufacturer’s specifications, this device generates particles of 3.0–4.5 µm with a geometric standard deviation of 2.0 and has a reported residual volume of < 0.1 mL for a 3 mL dose. The 1.5 mL inhaled solution contained technetium-labeled diethylene-triamine-pentaacetic acid (99mTc-DTPA) with an activity of 5 mCi, mixed with 0.9% saline solution. The inhalation circuit consisted of the following components: a mouthpiece, a Y-tube, a mesh nebulizer, an expiratory filter, and a nasal clip. 21 Radioaerosol inhalation was performed with the nose-clipped individual in a seated position for 4 to 5 minutes. Participants were instructed to breathe slowly and deeply through the mouth, maintaining a 3-second inspiratory pause in each breath. The nebulization was stopped when no aerosol was visible escaping from the mouthpiece, indicating that the inhalation process was complete. This procedure was consistently followed for all participants during each visit to ensure uniformity across the study. After inhalation, participants were advised to rinse their mouths and drink water to clear any radioaerosol deposits in the throat and esophagus. A lung scan was performed immediately following radioaerosol inhalation (see section on Image Acquisition for details).
Perfusion
Following the post-inhalation image acquisition, an intravenous injection of a 0.5 mL solution containing 99mTc-labeled macroaggregated human serum albumin (99mTc-MAA) with an activity of 5 mCi, mixed with 0.9% saline solution, was administered. The patient remained in a supine position, entering the scanner feet-first, with the right arm extended and supported. The solution was administered via the right cubital fossa. The preparation and intravenous administration of the radiopharmaceutical, prior to the perfusion image acquisition, lasted ∼20 minutes.
Image acquisition
Each participant underwent two imaging sessions, one before (pre-intervention) and one after (post-intervention) the 8-week study period. All scans were acquired using a dual-head detector gamma camera (NM830, GE Medical Systems, Israel). For aerosol deposition assessment, planar 2 D scintigraphy was performed immediately after inhalation of 99mTc-DTPA using a mesh nebulizer (Aerogen® Solo, Galway, Ireland). The acquisition included anterior and posterior views, with a 256 × 256 matrix, a zoom factor of 1.33, and a 300-second acquisition time per projection. The distance between the thorax and detector was standardized at < 10 cm. For perfusion imaging, following intravenous injection of 99mTc-MAA (5 mCi in 0.5 mL saline), images were acquired using the same camera settings, except for a shorter acquisition time (150 seconds per projection). 22 All image acquisitions were conducted under resting conditions. The full inhaled volume (1.5 mL) was delivered in each case, with total inhalation time varying slightly (4–5 minutes) according to individual breathing pattern. The procedure was considered complete only after total nebulization of the dose.
Total counts corresponded to the sum of the activity recorded across all regions of interest, including pulmonary, trachea, oropharynx, stomach, and circuit components. Pulmonary counts (total, right, and left) were then expressed as a fraction of the total counts, representing the activity retained in the lungs relative to the total activity. Activity in the trachea was excluded from the pulmonary counts. Counts were combined using the geometric mean of the anterior and posterior projections to minimize the depth/attenuation effect on planar images.
To ensure differentiation between the counts associated with 99mTc-DTPA aerosol inhalation and those associated with 99mTc-MAA intravenous injection, we compared the counting rates of the two procedures. The counting rates for the total lung and the right and left lungs separately following perfusion (99mTc-MAA) were ∼3–4 times higher than those recorded following inhalation (99mTc-DTPA), consistent across participants. This difference in counting rate provided a clear distinction between the two acquisitions, minimizing the risk of overlap between inhalation and perfusion signals. 23 No background correction was applied.
Training protocol (IMT)
Participants performed moderate-load inspiratory training, set at 50% of maximal inspiratory pressure (MIP), with weekly adjustments during in-person visits to the laboratory over an 8-week period. The training was conducted using the PowerBreathe® Classic Light device (HaB International Ltd., Southam, UK), which was calibrated according to the manufacturer’s specifications prior to the start of the intervention to ensure accurate and consistent resistance levels. In the control group, the internal spring of the device was removed, ensuring no resistance to inspiratory flow throughout the 8-week period. Training sessions were performed in a seated position, with knees and ankles flexed at 90°, feet flat on the floor, one hand holding the device, and the other resting on the leg. A nasal clip was used to prevent air leakage. The IMT protocol consisted of three cycles of 30 maximal and rapid inhalations, performed against a predefined resistance using a threshold loading device, with a 1-minute rest interval between cycles. Participants were instructed to perform the sessions twice daily, 7 days a week, over a period of 8 weeks. 12 Each inspiratory effort was to be executed from functional residual capacity to total lung capacity as explosively and forcefully as possible, with emphasis on speed and maximal effort, aiming to recruit fast-twitch inspiratory muscle fibers. Adherence to the protocol was closely monitored through weekly in-person visits and reinforced by structured telephone follow-ups. During each visit, a training diary was reviewed, and participants’ reports were cross-checked to ensure compliance. Adherence was considered satisfactory when participants completed at least 80% of the prescribed sessions over the 8-week period. Inspiratory muscle strength was reassessed weekly using MIP measurements, and the training load was adjusted accordingly (i.e., typically recalibrated to 50% of the newly measured MIP) to ensure progressive overload and individualized training intensity. After completing the training period, all individuals were reassessed using the same instruments and protocols as in the initial evaluation. All assessments were conducted by the same evaluator to ensure intra-rater reliability and consistency in data collection. Peripheral oxygen saturation (SpO2) was assessed using a validated digital pulse oximeter under resting conditions. Measurements were performed twice: once at baseline (prior to randomization) and once immediately following completion of the 8-week intervention period.
Outcomes
The primary outcome was the change in pulmonary radiopharmaceutical activity, expressed in kilocounts (Kct), measured by inhalation and perfusion scintigraphy. Analyses were performed considering total lung counts as well as right and left lungs separately, comparing pre- and post-intervention values. Secondary outcomes included changes in SpO2, inspiratory muscle strength, and the incidence of adverse events during the training period. All outcomes were prospectively defined in the study protocol and registered prior to participant enrollment (ClinicalTrials.gov ID: NCT05282199).
Sample size
The sample size calculation was performed using an a priori analysis with G*Power 3.1.9.7, based on a previous study conducted by our team that investigated the effects of IMT in a distinct population. At the time the present study was designed, no data were available regarding the effects of IMT in individuals with persistent post-COVID-19 symptoms; therefore, the previous trial was used as the best available reference. In that study, after 8 weeks of IMT, maximal inspiratory pressure (MIP) increased from 83.6 ± 26.6 cmH2O at baseline in eight subjects to 127.9 ± 32.5 cmH2O, corresponding to an absolute mean gain of 44.3 cmH2O and an approximate 53% increase in inspiratory muscle strength relative to baseline. Over the same period, the placebo group of eight subjects showed an ∼15% increase in MIP (from 74.6 ± 25.4 cmH2O to 86.0 ± 23.9 cmH2O), yielding an estimated net advantage of ∼38% in favor of IMT. These between-group differences in MIP were used to define the expected effect size for the present trial, which was calculated to be 1.4688, corresponding to a large effect size. To account for the sample size with nine participants per group, this effect size was maintained, ensuring the ability to detect statistically and clinically significant differences. To ensure robust detection of effects, a significance level of 5% (α error) and a power of 90% (β error = 10%) were adopted, in accordance with standard statistical guidelines. Considering a dropout rate of 15%, the final sample size was adjusted to a minimum of 18 participants, with 9 participants per group.
Statistical analysis
Data analysis was performed using SPSS® version 20 (IBM Corp., USA). Data were assessed for homogeneity and distribution using Levene’s test and the Shapiro–Wilk test. To compare baseline characteristics between groups, the Mann–Whitney U test was applied. For within-group comparisons (pre- and post-intervention), the Wilcoxon signed-rank test was used to assess changes in total lung activity, as well as in the activity of the right and left lungs. Between-group differences in activity between the IMT and control groups were evaluated using the Mann–Whitney U test. Oxygen saturation (SpO2) changes were compared between the groups using the Mann–Whitney U test. Results were reported as medians, median differences with interquartile ranges (IQR), and effect sizes (r). The analysis of inspiratory muscle strength employed the Mann–Whitney U test for between-group comparisons, and the Wilcoxon signed-rank test for within-group comparisons. A significance level of p < 0.05 was applied, and effect sizes were interpreted according to Cohen’s criteria: very small (0.1), small (0.2), medium (0.5), and large (0.8). 24
Results
Figure 1 illustrates the process of participant recruitment, randomization, and allocation.
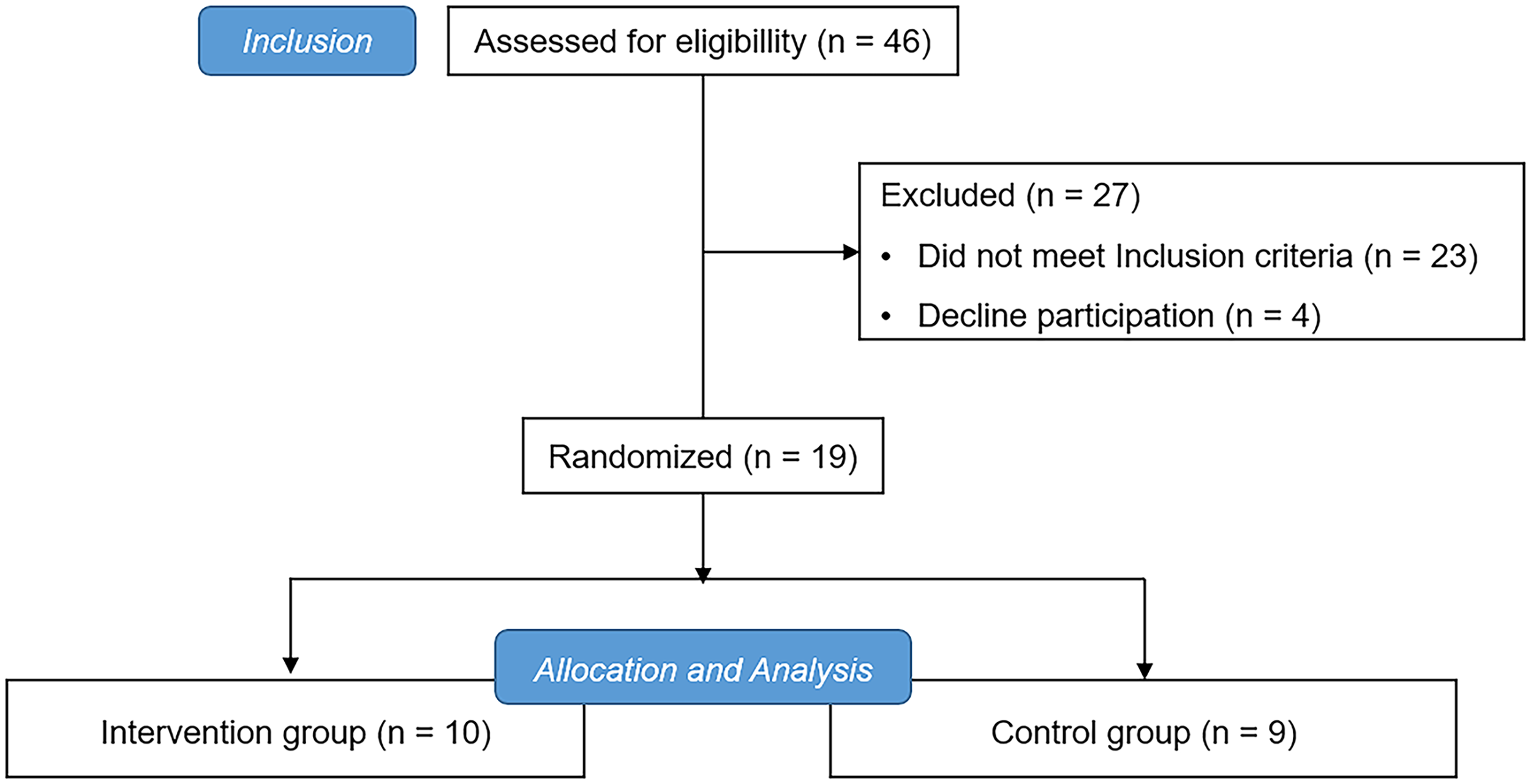
The study flowchart.
A total of 19 patients participated in the study, with 10 in the IMT group and 9 in the control group. The training program was well tolerated. A higher proportion of female participants were observed, accounting for 90% in the IMT group and 66.7% in the control group. The proportion of moderate and severe cases was identical in both groups, with 40% in the IMT group and 33.3% in the control group for each severity level. Only two individuals in each group reported having obstructive lung disease (Table 1).
Baseline Characteristics of Participants in IMT and Control Groups
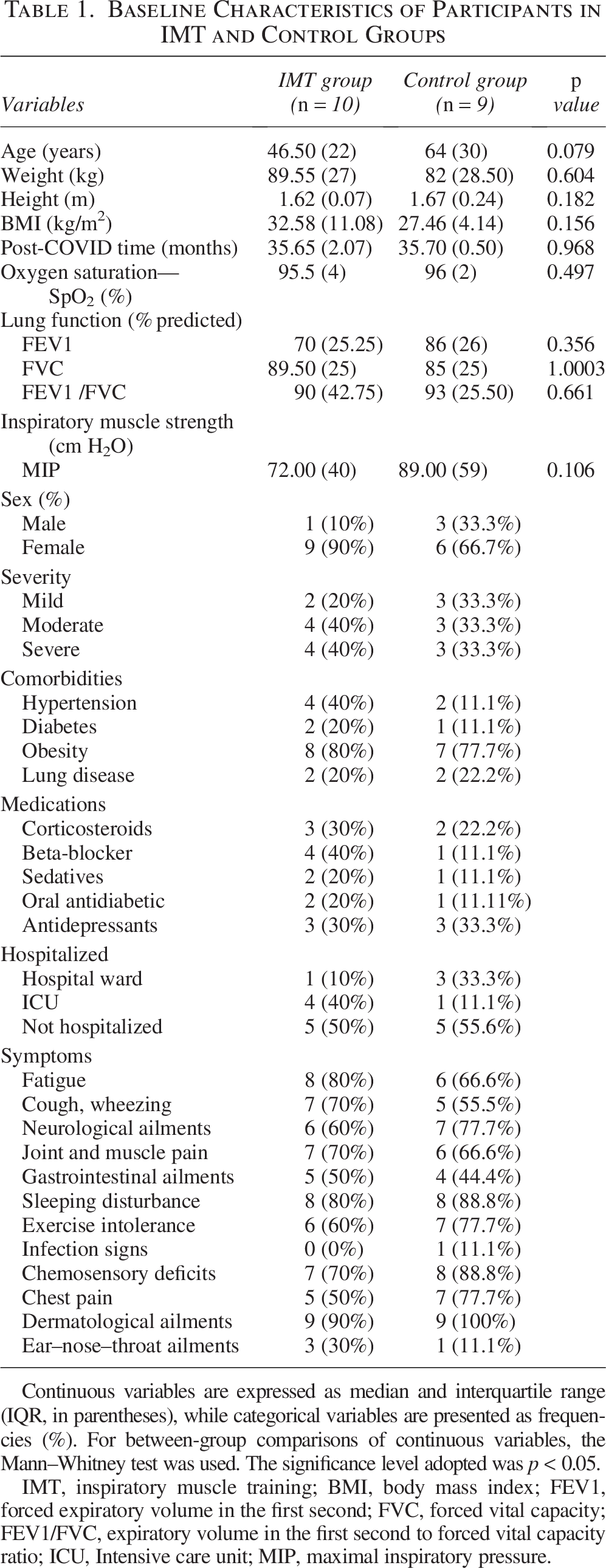
Continuous variables are expressed as median and interquartile range (IQR, in parentheses), while categorical variables are presented as frequencies (%). For between-group comparisons of continuous variables, the Mann–Whitney test was used. The significance level adopted was p < 0.05.
IMT, inspiratory muscle training; BMI, body mass index; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; FEV1/FVC, expiratory volume in the first second to forced vital capacity ratio; ICU, Intensive care unit; MIP, maximal inspiratory pressure.
Inspiratory muscle strength
Analysis of the treatment effects showed a significant increase in MIP (Median [IQR]: 72 [40] vs. 135.5 [40] cmH2O; p = 0.005; r = 0.64), pre- and post-treatment, respectively. There was no significant increase pre- and post-treatment in the sham group with Median [IQR]: 89 [59] versus 87 [58] cmH2O; p = 0.407; r = 0.057, respectively. In the between-group comparison, the IMT treatment showed a significant improvement in MIP, with results superior to the control group (Median [IQR]: 135.5 [40] cmH2O vs. 87 [58]; p = 0.010; r = 0.53).
After the 8-week intervention, the IMT group exhibited higher peripheral oxygen saturation compared with the control group. The median SpO2 was 98% (IQR = 2) in the IMT group and 96% (IQR = 2) in the control group (p = 0.017, r = 0.61). The within-group analysis revealed a significant difference in the IMT group, with the median SpO2 increasing from 95.5 (IQR = 4) to 98 (IQR = 2) cmH2O (p = 0.028, r = 0.50), while in the control group, no significant change was observed (Median [IQR]: 96 [2] vs. 95 [2] cmH2O; p = 0.903; r = 0.02).
Inhalation
In the inhalation testing, the IMT group showed an increase in total lung count (Kcts) post-treatment (p = 0.028, r = 0.50), whereas no significant changes were observed in the control group (p = 0.374, r = 0.22). The increase in the IMT group was most significant in the right lung (p = 0.005; r = 0.64). In the left lung, no significant difference was found in the total count (p = 0.093, r = 0.39). In the between-group analysis, significant differences were observed for all variables (Table 2).
Comparison of Radiopharmaceutical Activity in the Inhalation Phase Between the IMT and Control Groups Across Different Pulmonary Regions
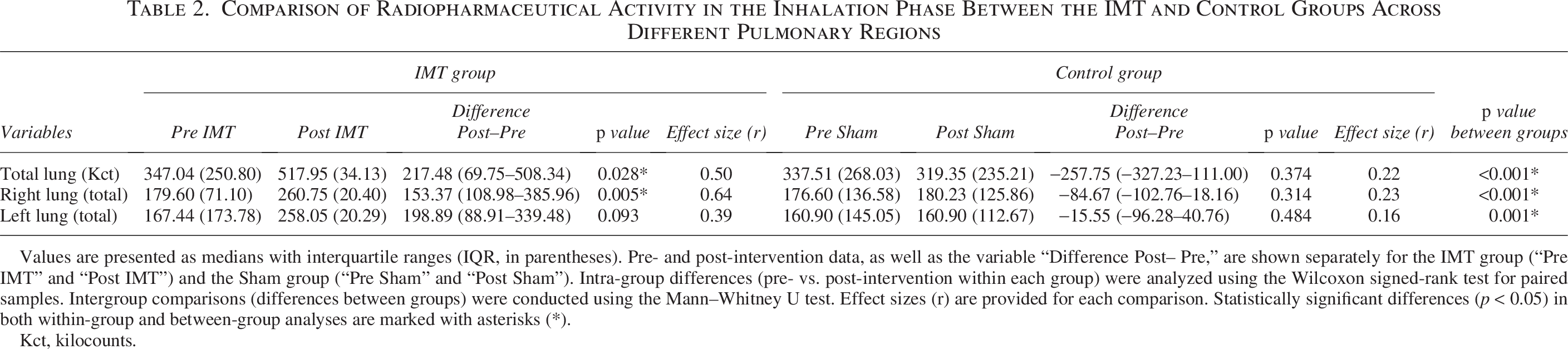
Values are presented as medians with interquartile ranges (IQR, in parentheses). Pre- and post-intervention data, as well as the variable “Difference Post– Pre,” are shown separately for the IMT group (“Pre IMT” and “Post IMT”) and the Sham group (“Pre Sham” and “Post Sham”). Intra-group differences (pre- vs. post-intervention within each group) were analyzed using the Wilcoxon signed-rank test for paired samples. Intergroup comparisons (differences between groups) were conducted using the Mann–Whitney U test. Effect sizes (r) are provided for each comparison. Statistically significant differences (p < 0.05) in both within-group and between-group analyses are marked with asterisks (*).
Kct, kilocounts.
Perfusion
A significant increase in counts was observed in the total lung (p = 0.013, r = 0.57) and in both the right (p = 0.005, r = 0.64) and left (p = 0.007, r = 0.62) lungs separately post-treatment in the IMT group (Table 3). In contrast, total lung counts decreased significantly post-treatment, compared with pre-treatment, in the control group (p = 0.015, r = 0.55), and there were no significant differences between pre- and post-treatment in the right (p = 0.161, r = 0.32) and left (p = 0.515, r = 0.15) lungs separately (Table 3). The difference in counts between pre- and post-treatment in the right lung was significantly greater for the IMT versus the Sham group (p = 0.010) (Table 3).
Comparison of Radioaerosol Activity During the Perfusion Testing Between the IMT and Control Groups

Data are expressed as medians with interquartile ranges (IQR, shown in parentheses). For both groups, values are presented at baseline (“Pre IMT” or “Pre Sham”) and after intervention (“Post IMT” or “Post Sham”), together with the calculated “Difference Post–Pre.” Within-group comparisons (pre- vs. post-intervention) were performed using the Wilcoxon signed-rank test, while between-group comparisons were analyzed with the Mann–Whitney U test. Effect sizes (r) are also reported. Statistically significant differences (p < 0.05) are indicated by asterisks (*).
The incidence of adverse effects related to IMT was low in both groups. In the IMT group, 8% of participants experienced transient dizziness and 12% reported mild muscle pain. These were not considered severe enough to interrupt the protocol. In the control group, 4% of participants complained of fatigue.
A representative set of scintigraphic images from each group is displayed in Figure 2, illustrating the visual changes in aerosol deposition and pulmonary perfusion pre- and post-intervention. Notably, the IMT group exhibited a visible enhancement in both aerosol deposition and perfusion patterns following treatment, whereas the control group showed no appreciable visual difference following treatment. These qualitative findings align with the quantitative results reported.
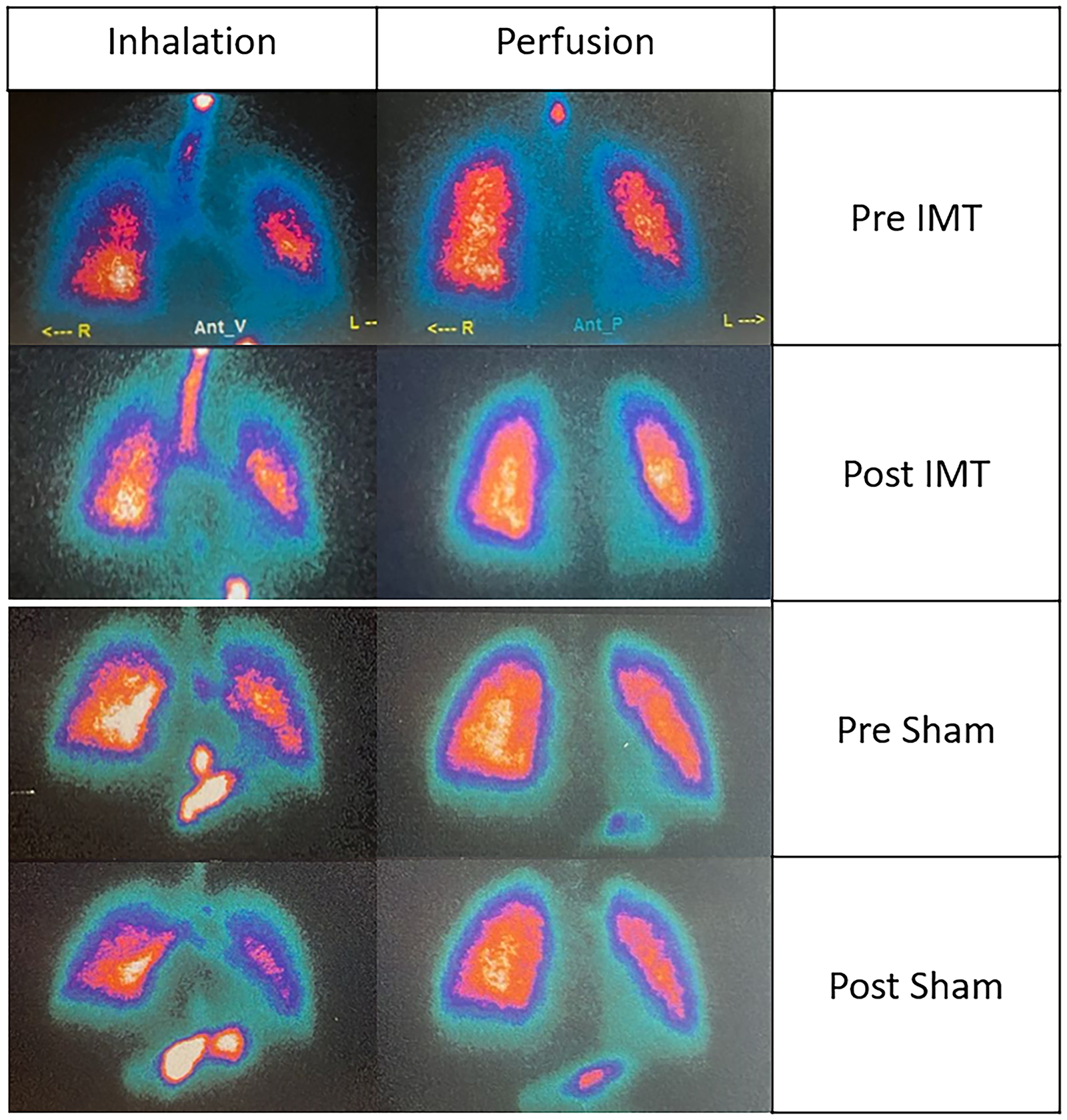
Representative pulmonary scintigraphy images showing inhalation (left) and perfusion (right) scans in one subject from each group, before and after the intervention. For the IMT-treated individual (top two rows), radioactivity appears visibly increased on the perfusion and inhalation scans following treatment. Scans for the individual in the Sham-treated group (bottom two rows) show no, or minimal, changes following treatment.
Discussion
This is the first study to report improved aerosol deposition and perfusion following IMT treatment in individuals with post-COVID-19 syndrome. Within-group comparisons showed that aerosol deposition was significantly increased in the total lung and the right and left lungs separately, post-treatment, in the IMT-treated group. This was demonstrated by a significant increase in radioactivity (counts) in these regions following radioaerosol inhalation post IMT treatment. No significant increases in activity were observed in the Sham-treated group post-treatment. Previous research has shown that post-COVID-19 patients often exhibit altered pulmonary function, with some regions experiencing suboptimal airflow and deposition.25–27 These results suggest that IMT treatment may enhance airflow, thereby improving deposition of aerosols in post-COVID-19 patients.
Between-group comparisons of post-treatment differences in activity in the three regions following radioaerosol inhalation revealed significant differences, with increased activity in all regions in the IMT-treated group compared with the Sham-treated group. Interestingly, 40% of the IMT-treated groups were classified with moderate to severe disease, versus 33.3% of the Sham-treated group, and 70% of the IMT-treated group complained of coughing and wheezing symptoms versus only 55.5% of the Sham-treated group. These findings suggest that individuals in the Sham-treated group may have been healthier than those in the IMT-treated group, with only right lung involvement. Long COVID is a condition that remains heterogeneous and insufficiently phenotyped. Although we employed a standardized symptom severity score to classify participants and enhance comparability between groups, residual differences in unmeasured clinical, or biological, characteristics may still have influenced these results. An additional limitation that could have influenced this result was the absence of computed tomography (CT) images, which restricted our ability to perform a more detailed evaluation of each participant’s pulmonary impairment, which could have improved our ability to classify the severity of their disease.
Radioactivity was significantly increased in all regions in the IMT-treated individuals following perfusion with 99mTc-MAA. No increase was observed in any of the three regions in Sham-treated individuals. It remains unclear why between-group comparisons did not reveal a significant increase in activity in the left lung or in total lung counts of IMT-treated individuals following perfusion. However, anatomical co-registration for region of interest delineation was not possible for this study. Therefore, no transmission image, or CT scan, was available to standardize the right and left lung boundaries. Instead, lung borders were determined from the radioactivity patterns, using consistent image contrast and blinded visual assessment by an experienced nuclear medicine specialist. While every effort was made to minimize variability, the lack of anatomical references limited reproducibility of the lung borders for each participant on each study visit, and this lack of reproducibility could have affected regional quantification.
In contrast to the perfusion findings, between-group comparisons of post-treatment differences following aerosol deposition with 99mTc-DTPA showed that activity was significantly increased in the total lung as well as in both the right and left lungs of IMT-treated individuals compared with the Sham-treated individuals. This suggests that aerosol deposition may have been more affected by the IMT treatment than perfusion.
One explanation for the above finding could be the significant increase in inspiratory muscle strength induced by IMT training. The data show that the IMT group exhibited a marked improvement in MIP, representing a medium effect size, indicating superior performance compared with the Sham group, which showed no significant change. This improvement in muscle strength may have contributed to greater lung expansion, thereby enhancing airflow and improving aerosol deposition. In this context, aerosol deposition measurements may have been more sensitive to the functional improvements achieved through IMT than perfusion measurements. Furthermore, the between-group comparison further demonstrated that the IMT treatment resulted in significantly greater improvements in inspiratory muscle strength than the Sham group, reinforcing the effectiveness of IMT in enhancing respiratory function and aerosol delivery.
The observed improvement in overall perfusion is aligned with a statistically significant increase in oxygen saturation (SpO2) in the IMT-treated group, but not in the Sham-treated group, following the 8-week intervention. After the 8-week intervention, the IMT group exhibited higher peripheral oxygen saturation compared with the control group. The within-group analysis also revealed a significant difference (pre- vs. post-treatment) in the IMT group, while in the control group, no significant change was observed. It is generally accepted that even modest increases in SpO2 can indicate relevant physiological adaptations. 28 These results suggest a positive impact of IMT training on oxygenation through improved perfusion, as previously described.29–31
The effect sizes observed in our study provide important information regarding the clinical significance of IMT treatment in this population. According to Cohen’s criteria, the effect sizes for aerosol deposition in the IMT-treated group were moderate for total lung (r = 0.50) and right lung (r = 0.64), and small to moderate for the left lung (r = 0.39), indicating clinically relevant improvements in pulmonary deposition following IMT compared with the sham treatment. Similarly, the effect sizes for perfusion in the IMT group were moderate for the total lung (r = 0.57) and left lung (r = 0.62), and moderate-to-large for the right lung (r = 0.64). In contrast, the effect sizes in the Sham-treated group were consistently small or negligible. These results suggest that IMT not only led to statistically significant improvements but also produced effects of moderate magnitude, reinforcing the clinical relevance of IMT in enhancing aerosol deposition and pulmonary perfusion in individuals after COVID-19.
It is worth noting that participants in the Sham-treated group also performed maximal inspiratory maneuvers, at ambient pressure without resistance, and these maneuvers represent a greater respiratory workload than their usual breathing pattern. While this regimen did not result in statistically significant improvements in perfusion and radioaerosol deposition, it may have induced minor physiological responses such as transient alveolar recruitment or neuromuscular adaptation through motor learning. However, these possible non-specific effects are unlikely to explain the magnitude and consistency of the improvements observed in the IMT-treated group, which were likely driven by true physiological adaptation to inspiratory muscle overload.
Conclusion
Our findings suggest a role for IMT for the rehabilitation of patients with post-COVID-19 syndrome. Incorporating IMT into pulmonary rehabilitation programs may represent a cost-effective tool to improve the deposition of inhaled medications and enhance pulmonary perfusion and oxygenation. Further research is warranted to better understand how these findings of IMT-related changes on perfusion and aerosol deposition may translate to reduced symptoms reported by post-COVID-19 patients.
Authors’ Contributions
J.C.N.J.: Methodology, conceptualization, investigation, data curation, formal analysis, writing—original draft. A.D.A.: Writing—review and editing, resources, methodology, investigation, supervision, conceptualization. S.S.B.: Writing— review and editing, resources, supervision, investigation. J.B.F.: Writing— review and editing, conceptualization. D.X.: Writing— investigation, data curation, methodology, conceptualization. R.T.: Writing— investigation, data curation, methodology, conceptualization. A.A.: Writing—review and editing, conceptualization. C.R.: Writing—review and editing, resources, methodology, conceptualization. S.C.: Writing—review and editing, visualization, supervision, resources, methodology, investigation, conceptualization. D.B.: Writing—review and editing, visualization, supervision, resources, methodology, investigation, conceptualization. All authors read and approved the final article.
Footnotes
Acknowledgments
The authors dedicate this work to the memory of Anna Myrna Jaguaribe de Lima, their co-supervisor, whose guidance, commitment, and invaluable contributions were essential to the completion of this study.
Author Disclosure Statement
J.B.F. is the Chief Scientific Officer (CSO) of Aerogen Pharm. A.A. discloses her relationships with the COPD Foundation, Aerogen Ltd., Fisher & Paykel Healthcare, and the U.S. Department of Labor. The remaining authors declare no conflicts of interest related to this study.
Funding Information
This study was partly financed by CNPq 421756/2021-7, 40334/2020-5, 312587/2022-8, 403341/2020-5, and 445567/2023-6, the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) Finance code 001, and FACEPE APQ 0801-4.08/21, APQ 306240/2021-1, APQ 0801-4.08/21, and APQ 0249-4.08/20.