
Abstract
Background/Aim:
In the treatment of respiratory diseases, the skill and adherence to inhaler device use are very important. Therefore, frequent replacements of devices that patients are accustomed to are not recommended due to concerns that it may disrupt adherence. The purpose of the study is to determine the frequency of inhaler device replacement, the reasons for replacement, and to evaluate inhaler adherence and usage skills after replacement.
Materials and Methods:
Patients who had been receiving inhaler treatment for at least 1 year due to chronic respiratory diseases (COPD and asthma) were consecutively included in the study. Patients’ inhaler device satisfaction, skill status, device education status, and whether their devices were changed were noted.
Results:
A total of 260 patients were included in the study. Thirty-one patients (11.9%) stated that they did not receive device training, and 40 patients (15.4%) stated that they received insufficient training. Device replacement had been performed in 158 patients (60.8%). 138 (87.3%) of the patients whose devices were changed were satisfied with their new devices. The most common reason for the change was that the patient wanted the change (54/34.2%). In 45 of the patients, the change was made without any explanation (28.4%). In 27 patients (17.1%), the replacement had been made because the formulation needed to be replaced. In 17 patients (10.8%), the device had been replaced due to side effects of the old device, and in 15 patients (9.5%), the device had been replaced because they could not use the device with the correct technique. Device usage skills were found to be better in the group whose devices were replaced than in the group whose devices were not replaced. (p = 0.04).
Conclusion:
Our findings suggest that device replacement seems to be a good option for patients who are not satisfied with their device. Although frequent device replacement is not recommended, it may be useful for patients with insufficient prior education, as the new device will provide a new training opportunity.
Introduction
The main treatment for chronic respiratory diseases is inhalation therapies due to their many advantages. The most important of these advantages are “quick onset of effect, long duration of effect, and fewer side effects”. In addition to all these advantages, inhalation therapy has an important and “often overlooked” disadvantage. A device is needed to deliver the formulation to the lungs by inhalation. When giving a device to patients, regardless of its simplicity or complexity, it is necessary to describe it to the users. However, due to reasons such as intense workload, insufficient time allocated to a patient in outpatient clinics, lack of awareness in the physician prescribing the device, lack of habit of teaching inhaler devices to patients, variety of inhaler devices on the market, communication/language problems, and cognitive deficiencies of patients, ideal device training is not always possible. When inhaler training is not provided, approximately half of the patients use their medications incorrectly or “fail to use” their medications in a way that prevents the active ingredient from reaching the lungs at all.1,2 As a result, situations such as “failure to achieve clinical improvement, progression of the disease, frequent exacerbations, frequent hospital visits, frequent hospital stays, increased treatment costs and bed occupation, waste of medicine, loss of trust in the physician, loss of faith in medical treatment, and resorting to non-medical alternative methods” occur. 3 Additionally, it has been shown that some patients cannot use some devices correctly despite training.4,5 Therefore, this statement is not incorrect: “The best inhaler is the one that the patient can use best.” 6 Patient adherence with the device is very important for the success of the treatment. For this reason, it is not recommended that the physician change the inhaler device that the patient is using correctly unless necessary. However, in clinical practice, we see a wide variety of inhaler devices in the hands of patients. There are many different types of inhaler devices from many pharmaceutical companies on the market, and changes can be made by the physician among these for various reasons. It seems reasonable to assume that patients continuing their treatment with a single type of inhaler would improve medication adherence. Based on this logic, frequent device changes could negatively impact patients’ ability to use the device correctly.
There are many studies investigating inhaler device adherence issues. However, studies evaluating device replacement are scarce.7,8 Our aim in the study is to reveal the frequency of inhaler device replacement, the reasons for it, and to evaluate inhaler usage skills with the new device after replacement.
Materials and Methods
The study was conducted as a multicenter study. Data were collected by experienced pulmonologists through detailed questions about patients’ past inhaler device usage characteristics. Patients who presented to the pulmonary outpatient clinic of 7 centers and used inhalers for at least 1 year due to chronic respiratory diseases (COPD and asthma) were consecutively included in the study. Their diagnoses were confirmed by pulmonary function tests and specialist physician evaluation. Patients who could not use the device on their own due to visual, auditory, and cognitive impairments were not included in the study. Patients who had difficulty recalling or showed hesitation weren’t included in the study. Patients using multiple types of devices and patients using nebulizers were not included in the study. Patients in acute attacks or exacerbations were excluded from the study (Fig. 1). Following the participants’ consent, a study questionnaire was applied, including their sociodemographic characteristics, whether they received training on the correct use (CU) of the inhaler, information on the device they currently use, and whether their inhaler devices were changed. Patients’ use of their current devices was observed by a pulmonologist.
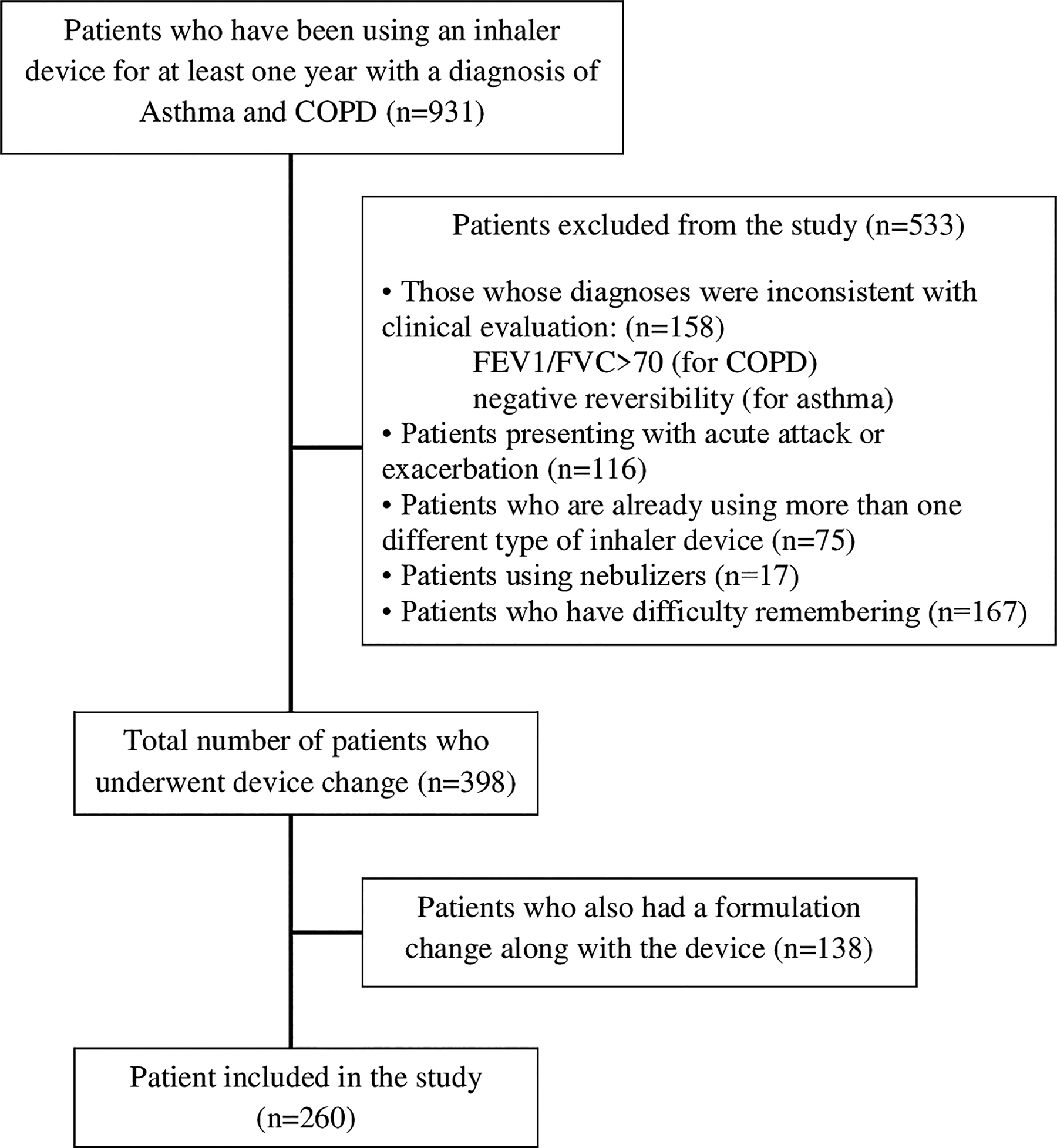
Flowchart of the study.
Device usage skills were assessed based on the “A Guide to Aerosol Delivery Devices for Respiratory Therapists” 9 published by the American Association of Respiratory Care. Since the number of inhalation procedure steps was different for each device, two common statuses were defined to facilitate statistical analyses: CU and incorrect use (IU). Patients who completed all steps correctly, as well as those who made errors in steps other than critical errors such as not rinsing the mouth, not fully exhaling before use, not fully holding the device upright, and holding their breath for <10 seconds, were recorded as “Correct usage.” Any errors outside of these steps (where the active substance was partially or completely prevented from reaching the lungs) were recorded as “Incorrect usage.” The inhaler devices and maintenance therapy formulations included in the study consisted of combinations of long-acting muscarinic antagonists (LAMA), long-acting beta2-agonists (LABA), and corticosteroids (ICS).
The aim of the study was to focus on adherence and satisfaction after device change. Therefore, patients who underwent a formulation change along with the device change were excluded (as this would affect satisfaction). Changes between LABA, LAMA, and ICS groups were considered as formulation changes.
All applications and trainings were performed face-to-face by chest diseases specialist physicians. Training was provided to patients who used it incorrectly. Informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki. Artificial intelligence (AI)-supported technologies were not used in the production of the study.
Statistical analysis
Statistital analyses were carried out using the SPSS/PC software (IBM Inc., version 21, Armonk, NY, USA.) Since the obtained data were categorical variables, descriptive statistics were given as frequency and percentage n (%). Evaluation of normality was performed with the Shapiro-Wilk test. Normally distributed continuous variables were compared with the paired sample t-test. The Mann-Whitney U test was used in groups with non-normal distribution. A p value < 0.05 was considered significant.
Results
A total of 260 patients were included in the study. Of these, 130 (50%) had COPD, 118 (45.4%) had asthma, and 12 (4.6%) had asthma-COPD overlap syndrome. The average number of years of use of the inhaler device was 7.4 years. When the current devices were evaluated, capsule inhalers were used most frequently by 118 patients (45.4%). This was followed by Diskus-Ellipta with 111 (42.7%) and metered dose inhalers (pMDI) with 19 (6.5%). Thirty-one (11.9%) of the patients stated that they did not receive device training, and 40 (15.4%) stated that they received insufficient training. Device replacement had been performed in 158 patients (60.8%). Of these, 128 (49.2%) had their devices changed once, 24 (9.2%) had their devices changed twice, and 6 (2.3%) had their devices changed three times. 138 (87.3%) of the patients whose devices were changed were satisfied with their new devices. The most common reason for the change was that the patient wanted the change (54/34.2%). In 45 of the patients, the change was made without any explanation (28.4%). In 27 patients (17.1%), the change was made because the active ingredient needed to be changed (provided they are from the same group). In 17 patients (10.8%), the device was changed due to side effects of the old device, and in 15 patients (9.5%), the device was changed because they could not use the device with the correct technique. When the patients who wanted to change their devices because they could not use them with the correct technique were evaluated, all but one patient (93.3%) were satisfied with their new devices.
When the reasons of the patients who wanted the change were evaluated, 17 stated that it was not sufficient for the treatment, 6 stated that they could not use it correctly, 5 stated that it had side effects, and 5 stated that they did not feel the medicine coming. (Table 1).
Sociodemographic and Clinical Characteristics of Patients
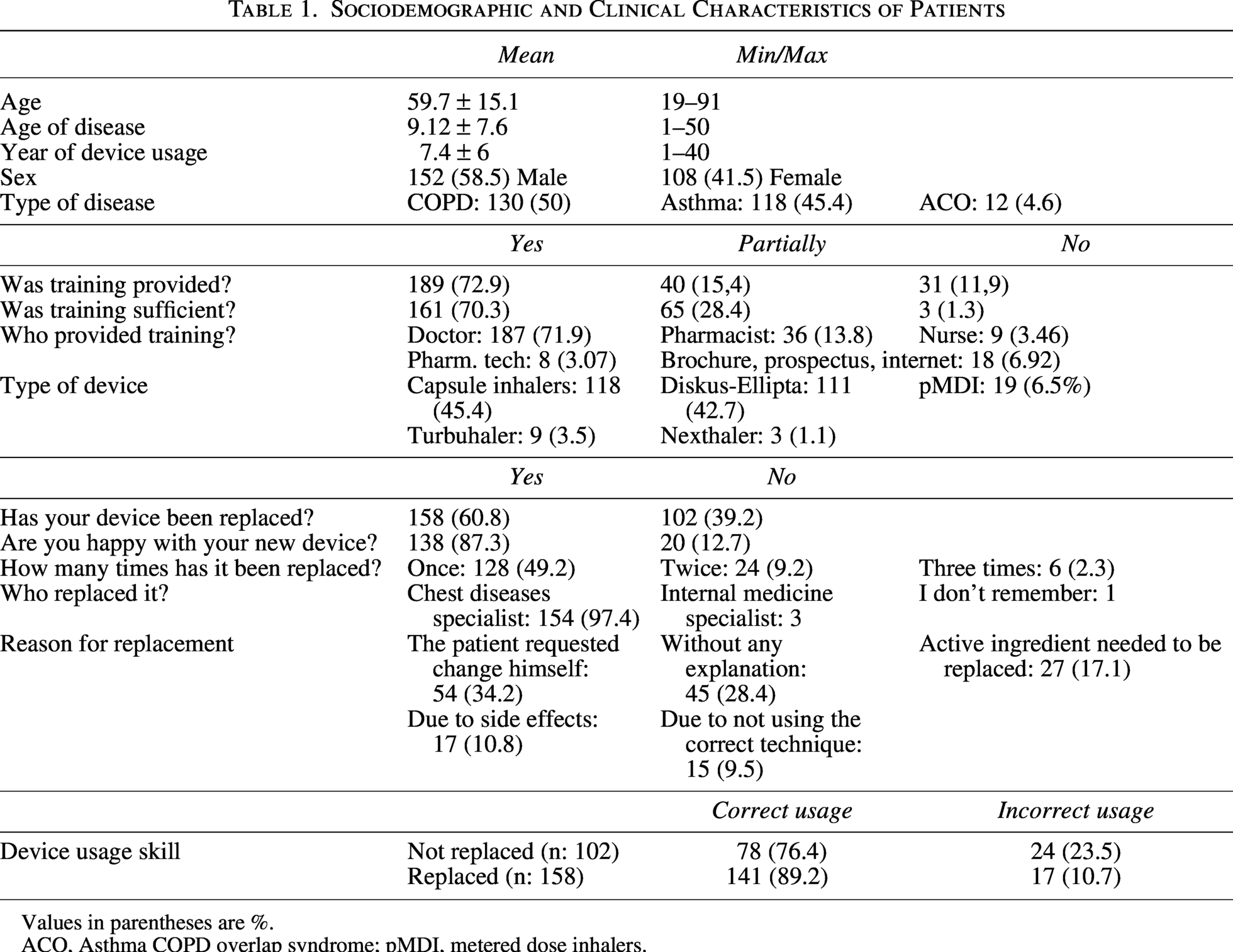
Values in parentheses are %.
ACO, Asthma COPD overlap syndrome; pMDI, metered dose inhalers.
Twenty patients who were also not satisfied with their new device after the change were examined. As for the reasons for dissatisfaction, 9 stated that it was not sufficient for the treatment, 4 stated that they could not use it correctly, and 4 stated that they did not feel the medicine coming.
The most changes were made from the capsule inhaler to the Discus-Ellipta device (n = 32). Secondly, the opposite was the case, with a change from Discus-Ellipta to a capsule inhaler (n = 26).
Device usage skills were found to be better in the group whose devices were replaced than in the group whose devices were not replaced. (p = 0.04)
Discussion
There is a wide range of inhalers for COPD and asthma on the market, each with its own required technique. Previous studies showed that using a mix of inhaler devices could lead to more inhaler technique errors due to the confusion and mismatch between inhaler technique instructions between devices.10,11 Therefore, the GOLD 2026 and GINA 2025 guidelines recommend that, if possible, the formulation be administered via a single inhaler device.12,13 Unlike others, our study focused on the effect of device change on adherence, rather than potential issues for those using multiple types of devices.
Contrary to our expectations, satisfaction rates following device replacement were high. There may be two reasons for this. First, the patient may not be able to use their previous device correctly due to the inadequacy of the training given before the change. Thus, the training given after the change may have increased adherence. To prove this, we would have needed to evaluate the patient’s technique for using the previous device. However, we were not able to do this. This was an important limitation of our study. The second possibility may be related to the physician’s behavior of emphasizing device training more when making the change. In our opinion, this is related to the aim of convincing the patient to make the change. It is natural for success to increase after the change in patients whose reason for the change was already determined as not being able to use the previous drug with the correct technique. In our study, all but one of the patients in this group who underwent a device change were satisfied with their new devices.
Secondly, patients who wanted the change themselves may have requested training to cooperate with the new device. The satisfaction rate in this group of patients was found also to be high. The lowest satisfaction rate was obtained in patients who were changed without explanation.
Perhaps this group includes patients who were changed due to sponsorship activities of the pharmaceutical industry. In fact, this data revealed an important result of our study. Based on this data, we do not recommend making a change without sufficient justification (formulation change, side effects, inability to use with the correct technique, etc.).
There are very few studies in the literature focusing on the effect of device changes on adherence. Studies have focused more on the error rates of multiple and different types of device use. In the study conducted by van der Palen J and colleagues in the Netherlands, three hypotheses were tested: first, patients using only one type of inhaler will demonstrate adequate inhalation technique more often than those with two or more types. Secondly, patients using a combination of dry powder inhalers (DPIs) will demonstrate correct inhalation technique more often than those using the combination of an MDI and a DPI. Thirdly, some inhalers or combinations of inhalers are more prone to erroneous inhalation technique than others. As a result, it has been found that patients using a single type of inhaler make fewer errors. It has been argued that, whenever possible, only one type of inhaler should be prescribed, and if a combination is unavoidable, DPI combinations should be preferred over MDI and DPI. 14
In a study conducted in the UK on a cohort of 8225 COPD patients in both arms, patients in the similar-devices cohort had a lower rate of exacerbations compared with those in the mixed-devices cohort and were less likely to be in a higher-dose SABA group. As a result, COPD patients prescribed one or more additional inhalers requiring similar inhalation techniques had better outcomes compared to those prescribed devices requiring different techniques. 10
Park et al. conducted a switch study based on the hypothesis that use of combination inhalers for asthma would be associated with poorer inhaler technique and outcomes. They switched patients’ medications to pMDI only. They found significant improvements in asthma exacerbation-free days and asthma control when patients’ devices were switched to a single type. 15
Dijk et al., in their study comparing the nature and frequency of inhaler technique errors in COPD patients using single DPI or mixed devices (one DPI and one pMDI), showed the opposite result. They found no significant difference between patients prescribed single DPI and mixed devices. In this study, patients with COPD using mixed devices did not make more errors compared with patients using a single DPI, although the unadjusted analysis showed a higher proportion of ‘critical’ inhaler technique errors in patients prescribed with mixed devices as compared with patients using a DPI-only. 16
Since objective data on inhaler device replacement are insufficient, this issue is not clear enough. Larger studies are needed to reveal the results of replacement. In our opinion, device replacement may disrupt adherence in a patient who uses it properly, and it seems to be a good option for patients who are not satisfied with their device. Although frequent device replacement is not recommended, it may be useful for patients with insufficient prior education, as the new device will provide a new training opportunity. ∼30% of our patients declared that they did not receive adequate inhaler device training. This result reveals that we are still not at a sufficient level in inhaler device training and suggested that we need to work on increasing training rates.
Our study has some limitations. One of them is that we could not determine our patients’ device usage skills before the replacement. Secondly, It would be interesting to know whether disease control is better or worse after the device is replaced. Unfortunately, we were unable to determine this because we did not obtain the previous control data. Thirdly, the reasons for the replacement were based on patient statements. All these reasons make it difficult to generalize our study. However, we believe it can provide an idea for future studies. The valuable aspect of our study is that it is multicenter and one of the rare studies focusing on this area. We believe it is considerable in supporting future research.
In our opinion, in countries/regions where medication is prescribed with adequate device inhaler training at the beginning, replacing medication may impair adherence. Conversely, in countries/regions where devices are prescribed without adequate training at the beginning, replacing device may improve adherence by re-providing training. National and regional studies are needed on this issue.
Switching requires careful consideration and if possible, should not be done without patient consent. Switching devices requires several steps to consider. The first step should be to review the patient’s control status. Then, the causes of suboptimal control (e.g., triggers, smoking, noncompliance, poor inhaler technique) should be addressed before device switching. The patient’s inhalation skills, such as inhalation effort strength, should also be assessed. Next, device switching should be performed, and retraining should be provided for the new device, taking into account patient preferences. 8
In conclusion, our study has shown that patients should be asked about their device satisfaction and their change requests at each visit, and that device change increases adherence in patients who are dissatisfied with their medications and request a change.
Authors’ Contributions
Study conception and design: M.S. and Y.A. Material preparation, data collection, and analysis: Ş.A.A., D.S.U., Ç.K., M.B.G., E.S.G., F.E., M.Ö.A., Y.S., and M.Ç. First draft of the manuscript was written: Y.A. All authors read and approved the final manuscript.
Footnotes
Author Disclosure Statement
All authors should also disclose any conflict of interest that may have influenced either the conduct or the presentation of the research.
Funding Information
Made with the support of the Turkish Respiratory Association (TUSAD) Young Academicians Group (GEAK).
Ethics Committee Approval
This study received ethical approval from the Clinical Research Ethics Committee of Sakarya University on 15.05.2024, with decision number 372956-167.