
Abstract
Injuries to the ulnar collateral ligament (UCL) in throwing athletes frequently occurs from the repetitive valgus loading of the elbow during the throwing motion, which often results in surgical reconstruction of the UCL requiring a structured postoperative rehabilitation program. Several methods are currently used and recommended for UCL reconstruction using autogenous grafts in an attempt to reproduce the stabilizing function of the native UCL. Rehabilitation following surgical reconstruction of the UCL begins with range of motion and initial protection of the surgical reconstruction, along with resistive exercise for the entire upper extremity kinetic chain. Progressions for resistive exercise are followed that attempt to fully restore strength and local muscular endurance in the rotator cuff and scapular stabilizers, in addition to the distal upper extremity musculature, to allow for a return to throwing and overhead functional activities. Rehabilitation following UCL reconstruction has produced favorable outcomes, allowing for a return to throwing in competitive environments.
Injury to the ulnar collateral ligament (UCL) in overhead athletes has been widely reported, 4,19 resulting in significant functional limitations in throwing athletes, including medial elbow pain, loss of throwing velocity and accuracy, instability, neurologic symptoms, and decreased muscular strength. These problems emerge during the acceleration phase of the throwing motion, where chronic, repetitive, microtraumatic stress occurs as the elbow extends at speeds over 2300 degrees per second, producing a medial shear force of 300 N and a compressive force of 900 N. 11,21 The valgus stress applied to the elbow during the acceleration phase of throwing is 64 N·m, 11,21 which exceeds the ultimate tensile strength of the native UCL. 7 Therefore, proper mechanics and optimal strength and endurance of the muscles of the upper extremity kinetic chain are needed to assist with load attenuation to prevent injury. The postoperative rehabilitation guidelines following 2 common surgical techniques of UCL reconstruction: the figure of 8 (modified Jobe procedure) and the docking procedure are presented. Although limited evidence exists supporting one method of rehabilitation over another, this review emphasizes the application of controlled stressors and progressive resistance exercise using basic science knowledge and includes protocols to assist the clinician with progression of athletes during rehabilitation following surgical reconstruction of the UCL.
Surgical reconstruction of the UCL attempts to restore the stabilizing functions of the anterior bundle. 2 The palmaris longus or gracilis graft from the ipsilateral or contralateral side is taken and passed in a figure-of-8 pattern through drill holes in the sublime tubercle of the ulna and the medial epicondyle 2 or in a docking procedure by Rohrbough et al 16 or in a modification of these procedures. Armstrong et al 3 performed cadaveric loading research with the native UCL and several reconstructive procedures using load-to-failure and cyclic loading paradigms. Failure in the native UCL occurred with 2536 cycles, whereas the figure of 8 and the docking procedure required 333 and 701 cycles, respectively. The native UCL failed at 142 N, and the docking procedure and the figure of 8 failed at 53 and 33 N, respectively. Cyclic loading data reflect the initial protective range of motion (ROM), repetitive load to tolerance, and rehabilitation progressions used and recommended during rehabilitation following UCL reconstruction.
Additional surgical procedures are often performed concomitantly with a UCL reconstruction, including subcutaneous ulnar nerve transposition, as well as osteophyte debridement posteromedially on the ulna because of valgus extension overload. 1,29 The rehabilitation program following UCL reconstruction should be based on the surgical procedure performed: the traditional figure of 8 (Table 1) and the docking surgical technique (Table 2).
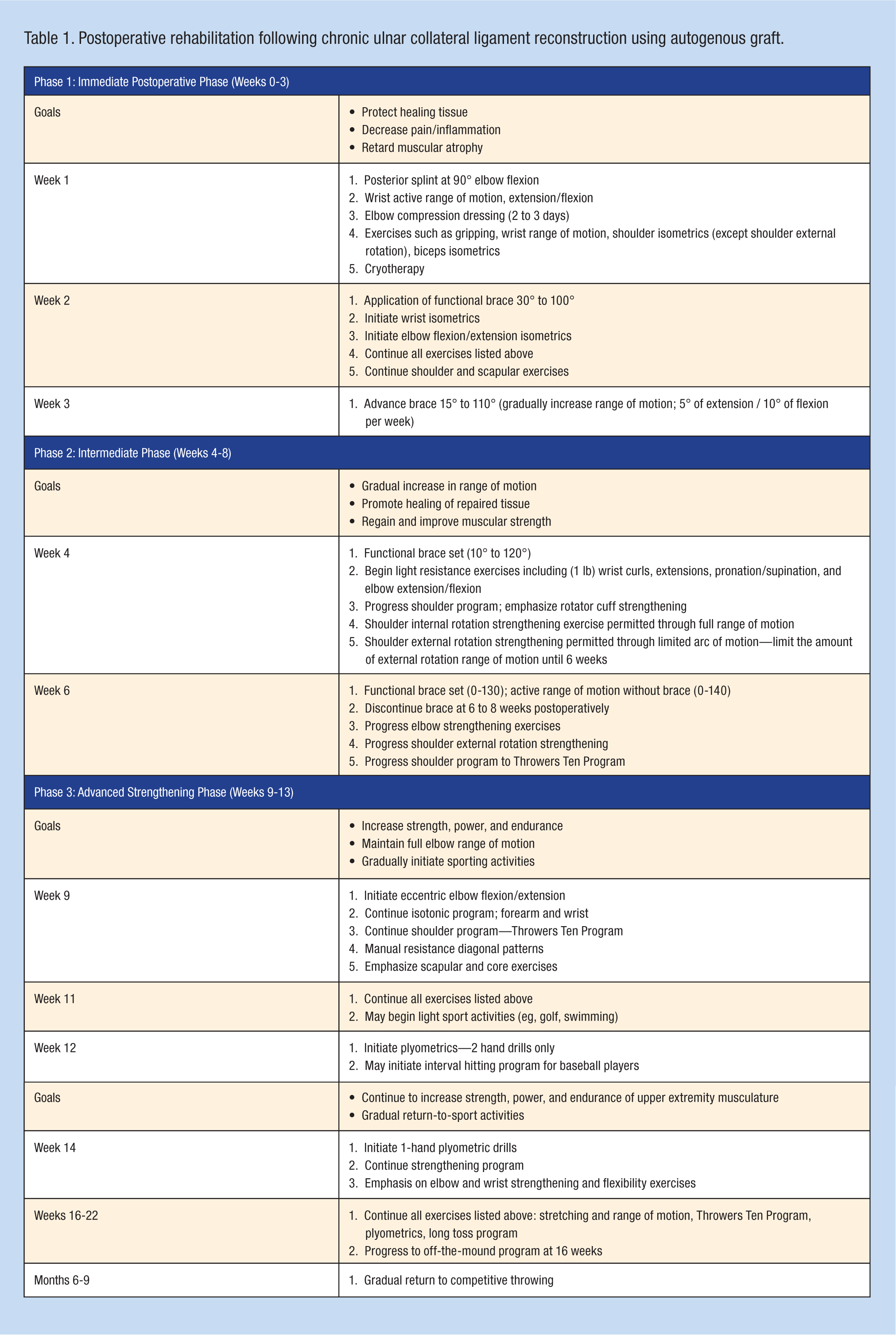
Postoperative rehabilitation following chronic ulnar collateral ligament reconstruction using autogenous graft.
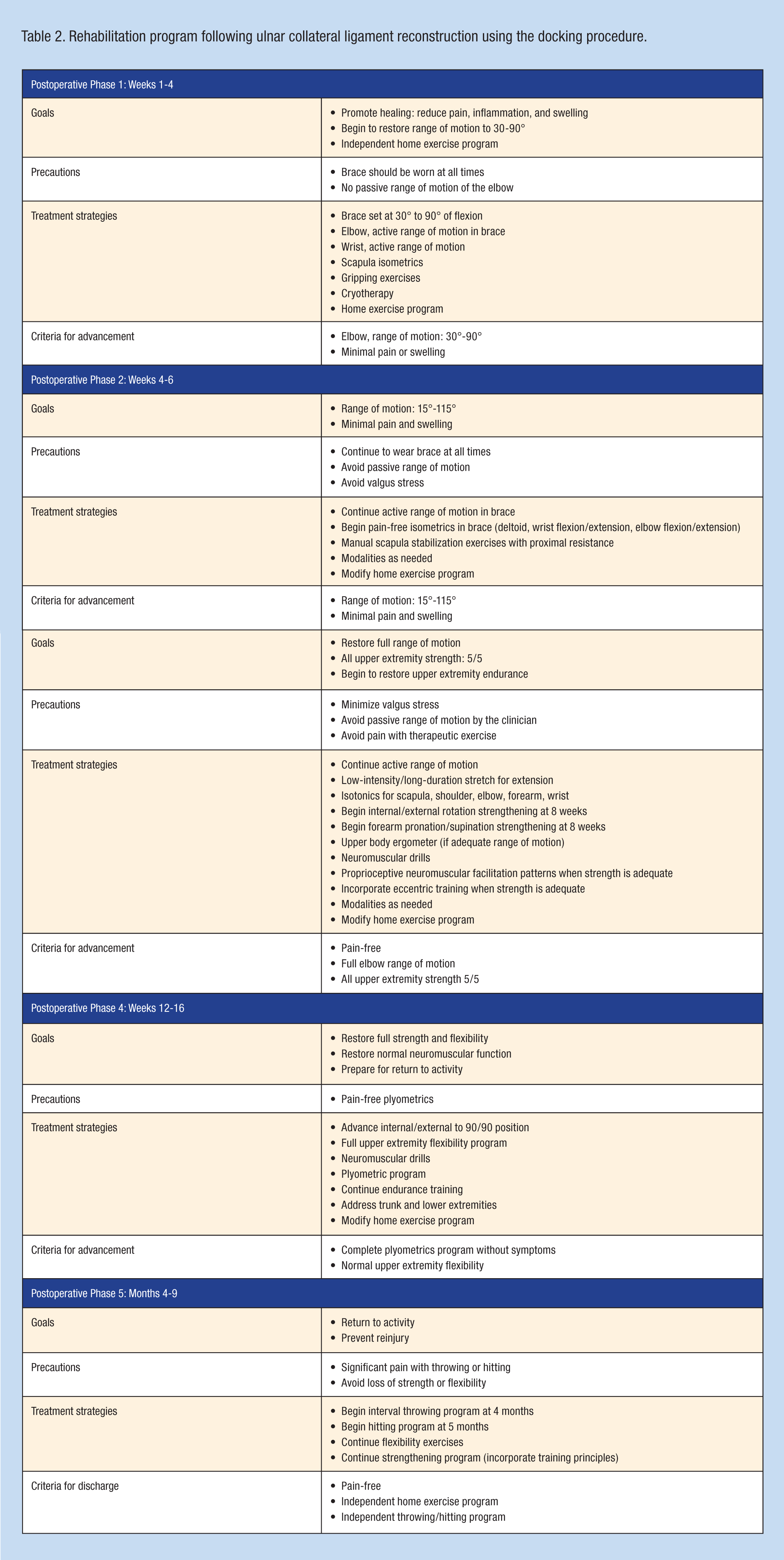
Rehabilitation program following ulnar collateral ligament reconstruction using the docking procedure.
Rehabilitation Program Following the Modified Jobe Procedure
Initial Postoperative Management
The athlete is often placed in a posterior splint, with the elbow immobilized at 90° of flexion for the first 7 days, postoperatively. This allows preliminary healing of the UCL graft and soft tissue slings involved in the nerve transposition. Close monitoring of the ulnar nerve is recommended. The patient is instructed to perform wrist active ROM and gripping, as well as submaximal multiple angle isometrics for the wrist and elbow. One consideration for early postoperative rehabilitation is based on the surgical approach and condition of the flexor pronator origin. The figure of 8 involves the complete detachment of the flexor/pronator origin from the medial epicondyle. Care must be taken not to perform active wrist extension during the initial 6 postoperative weeks. The modified Jobe procedure utilizes a muscle-splitting approach that does not interrupt the flexor/pronator origin, thereby allowing more aggressive early ROM of the wrist and forearm, as well as the initiation of the submaximal isometric exercises. Knowledge of the surgical approach is important to guide the early ROM and resistive exercise progressions.
The patient is progressed from the posterior splint to an elbow ROM brace at 7 days postoperative to initially allow 30° to 100° of extension/flexion ROM. Motion is increased each week by 5° of extension and 10° of flexion. Full passive range of motion (PROM; 0°-145°) is expected by the end of week 6. The brace is discontinued between week 6 and week 8 in most patients. A more rapid return of PROM with acute UCL injuries may be appropriate, with full PROM by week 5 or week 6. For the chronic tears, full PROM is restored more slowly, usually 6 to 8 weeks, postoperatively.
Recent research by Bernas et al (unpublished data, 2008) has provided objective quantification of internal forces on the reconstructed UCL (gracilis graft and docking procedure) during PROM. Simulating early rehabilitative stressors in cadaveric UCL reconstructions, PROM between full extension to 50° of elbow flexion produced less than 3% strain in the anterior and posterior bands of the UCL. In addition, forearm rotation (supination and pronation) has no effect on graft strain. Simulated isometric muscle contractions had no effect on the strain in the UCL reconstructions. The UCL graft and the fascial slings, which stabilize the transposed ulnar nerve, are protected by gradually progressing elbow extension to 30° by week 2 and finally to full elbow extension by week 4 to week 6, postoperatively.
Research has identified the presence of significant elbow flexion contractures in elite-level throwing athletes and in other overhead athletes. Wright et al 30 reported that the average loss of elbow extension was 7.9° and that the average loss of flexion was 5.5° in 33 throwing athletes before the competitive season. Furthermore, Ellenbecker et al 10 measured elbow flexion contractures, averaging 5° in a population of 40 healthy professional baseball pitchers. Directly related to elbow function was wrist flexibility, which was significantly less in extension on the dominant arm because of tightness of the wrist flexor musculature. There was no difference in wrist flexion ROM between extremities.
If the patient has difficulty achieving full extension after UCL reconstruction using ROM and mobilization techniques, a low-load, long-duration stretch may be performed. 13,17,20 This technique can be extremely beneficial for regaining full elbow extension. 25 -27 The patient lies supine with a towel roll or foam placed under the distal humerus to act as a cushion and fulcrum. Light-resistance exercise tubing is applied to the wrist of the patient and secured to the table or a dumbbell on the ground (Figure 1). The patient is instructed to relax as much as possible with the arm in full extension and in forearm pronation for 10 to 15 minutes per treatment. 22,26 The resistance applied should be of low magnitude, to enable the stretch for the entire duration without pain or muscle spasm (ie, low load, long duration). Patients perform the low-load, long-duration stretches several times per day, totaling 60 minutes (eg, 15-minute stretch, 4 times per day). The total end-range time program 12 has been extremely beneficial for patients with a stiff elbow. 26,27

A low-load, long-duration stretch into elbow extension, performed using light resistance.
The aggressiveness of stretching and mobilization techniques is dictated by the healing constraints of involved tissues, the pathology/surgery, the ROM, and the end feel. If the patient presents with a decrease in motion and hard end feel without pain, aggressive stretching and mobilization technique may be used. Conversely, a patient with pain before resistance will be progressed slowly with gentle stretching.
Rehabilitation of the postoperative elbow should include proprioceptive exercises. Angular replication and end-range reproduction exercises can be used early in rehabilitation to stimulate mechanoreceptors in the postoperative joint. Loss of kinesthetic awareness of the upper extremity can occur following injury. 18 Manske et al 14 found decreased proprioceptive acuity in the dominant elbows of college-level baseball pitchers after simulated throwing for 3 innings.
The total arm-strengthening concept should be followed during rehabilitation after UCL reconstruction. Emphasizing proximal scapular stabilization early in the rehabilitation program and continuing this emphasis using a low-resistance, high-repetition program restores the necessary proximal stabilization to promote an optimal return to uncompensated throwing. This includes scapular stabilization via manual resistance to elicit serratus anterior and trapezius/rhomboid muscle activation without compromising the repair.
Rotator cuff strengthening can commence in the first few weeks following UCL surgery. The resistance is applied proximal to the elbow to prevent and/or minimize stresses across the elbow. Prone extension and horizontal abduction are used to recruit the posterior rotator cuff and scapular stabilizers. Internal or external glenohumeral rotation strengthening is permitted in a limited ROM. Excessive glenohumeral joint external rotation produces a valgus moment at the elbow joint.
At this stage in the rehabilitation program, resistance exer- cise is progressed with ROM. From isometric exercises in the immediate postoperative phase, progression including light- resistance isotonic exercises occurs at week 4 for the wrist and forearm. Progression to the full Throwers Ten Program (Figure 2) is targeted by week 6. Additional progressive resistance exercises are incorporated at week 8 to week 9 to develop dynamic stabilization of the medial elbow. Weeks 6 to 12 emphasize stretching, ROM, and strengthening exercises for the glenohumeral joint, scapula, core, and legs (Figure 3). The flexor carpi ulnaris and flexor digitorum superficialis overlay the UCL. Isotonic concentric exercises for these muscles may assist the UCL in resisting valgus stress at the medial elbow. 6

The Thrower’s Ten Program is designed to exercise the major muscles necessary for throwing. The Program’s goal is to be an organized and concise exercise program. In addition, all exercises included are specific to the thrower and are designed to improve strength, power, and endurance of the shoulder complex musculature.

Manual proprioceptive neuromuscular facilitation upper extremity D2 patterns with rhythmic stabilization.
Advanced Rehabilitation Phase
Aggressive strengthening exercises emphasizing higher resistance, functional movements, eccentric contraction, plyometric activities, and isokinetic exercise for the shoulder, forearm, and wrist are now employed at intermediate and fast contractile velocities. Wrist extension/flexion to forearm pronation/ supination followed by elbow extension/flexion is the usual progression. Training speeds from 180 to 300 degrees per second are used in sets of 15 to 20 repetitions to increase strength and muscle endurance (Figure 4).

Isokinetic wrist extension/flexion training at fast contractile velocities.
Elbow flexion exercises are progressed to emphasize eccentric control. The biceps muscle is an important stabilizer during the follow-through phase of overhead throwing. The deceleration of the elbow with eccentric muscle control prevents pathologic olecranon contact within the humeral fossa. 11,29 Elbow flexion can be performed with elastic tubing to isokinetic exercise equipment or manual resistance, emphasizing slow and fast concentric and eccentric contractions. Seated rowing and front latissimus dorsi pull-downs on weight machines are incorporated during this phase. A concentric contraction of the triceps is used because of the acceleration (muscle-shortening) activity during the acceleration phase of throwing.
Neuromuscular control exercises—concentric and eccentric external rotation, including side-lying external rotation with manual resistance—are performed with the addition of rhythmic stabilizations. Manual-resistance exercise including external rotation may progress to standing with exercise tubing at 0° and finally at 90° (Figure 5).

External rotation at 90° of abduction with exercise tubing, manual resistance, and rhythmic stabilizations.
For overhead athletes, plyometric drills can be an extremely beneficial form of functional exercise for training the elbow 24,28 using a weighted medicine ball during the later stages of this phase. Plyometric exercises are initially performed with 2 hands at 12 weeks postinjury: a chest pass, a side-to-side throw, and an overhead soccer throw. Plyometrics progress to 1-hand activities at 14 weeks: 90/90 throws (Figure 6), external and internal rotation throws at 0° of abduction (Figures 7 and 8), and wall dribbles. Plyometric drills for the forearm musculature include wrist flexion flips (Figure 9), snaps, and extension grips.

Plyometric external rotation 90/90 throws for posterior rotator cuff strengthening.

Plyometric internal rotation throws at 90° of abduction.

Plyometric internal rotation throws at 0° of abduction.

Plyometric wrist flips and snaps for the wrist flexors.
An athlete is allowed to begin the return-to-activity phase of rehabilitation upon achieving full ROM, no pain or tenderness, satisfactory isokinetic strength, and a good clinical examination. 15 An interval throwing program is allowed at 16 weeks. The “off the mound” program requires 6 to 8 weeks to normalize pitching mechanics and to reestablish ball velocity and accuracy. In most cases, throwing from a mound is allowed 6 to 8 weeks following the initiation of an interval throwing program. A return to competitive throwing is expected at approximately 9 months following surgery.
Professional throwing athletes have significantly greater wrist flexion and forearm pronation strength on the dominant arm (15%-35%), 9 with no difference in wrist extension or forearm supination between extremities. Greater elbow flexion (10%-20%) in the dominant arm of professional baseball pitchers, as well as greater elbow extension (5%-15%) in bilateral comparisons, has been reported. 23
Rehabilitation Following the Docking Procedure
Postoperative Rehabilitation Program for the Docking Procedure
The rehabilitation program following the docking procedure is similar to the modified Jobe procedure. The most significant differences involve the restoration of elbow ROM: Immediately following surgery, the patient is limited to 30° to 90° for 4 weeks. From 4 to 6 weeks, their ROM is increased to 15° to 115°. The goal is to restore full elbow ROM at 6 to 12 weeks. The strengthening program following the docking procedure is similar to the modified Jobe procedure: Wrist, hand, and elbow ROM and isometrics are permitted immediately following surgery. Shoulder isometrics are not permitted until 4 weeks, postoperatively; isotonic strengthening for shoulder and arm, at 8 weeks; and plyometrics, at 12 weeks. Interval throwing begins at 4 months, postoperatively, and progresses to off-the-mound throwing with a return to competition at 9 to 12 months, postoperatively.
Outcomes Following UCL Reconstruction
The most extensive analysis of outcomes of UCL reconstruction was published in a meta-analysis in 2008. 19 Conway et al 5 reported on 56 baseball players throwing a distance of 15 feet by 4.5 months, with competition at 12.5, postoperatively. The average throwing athlete can throw 15 feet at 3 months and compete at 9 months. An excellent result was achieved in 64% of the reconstructed elbows in elite athletes (ie, achieving a level of activity equal to or greater than that at preinjury), 5 but a flexion contracture was present in 50% at a mean of 6 years following an autogenous UCL reconstruction. 5
A 36-month mean follow-up of 22 patients who underwent the DANE TJ UCL reconstruction technique (ie, humeral docking procedure and distal interference crew fixation in the ulna) 8 revealed 4 complications: 2 patients had ROM loss that required lysis of adhesions and 2 had ulnar neuritis that resolved. Nineteen patients had excellent modified Conway scores at follow-up.
Follow-up on 1294 athletes with modified Jobe procedure and the above rehabilitation program (average follow-up, 4.1 years) showed that 84% had returned to a preinjury level of throwing. The average time to competition was 11.2 months.
Conclusion
Rehabilitation following surgical reconstruction of the UCL requires a gradual and protected return of ROM and an extensive resistive exercise program for the entire upper extremity kinetic chain. Advances in surgical technique and modifications that preserve the origin of the wrist flexors and forearm pronators allow for earlier advancement of the rehabilitation program. Specific resistive exercise progressions aimed at providing dynamic stability to the scapulothoracic, glenohumeral, and ulnohumeral joints form an integral part of the comprehensive rehabilitation of the overhead athlete following reconstruction of the UCL.
Footnotes
No potential conflict of interest declared.